1. Recent Advances in the Pathophysiology of Asthma Desmond M.
Murphy and Paul M. OByrne Chest 2010;137;1417-1426 DOI
10.1378/chest.09-1895 The online version of this article, along
with updated information and services can be found online on the
World Wide Web at:
http://chestjournal.chestpubs.org/content/137/6/1417.full.html
Chest is the official journal of the American College of Chest
Physicians. It has been published monthly since 1935.
Copyright2010by the American College of Chest Physicians, 3300
Dundee Road, Northbrook, IL 60062. All rights reserved. No part of
this article or PDF may be reproduced or distributed without the
prior written permission of the copyright holder.
(http://chestjournal.chestpubs.org/site/misc/reprints.xhtml)
ISSN:0012-3692Downloaded from chestjournal.chestpubs.org by guest
on July 22, 2011 2010 American College of Chest Physicians
2. CHEST Recent Advances in Chest Medicine Recent Advances in
the Pathophysiology of Asthma Desmond M. Murphy, MB, PhD; and Paul
M. OByrne, MB, FCCP There has been an increased understanding, over
the past 2 decades, that asthma is a chronic, immunologically
mediated condition with a disturbance of the normal airway repair
mechanism, which results in inammatory changes and airway
remodeling. The airway inammation and remodeling together likely
explain the clinical manifestations of asthma. The mechanisms by
which the external environmental cues, together with the complex
genetic actions, propagate the inammatory process that characterize
asthma are beginning to be understood. There is also an evolving
awareness of the active participation of structural elements, such
as the airway epithe- lium, airway smooth muscle, and endothelium,
in this process. In tandem with this has come the realization that
inammatory cells respond in a coordinated, albeit dysfunctional
manner, via an array of complex signaling pathways that facilitate
communication between these cells; these structural elements within
the lung and the bone marrow serve as reservoirs for and the source
of inammatory cells and their precursors. Although often viewed as
separate mechanistic enti- ties, so-called innate and acquired
immunity often overlap in the propagation of the asthmatic
response. This review examines the newer information on the
pathophysiologic characteristics of asthma and focuses on papers
published over the past 3 years that have helped to improve current
levels of understanding. CHEST 2010; 137(6):14171426 Abbreviations:
CCR 5 chemokine receptor; IL 5 interleukin; NK 5 natural killer;
TGF 5 transforming growth factor; Th 5 T-helper; TLR 5 toll-like
receptor; TNF 5 tumor necrosis factor; Treg 5 T-regulatory; VEGF 5
vascular endothe- lial growth factorAsthmaclinically awith
repeated, variable, episodic fests remains major health-care issue.
It mani- cytokines such as interleukin (IL)-4, IL-5, and IL-13, the
so-called Th2 cytokine milieu. These cytokinesattacks of
breathlessness, cough, and wheeze occur- stimulate mast cells,
cause eosinophilia, promote leu-ring secondary to
bronchoconstriction in the setting kocytosis, and enhance B-cell
IgE production, andof airway hyperresponsiveness and mucous
hyperse- may also participate in the characteristic airwaycretion.
Clinically, the disease may be divided into remodeling of asthma.
However, for an individual toallergic and nonallergic asthma,
distinguished by the develop an asthmatic phenotype appears to
requirepresence or absence of IgE antibodies to common the
combination of both exposure to appropriateenvironmental allergens.
However, in both forms stimuli and a genetic predisposition.1,2of
the disease, the airway is inltrated by T-helper The last 3 decades
have provided vast quantities(Th) cells, which predominantly
secrete characteristic of research affording signicant insights
into the pathophysiologic characteristics of this complex
entity.Manuscript received August 10, 2009; revision accepted
November In this article, we review progress, over the past 3
years,16, 2009.Afliations: From the Firestone Institute for
Respiratory Health, that has augmented the level of understanding
of theSt Josephs Healthcare; and the Department of Medicine,
pathophysiologic characteristics of asthma.McMaster University,
Hamilton, ON, Canada.Correspondence to: Paul OByrne, MB, FCCP, HSC
3W10,McMaster University, 1200 Main St W, Hamilton, ON, Canada,
Innate and Acquired ImmuneL8N 3Z5; e-mail: [email protected]
Mechanisms in Asthma 2010 American College of Chest Physicians.
Reproductionof this article is prohibited without written
permission from the The trigger factors precipitating acute
asthmatic exa-American College of Chest Physicians
(www.chestpubs.org/site/misc/reprints.xhtml). cerbations are, for
the most part, either environmen-DOI: 10.1378/chest.09-1895 tal
allergens or viruses, suggesting that immunologicwww.chestpubs.org
CHEST / 137 / 6 / JUNE, 2010 1417 Downloaded from
chestjournal.chestpubs.org by guest on July 22, 2011 2010 American
College of Chest Physicians
3. responses viewed traditionally as either innate or and the
host immune response. Airway inammationacquired are in fact
intertwined. The hygiene in asthma reects a distortion of this
balance andhypothesis for asthma pathogenesis contends that is
orchestrated through complex interplay betweenmicrobiologic factors
may also be inherently involved multiple effector and target
components.in the suppression of the asthmatic phenotype,
withchildhood exposure to microbiologic stimuli confer- Mast
Cellsring a protective effect against the development of Mast cells
are critical in mediating the acuteatopy.3 The proposed explanation
for this effect is that response in asthma. While classically, mast
cell acti-infection early in life stimulates a Th1 immunologic
vation occurs following the binding of antigens toresponse
(characterized by the release of cytokines FcR1-bound,
antigen-specic IgE, they may also besuch as interferon-g), rather
than the Th2 response activated through other mechanisms, including
stim-(characterized by cytokines such as IL-4, IL-5, IL-13, ulation
of complement receptors, FcgR1, and viaand tumor necrosis factor
[TNF]-a) associated with TLRs.10 Other novel mechanisms of mast
cell activa-allergy and asthma. A persons initial exposure to tion,
independent of IgE, are via the protein S100A12microorganisms
occurs in the birth canal during normal and the receptors
CD200R3/CD200R, whereasvaginal delivery. A Dutch birth cohort study
suggests IL-33, a member of the IL-1 cytokine family, hasan
increased risk of asthma at 8 years of age in chil- demonstrated
the ability to activate mast cells, evendren delivered by caesarean
section and therefore in the absence of FcR1 stimulation.11-15lends
further credence to this hypothesis.4 Further TNF-a is preformed in
mast cells and released asstudies suggest that a rural upbringing
has a protective part of the asthmatic airway response. In animal
andeffect on later development of allergy.3,5 It has been ex vivo
models, mast-cell-derived TNF-a promotessuggested that the
consumption of farm milk may be antigen- and Th17 cell-dependant
neutrophilia afterprotective against subsequent atopy, with this
protec- allergenic stimulation and induces dendritic celltive
effect linked to CD14, thereby implicating toll- migration.16,17 In
murine culture experiments, mast cellslike receptor (TLR)
recognition and innate immune induce CD41 T-cell migration, but
down-regulateinvolvement in the evolution of an atopic phenotype.6
FcR1 expression only in Treg cells, while activated The main
function of TLRs is in the recognition of Treg cells suppress mast
cell FcR1 expression. Thisinfectious agents to facilitate an
appropriate host suggests bidirectional communication between
mastimmunologic response. Advocates of the hygiene cells and Treg
cells in modulating IgE-mediatedhypothesis originally believed that
microbiologic responses.18 A role for mast cells in antigen
presenta-stimulation of TLRs modied an individuals suscep- tion is
also suggested by the recent observation thattibility to asthma by
promoting a Th1 rather than a mast cells stimulated by IgE-specic
antigen undergoTh2 lymphocytic response to an allergen.3 However,
FcR1 cross-linking that enhances apoptosis. Thesewith the discovery
of other T-cell subtypes and dead mast cells become ingested by
dendritic cells,increasing evidence supporting pivotal roles for
and this incorporated antigen helps propagate ongoingT-regulatory
(Treg) and Th17 cells, the Th1/Th2 CD41 response.19paradigm of
infection/atopy appears to oversimplify Whereas mast cells are
generally considered proin-the complex mechanisms involved.
ammatory and mediators of tissue destruction, Recent studies may
help explain the similarity in they may conversely help limit
airway damage.20response evoked by allergens and microbes in the
Mast-cell-derived tryptase can cleave IgE, therebyasthmatic airway.
The house mite allergen Der p 2 has preventing further mast cell
activation and plau-been shown to have similar structural
characteristics sibly helping to contain the allergic
response.21,22to MD-2, an integral component of the TLR4/CD14/
Disappointingly, a recent human study examiningMD-2 transmembrane
receptor and TLR signaling.7,8 a potential role for therapeutic
intervention withAlso, Trompette et al9 have provided in vitro and
the monoclonal antibody to TNF-a, golimumab, inin vivo evidence of
functional similarity between Der severe, persistent asthma was
abandoned because ofp 2 and MD-2. These results place TLRs in an
ideal an unfavorable risk-benet prole.23position to coordinate
responses traditionally viewedseparately, as either innate or
adaptive immunologic Basophilsreactions that typify the asthmatic
response. Basophils have a crucial role in initiating allergic
Effector Cells of Inflammation inammation through the binding of
antigen-specic and Remodeling in Asthma IgE antibodies at the
FcR1.24 Basophils also drive Th2 cell differentiation of activated
naive CD41 T cells via In the healthy human airway there is
normally a production of IL-4 and direct cell-cell contact.25
Murinene balance between immune cells, the epithelium, studies show
that following activation, basophils migrate1418 Recent Advances in
Chest Medicine Downloaded from chestjournal.chestpubs.org by guest
on July 22, 2011 2010 American College of Chest Physicians
4. in small numbers to adjacent lymph nodes. Using a initiating
immune response against airborne antigen.basophil FcR1-specic
monoclonal antibody, it has Hence, dendritic cells may dictate the
subsequentbeen demonstrated that the presence of basophils but
T-cell response. Two major subsets of dendritic cellsnot mast cells
is an absolute requirement for Th2 cell have been described, based
on CD11c expression.differentiation.26 Basophils also increase
humoral Myeloid (CD11c1) dendritic cells are proinamma-immune
responses on repeat antigenic exposure in the tory, critical to
both Th2 sensitization and the second-presence of activated CD41
cells through the release of ary immune response, and typically
produce IL-12.IL-4 and IL-6, which provide support for B-cell
prolif- In contrast, plasmacytoid (CD11c2) dendritic cellseration
and antibody generation.27 play a role in the induction of
tolerance, preventing Mice lacking the Fc receptor for IgG FcgR
res- inammatory responses to harmless antigen, andpond to IL-3 in
terms of normal development and mainly produce interferon-g (Table
1). Plasmacytoidproliferation but have defective IL-4 (and also
IL-6) dendritic cells turn over peptide-major
histocompat-production and impaired ability to stimulate Th2
ibility complex class 2 complexes when activated,
withdifferentiation.28 In culture, basophils themselves the result
that they are inefcient at presenting exog-possess the ability to
release IL-3 following FcR1 enous antigen but useful at presenting
self-antigenactivation, and this IL-3 promotes IL-13 release, sug-
and viral antigen in a continuous manner followinggesting an
autocrine function of IL-3 in upregulating activation.30 Therefore,
in the regulation of allergythe basophilic response.29 and asthma,
plasmacytoid and myeloid dendritic cells would appear to have
opposing/balancing roles.Dendritic Cells T Lymphocytes Pulmonary
dendritic cells are potent antigen-presenting cells with the
capability to rapidly migrate A paradigm emerged whereby the
fundamentalto draining lymph nodes, suggesting an innate role in
problem in asthma was believed to be disturbance of Table 1Summary
of the Key Mediators of Asthmatic Inammatory ResponseMediator
Potential Sources Potential Key ActionsIL-4 Mast cells, basophils
Immunoglobulin class switching of B cells from IgG to IgE;
differentiation of Th2 cells; maturation of dendritic cellsIL-5
Mast cells Differentiation and enhanced survival of
eosinophilsIL-13 Mast cells, basophils Immunoglobulin class
switching of B cells from IgG to IgE; induction of inammatory
cytokine release from epithelial and other structural cellsTNF-a
Mast cells, alveolar macrophages, T cells, Induction of
proinammatory cytokine release from structural cells; epithelial
cells, airway smooth muscle promotion of Th17-induced neutrophilia;
enhancement of dendritic cell migration; induction of CD4 T-cell
migration; antigen presentation; modulation of Treg cellsIL-6
Structural cells, dendritic cells, basophils Aids Th17 expansion
and developmentIL-17A Th17 cells Promote neutrophilia via induction
of proinammatory cytokine and chemokine release from structural
cellsIL-33 Structural cells such as epithelial cells Promote
differentiation to Th2 cells; chemoattractant for Th2 cells;
enhance survival of, and cytokine production by, mast cellsSCF
Structural cells, mast cells, and eosinophils Growth factor and
chemoattractant for mast cellsTGF-b Eosinophils, mast cells, and
macrophages Proliferation of broblasts; possibly induction of EMT;
development of immune tolerance via promotion of a Treg response;
in combination with IL-6, may promote a Th17 responseVEGF
Structural cells, eosinophils Angiogenic promotion of vascular
remodelingTSLP Epithelial cells Promotion of a Th2 response;
activation of dendritic cells and mast cellsNeurotrophin Epithelial
cells, broblasts, airway smooth Enhanced airway eosinophilia; mast
cell recruitment and activation; (NGF and BDNF) muscle cells,
macrophages, mast cells, increased airway hyperresponsiveness;
promotion of airway eosinophils, and lymphocytes inammatory
responseLipoxins Derived at mucosal surface from interaction
Attenuate bronchial hyperresponsiveness and promote resolution
between neutrophils and primarily epithelial of inammation cells,
but also platelets, endothelial cells, leukocytes, and
broblastsResolvins Interaction between neutrophils and Enhance
resolution of airway inammation and attenuate bronchial structural
cells hyperresponsivenessProtectins Interaction between neutrophils
and Decrease allergic airway inammation and airway
hyperresponsiveness structural cellsBDNF 5 brain derived
neurotrophic factor; EMT 5 epithelial mysenchymal transition; IL 5
interleukin; NGF 5 nerve growth factor; SCF 5 stemcell factor; TGF
5 transforming growth factor; Th 5 T-helper; TNF 5 tumor necrosis
factor; Treg 5 T-regulatory; TSLP 5 thymic stromal
lymphopoietin;VEGF 5 vascular endothelial growth
factor.www.chestpubs.org CHEST / 137 / 6 / JUNE, 2010 1419
Downloaded from chestjournal.chestpubs.org by guest on July 22,
2011 2010 American College of Chest Physicians
5. the normal Th1/Th2 balance. Although elements ofthis
hypothesis remain useful, the emerging roles forother T-cell
subtypes in asthma suggest that it is toosimplistic. Th17 cells are
a distinct population ofCD41 cells that produce IL-17A, IL-17F,
IL-22,TNF-a, and IL-21, and express the transcription fac-tor
RORgt.31 Recently, Th17 cells were isolated frombiopsy samples
obtained from patients with asthma.32 IL-17 induces the release of
a range of proinam-matory cytokines and chemokines from a variety
ofcell types.31 It is linked to the development of
airwayneutrophilia, and its presence in the asthmatic
airwaycorrelates with increased disease severity. In murinemodels
of asthma, IL-23 and Th17 cells enhanceantigen-induced airway
recruitment of both eosino-phils and neutrophils, while
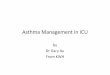
mast-cell-derived TNF Figure 1. Kaplan-Meier analysis of patients
without an asthmahas been shown to illicit a Th17-mediated airway
neu- exacerbation during a study by Nair et al47 examining the
effect of the monoclonal antibody to interleukin-5, mepolizumab,
introphilic response following antigen challenge.16,33 patients
with steroid-dependant asthma The median time to rst Treg cells
play roles in the determination of self- exacerbation was 20 weeks
in the mepolizumab group vs 12 weekstolerance and the regulation of
immune responses. in the placebo group (P 5 .003).Th17 and Treg
cells have opposing actions, being inthe main proinammatory and
antiinammatory, phenotype or the clinical manifestations of
asthma.respectively. Experimental data suggest that retinoic
Despite this, therapies that reduce sputum eosino-acid suppresses
Th17 cell differentiation while pro- philia are effective in both
forms of asthma.42moting Treg expansion.34,35 Further studies have
IL-5 has a key role in the modulation of eosinophilbrought this a
step further and demonstrated recip- differentiation and the
promotion of eosinophil sur-rocal generation of Treg and Th17
cells, with the vival. Hence, targeting IL-5 would seem a
logicalpresence of transforming growth factor (TGF)-b in
therapeutic strategy for allergic asthma. Indeed, anti-isolation
favoring a Treg response, while TGF-b in IL-5 therapy has
demonstrated clinical efcacy incombination with IL-6 favored a Th17
response.35,36 hypereosinophilic syndromes.43 In patients with
asthma,A similar reciprocal relationship between Th17 and a
monoclonal IL-5 antibody, while markedly reduc-Treg cells,
dependant on the relative levels of RORgt ing blood eosinophils,
only partially abrogated theand Foxp3, with Foxp3 attenuating the
function of pulmonary eosinophilic response and,
subsequently,RORgt, has also been shown.37 had minimal impact on
clinical outcomes.44,45 More Invariant natural killer (NK) T cells
produce both recent studies in patients with refractory,
eosinophilicTh1 and Th2 cytokines in large quantities and therefore
asthma have demonstrated the ability of an anti-IL-5enhance the
function of dendritic cells, NK-T cells, monoclonal antibody
(mepolizumab) to reduce bothB cells, and conventional T-cell
subsets. Initial studies blood and sputum eosinophil levels, reduce
exacer-suggested a potential role for invariant NK-T cells in
bations, and facilitate a reduction in oral corticosteroidthe
pathophysiologic development of asthma.38 Later dose (Fig 1).46,47
These results indicate that, at least instudies have, however,
disputed this.39,40 Furthermore, a subset of patients with asthma,
eosinophils areit has also been reported that NK-T cells alone or
in critical effector cells in persistent asthma and
severecombination with memory CD81 T cells are insuf-
exacerbations.cient to induce allergic airway inammation in miceand
their presence is not a prerequisite for its develop-
Neutrophilsment.41 The nature of the part played by invariant
NK-Tcells has therefore yet to be conclusively illustrated. In
acute, severe exacerbations of asthma, there are increased
eosinophils and neutrophils within the air-Eosinophils way, with
the increase in neutrophils proportionately higher than that of
eosinophils.48 Inhaled corticoster- The precise role eosinophils
play in the pathophys- oids reduce airway eosinophils, but increase
airwayiologic causes of asthma remains controversial. Asthma
neutrophils and increase the expression of the neu-can be divided
into eosinophilic and noneosinophilic trophil chemoattractant IL-8,
which is associatedasthma depending on the presence or absence of
air- with loss of asthma control.49 There has been long-way
eosinophils. The inference from this is that standing interest in
the observed differences andeosinophils are not a prerequisite for
the asthmatic similarities between the asthmatic airway and
that1420 Recent Advances in Chest Medicine Downloaded from
chestjournal.chestpubs.org by guest on July 22, 2011 2010 American
College of Chest Physicians
6. described in COPD. A recently published study has ticular in
patients with steroid-resistant asthma.64described elevated levels
of granulocyte-macrophage Particulate matter has also been shown to
induce thecolony-stimulating factor in the sputum of patients
release of proinammatory mediators and inducewith moderate to
severe asthma and also in patients cycloxygenase-2 expression in
human airway epithe-with COPD, regardless of its severity.50
Therefore, it lial cells.65 In addition to acting as a potent
source ofappears likely that an increase in airway neutrophils
proinammatory cytokines, epithelial cells possesshas important
clinical implications in asthma.51 the ability to present
self-antigen, with resultant effects on the regulation of CD41
T-cell function, including the induction of Foxp3 Treg cells, thus
pro- The Regulation of Inflammatory moting immune tolerance.66 Cell
Production in Asthma The process of airway remodeling involves
altera- tions to the various components of airway structure, The
bone marrow represents a vast source of with broproliferation, inux
of myobroblasts, col-potential effector cells with the ability to
affect lagen deposition, hypertrophy of airway smooth
mus-inammation.52 While the bone marrow may act as a cle, and
reticular basement membrane thickeningreservoir for mature
granulocytes, it is increasingly typical. Remodeling occurs in
asthma, and indeed,recognized that hemopoietic progenitor stem
cells parameters associated with remodeling are increasedmay be
released from the bone marrow and recruited in severe disease, with
the airway mucosa of patientsto sites of injury, including the
lung, and participate with severe asthma displaying evidence of
increasedin the inammatory and the reparative processes.53
proliferation of epithelium and increased thickening Allergen
inhalation challenge experiments impli- of the epithelium and
lamina reticularis.60 The para-cate upregulation of the chemokine
receptor (CCR) 3 digm of remodeling as a chronic, dysfunctional,
repairin facilitating the egress of these progenitors from the
response to ongoing inammation has, however,bone marrow. Eotaxin-1
up-regulates CCR3 on recently been challenged. While studies
demonstrateCD341 cells, with the resultant increased release of a
progressive loss of lung function associated withthese cells into
the circulation, while pharmacologic severe asthma
exacerbations,67,68 it has been recognizeddown-regulation of CCR3
attenuates sputum eosino- that remodeling may occur very early in
asthma andphilia in response to allergen inhalation in patients may
in some cases even predate clinical symptoms.with mild to moderate
asthma.54,55 Down-regulation Airway biopsy studies in children
suggest that patho-of CXCR4 on bone marrow CD341 cells and reduced
logic changes such as epithelial loss, basement
mem-stromal-cell-derived factor 1a may further promote brane
thickening, and angiogenesis occur early in theprogenitor cell efux
from the bone marrow following asthmatic airway.59,69 Although
there exist progenitorallergen challenge, while attenuation of
expression of cell types within the bronchial epithelium with
thethe adhesion molecule b1-integrin on progenitor cells capacity
for renewal following injury, repair pathwaysmay aid their release
into the circulation.56,57 are likely dysfunctional in asthma.70 In
the asthmatic airway, there are increased num- Airway Structural
Cells in Asthma bers of subepithelial myobroblasts, and allergen
challenge in people with asthma leads to increased Traditionally
viewed as a passive defensive barrier accumulation of
myofibroblasts in the airwayto pathogenic insult, the airway
epithelium is now mucosa.58,71 The precise source of these
broblasts inaccorded a pivotal position in orchestrating the host
airway disease remains a topical source of debate.inammatory
response in airway remodeling and Fibroblastic inltration of the
lung may plausibly bebroproliferation.58 Multiple asthma biopsy
studies secondary to the recruitment of circulating bone-have
demonstrated airway epithelial abnormality, marrow-derived
progenitors termed brocytes to theand the epithelium, placed at the
interface between airway and to the proliferation and expansion of
resi-the external environment and the host, appears to be dent
broblasts, or possibly, epithelial cells mayboth a site of action
and of reaction within the asth- undergo phenotypic change to
effector broblastsmatic inammatory cascade.58-60 through a process
termed epithelial-mesenchymal The airway epithelium is known to be
a major transition. Airway biopsies have demonstrated thesource of
proinammatory mediators. Recent examples increased presence of
brocytes in the airway smoothinclude thymic stromal lymphopoietin,
an epithelial- muscle bundle of patients with asthma of
varyingderived cytokine expressed in the asthmatic airway, severity
compared with control subjects. Further-which has been shown to
activate dendritic cells, more, in an ex vivo model, airway smooth
musclepromote Th2 responses, and activate mast cells.61-63 cells
promoted brocyte migration.72 A murine modelEndothelin-1 is also
increased in airway epithelial of chronic allergenic-stimulated
airway remodelingbiopsies in patients with severe asthma and in
par- has revealed a crucial role for stem cell factor
andwww.chestpubs.org CHEST / 137 / 6 / JUNE, 2010 1421 Downloaded
from chestjournal.chestpubs.org by guest on July 22, 2011 2010
American College of Chest Physicians
7. IL-31 in promoting the inux of bone-marrow-derived kinase,
with further experiments in rat models sug-broblast progenitors to
the lung.73 Recently, primary gesting that this may be associated
with the potentialairway epithelial cells derived from subjects
with to increase maximal ow and thereby contribute to theasthma
demonstrated increased susceptibility to TGF- airway
hyperresponsiveness seen in asthma.82 Airwayb-induced epithelial
mesenchymal transition than smooth muscle cells can also be induced
to secretethose derived from normal subjects.74 mediators that may
promote mast cell chemotaxis, Fibroblast culture, animal, and human
studies sup- proliferation, and survival, while cell-cell
interactionport the ability of leukotrienes to promote airway
between airway smooth muscle cells and mast cellsremodeling.75-77
Bronchial epithelial cell experiments enhances activated
complement-induced mast cellhave demonstrated a role for TLR
signaling in the degranulation.83-85 Interestingly, human lung mast
cellsactivation of epidermal growth factor receptor, sug- will
migrate toward Th2 cytokine-stimulated airwaygesting a role for
TLRs in potentiating remodeling.78 smooth muscle cells from
subjects with asthma,Histamine is capable of inducing the
transition from but not subjects without asthma, while
supernatantsbroblasts to myobroblasts, as measured by a-smooth
obtained from airway smooth muscle cell cultures ofmuscle actin
expression, and can, in addition, induce subjects without asthma
inhibit the chemotacticconnective-tissue-growth-factor expression
in bro- action of asthmatic airway smooth muscle cells.86blasts,
suggesting the ability to participate in the pro- In a recent study
examining differences betweencess of remodeling.79,80 chronic
persistent and intermittent persistent Airway smooth muscle mass is
increased in the asthma, endobronchial biopsy specimens
showedasthmatic airway.81 Asthmatic airway smooth muscle increased
a-smooth muscle actin immunoperoxidaseshows increased expression of
the fast myosin heavy staining in samples obtained from subjects
withchain isoform transgelin, as well as myosin light chain chronic
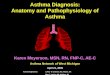
persistent asthma. There was also an increased Figure 2. The
pathophysiologic mechanism of asthma involves a coordinated, albeit
dysfunctional, multisystem response to airway stimulation,
involving the airway epithelium, airway smooth muscle, circulatory
system, regional lymph nodes, and the bone marrow, with these
elements in tandem with effector inammatory cells such as dendritic
cells, mast cells, T cells, and eosinophils, as well as cytok- ines
and chemokines propagating the host inammatory response. The airway
epithelium appears to be inherently abnormal. Over time, the
epithelium, smooth muscle, and vasculature undergo structural
changes termed remodeling. The regional lymph nodes serve as
stations to facilitate a specic immune response, while the bone
marrow serves as a source of both effector inammatory cells and
brocytes, which contribute to airway inammation and remodeling,
respectively. DC 5 dendritic cell; MC 5 mast cell; Th 5 T helper;
TLR 5 toll-like receptor.1422 Recent Advances in Chest Medicine
Downloaded from chestjournal.chestpubs.org by guest on July 22,
2011 2010 American College of Chest Physicians
8. proportion of both neutrophils and eosinophils in
manifestations of the disease, particularly in the devel-sputum
obtained from this group.87 opment of severe exacerbations. The
epithelium, The angiogenic changes associated with asthma smooth
muscle, and vascular and neuronal elements ofmay also occur early
in the pathophysiologic develop- the asthmatic lung also show
evidence of dysfunction.ment of the disease (Fig 2).59 Airway
smooth muscle While these structural components undergo
consider-cells from subjects with asthma but not healthy sub- able
architectural disturbance through remodeling,jects can promote in
vitro angiogenesis.88 BAL uid they additionally act as a potent
source of critical effec-obtained from patients with asthma has
been shown tor cells within the asthmatic airway.to possess a
proangiogenic effect, which appears tobe mediated through the
actions of vascular endothe-lial growth factor (VEGF), while
further studies of Acknowledgmentsthe asthmatic airway demonstrate
increased vascular- Financial/nonnancial disclosures: The authors
have reportedity and higher levels of VEGF, and potentially impli-
to CHEST the following conicts of interest: Dr Murphy is a past
recipient of an European Respiratory Society fellowship. Dr
OByrnecate mast cells as a signicant source of VEGF.89-92 is on
advisory boards for AstraZeneca, GlaxoSmithKline, Topigen,However,
increased vascularity and higher VEGF Wyeth, and Schering-Plough.
He has received speakers honorialevels exist both in patients with
asthma and patients from AstraZeneca and GlaxoSmithKline, and has
received research support from AstraZeneca, GlaxoSmithKline,
Merck,with eosinophilic bronchitis but without asthma, Wyeth,
Schering-Plough, and Alexion.implying that vascular remodeling may
not directlyinuence airway hyperresponsiveness.93 Studies point to
an interactive process between the Referencesimmunologic and
neuronal systems in the propaga- 1. Kabesch M, Schedel M, Carr D,
et al. IL-4/IL-13 pathwaytion of asthmatic response. Murine models
of asthma genetics strongly inuence serum IgE levels and
childhoodhave shown that the communicative process between asthma.
J Allergy Clin Immunol. 2006;117(2):269-274. 2. Loza MJ, Chang BL.
Association between Q551R IL4Rthe two systems may be linked via the
ion channel genetic variants and atopic asthma risk demonstrated
byTRPA1.94 In human studies, increased levels of brain-
meta-analysis. J Allergy Clin Immunol. 2007;120(3):578-585.derived
neurotrophic factor have been associated with 3. von Hertzen L,
Haahtela T. Disconnection of man and theloss of control in patients
with mild allergic asthma.95 soil: reason for the asthma and atopy
epidemic? J Allergy Clin Immunol. 2006;117(2):334-344. 4. Roduit C,
Scholtens S, de Jongste JC, et al. Asthma at 8 years of age in
children born by caesarean section. Thorax. 2009; Endogenous
Antiinflammatory Mediators 64(2):107-113. 5. Debarry J, Garn H,
Hanuszkiewicz A, et al. Acinetobacter Much of this article and
indeed research to date has lwofi and Lactococcus lactis strains
isolated from farmfocused on proinammation, broproliferation, and
cowsheds possess strong allergy-protective properties. J Allergythe
propagation of the remodeling response in asthma. Clin Immunol.
2007;119(6):1514-1521.There has, however, been recent interest in
the poten- 6. Bieli C, Eder W, Frei R, et al; PARSIFAL study group.
A poly- morphism in CD14 modies the effect of farm milk
consump-tial role of endogenous antiinammatory compounds tion on
allergic diseases and CD14 gene expression. J Allergyin attenuating
the asthmatic response. Culture models Clin Immunol.
2007;120(6):1308-1315.have suggested a role for lipoxins,
antiinammatory 7. Kim HM, Park BS, Kim JI, et al. Crystal structure
of theeicosanoids synthesized at a local level in response to
TLR4-MD-2 complex with bound endotoxin antagonistinammation, in
possibly inhibiting the actions of Eritoran. Cell.
2007;130(5):906-917. 8. Ohto U, Fukase K, Miyake K, Satow Y.
Crystal structures ofeosinophils.96 Recent studies point to roles
for addi- human MD-2 and its complex with antiendotoxic lipid
IVa.tional, novel, endogenous, lipid-derived, antiinam- Science.
2007;316(5831):1632-1634.matory compounds such as the protectins
and resolvins 9. Trompette A, Divanovic S, Visintin A, et al.
Allergenicityin resolution of human airway inammation.97,98 While
resulting from functional mimicry of a toll-like receptor
com-preliminary, animal models have demonstrated plau- plex
protein. Nature. 2009;457(7229):585-588. 10. Nigo YI, Yamashita M,
Hirahara K, et al. Regulation of aller-sible roles in asthma, but
these results have yet to be gic airway inammation through
toll-like receptor 4-mediatedfully translated into human studies.98
modification of mast cell function. Proc Natl Acad Sci U S A.
2006;103(7):2286-2291. 11. Yang Z, Yan WX, Cai H, et al. S100A12
provokes mast cell acti- Conclusions vation: a potential
amplication pathway in asthma and innate immunity. J Allergy Clin
Immunol. 2007;119(1):106-114. Asthma is a complex, coordinated,
multisystem, mul- 12. Kojima T, Obata K, Mukai K, et al. Mast cells
and basophils areticellular, inammatory disorder. The development
of selectively activated in vitro and in vivo through CD200R3asthma
requires an interaction between the environ- in an IgE-independent
manner. J Immunol. 2007;179(10): 7093-7100.ment and genetic
susceptibility. Recent studies have 13. Ho LH, Ohno T, Oboki K, et
al. IL-33 induces IL-13 produc-highlighted important interactions
between the innate tion by mouse mast cells independently of
IgE-FcepsilonRIand acquired immune system in some of the clinical
signals. J Leukoc Biol. 2007;82(6):1481-1490.www.chestpubs.org
CHEST / 137 / 6 / JUNE, 2010 1423 Downloaded from
chestjournal.chestpubs.org by guest on July 22, 2011 2010 American
College of Chest Physicians
9. 14. Iikura M, Suto H, Kajiwara N, et al. IL-33 can promote
sur- 35. Xiao S, Jin H, Korn T, et al. Retinoic acid increases
Foxp3+ vival, adhesion and cytokine production in human mast cells.
regulatory T cells and inhibits development of Th17 cells by Lab
Invest. 2007;87(10):971-978. enhancing TGF-beta-driven Smad3
signaling and inhibiting15. Allakhverdi Z, Smith DE, Comeau MR,
Delespesse G. Cutting IL-6 and IL-23 receptor expression. J
Immunol. 2008;181(4): edge: the ST2 ligand IL-33 potently activates
and drives 2277-2284. maturation of human mast cells . J Immunol.
2007;179( 4): 36. Bettelli E, Carrier Y, Gao W, et al. Reciprocal
developmental 2051-2054. pathways for the generation of pathogenic
effector TH17 and16. Nakae S, Suto H, Berry GJ, Galli SJ. Mast
cell-derived TNF regulatory T cells. Nature.
2006;441(7090):235-238. can promote Th17 cell-dependent neutrophil
recruitment in 37. Zhou L, Lopes JE, Chong MM, et al.
TGF-beta-induced ovalbumin-challenged OTII mice. Blood.
2007;109(9):3640-3648. Foxp3 inhibits T(H)17 cell differentiation
by antagonizing17. Suto H, Nakae S, Kakurai M, Sedgwick JD, Tsai M,
Galli SJ. RORgammat function. Nature. 2008;453(7192):236-240. Mast
cell-associated TNF promotes dendritic cell migration. 38. Akbari
O, Faul JL, Hoyte EG, et al. CD41 invariant T-cell- J Immunol.
2006;176(7):4102-4112. receptor1 natural killer T cells in
bronchial asthma. N Engl J18. Kashyap M, Thornton AM, Norton SK, et
al. Cutting edge: Med. 2006;354(11):1117-1129. CD4 T cell-mast cell
interactions alter IgE receptor expres- 39. Thomas SY, Lilly CM,
Luster AD. Invariant natural killer sion and signaling. J Immunol.
2008;180(4):2039-2043. T cells in bronchial asthma. N Engl J Med.
2006;354(24):19. Kambayashi T, Baranski JD, Baker RG, et al.
Indirect involve- 2613-2616. ment of allergen-captured mast cells
in antigen presentation. 40. Vijayanand P, Seumois G, Pickard C, et
al. Invariant natural Blood. 2008;111(3):1489-1496. killer T cells
in asthma and chronic obstructive pulmonary20. Kalesnikoff J, Galli
SJ. New developments in mast cell biol- disease. N Engl J Med.
2007;356(14):1410-1422. ogy. Nat Immunol. 2008;9(11):1215-1223. 41.
Das J, Eynott P, Jupp R, et al. Natural killer T cells and CD8121.
Schneider LA, Schlenner SM, Feyerabend TB, Wunderlin M, T cells are
dispensable for T cell-dependent allergic airway Rodewald HR.
Molecular mechanism of mast cell mediated inammation. Nat Med.
2006;12(12):1345-1346. innate defense against endothelin and snake
venom sarafo- 42. Jayaram L, Pizzichini MM, Cook RJ, et al.
Determining toxin. J Exp Med. 2007;204(11):2629-2639. asthma
treatment by monitoring sputum cell counts: effect on22. Rauter I,
Krauth MT, Westritschnig K, et al. Mast cell-derived exacerbations.
Eur Respir J. 2006;27(3):483-494. proteases control allergic
inammation through cleavage of 43. Rothenberg ME, Klion AD,
Roufosse FE, et al; Mepolizumab IgE. J Allergy Clin Immunol.
2008;121(1):197-202. HES Study Group. Treatment of patients with
the hypere-23. Wenzel SE, Barnes PJ, Bleecker ER, et al; T03 Asthma
osinophilic syndrome with mepolizumab. N Engl J Med. Investigators.
A randomized, double-blind, placebo-controlled
2008;358(12):1215-1228. study of tumor necrosis factor-alpha
blockade in severe persis- 44. Flood-Page P, Swenson C, Faiferman
I, et al; International tent asthma. Am J Respir Crit Care Med.
2009;179(7):549-558. Mepolizumab Study Group. A study to evaluate
safety and24. Obata K, Mukai K, Tsujimura Y, et al. Basophils are
essen- efficacy of mepolizumab in patients with moderate per- tial
initiators of a novel type of chronic allergic inammation. sistent
asthma. Am J Respir Crit Care Med. 2007;176(11): Blood.
2007;110(3):913-920. 1062-1071.25. Oh K, Shen T, Le Gros G, Min B.
Induction of Th2 type 45. Flood-Page PT, Menzies-Gow AN, Kay AB,
Robinson DS. immunity in a mouse system reveals a novel
immunoregula- Eosinophils role remains uncertain as
anti-interleukin-5 only tory role of basophils. Blood.
2007;109(7):2921-2927. partially depletes numbers in asthmatic
airway. Am J Respir26. Sokol CL, Barton GM, Farr AG, Medzhitov R. A
mecha- Crit Care Med. 2003;167(2):199-204. nism for the initiation
of allergen-induced T helper type 2 46. Haldar P, Brightling CE,
Hargadon B, et al. Mepolizumab responses. Nat Immunol.
2008;9(3):310-318. and exacerbations of refractory eosinophilic
asthma. N Engl J27. Denzel A, Maus UA, Rodriguez Gomez M, et al.
Basophils Med. 2009;360(10):973-984. enhance immunological memory
responses. Nat Immunol. 47. Nair P, Pizzichini MM, Kjarsgaard M, et
al. Mepolizumab for 2008;9(7):733-742. prednisone-dependent asthma
with sputum eosinophilia.28. Hida S, Yamasaki S, Sakamoto Y, et al.
Fc receptor gamma-chain, N Engl J Med. 2009;360(10):985-993. a
constitutive component of the IL-3 receptor, is required for 48.
Qiu Y, Zhu J, Bandi V, Guntupalli KK, Jeffery PK. Bronchial
IL-3-induced IL-4 production in basophils. Nat Immunol. 2009;
mucosal inammation and upregulation of CXC chemoattrac-
10(2):214-222. tants and receptors in severe exacerbations of
asthma. Thorax.29. Schroeder JT, Chichester KL, Bieneman AP. Human
baso- 2007;62(6):475-482. phils secrete IL-3: evidence of autocrine
priming for pheno- 49. Maneechotesuwan K, Essile-Quaye S,
Kharitonov SA, typic and functional responses in allergic disease.
J Immunol. Adcock IM, Barnes PJ. Loss of control of asthma
following 2009;182(4):2432-2438. inhaled corticosteroid withdrawal
is associated with increased30. Young LJ, Wilson NS, Schnorrer P,
et al. Differential MHC sputum interleukin-8 and neutrophils.
Chest. 2007;132(1): class II synthesis and ubiquitination confers
distinct antigen- 98-105. presenting properties on conventional and
plasmacytoid den- 50. Saha S, Doe C, Mistry V, et al.
Granulocyte-macrophage dritic cells. Nat Immunol.
2008;9(11):1244-1252. colony-stimulating factor expression in
induced sputum and31. Miossec P, Korn T, Kuchroo VK. Interleukin-17
and type 17 bronchial mucosa in asthma and COPD. Thorax.
2009;64(8): helper T cells. N Engl J Med. 2009;361(9):888-898.
671-676.32. Pne J, Chevalier S, Preisser L, et al. Chronically
inamed 51. Pallan S, Mahony JB, OByrne PM, Nair P. Asthma man-
human tissues are inltrated by highly differentiated Th17 agement
by monitoring sputum neutrophil count. Chest. lymphocytes. J
Immunol. 2008;180(11):7423-7430. 2008;134(3):628-630.33. Wakashin
H, Hirose K, Maezawa Y, et al. IL-23 and Th17 cells 52. Rankin SM.
Impact of bone marrow on respiratory disease. enhance
Th2-cell-mediated eosinophilic airway inammation Curr Opin
Pharmacol. 2008;8(3):236-241. in mice. Am J Respir Crit Care Med.
2008;178(10):1023-1032. 53. Denburg JA, Keith PK. Eosinophil
progenitors in airway34. Mucida D, Park Y, Kim G, et al. Reciprocal
TH17 and regula- diseases: clinical implications. Chest.
2008;134(5):1037-1043. tory T cell differentiation mediated by
retinoic acid. Science. 54. Sehmi R, Dorman S, Baatjes A, et al.
Allergen-induced 2007;317(5835):256-260. uctuation in CC chemokine
receptor 3 expression on bone1424 Recent Advances in Chest Medicine
Downloaded from chestjournal.chestpubs.org by guest on July 22,
2011 2010 American College of Chest Physicians
10. marrow CD34+ cells from asthmatic subjects: signicance 74.
Hackett TL, Warner SM, Stefanowicz D, et al. Induction of for
mobilization of haemopoietic progenitor cells in allergic
epithelial-mesenchymal transition in primary airway epithelial
inammation. Immunology. 2003;109(4):536-546. cells from patients
with asthma by transforming growth factor-55. Gauvreau GM, Boulet
LP, Cockcroft DW, et al. Antisense beta1. Am J Respir Crit Care
Med. 2009;180(2):122-133. therapy against CCR3 and the common beta
chain attenuates 75. Yoshisue H, Kirkham-Brown J, Healy E, Holgate
ST, Sampson allergen-induced eosinophilic responses. Am J Respir
Crit AP, Davies DE. Cysteinyl leukotrienes synergize with growth
Care Med. 2008;177(9):952-958. factors to induce proliferation of
human bronchial broblasts.56. Dorman SC, Babirad I, Post J, et al.
Progenitor egress from J Allergy Clin Immunol. 2007;119(1):132-140.
the bone marrow after allergen challenge: role of stromal cell- 76.
Henderson WR Jr, Chiang GK, Tien YT, Chi EY. Reversal derived
factor 1alpha and eotaxin. J Allergy Clin Immunol. of
allergen-induced airway remodeling by CysLT1 receptor
2005;115(3):501-507. blockade. Am J Respir Crit Care Med.
2006;173(7):718-728.57. Catalli AE, Thomson JV, Babirad IM, et al.
Modulation of 77. Kelly MM, Chakir J, Vethanayagam D, et al.
Montelukast beta1-integrins on hemopoietic progenitor cells after
aller- treatment attenuates the increase in myobroblasts following
gen challenge in asthmatic subjects. J Allergy Clin Immunol.
low-dose allergen challenge. Chest. 2006;130(3):741-753.
2008;122(4):803-810. 78. Koff JL, Shao MX, Ueki IF, Nadel JA.
Multiple TLRs acti-58. Holgate ST. Epithelium dysfunction in
asthma. J Allergy Clin vate EGFR via a signaling cascade to produce
innate immune Immunol. 2007;120(6):1233-1244. responses in airway
epithelium. Am J Physiol Lung Cell Mol59. Barbato A, Turato G,
Baraldo S, et al. Epithelial damage Physiol.
2008;294(6):L1068-L1075. and angiogenesis in the airways of
children with asthma. 79. Vancheri C, Gili E, Failla M, et al.
Bradykinin differenti- Am J Respir Crit Care Med.
2006;174(9):975-981. ates human lung fibroblasts to a myofibroblast
phenotype60. Cohen L, E X, Tarsi J, et al; and the NHLBI Severe
Asthma via the B2 receptor. J Allergy Clin Immunol. 2005;116 (6):
Research Program (SARP). Epithelial cell proliferation con-
1242-1248. tributes to airway remodeling in severe asthma. Am J
Respir 80. Kunzmann S, Schmidt-Weber C, Zingg JM, et al. Connective
Crit Care Med. 2007;176(2):138-145. tissue growth factor expression
is regulated by histamine in61. Ziegler SF, Liu YJ. Thymic stromal
lymphopoietin in nor- lung broblasts: potential role of histamine
in airway remod- mal and pathogenic T cell development and
function. Nat eling. J Allergy Clin Immunol. 2007;119(6):1398-1407.
Immunol. 2006;7(7):709-714. 81. Panettieri RA Jr, Kotlikoff MI,
Gerthoffer WT, et al; National62. Allakhverdi Z, Comeau MR, Jessup
HK, et al. Thymic Heart, Lung, and Blood Institute. Airway smooth
muscle in stromal lymphopoietin is released by human epithelial
cells bronchial tone, inammation, and remodeling: basic knowl- in
response to microbes, trauma, or inflammation and edge to clinical
relevance. Am J Respir Crit Care Med. 2008; potently activates mast
cells. J Exp Med. 2007;204(2):253-258. 177(3):248-252.63. Ying S,
OConnor B, Ratoff J, et al. Thymic stromal lym- 82. Lguillette R,
Laviolette M, Bergeron C, et al. Myosin, trans- phopoietin
expression is increased in asthmatic airways and gelin, and myosin
light chain kinase: expression and function correlates with
expression of Th2-attracting chemokines and in asthma. Am J Respir
Crit Care Med. 2009;179(3):194-204. disease severity. J Immunol.
2005;174(12):8183-8190. 83. El-Shazly A, Berger P, Girodet PO, et
al. Fraktalkine64. Pgorier S, Arouche N, Dombret MC, Aubier M,
Pretolani produced by airway smooth muscle cells contributes to M.
Augmented epithelial endothelin-1 expression in refrac- mast cell
recruitment in asthma. J Immunol. 2006;176(3): tory asthma. J
Allergy Clin Immunol. 2007;120(6):1301-1307. 1860-1868.65. Zhao Y,
Usatyuk PV, Gorshkova IA, et al. Regulation of COX-2 84. Hollins F,
Kaur D, Yang W, et al. Human airway smooth mus- expression and IL-6
release by particulate matter in airway cle promotes human lung
mast cell survival, proliferation, and epithelial cells. Am J
Respir Cell Mol Biol. 2009;40(1):19-30. constitutive activation:
cooperative roles for CADM1, stem66. Gereke M, Jung S, Buer J,
Bruder D. Alveolar type II epi- cell factor, and IL-6. J Immunol.
2008;181(4):2772-2780. thelial cells present antigen to CD4(1) T
cells and induce 85. Thangam EB, Venkatesha RT, Zaidi AK, et al.
Airway smooth Foxp3(1) regulatory T cells. Am J Respir Crit Care
Med. 2009; muscle cells enhance C3a-induced mast cell degranulation
179(5):344-355. following cell-cell contact. FASEB J.
2005;19(7):798-800.67. Bai TR, Vonk JM, Postma DS, Boezen HM.
Severe exacer- 86. Sutcliffe A, Kaur D, Page S, et al. Mast cell
migration to Th2 bations predict excess lung function decline in
asthma. Eur stimulated airway smooth muscle from asthmatics.
Thorax. Respir J. 2007;30(3):452-456. 2006;61(8):657-662.68. OByrne
PM, Pedersen S, Lamm CJ, Tan WC, Busse WW; 87. Kaminska M, Foley S,
Maghni K, et al. Airway remodeling in START Investigators Group.
Severe exacerbations and subjects with severe asthma with or
without chronic persis- decline in lung function in asthma. Am J
Respir Crit Care Med. tent airow obstruction. J Allergy Clin
Immunol. 2009;124(1): 2009;179(1):19-24. 45-51.69. Turato G,
Barbato A, Baraldo S, et al. Nonatopic children 88. Simcock DE,
Kanabar V, Clarke GW, et al. Induction of with multitrigger
wheezing have airway pathology comparable angiogenesis by airway
smooth muscle from patients with to atopic asthma. Am J Respir Crit
Care Med. 2008;178(5): asthma. Am J Respir Crit Care Med.
2008;178(5):460-468. 476-482. 89. Simcock DE, Kanabar V, Clarke GW,
OConnor BJ, Lee TH,70. Rawlins EL. Lung epithelial progenitor
cells: lessons from Hirst SJ. Proangiogenic activity in
bronchoalveolar lavage development. Proc Am Thorac Soc.
2008;5(6):675-681. uid from patients with asthma. Am J Respir Crit
Care Med.71. Schmidt M, Sun G, Stacey MA, Mori L, Mattoli S.
Identication 2007;176(2):146-153. of circulating brocytes as
precursors of bronchial myobro- 90. Hoshino M, Takahashi M, Aoike
N. Expression of vascular blasts in asthma. J Immunol.
2003;171(1):380-389. endothelial growth factor, basic broblast
growth factor,72. Saunders R, Siddiqui S, Kaur D, et al. Fibrocyte
localization and angiogenin immunoreactivity in asthmatic airways
and to the airway smooth muscle is a feature of asthma. J Allergy
its relationship to angiogenesis. J Allergy Clin Immunol. Clin
Immunol. 2009;123(2):376-384. 2001;107(2):295-301.73. Dolgachev VA,
Ullenbruch MR, Lukacs NW, Phan SH. Role 91. Chetta A, Zanini A,
Foresi A, et al. Vascular endothelial of stem cell factor and bone
marrow-derived broblasts in growth factor up-regulation and
bronchial wall remodelling airway remodeling. Am J Pathol.
2009;174(2):390-400. in asthma. Clin Exp Allergy.
2005;35(11):1437-1442.www.chestpubs.org CHEST / 137 / 6 / JUNE,
2010 1425 Downloaded from chestjournal.chestpubs.org by guest on
July 22, 2011 2010 American College of Chest Physicians
11. 92. Zanini A, Chetta A, Saetta M, et al. Chymase-positive
mast 95. Lommatzsch M, Lindner Y, Edner A, Bratke K, Kuepper cells
play a role in the vascular component of airway remod- M , Virchow
JC . Adverse effects of salmeterol in asthma: eling in asthma. J
Allergy Clin Immunol. 2007;120( 2): a neuronal perspective. Thorax.
2009;64(9):763-769. 329-333. 96. Starosta V, Pazdrak K, Boldogh I,
Svider T, Kurosky A.93. Siddiqui S, Sutcliffe A, Shikotra A, et al.
Vascular remodeling Lipoxin A4 counterregulates GM-CSF signaling in
eosino- is a feature of asthma and nonasthmatic eosinophilic
bronchitis. philic granulocytes. J Immunol. 2008;181(12):8688-8699.
J Allergy Clin Immunol. 2007;120(4):813-819. 97. Kohli P, Levy BD.
Resolvins and protectins: mediating solu-94. Caceres AI, Brackmann
M, Elia MD, et al. A sensory neuronal tions to inammation. Br J
Pharmacol. 2009;158(4):960-971. ion channel essential for airway
inammation and hyperre- 98. Levy BD, Kohli P, Gotlinger K, et al.
Protectin D1 is gener- activity in asthma. Proc Natl Acad Sci U S
A. 2009;106(22): ated in asthma and dampens airway inammation and
hyper- 9099-9104. responsiveness. J Immunol.
2007;178(1):496-502.1426 Recent Advances in Chest Medicine
Downloaded from chestjournal.chestpubs.org by guest on July 22,
2011 2010 American College of Chest Physicians
12. Recent Advances in the Pathophysiology of Asthma Desmond M.
Murphy and Paul M. OByrne Chest 2010;137; 1417-1426 DOI
10.1378/chest.09-1895 This information is current as of July 22,
2011Updated Information & ServicesUpdated Information and
services can be found
at:http://chestjournal.chestpubs.org/content/137/6/1417.full.htmlReferencesThis
article cites 98 articles, 56 of which can be accessed free
at:http://chestjournal.chestpubs.org/content/137/6/1417.full.html#ref-list-1Permissions
& LicensingInformation about reproducing this article in parts
(figures, tables) or in its entirety can befound online
at:http://www.chestpubs.org/site/misc/reprints.xhtmlReprintsInformation
about ordering reprints can be found
online:http://www.chestpubs.org/site/misc/reprints.xhtmlCitation
AlertsReceive free e-mail alerts when new articles cite this
article. To sign up, select the"Services" link to the right of the
online article.Images in PowerPoint formatFigures that appear in
CHEST articles can be downloaded for teaching purposes inPowerPoint
slide format. See any online figure for directions. Downloaded from
chestjournal.chestpubs.org by guest on July 22, 2011 2010 American
College of Chest Physicians