Embed Size (px)
Citation preview

Dysphagia Done by : Yahyia AL-Abri
90440Senior

Outline
• Anatomy of the pharynx.• Phases of swallowing.• Dysphagia Vs. Odynophagia.• Types of dysphagia.• How we approach ?• DDx of dysphagia.

Anatomy of the pharynx

Phases of swallowing oral phase - Stage I transport
- to the post-canine region. And rotates laterally
- Food Processing - are reduced in
size - Softened
- Stage II transport - to the
oropharynx

Pharyngeal stage
It has two crucial biological features: (1) food passage, propelling the food bolus through the pharynx and UES to the esophagus; and (2) airway protection

Esophageal stage
• (upper one third) : striated muscle • (lower two thirds) is smooth muscle• true peristalsis regulated by the autonomic
nervous system

Dysphagia Vs. Odynophagia
• Dysphagia– Difficulty in swallowing
• Odynophagia– Painful swallowing
• Globus sensation– A persistent or intermittent non painful sensation of a
lump or foreign body with the absence of dysphagia.

Classifications
• Orophayngeal dysphagia• transfer dysphagia is characterized by difficulty initiating a swallow.
• Swallowing may be accompanied by coughing, choking, nasopharyngeal regurgitation, aspiration, and a sensation of residual food remaining in the pharynx
• Esophageal dysphagia • characterized by difficulty swallowing several seconds after initiating a
swallow and a sensation of food getting stuck in the esophagus.

Causes of oropharyngeal dysphagia
Diseases of myoneural junction
Myasthnia gravies. Eaton - Lambert syndrome.
Structural abnormalities Oropharyngeal neoplasm. Extrinsic compression
(cervical osteophytes, thyromegaly).
Congenital web. Zenker diverticulum. Foreign body.
Neurological disorders Cerebo vascular accident
(especially brain stem). Multiple sclerosis. Parkinson’s disease.
Muscular disorders Muscular dystrophies. Amyloidosis.

Types
Mechanical obstruction• Dysphagia for solids that
later progresses to involve liquids is more likely to reflect mechanical obstruction 1
Neuromuscular • Dysphagia to both solids
and liquids from the onset of symptoms is probably due to a motility disorder of the esophagus.
1-Gasiorowska A, Fass R, Current approach to dysphagia:Gastroenterol Hepatol. 2009;5:269.

How to approach ?

History • Do you have problems initiating a swallow or do you feel food getting
stuck a few seconds after swallowing?– (Helps distinguish oropharyngeal from esophageal dysphagia.)
• Do you cough or choke or is food coming back through your nose after swallowing?– (Coughing, choking, or nasal regurgitation suggests aspiration and
oropharyngeal dysphagia.)• Do you have problem swallowing solids, liquids, or both?
– (Liquids, not solids, suggests a motility disorder; solids progressing to liquids suggests a benign or malignant obstruction.)
• How long have you had problems swallowing and have your symptoms progressed, remained stable, or are they intermittent? – (Rapidly progressive dysphagia is concerning for malignancy.)

History
• Systematic review • Past medical history • Past surgical history • Radiation therapy• medications using now (ask specifically about
potassium chloride, ferrous sulfate, quinidine, ascorbic acid, tetracycline, aspirin and NSAIDs)?

• General examination.• Vital signs.• Complete E.N.T. Examination.• Neck examination • Neurological Examination • Associated physical examination
Skin: features of CTD, e.g. scleroderma.
Pulmonary complications from aspiration.
Physical Examination

Investigations
• Upper endoscopy • diagnostic, biopsy, therapeutic
• Barium swallow – prior to upper endoscopy with suggestive history or
clinical features of a proximal esophageal lesion– negative upper endoscopy

Investigations
• Motility testing– suspected esophageal motility disorder
CXR aspiration pneumonia
CT/ MRI structural abnormalities & staging of
malignancy

Types
Mechanical obstruction• Intermittent
– Lower esophageal ring
• Progressive – Peptic stricture– Carcinoma
Neuromuscular • Intermittent
– Esophageal spasm
• Progressive – Scleroderma– Achalasia

Esophageal rings and webs
Rings Webs
• Concentric,• smooth, thin (3-5
mm) • normal esophageal
tissue (3 anatomic layers of mucosa, submucosa, and muscle).
• Eccentric• thin (2-3 mm),
smooth • normal esophageal
tissue ( mucosa and submucosa )

Esophageal rings and webs
• The pathogenesis of esophageal rings is controversial– both chronic damage from gastroesophageal
reflux – a congenital or developmental origin
• Schatzki rings are almost always associated with hiatal hernias (B type)

Diagnose
• An esophageal ring is diagnosed on barium swallow and upper endoscopy:
Hirano I, Gilliam J, Goyal RK; Clinical and manometric features of the lower esophageal muscular ring. Am J Gastroenterol. 2000;95(1):43.
thick constriction of variable luminal diameter

TREATMENT
• First line : a single dilation with a large bougie dilator (≥50 French) or balloon dilator (18 to 20 mm).– eosinophilic esophagitis, dilation should be
deferred.• Risk of recurrence : high risk 63%

Treatment
• Acid suppression– Decrease risk of recurrence
• Refractory rings– Intralesional steroid injection prior to dilation– Endoscopic electrosurgical incision

Types
Mechanical obstruction• Intermittent
– Lower esophageal ring
• Progressive – Peptic stricture– Carcinoma
Neuromuscular • Intermittent
– Esophageal spasm
• Progressive – Scleroderma– Achalasia

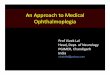
Peptic esophageal strictures
• Peptic esophageal strictures are sequelae of gastroesophageal
reflux -induced esophagitis,
• 10 percent of patients with gastroesophageal reflux disease
(GERD) who seek medical attention*1
• Malignancy
• Risk factors
– older age, male gender, and longer duration of reflux symptoms *2
1-Katz PO, Knuff TE, Benjamin SB, Castell DO ; Abnormal esophageal pressures in reflux esophagitis: cause or effect? Am J Gastroenterol. 1986;81(9):744.
El-Serag HB, Sonnenberg A; Association of esophagitis and esophageal strictures with diseases treated with nonsteroidal anti-inflammatory drugs.Am J Gastroenterol. 1997;92(1):52.

• Diagnosis:• Endoscopy • barium study • The location, length, and diameter of the stricture and
the smoothness or irregularity of the esophageal wall.• Biopsy
• Treatment:• endoscopic dilatation and PPI.• anti-reflux surgery if above treatment unsuccessful.
Peptic stricture

Types
Mechanical obstruction• Intermittent
– Lower esophageal ring
• Progressive – Peptic stricture– Carcinoma
Neuromuscular • Intermittent
– Esophageal spasm
• Progressive – Scleroderma– Achalasia

2 histologic subtypes:1. Squamous cell carcinoma (most common) → upper 2/3,
increase with smoking, alcohol, black ppl.2. Adenocarcinoma → lower 1/3, increase with GERD, white ppl.
Symptoms: Retrosternal chest pain, dysphagia which progress to include
liquid, unintentional weight loss, upper GI bleed, epigastric pain, lymphadenopathy, GERD sx.
Diagnosis: Barium swallow. Endoscopy with biopsy.
Esophageal Carcinoma

Types
Mechanical obstruction• Intermittent
– Lower esophageal ring
• Progressive – Peptic stricture– Carcinoma
Neuromuscular • Intermittent
– Esophageal spasm
• Progressive – Scleroderma– Achalasia

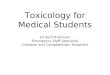
Definition:contractions of the esophagus are irregular, uncoordinated, and Sometimes powerful.
Symptoms:Retrosternal chest pain, dysphagia to bothSolids and liquids, regurgitation.
Diagnosis:Barium swallow: “Corkscrew pattern”Manometry: >30% (but <100%) of esophageal contractions are A peristaltic.
Diffuse Esophageal Spasm (DES)

Management:• Medical:• Botulinum toxin• Proton pump inhibitors• tricyclic antidepressants
• Surgical: • long esophageal myotomy if unresponsive to above treatment
• Balloon dilatation.
Diffuse Esophageal Spasm (DES)

Types
Mechanical obstruction• Intermittent
– Lower esophageal ring
• Progressive – Peptic stricture– Carcinoma
Neuromuscular • Intermittent
– Esophageal spasm
• Progressive – Scleroderma– Achalasia

Definition:Systemic disease characterized by Vascular dysfunction and tissue fibrosis of the skin and internal organs.
Diagnosis:• Clinical features of scleroderma with serologic tests• Manometry: decreased pressure in LES, decreased peristalsis in
body of esophagus.
Scleroderma

Treatment: Medical: aggressive GERD therapy .
Surgery: anti-reflux surgery fundoplication, which involves wrapping the
upper portion of the stomach around the end of the esophagus
Scleroderma

Types
Mechanical obstruction• Intermittent
– Lower esophageal ring
• Progressive – Peptic stricture– Carcinoma
Neuromuscular • Intermittent
– Esophageal spasm
• Progressive – Scleroderma– Achalasia

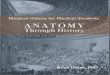
Definition:- Failure of smooth muscle relaxation at LES- aperistalsis.-autoimune 1
Symptoms: Dysphagia to both solids and liquids, regurgitation of undigested food, heartburn.
Diagnosis: Barium studies : esophagus terminates in narrowing at LES (“bird’s beak”). Manometry: definitive diagnosis.
Achalasia
Gockel I, Becker J, Wouters MM, et al. Common variants in the HLA-DQ region confer susceptibility to idiopathic achalasia. Nat Genet. 2014 Aug. 46(8):901-4. [Medline]. Mysterious esophagus disease is autoimmune after all. Ku Leuven. Available at http://www.kuleuven.be/english/news/mysterious-esophagus-disease-is-autoimmune-after-all. Accessed: Oct 29, 2014.

Treatment:
• Initial therapy – graded pneumatic dilation (PD) – laparoscopic surgical myotomy with a partial fundoplication in
patients fit to undergo surgery.
• Botulinum toxin therapy is recommended for patients not suited to PD or surgery.
Achalasia


References • www.uptodate.com• www.medscape.com • https://www.ncbi.nlm.nih.gov/• Ear, Nose, Throat and Head and Neck Surgery; R.S. Dhillon, C.A. East; 3rd edition• Gockel I, Becker J, Wouters MM, et al. Common variants in the HLA-DQ region confer
susceptibility to idiopathic achalasia. Nat Genet. 2014 Aug. 46(8):901-4. [Medline]. • Mysterious esophagus disease is autoimmune after all. Ku Leuven. Available at
http://www.kuleuven.be/english/news/mysterious-esophagus-disease-is-autoimmune-after-all. Accessed: Oct 29, 2014.
• 1-Katz PO, Knuff TE, Benjamin SB, Castell DO ; Abnormal esophageal pressures in reflux esophagitis: cause or effect? Am J Gastroenterol. 1986;81(9):744.
• El-Serag HB, Sonnenberg A; Association of esophagitis and esophageal strictures with diseases treated with nonsteroidal anti-inflammatory drugs.
• Am J Gastroenterol. 1997;92(1):52. • 1-Gasiorowska A, Fass R, Current approach to dysphagia:Gastroenterol Hepatol.
2009;5:269.