Embed Size (px)
Citation preview
Sherif H Zaky, MD
Professor of critical care medicine,
Cairo University

Emergency medicine and critical care are fields that
often require rapid diagnosis and intervention for
specific situations.
cardiac arrhythmias in intensive care are not only
common ,but can be life threatening or a clue to
more serious prognosis.
AF in The ICU

The purpose of this presentation is to summarize
Atrial tachyarrhythmias in the ICU and strategies
for their management.
AF in The ICU

We mean by atrial tachyarrhythmias ;
Frequent premature atrial ectopies
Atrial tachycardia.
Atrial flutter, and
Atrial fibrillation.
AF in The ICU

Why critically ill ? Structural heart disease
Pulmonary diseases ( hypoxia, acidosis, 2ry pulmonary HTN)
Electrolyte imbalance (K+, Mg+2)
Incidence with sepsis as high as 45% ( Cytokines ?).
AF in The ICU

Atrial Fibrillation: Cardiac Causes Hypertensive heart disease
Ischemic heart disease
Valvular heart disease
Rheumatic: mitral stenosis
Non-rheumatic: aortic stenosis, mitral regurgitation
Pericarditis
Cardiac tumors: atrial myxoma
Sick sinus syndrome
Cardiomyopathy
Hypertrophic
Idiopathic dilated (? cause vs. effect)
Post-open heart surgery
AF in The ICU

Atrial Fibrillation: Non-Cardiac Causes Pulmonary
COPD
Pneumonia
Pulmonary embolism
Metabolic
Thyroid disease: hyperthyroidism
Electrolyte disorder
Septicemia.
AF in The ICU

“Lone” Atrial Fibrillation Absence of identifiable cardiovascular,
pulmonary, or associated systemicdisease
Approximately 0.8 - 2.0% of patients with atrialfibrillation (Framingham Study).
In one series of patients undergoing electrical cardioversion, 10% had lone AF.
1 Brand FN. JAMA. 1985;254(24):3449-3453.2 Van Gelder IC. Am J Cardiol. 1991;68:41-46.
AF in The ICU
AF in The ICU
Most common arrhythmia requiring hospitalization.
Structural changes
• Left atrium and left atrial appendage enlargement.
• Reduced atrial contractility.
• Decrease in cardiac output (loss of AV synchrony and
rapid ventricular rate.)
• Histologic: cardiomyocyte degeneration.
• Increased propensity for clot formation.
Electrophysiologic background
Shortening of atrial refractory periods
Loss of normal adaptation of atrial refractoriness to
heart rate.
Longer duration of AF results in shorter AF intervals
“AF begets AF” (electric remodeling)
AF in The ICU
Management :
I) Rhythm control
Intravenous amiodarone (150 mg IV) in the
treatment of critically ill patients with recent-
onset atrial fibrillation, there are an increasing
number of reports highlighting occasional
serious acute pulmonary toxicity.
AF in The ICU
Ibutilide (1 mg IV; in the case of persisting
arrhythmia and body weight > 70 kg, has a
71% conversion rate with adjustment of
magnesium level and high normal K+ level.
AF in The ICU

II) Rate control :
According to the AFFIRM and the RACE studies
, Lower mortality and hospitalizations are
documented with rate control rather than
rhythm control.
AF in The ICU
Digoxin may be helpful for rate control, with an initial dose of 0.5 mg. After 30 minutes, 0.25 mg should be administered again.
verapamil (5 to 10 mg IV)
diltiazem (20 mg IV)
AF in The ICU
Beta-blockade
Propranolol (1 to 5 mg IV, additional infusion of 10 to 120 mgper day) and
Esmolol (500 µg/kg over 1 minute, followed
by a 4-minute maintenance infusion of 50 µg/kg/min
with further dose adjustment as necessary)
AF in The ICU
In one study done on critically ill ,60 patients
with atrial tachy-arrhythmias (atrial fibrillation
57 patients, atrial flutter 2 patients, atrial
tachycardia 1 patient)
The primary end-point was a >30% heart rate
reduction within 4 hours.
The secondary endpoint was a heart rate <120
beats/min
AF in The ICU

Patients were randomized to :
diltiazem (25 mg bolus followed by a
continuous infusion of 20 mg/h for 24 hours)
(group I),
amiodarone (300 mg bolus) (group II) or
amiodarone (300 mg bolus followed by 45
mg/h for 24 hours) (group III).
AF in The ICU

The primary endpoint was achieved in
70% of group I patients, 55% of patients in group II, and in 75% of patients in group III (P = 0.38).
In patients achieving heart rate control, diltiazem showed a significantly better rate reduction when compared with group II and III (P < 0.01
AF in The ICU

AF in The ICU

Atrial tachycardia
Defined as a supraventricular tachycardia (SVT)
that does not require the atrioventricular (AV)
junction, accessory pathways, or ventricular
tissue for initiation and maintenance of the
tachycardia. Its rate varies between 150-250
BPM.

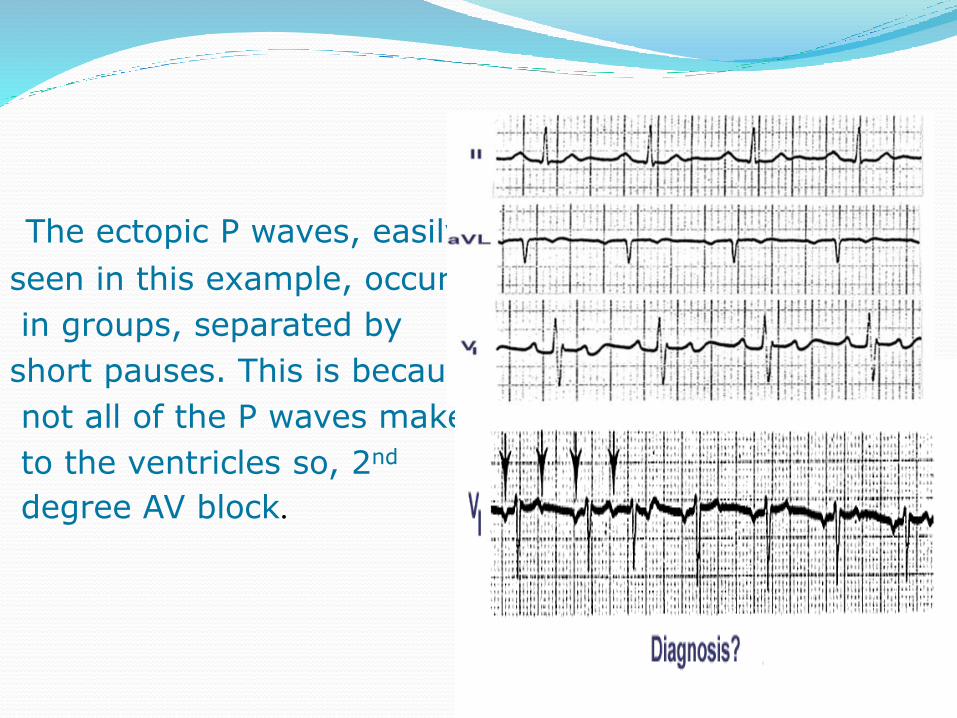
The ectopic P waves, easily
seen in this example, occur
in groups, separated by
short pauses. This is because
not all of the P waves make it
to the ventricles so, 2nd
degree AV block.

Diagnosis
The primary abnormality noted upon physical
examination is a rapid pulse rate. In most atrial
tachycardias this is regular. However, in rapid
atrial tachycardias with variable AV conduction
and in multifocal atrial tachycardia (MAT), the
pulse may be irregular.

Very Subtle Atrial Tachycardia With 2:1 Block-KH
Multifocal Atrial Tachycardia (MAT)
MAT often occurs in patients experiencing an
exacerbation of chronic obstructive pulmonary
disease, a pulmonary thromboembolism, an
exacerbation of congestive heart failure, or severe
illness especially under critical care with Inotropic
infusion or Digitalis toxicity. Abnormal thyroid
function should also be in the differential
diagnosis

ManagementCarotid sinus massage and adenosine do not
terminate the tachycardia even if they
produce a transient AV nodal block.
Electrical cardioversion is ineffective
(being equivalent to attempting electrical
cardioversion in a sinus tachycardia

Again Rate control with agents mentioned in AF
management.
However treating the primary pathology is the
main stay.
Unlike AF anticoagulation is not necessary.

Thanks






















![Bridgingancoagulana - Intensivistenopleidingintensivistenopleiding.nl/downloads-25/files/Bridging.pdf · x thrombosis critically x C] intensivistenopleidir NEJMoa1501035.pdfx Atrial](https://img.dokumen.tips/doc/110x75/5e220a8e3e04e84a3a609949/bridgingancoagulana-intensivistenopleidingin-x-thrombosis-critically-x-c-intensivistenopleidir.jpg)






