Embed Size (px)
Citation preview

Fulfilling the Legacy and Vision of Alan Magill: Malaria Delenda Est
Chris Plowe MD MPH FASTMHInstitute for Global Health, University of Maryland School of Medicine
Baltimore, Maryland USA
~~~Alan Magill Malaria Symposium
~~~WRAIR, Silver Spring, MD
23 June 2016



Malaria can be eliminated
COL John Boyd Coates, Jr., MC, USA http://history.amedd.army.mil/booksdocs/wwii/Malaria/default.htm

• Control – reduction of disease incidence and burden to the point where it is no longer a public health priority
• Elimination – interruption of transmission of the pathogen and a fall in disease incidence to zero in a defined geographical area
• Eradication – interruption of pathogen transmission worldwide & fall in disease incidence to zero
• Extinction – disappearance of the pathogen from the planet
Definitions

100 yearspre-eradication
Source:Global malaria control and eliminationWHO 2008

Eradication era1945 - 1977
Source:Global malaria control and eliminationWHO 2008

Control era1977 - 2007
Source:Global malaria control and eliminationWHO 2008

Shrinking the malaria map• 62 countries have
eliminated malaria• 96 countries still have
malaria• 35 countries now
actively committed to eliminating malaria
• 9 countries are close to elimination

Today’s tools for malaria control, elimination, eradication:
• LLIN = Long-lasting insecticide-treated nets• IRS = Indoor residual spraying (DDT)• IPT = Intermittent preventive treatment for pregnant women,
infants, children• ACT = Artemisinin-based combination therapy~~~ Tomorrow’s tools?~~~• SERCaP = Single Encounter Radical Cure & Prophylaxis
– (Targeted) Mass Drug Administration– Focal/Mass Screening and Treatment
• VIMT = Vaccines that interrupt malaria transmission• New surveillance tools?• Transgenic mosquitoes?• …?

Debate!

Current tools:Long-lasting insecticide-impregnated nets
WHO/S. Hollyman
C. Plowe

Elimination eradication

Can malaria be eradicated?Yes…
…eventually…with an end to poverty and strife.
and/orwith new and better tools that can be
implemented everywhere.

What has worked for eradicating other diseases?

Eradication programs• Failure
HookwormYellow feverYawsMalaria
• Success SmallpoxPolio (Americas)Measles (Americas)
• Near successPolioGuinea wormRinderpestRubella (Americas)
DA Henderson, malERA Zenith Week, March 2010

Eradication programs• Failure
HookwormYellow feverYawsMalaria
• Success SmallpoxPolio (Americas)Measles (Americas)
• Near successPolioGuinea wormRinderpestRubella (Americas)
DA Henderson, malERA Zenith Week, March 2010
Vaccines: Principal tool

Breman and Plowe J Inf Dis 2009Modified from PATH Malaria Vaccine Initiative
Malaria vaccines

Is RTS,S an elimination vaccine?



R A Seder et al. Science 2013;341:1359-1365
Published by AAAS
IV PfSPZ Vaccine had 100% protective efficacy in highest dose group

Snowden “The Conquest of Malaria” 2006
Malaria elimination in Italy 1900-1962
The logistical challenges are considerable…
Mali 2012

…but a frozen live sporozoite vaccine is already being delivered in liquid nitrogen in Africa
International Livestock Research Institute, Kenya
Theileria parva (East Coast Fever)


“This artemisinin resistance—is it popping, or is it jumping?”
Professor Pe Thet Khin, former Minister of Health, MyanmarApril 2014

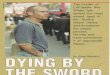
K13 molecular marker map Woodrow et al. Lancet Inf Dis 2015
A wave of artemisinin resistance?

Artemisinin resistance “paternity testing” using K13 molecular marker

Most common resistance mutation has both emerged independently (popped) and spread

K13 migration: Implications
• Many different K13 mutations arose independently on many different genetic backgrounds
• Several resistance mutations have spread between countries in the Greater Mekong Subregion (GMS)
• Based on this result, new WHO recommendation:
– Containment is not possible
– Elimination is imperative for the GMS

Malaria as a catalyst for social change

Washington DC August 2015

Surveillance & response:Stratification of malaria risk to guide
elimination interventions
• Myanmar NMCP: Malaria risk stratification at the township level is inadequate– Ecological risks of vector exposure, reported clinical
cases
• Goal: Microstratification of malaria risk at village level
• Identify sources and sinks of migrating parasites to guide elimination interventions?

Gene flow:Parasite migration patterns
• SNP chip: Genome-wide genotyping• Coalescent theory to estimate gene
flow magnitude and direction• 19 sites across Greater Mekong
Subregion
• Aim to identify sources, sinks, pathways of malaria transmission to target interventions
Chris Jacob PhD thesis

Molecular evolution methods may provide new tools for mapping contemporary parasite migration
• Next step: Move from regional to local mapping to identify sources and sinks of malaria transmission
• Useful for mapping transmission and spread patterns of other parasites?

Subclinical, submicroscopic malaria reservoir
Malaria elimination may require elimination of all parasitesDemanding more sensitive tools to detect and map low density malaria

New WHO recommendations:MDA is OK, but FSAT & MSAT need better diagnostic tests
http://www.who.int/malaria/publications/atoz/role-of-mda-for-malaria.pdf


Hunting for low density malaria
• Field scalable: No sample processing, no cold chain x 14 days• High throughput pipeline in Yangon: >20,000 samples since 2015• Concordant with high volume PCR from frozen venous blood• Now achieving same lower limit of detection from dried blood spots
• RDT: 100,000 parasites/mL; conventional PCR 1000-5000 parasites/mL)• Ultrasensitive low-volume Reverse Transcriptase PCR
– Sensitivity: 16 parasites/mL & can detect both Pf & Pv simultaneously
0.3mL finger prick blood in cap tube
+
Mix with DNA-RNA shield
Transport to labExtract DNA/RNA Ultrasensitive
qPCR
Adams et al. Malaria Journal 2015

Mapping subclinical malaria in Myanmar

Simply increasing access to diagnosis and treatment reduces malaria
• Village malaria workers
• Need for integration especially as burden falls
• Will this be enough to eliminate?
• Need tools to stratify and forecast malaria risk and target interventions

Alan Magill, February 2015Siem Reap, Cambodia


Malaria
delenda est

Thanks to
Shannon Takala-HarrisonChris JacobJason BaileyAndrew PikeAlexa MachikisSonia AgarwalAndrea BerryMark TravassosMatthew AdamsNicole Eddington JohnsonGillian MbamboBiraj ShresthaKayvan ZainabadiMyaing Nyunt
Institute for Genome SciencesUniversity of MarylandJoana SilvaAmol ShettyTim O’Connor
Department of Geographical SciencesUniversity of Maryland College ParkDemian RybockKathleen StewartTatiana Loboda
Department of Medical ResearchMyanmar Ministry of HealthZayar HanHnin Hnin Wai LwinKay Thwe HanMyat Phone KyawKyaw Zin Thant
Defence Services Military AcademyMyanmar Ministry of DefenceKhine Zaw OoYe Myat KyawTin Maung Hlaing
National Institute of Parasitic DiseasesChinese CDCHuang FangXiao-Nong Zhou
Global Malaria ProgramWorld Health OrganizationPascal Ringwald
Roche Innovation TechnologyJohn Tan
TRAC, ARC3 & ARCE investigatorsArjen Dondorp, Mark Fukuda, Francois Nosten, Harald Noedl, Mallika Imwong, Delia Bethell, Youry Se, Chanthap Lon, Stuart Tyner, David L Saunders, Charlotte Lanteri, Frederic Ariey, Aung Pyae Phyo, Peter Starzengruber, Hans-Peter Fuehrer, Paul Swododa, Nicholas White, Odile Mercereau-Puijalon, Didier Menard, Paul Newton, Maniphone Khanthavong, Bouasy Hongvanthong, Wasif A. Khan