Embed Size (px)
Citation preview
Case capsule
Dr. Zeeshan

• 40 / M
• No comorbidities
• Epigastric pain associated with epigastric fullness• Dysphagia to solids for 1 month• Cough after food intake• Dyspnoea on exertion
• ? Relevant H/O
NO SIGNIFICANT FINDINGS ON EXAMINATION
DIFFERENTIALS
• Esophageal pathology- Intraluminal: Benign : GERD, Esophageal webs, rings , Zencker’s
diverticulum
Malignant : Ca esophagus
- Extrinsic compression
BLOOD INVESTIGATIONS WITHIN NORMAL LIMITS
HOW WOULD YOU LIKE TO PROCEED?
WHAT NEXT?
• UGI scopy
• Barium swallow
• ? Importance of order
WHAT NEXT?
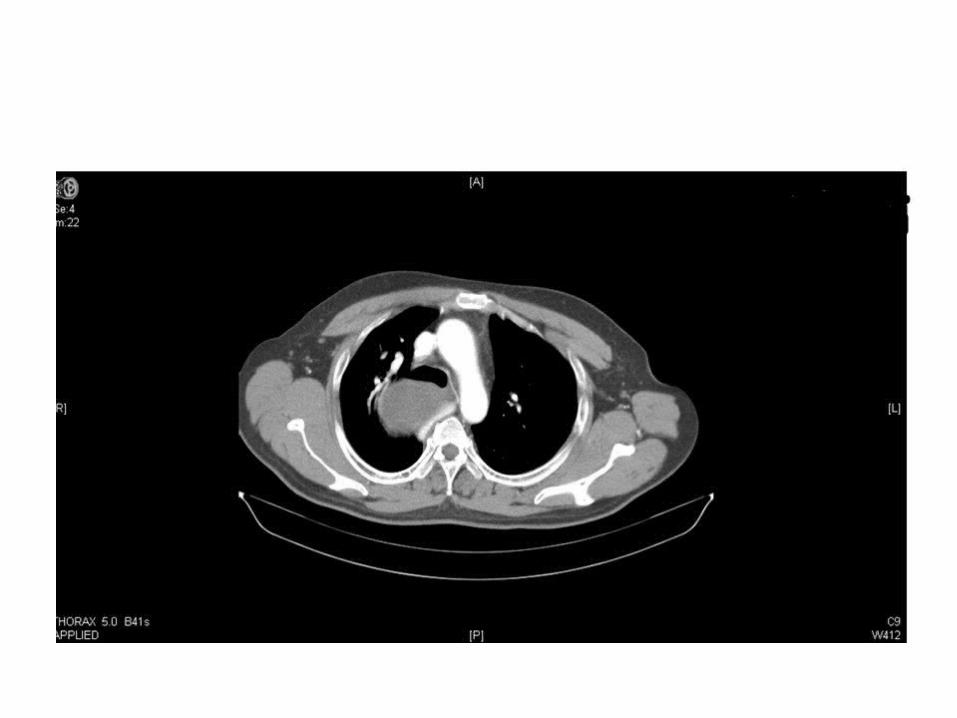


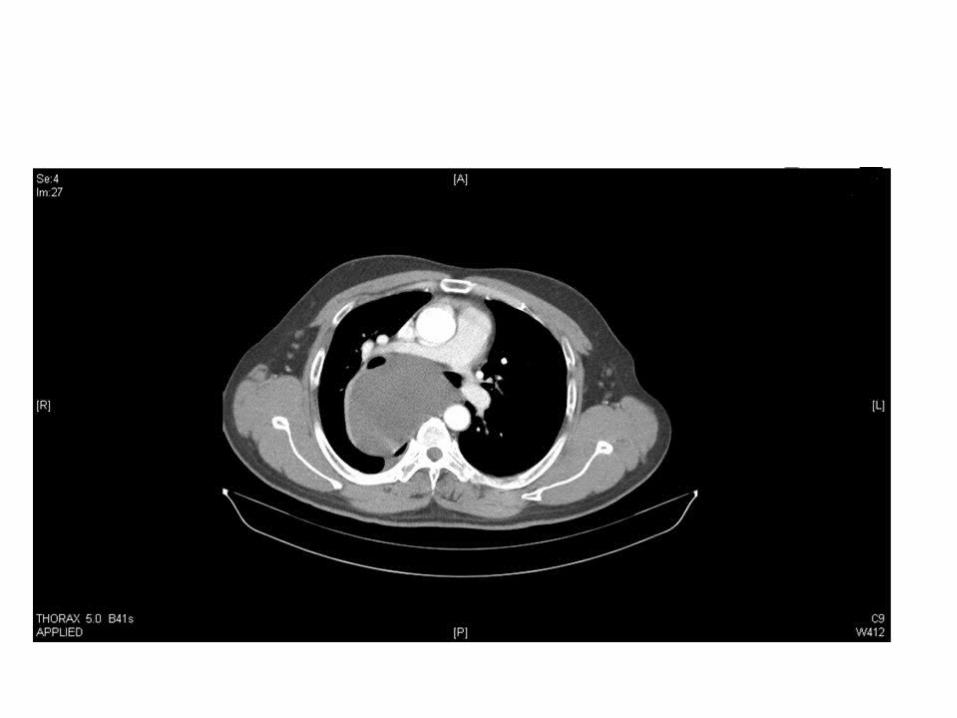


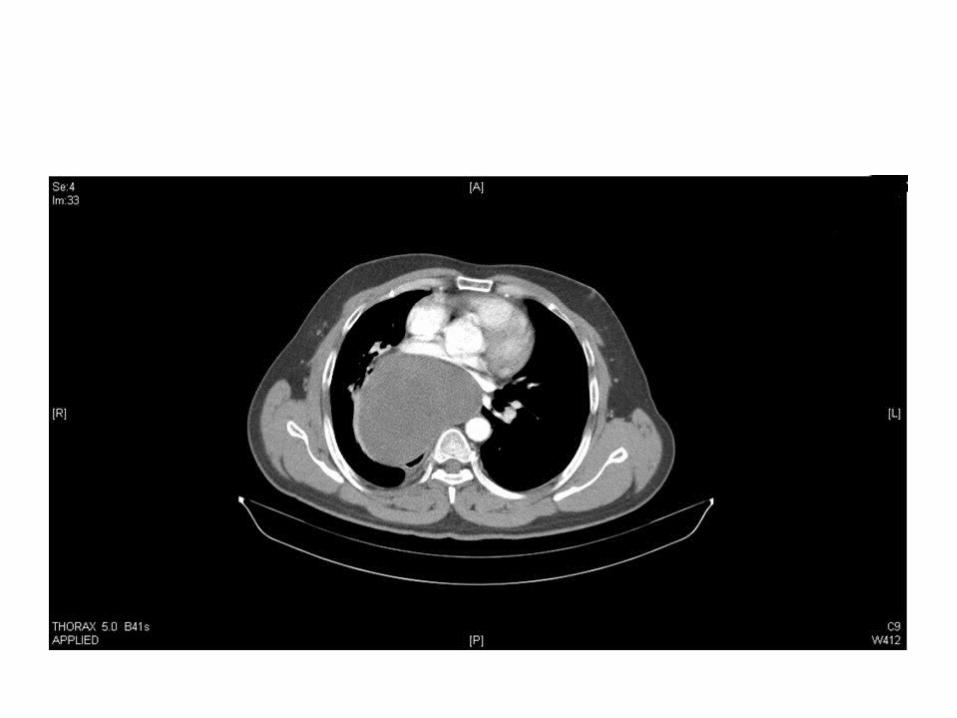
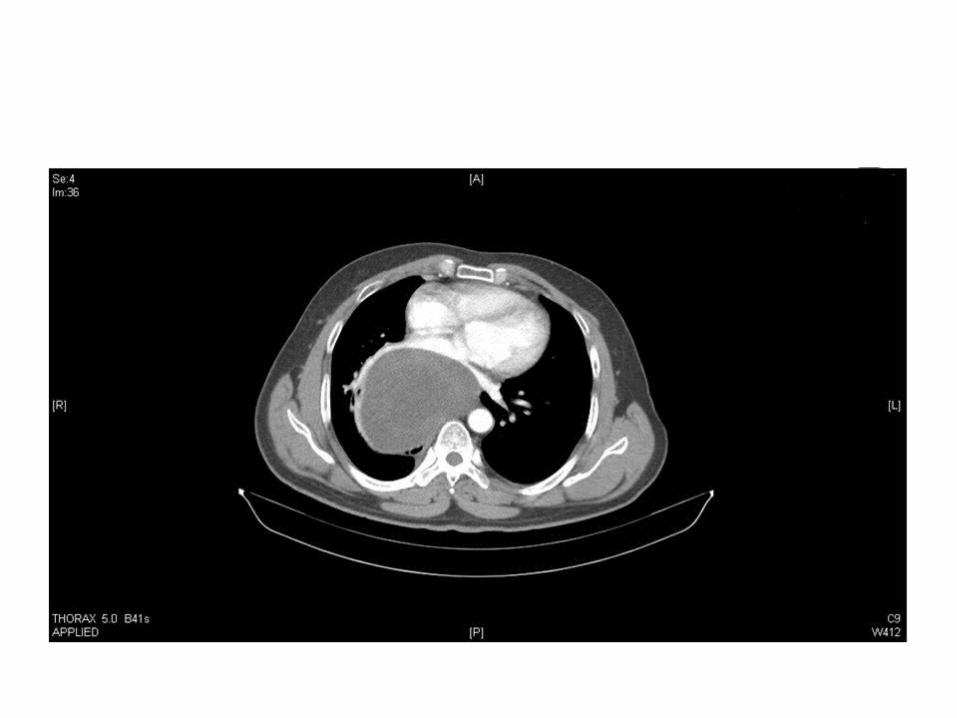

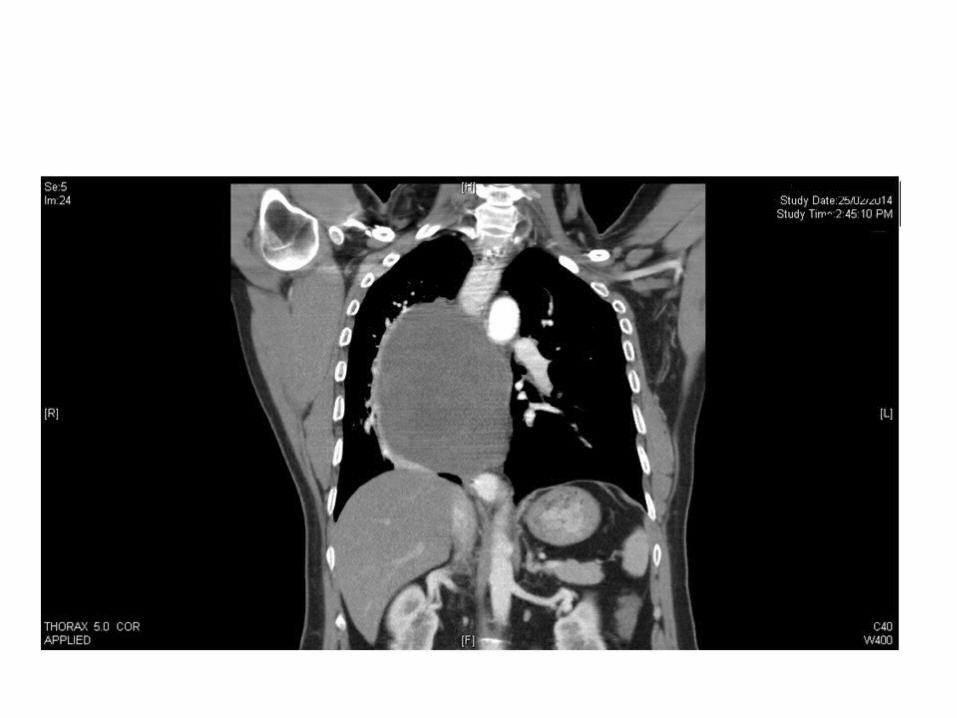
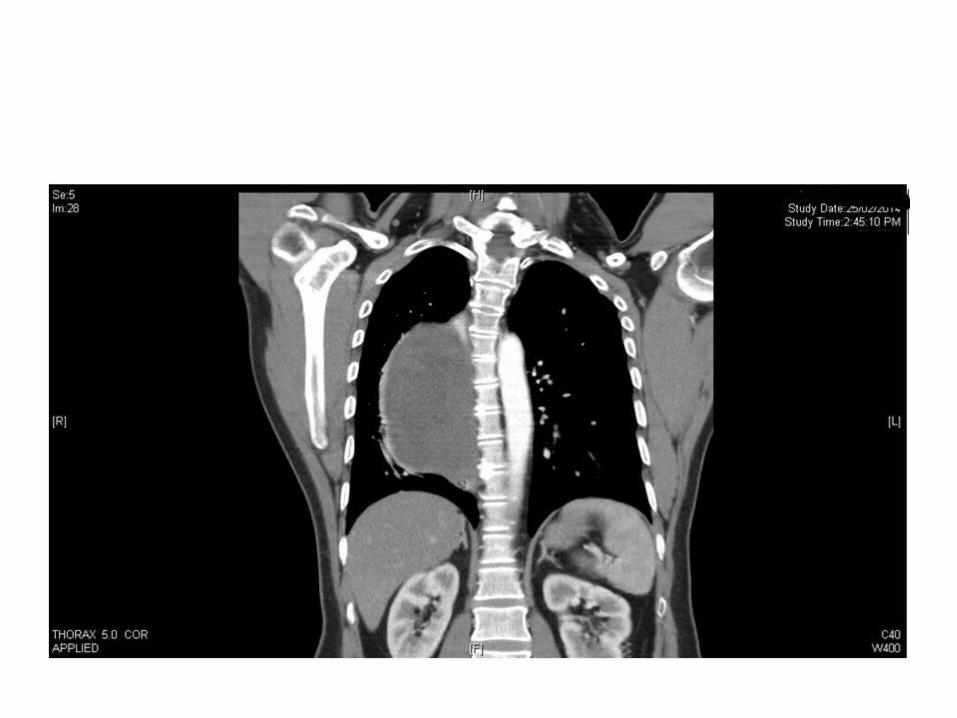
CT report A well defined, thin walled, large, nonenhancing, fluid density
lesion, measuring 13 mm x 11 mm x 9.1 mm in the middle and posterior mediastinum, extending from T4 to T9 vertebrae and predominantly on the right.
The lesion is displacing the trachea anteriorly, the lower two third of the esophagus to the ipsilateral side, and causing splaying of the carina, main bronchi and right pulmonary artery
The lesion is seen compressing upon the esophageal lumen; fat planes between the lesion and the esophageal wall is indistinct. The lesion causes compression of the left atrium and the pulmonary veins are stretched over the anterior surface of the lesion, however the fat plane is preserved
Approach to a mediastinal mass
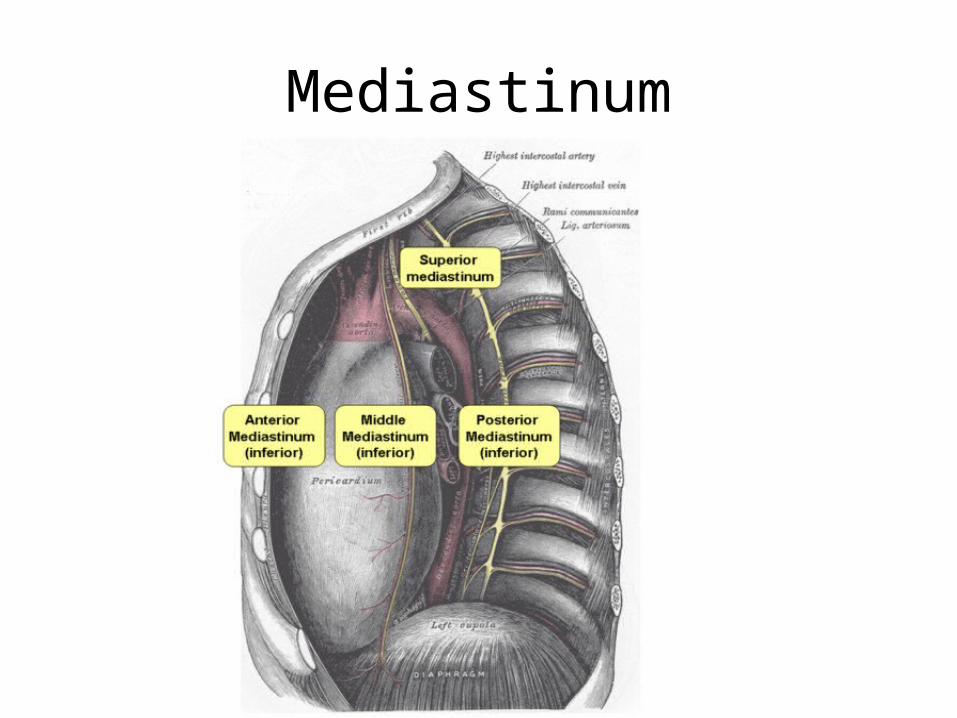
Mediastinum
Compartments
• Anterior
• Middle
• Posterior
Anterior compartment
• Between sternum and anterior aspect of pericardium
• Contents:- Thymus- Internal mammary A.- Lymph node- Connective tissue - Fat
Anomalies of Ant. Compartment
• Terrible T’s
- Thymoma- Teratoma- (Terrible) lymphoma- Thyroid tissue
Middle compartment
• Ant: Pericardium• Posteriorly : Ventral surface of thoracic spineContents:- Heart- Airway- Pericardium- Ascending thoracic aorta- SVC with azygos vein

Anomalies of middle compartment
• Lymphadenopathy : MC cause- Sarcoidosis- Lymphoma- Metastatic lung malignancy
Posterior mediastinum
• Artery– Thoracic part of descending Aorta
• Veins– Azygos vein– Hemiazygos, accessory hemiazygos veins
• Nerves– Vagus nerve– Splanchnic nerve
• Esophagus• Thoracic duct
Anomalies of Post. Mediastinum
• Mass arising from Esophagus
• Aneurysms of descending aorta
• Neurogenic tumors
Importance of H/O
• Age
• Anatomic location
• Associated symptoms
Why age?
• Adults :- Thymomas
- Lymphomas
- Germ cell tumors
- Only 1/3rd lesion are symptomatic
• Children:
- Post. Neurogenic tumors
- Lymphomas
- Germ cell tumors
- 2/3rd symptomatic

Anatomic location
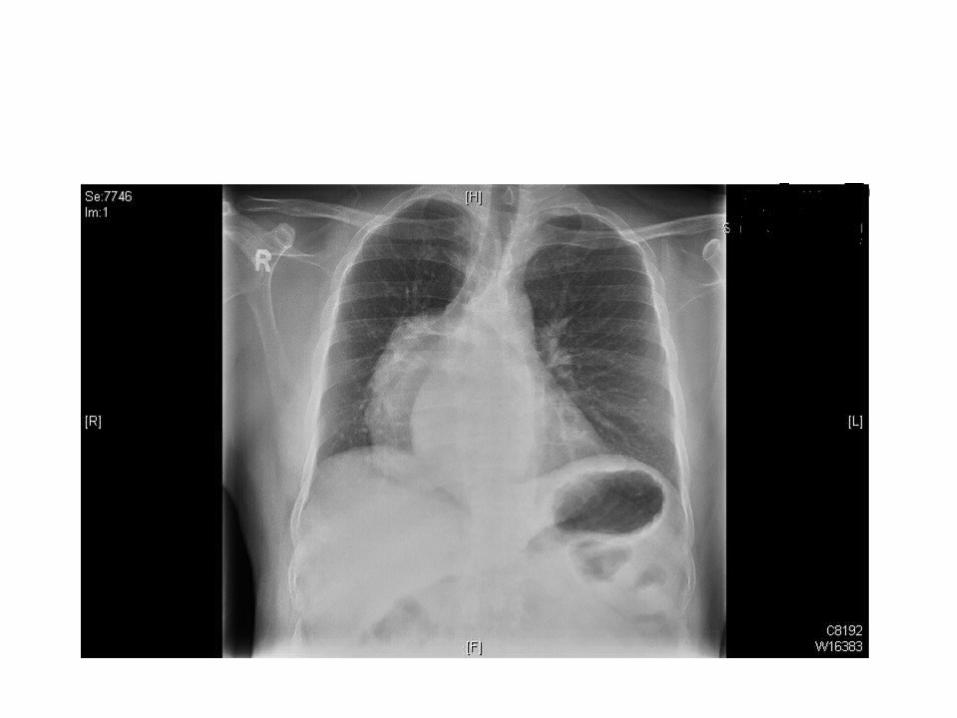
• Chest X-ray- AP- Lateral
• CT thorax
WHICH PART OF MEDIASTINUM IS THE MASS ARISING FROM??







Posterior mediastinum
• Differentials for a cystic mass in posterior mediastinum:
- Bronchogenic cyst
- Esophageal duplication cyst
Bronchogenic cyst
• MC cystic lesion
• Abnormal budding of the lungs
• MC in men/ right paratracheal location
• Symptoms of cough, substernal pain, recurrent infections, dyspnoea
Esophageal duplication cysts
• Third most common benign esophageal mass• MC – Leiomyoma• 2nd MC – Polyp
• Three criteria to establish diagnosis:1.Esophageal attachment2.Presence of 2 layers of muscularis propria3.Epithelium characteristic of GI tract
HOW WOULD YOU LIKE TO PROCEED

• EUS
• Preoperative biopsy : debatable Not recommended
• Pt was posted for Thoracotomy proceed
• He underwent excision of posterior mediastinal tumor with resection of thoracic esophagus + stomach pullup.
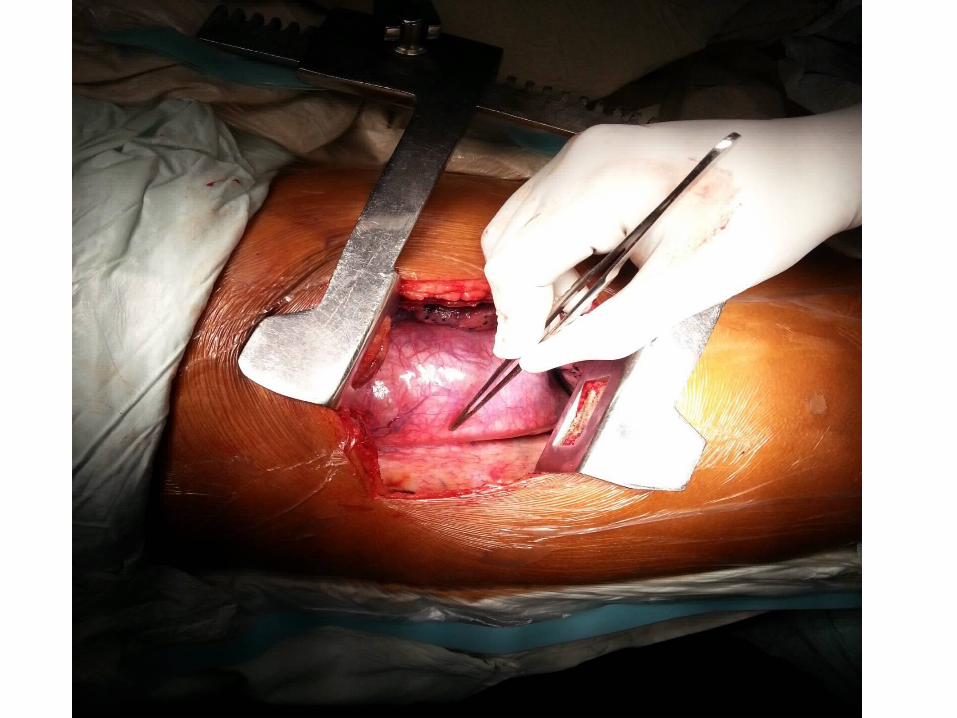
Findings
• 15 x 25x12 cm sized mass arising from the posterior mediastinum ? site of origin with the oesophagus stretched over it laterally and the tumour was crossing the midline.
• The lower limit was about 4 cm from the oesophageal hiatus.
• The tumour contained jelly like material and was infiltrating the posterior pericardium.
• There were few enlarged nodes in relation to the tumour.
• The tumour was very vascular.


Biopsy
• Smooth muscle tumor probably benign
• Leiomyoma
• Maximum tumor size – 11.2cm
• Tumor was adherent to wall of esophagus
Leiomyoma of esophagus
Incidence
• Most common benign tumors of the esophagus
• 90% occur in the lower/middle third
• Arise from muscularis mucosa
• Male predominance
• Most lesion are intramural/submucosal
• Solitary
• Size : 2-8cm
• Slow growing tumors
• 50% patients asymptomatic
Symptoms
• Dysphagia – Most common symptom
• Retrosternal pain/discomfort
• Heart burn
• Weight loss
Diagnosis
• UGI scopy : Submucosal mass lesion
• Barium swallow : Smooth filling defect in the esophageal lumen without a mucosal abnormality
• CT Thorax: Well defined eccentric intramural mass with homogenous enhancement after administration of IV contrast
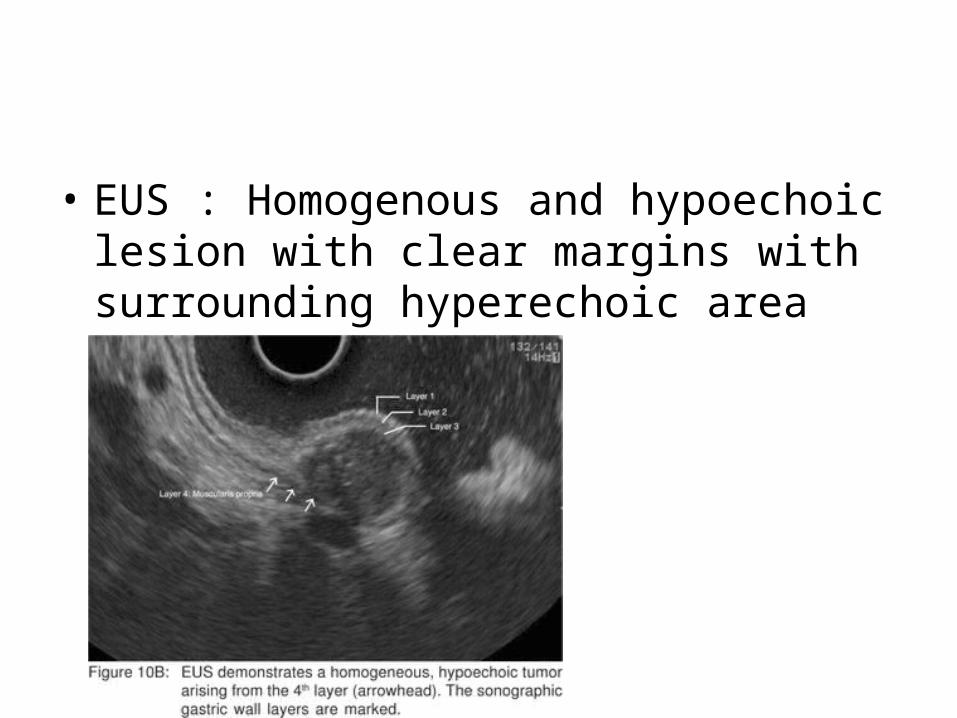
• EUS : Homogenous and hypoechoic lesion with clear margins with surrounding hyperechoic area

• Biopsy : To be avoided
- Cause scarring and hampers extramucosal excision of tumor
- Usually non diagnostic
Management
• Asymptomatic/ small leiomyomas
• Monitor periodically using UGI scopy, EUS and CT thorax
• Risk of malignant transformation < 1%
Indication for surgery
• Symptomatic leiomyomas
• Leiomyomas > 5cm
Modes of excision
• Thoracoscopic excision of lesion
• Open surgery
Open approach
• Middle third of esophagus – Right thoracotomy
• Lower third of esophagus - Left thoracotomy/ Left thoraco-abdominal / Transhiatal approach
Summary
• Leiomyomas are rare tumors of esophagus
• If <5cm patient usually kept on follow-up
• Large leiomyomas are excised with segmental esophageal resections
• Malignant potential <1%