Embed Size (px)
Citation preview

Stent e fibrillazione atriale: singola,
duplice o triplice terapia
antitrombotica?
F Arrigo, Messina
Arrigo, Messina (Italy) 2016
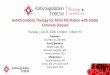
Prevalenza con l’età
Trend futuro
Arrigo, Messina (Italy) 2016
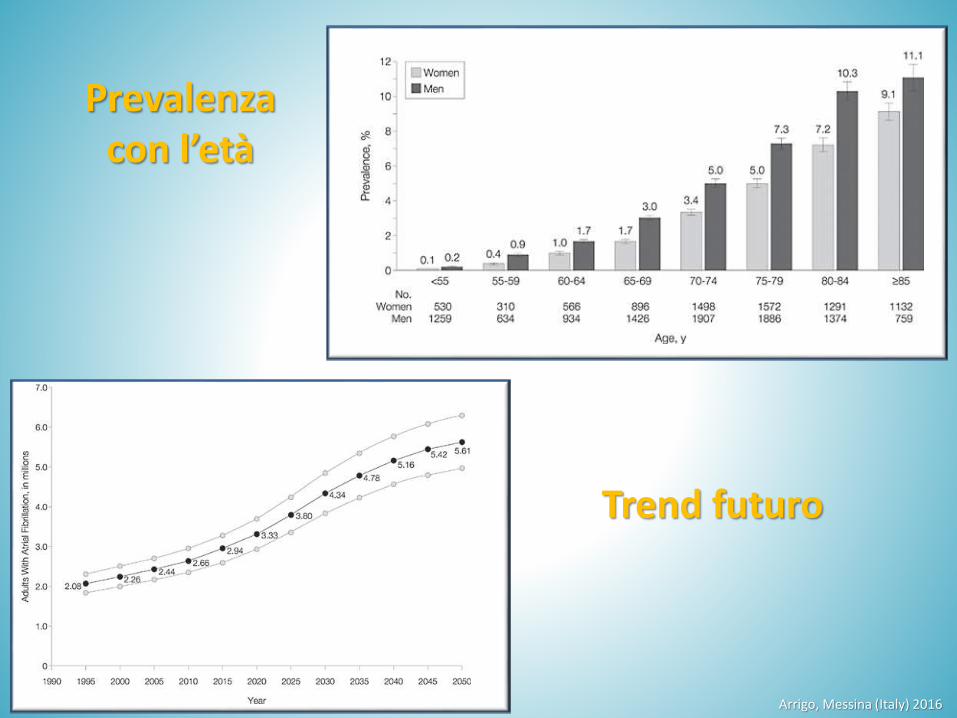
104 cohort studies. 587,867 participants with AF Outcome Relative risk 95% CI
Heart failure 4.99 3.04–8.22
Stroke 2.42 2.17–2.71
CV mortality 2.03 1.79–2.30
Major CV events 1.96 1.53–2.51
Sudden cardiac death 1.88 1.36–2.60
Chronic kidney disease 1.64 1.41–1.91
Ischemic heart disease 1.61 1.38–1.87
Allcause mortality 1.46 1.39–1.53
Peripheral arterial disease 1.31 1.19–1.45
Odutayo A, Wong CX, Hsaio AJ, et al. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: systematic review and metaanalysis. BMJ 2016; DOI:10.1136/bmj.i4482
Atrial Fibrillation and Nonstroke Outcomes
Arrigo, Messina (Italy) 2016
RiskAdjusted InHospital Mortality After PCI
Multicenter registry Blue Cross Blue Shield of Michigan CV Consortium.
• Data for consecutive 113,283 PCI cases from 47 hospitals between 4/2011 and 12/2014.
• A history of AF was present in 13,912 patients (12%).
• Except in rare cases, patients were not taking oral anticoagulation at the time of PCI
• Patients with a history of AF were more likely to have inhospital complications, including inhospitalmortality (3% vs. 1%).
Sutton NR et al2016;68(9):895904.
Outcomes of Patients With Atrial Fibrillation Undergoing PCI
Arrigo, Messina (Italy) 2016
Multicenter registry Blue Cross Blue Shield of Michigan CV Consortium.
• Data for consecutive 113,283 PCI cases from 47 hospitals between 4/2011 and 12/2014.
• A history of AF was present in 13,912 patients (12%).
• Except in rare cases, patients were not taking oral anticoagulation at the time of PCI
• Patients with a history of AF were more likely to have inhospitalcomplications, including inhospital mortality (3% vs. 1%).
RiskAdjusted InHospital Mortality After PCISutton NR et al2016;68(9):895904.
Outcomes of Patients With Atrial Fibrillation Undergoing PCI
Arrigo, Messina (Italy) 2016
Sutton NR et al2016;68(9):895-904.
Outcomes of Patients With Atrial Fibrillation Undergoing PCI
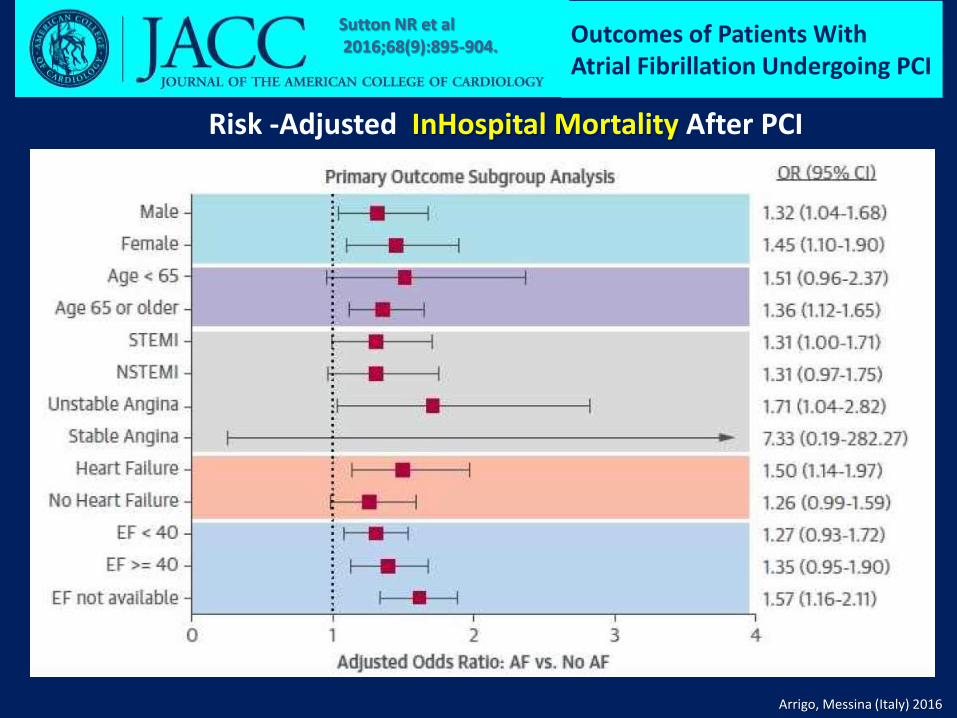
Risk -Adjusted InHospital Mortality After PCI
Arrigo, Messina (Italy) 2016
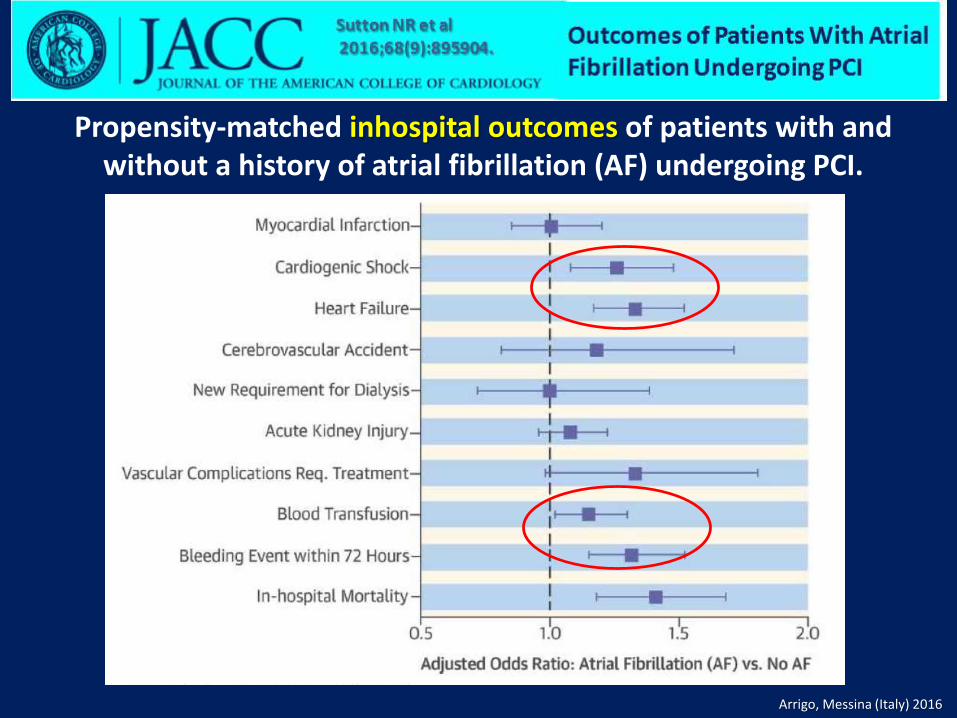
Propensity-matched inhospital outcomes of patients with and without a history of atrial fibrillation (AF) undergoing PCI.
Arrigo, Messina (Italy) 2016
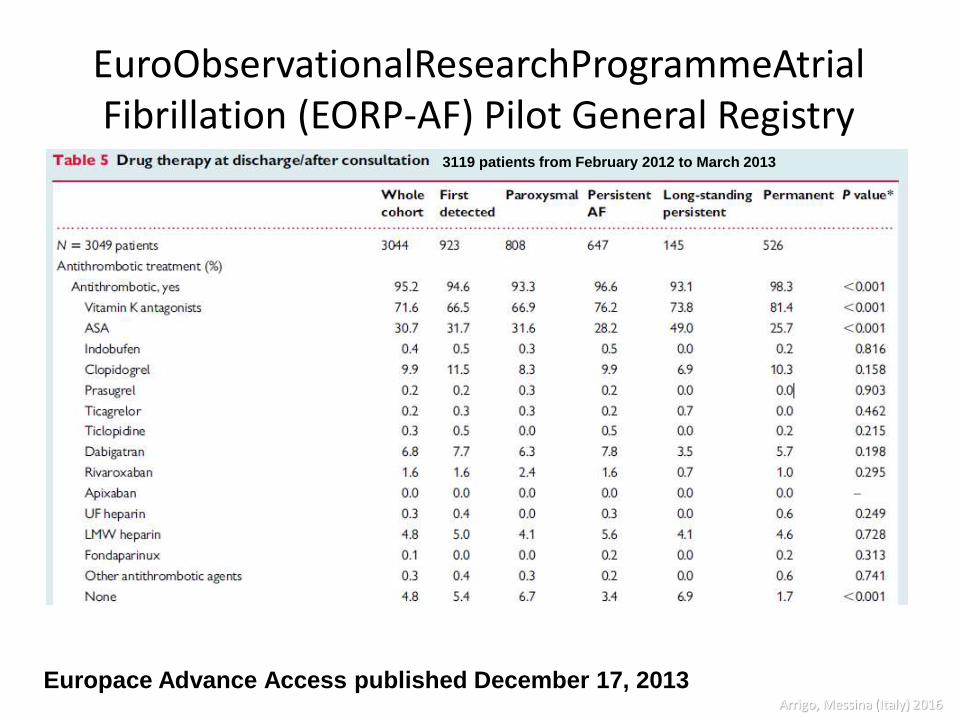
EuroObservationalResearchProgrammeAtrialFibrillation (EORP-AF) Pilot General Registry
Europace Advance Access published December 17, 2013
3119 patients from February 2012 to March 2013
Arrigo, Messina (Italy) 2016

Stent e fibrillazione atriale
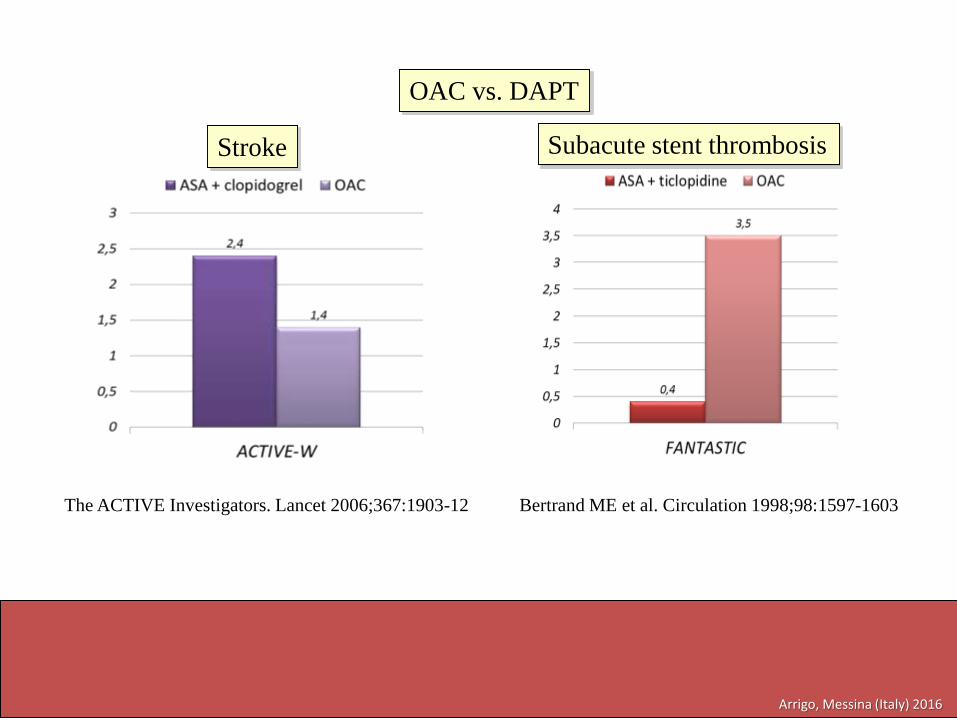
• Il trattamento più efficace per prevenire iltromboembolismo nella fibrillazione atriale è la Terapia Anticoagulante Orale (TAO).
• La terapia più efficace per prevenire la trombosi intrastent dopo PCI è la doppiaantiaggrezione piastrinica (DAPT) con aspirinae P2Y12 inibitori.
Arrigo, Messina (Italy) 2016
Go, A. S. et al. JAMA 2001;285:2370-2375.
OAC vs. DAPT
Stroke Subacute stent thrombosis
The ACTIVE Investigators. Lancet 2006;367:1903-12 Bertrand ME et al. Circulation 1998;98:1597-1603
Arrigo, Messina (Italy) 2016
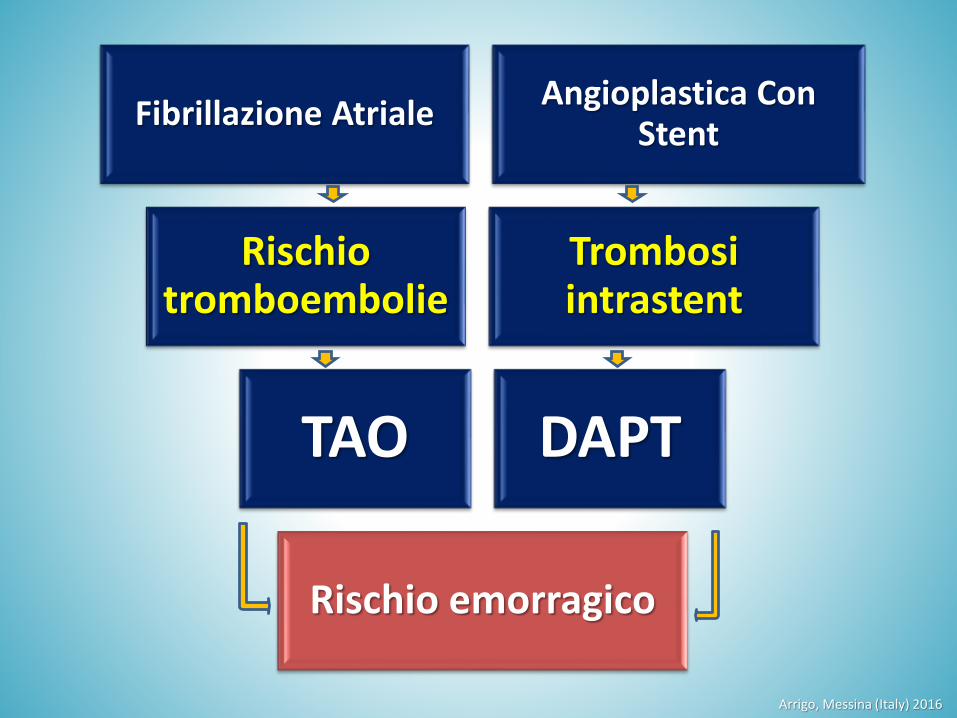
Fibrillazione AtrialeAngioplastica Con
Stent
Rischiotromboembolie
Trombosiintrastent
TAO DAPT
Rischio emorragico
Arrigo, Messina (Italy) 2016
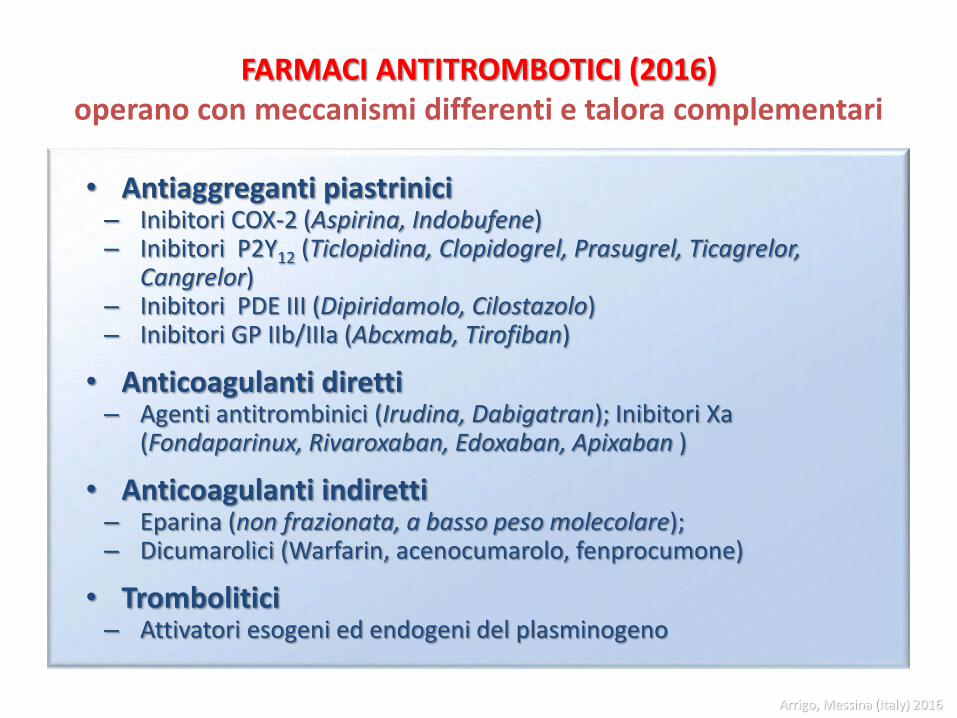
FARMACI ANTITROMBOTICI (2016)operano con meccanismi differenti e talora complementari
• Antiaggreganti piastrinici – Inibitori COX-2 (Aspirina, Indobufene)– Inibitori P2Y12 (Ticlopidina, Clopidogrel, Prasugrel, Ticagrelor,
Cangrelor)– Inibitori PDE III (Dipiridamolo, Cilostazolo) – Inibitori GP IIb/IIIa (Abcxmab, Tirofiban)
• Anticoagulanti diretti – Agenti antitrombinici (Irudina, Dabigatran); Inibitori Xa
(Fondaparinux, Rivaroxaban, Edoxaban, Apixaban )
• Anticoagulanti indiretti – Eparina (non frazionata, a basso peso molecolare);– Dicumarolici (Warfarin, acenocumarolo, fenprocumone)
• Trombolitici – Attivatori esogeni ed endogeni del plasminogeno
Arrigo, Messina (Italy) 2016
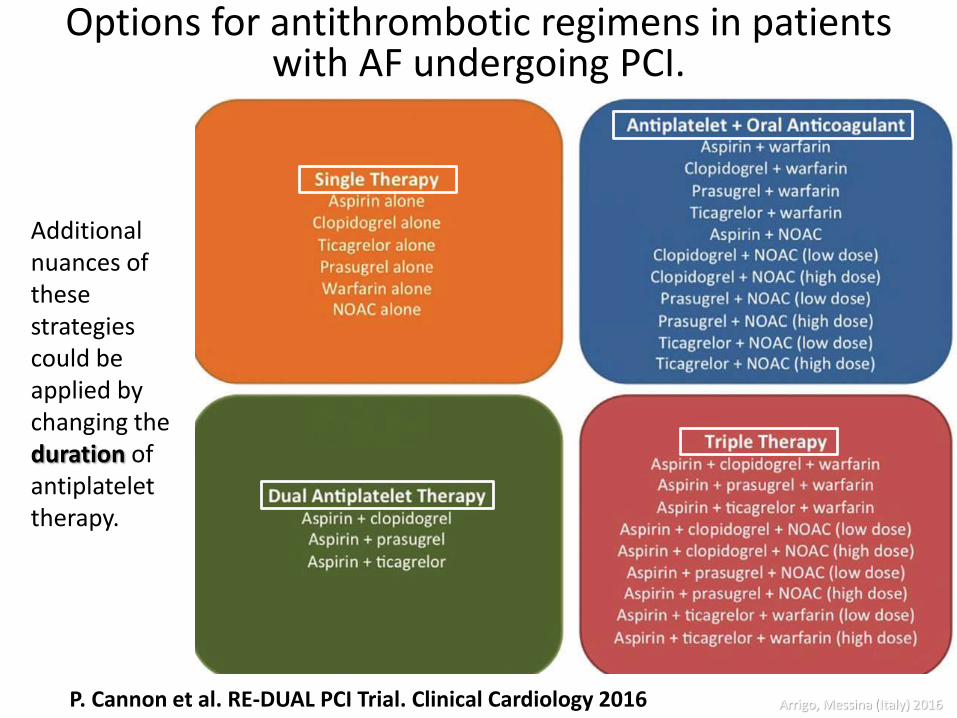
Options for antithrombotic regimens in patients with AF undergoing PCI.
P. Cannon et al. RE-DUAL PCI Trial. Clinical Cardiology 2016
Additional nuances of these strategies could be applied by changing the duration of antiplatelettherapy.
Arrigo, Messina (Italy) 2016
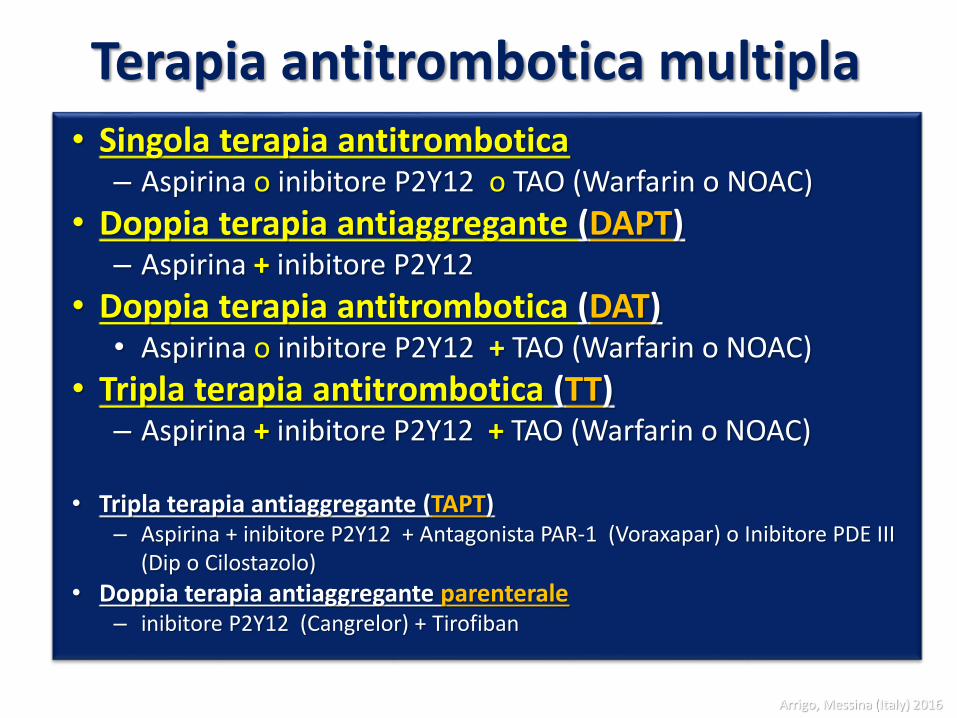
Terapia antitrombotica multipla• Singola terapia antitrombotica
– Aspirina o inibitore P2Y12 o TAO (Warfarin o NOAC)
• Doppia terapia antiaggregante (DAPT)– Aspirina + inibitore P2Y12
• Doppia terapia antitrombotica (DAT) • Aspirina o inibitore P2Y12 + TAO (Warfarin o NOAC)
• Tripla terapia antitrombotica (TT)– Aspirina + inibitore P2Y12 + TAO (Warfarin o NOAC)
• Tripla terapia antiaggregante (TAPT)– Aspirina + inibitore P2Y12 + Antagonista PAR-1 (Voraxapar) o Inibitore PDE III
(Dip o Cilostazolo)
• Doppia terapia antiaggregante parenterale– inibitore P2Y12 (Cangrelor) + Tirofiban
Arrigo, Messina (Italy) 2016
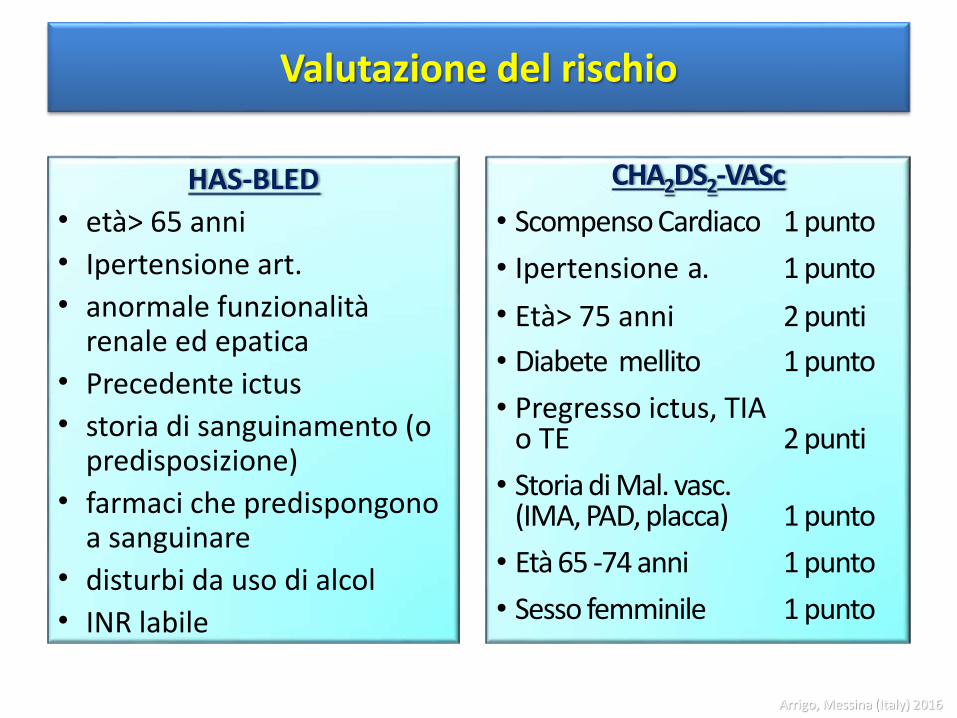
Valutazione del rischio
CHA2DS2-VASc
• Scompenso Cardiaco 1 punto
• Ipertensione a. 1 punto
• Età> 75 anni 2 punti
• Diabete mellito 1 punto
• Pregresso ictus, TIAo TE 2 punti
• Storia di Mal. vasc. (IMA, PAD, placca) 1 punto
• Età 65 -74 anni 1 punto
• Sesso femminile 1 punto
HAS-BLED
• età> 65 anni
• Ipertensione art.
• anormale funzionalità renale ed epatica
• Precedente ictus
• storia di sanguinamento (o predisposizione)
• farmaci che predispongono a sanguinare
• disturbi da uso di alcol
• INR labile
Arrigo, Messina (Italy) 2016
2014
Arrigo, Messina (Italy) 2016
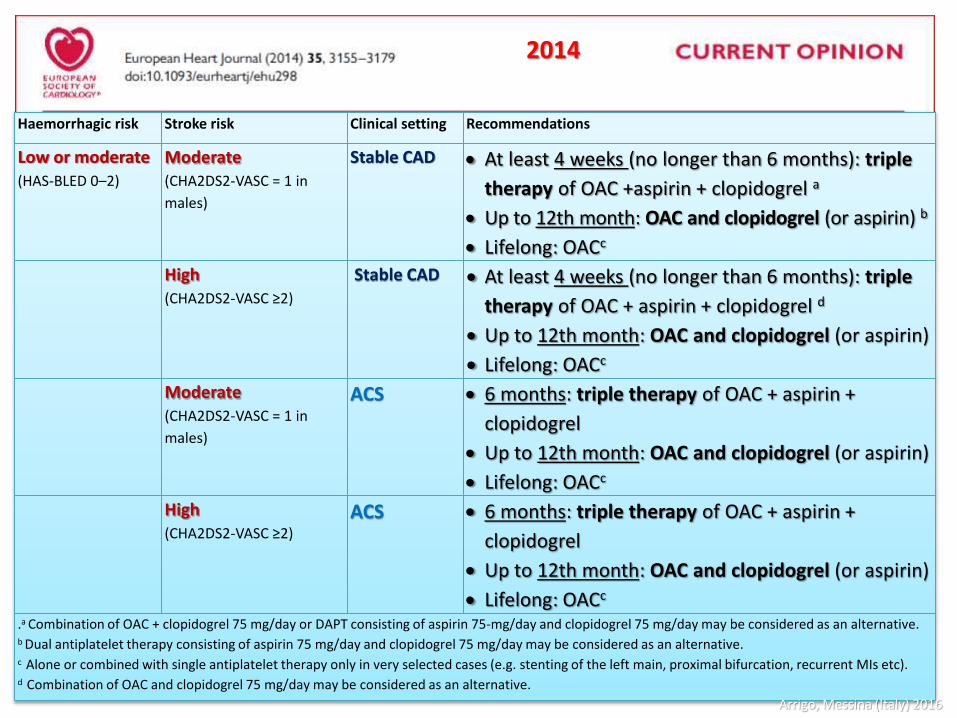
Haemorrhagic risk Stroke risk Clinical setting Recommendations
Low or moderate (HAS-BLED 0–2)
Moderate(CHA2DS2-VASC = 1 in
males)
Stable CAD At least 4 weeks (no longer than 6 months): triple
therapy of OAC +aspirin + clopidogrel a
Up to 12th month: OAC and clopidogrel (or aspirin) b
Lifelong: OACc
High (CHA2DS2-VASC ≥2)
Stable CAD At least 4 weeks (no longer than 6 months): triple
therapy of OAC + aspirin + clopidogrel d
Up to 12th month: OAC and clopidogrel (or aspirin)
Lifelong: OACc
Moderate (CHA2DS2-VASC = 1 in
males)
ACS 6 months: triple therapy of OAC + aspirin +
clopidogrel
Up to 12th month: OAC and clopidogrel (or aspirin)
Lifelong: OACc
High (CHA2DS2-VASC ≥2)
ACS 6 months: triple therapy of OAC + aspirin +
clopidogrel
Up to 12th month: OAC and clopidogrel (or aspirin)
Lifelong: OACc
.a Combination of OAC + clopidogrel 75 mg/day or DAPT consisting of aspirin 75-mg/day and clopidogrel 75 mg/day may be considered as an alternative.b Dual antiplatelet therapy consisting of aspirin 75 mg/day and clopidogrel 75 mg/day may be considered as an alternative.c Alone or combined with single antiplatelet therapy only in very selected cases (e.g. stenting of the left main, proximal bifurcation, recurrent MIs etc).d Combination of OAC and clopidogrel 75 mg/day may be considered as an alternative.
2014
Arrigo, Messina (Italy) 2016
7. TheACStrialswere underpowered to demonstrate a reduction in stroke risk by usingNOACsincombination with (dual) antiplatelet therapy in non-AF patients.
8. Given the absence of new data from RCTs and the outcome data coming from‘real-world’ registries, it appears questionable to consider the potential risk of MI as a criterion for selecting the most appropriate NOAC agent in a patient with non-valvular AF. The available data do not suggest that there is a need to switch patients on dabigatran to one of the other NOACs in the event of an ACS developing in a patient with AF.
9. Conversely, in an ACS patient who develops new onset AF, and is at high stroke risk,OACshould be started, whether with a VKA or NOAC. Limited data suggest that use of the new P2Y12 inhibitors would increase the risk of major bleeding, and thus, clopidogrel would be the preferred P2Y12 inhibitor.
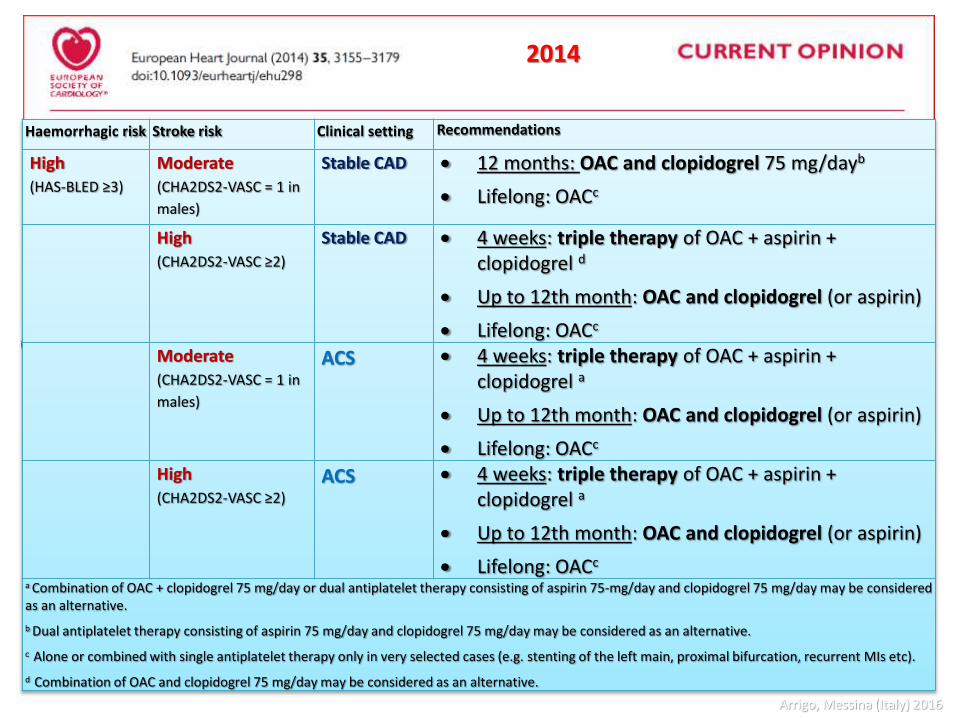
Haemorrhagic risk Stroke risk Clinical setting Recommendations
High (HAS-BLED ≥3)
Moderate (CHA2DS2-VASC = 1 in
males)
Stable CAD 12 months: OAC and clopidogrel 75 mg/dayb
Lifelong: OACc
High (CHA2DS2-VASC ≥2)
Stable CAD 4 weeks: triple therapy of OAC + aspirin + clopidogrel d
Up to 12th month: OAC and clopidogrel (or aspirin)
Lifelong: OACc
Moderate (CHA2DS2-VASC = 1 in
males)
ACS 4 weeks: triple therapy of OAC + aspirin + clopidogrel a
Up to 12th month: OAC and clopidogrel (or aspirin)
Lifelong: OACc
High (CHA2DS2-VASC ≥2)
ACS 4 weeks: triple therapy of OAC + aspirin + clopidogrel a
Up to 12th month: OAC and clopidogrel (or aspirin)
Lifelong: OACc
a Combination of OAC + clopidogrel 75 mg/day or dual antiplatelet therapy consisting of aspirin 75-mg/day and clopidogrel 75 mg/day may be considered as an alternative.
b Dual antiplatelet therapy consisting of aspirin 75 mg/day and clopidogrel 75 mg/day may be considered as an alternative.
c Alone or combined with single antiplatelet therapy only in very selected cases (e.g. stenting of the left main, proximal bifurcation, recurrent MIs etc).
d Combination of OAC and clopidogrel 75 mg/day may be considered as an alternative.
2014
Arrigo, Messina (Italy) 2016
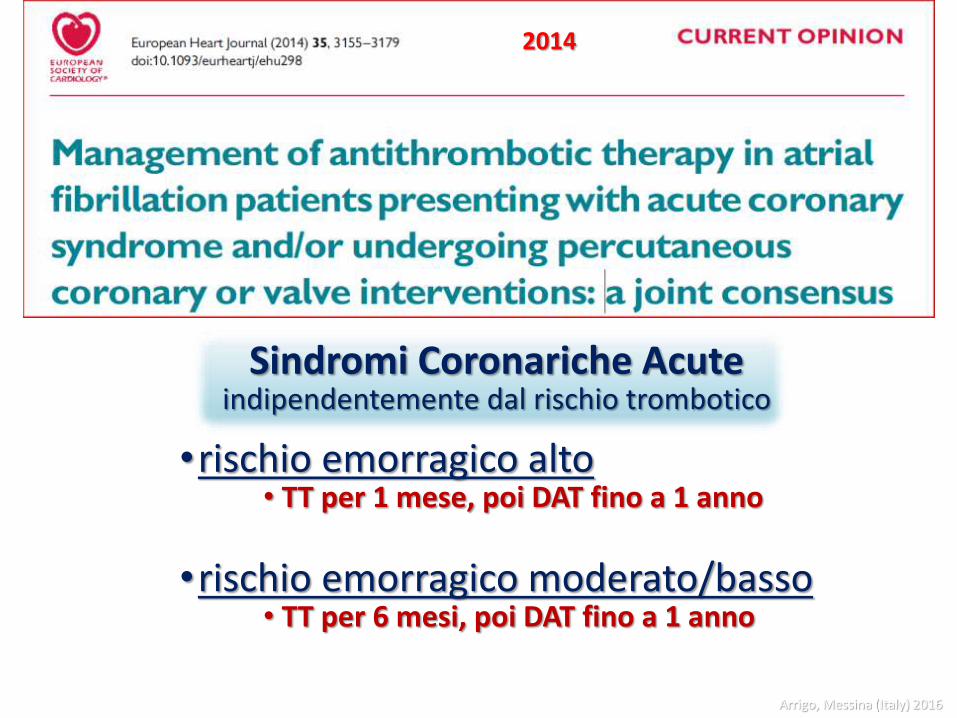
•rischio emorragico alto• TT per 1 mese, poi DAT fino a 1 anno
•rischio emorragico moderato/basso• TT per 6 mesi, poi DAT fino a 1 anno
Sindromi Coronariche Acuteindipendentemente dal rischio trombotico
2014
Arrigo, Messina (Italy) 2016
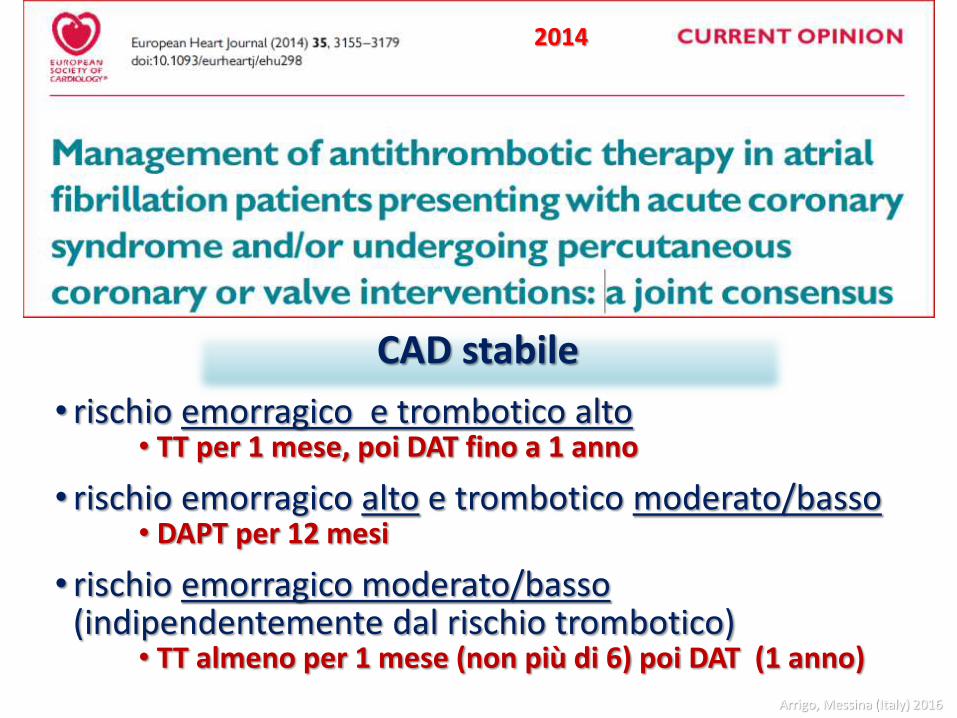
• rischio emorragico e trombotico alto• TT per 1 mese, poi DAT fino a 1 anno
• rischio emorragico alto e trombotico moderato/basso• DAPT per 12 mesi
• rischio emorragico moderato/basso(indipendentemente dal rischio trombotico)
• TT almeno per 1 mese (non più di 6) poi DAT (1 anno)
CAD stabile
2014
Arrigo, Messina (Italy) 2016
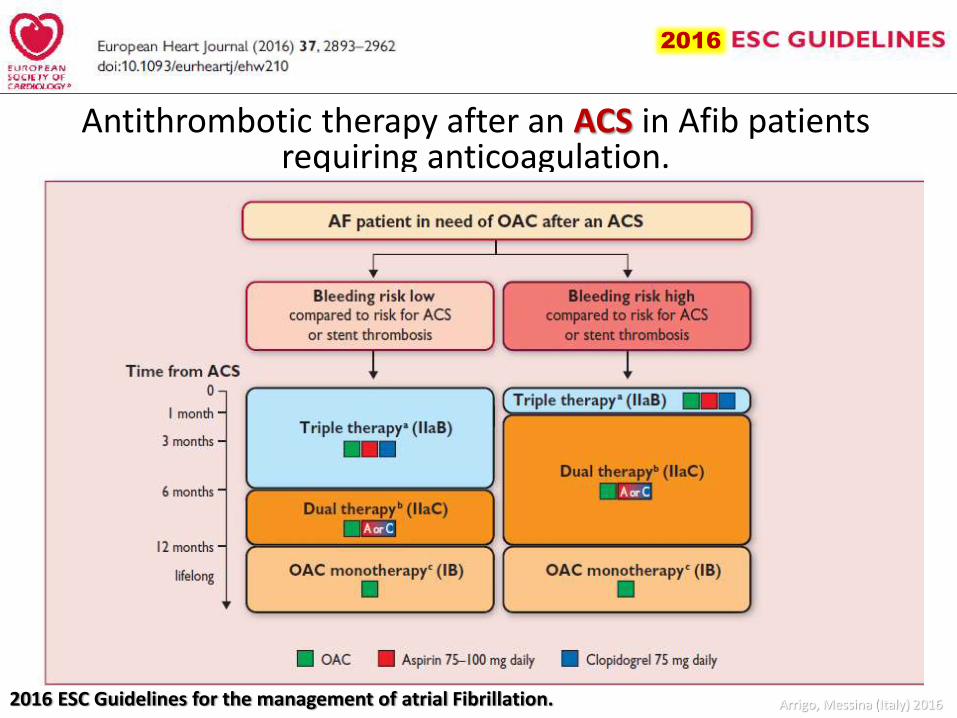
Antithrombotic therapy after an ACS in Afib patients requiring anticoagulation.
2016
2016 ESC Guidelines for the management of atrial Fibrillation. Arrigo, Messina (Italy) 2016
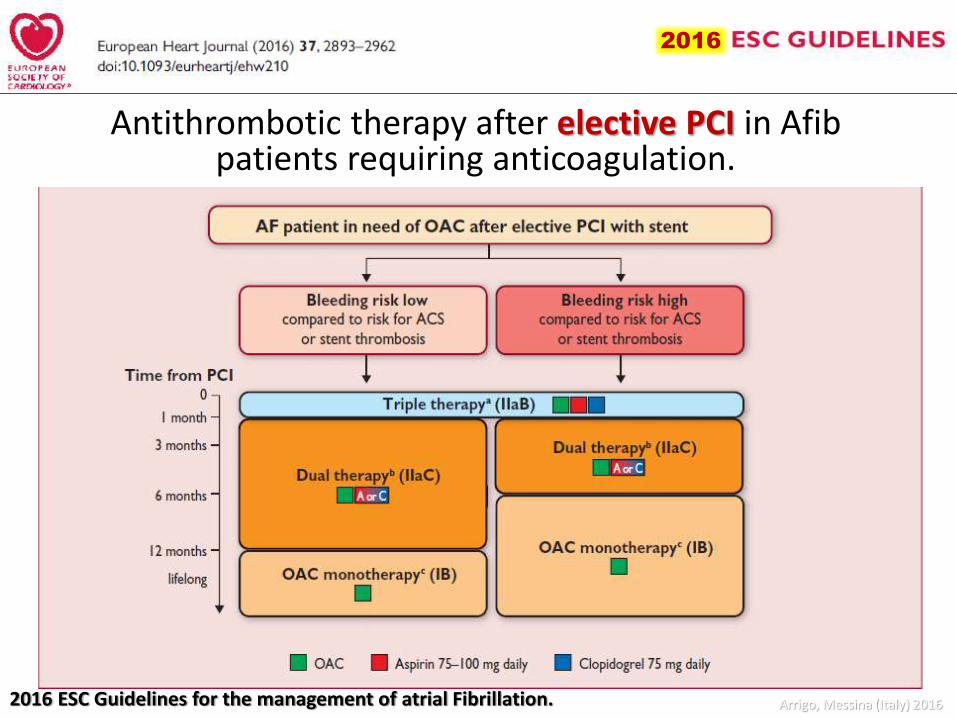
Antithrombotic therapy after elective PCI in Afibpatients requiring anticoagulation.
20162016
2016 ESC Guidelines for the management of atrial Fibrillation. Arrigo, Messina (Italy) 2016
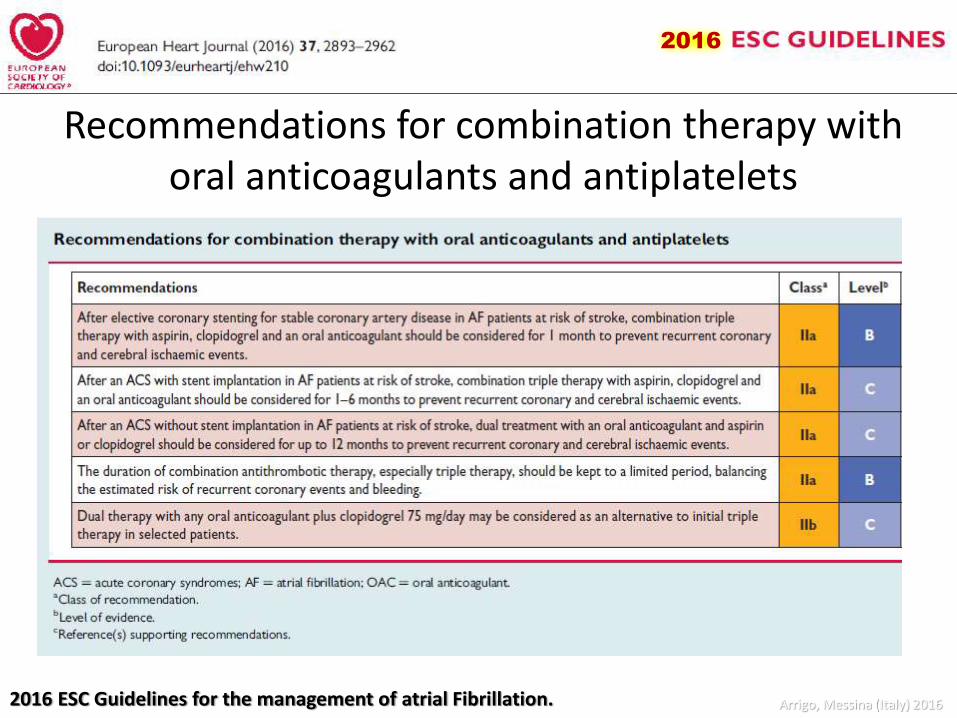
Recommendations for combination therapy with oral anticoagulants and antiplatelets
2016
2016 ESC Guidelines for the management of atrial Fibrillation. Arrigo, Messina (Italy) 2016
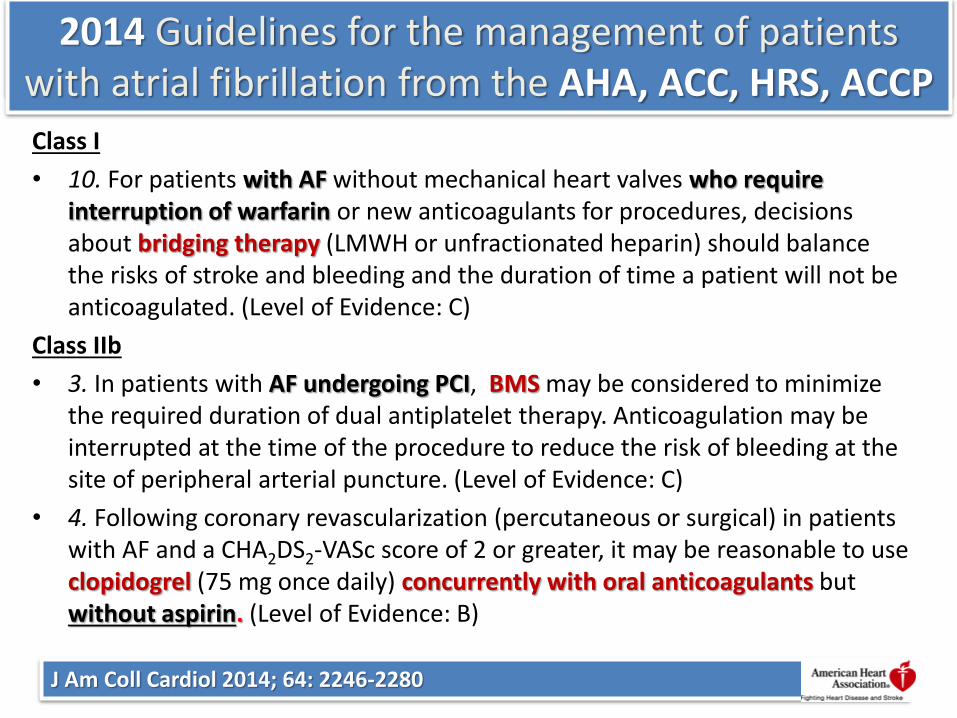
2014 Guidelines from the AHA, ACC, HRS, ACCP
J Am Coll Cardiol 2014; 64: 2246-2280
Class I
• 10. For patients with AF without mechanical heart valves who require interruption of warfarin or new anticoagulants for procedures, decisions about bridging therapy (LMWH or unfractionated heparin) should balance the risks of stroke and bleeding and the duration of time a patient will not be anticoagulated. (Level of Evidence: C)
Class IIb
• 3. In patients with AF undergoing PCI, BMS may be considered to minimize the required duration of dual antiplatelet therapy. Anticoagulation may be interrupted at the time of the procedure to reduce the risk of bleeding at the site of peripheral arterial puncture. (Level of Evidence: C)
• 4. Following coronary revascularization (percutaneous or surgical) in patients with AF and a CHA2DS2-VASc score of 2 or greater, it may be reasonable to use clopidogrel (75 mg once daily) concurrently with oral anticoagulants but without aspirin. (Level of Evidence: B)
2014 Guidelines for the management of patients with atrial fibrillation from the AHA, ACC, HRS, ACCP
Stephen Rechenmacher e James Fang dell’Utah Health Sciences
Center in una ampia review pubblicata sul JACC del 22 settembre, in cui si definiscono tre principi
fondamentali:
•Bridging procedure
Rechenmacher S, Fang J. J Am Coll Cardiol 2015;66:1392–403Arrigo, Messina (Italy) 2016
Bridging procedurereview in cui si definiscono tre principi fondamentali:
• la TAO non deve essere interrotta nelle procedure a basso rischio emorragico
• la bridging therapy non deve mai essere proposta nei pazienti a basso rischio di eventi tromboembolici
• la bridging therapy deve essere limitata ai casi ad alto rischio tromboembolico (TE) e rischio emorragico basso o intermedio
Rechenmacher S, Fang J. J Am Coll Cardiol 2015;66:1392–403Arrigo, Messina (Italy) 2016
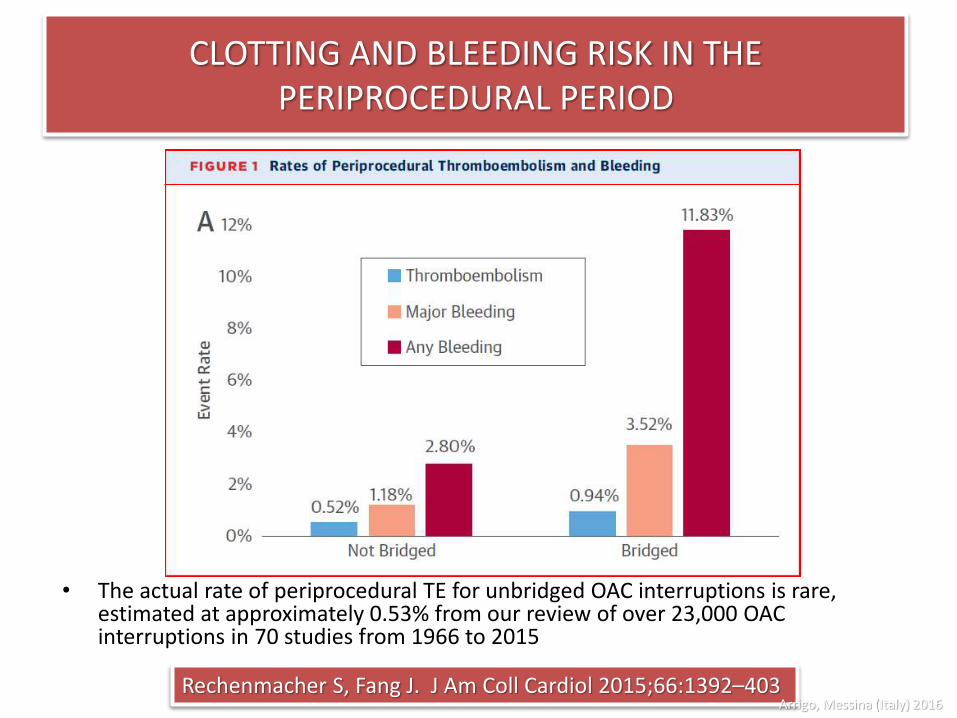
Rechenmacher S, Fang J. J Am Coll Cardiol 2015;66:1392–403
• The actual rate of periprocedural TE for unbridged OAC interruptions is rare, estimated at approximately 0.53% from our review of over 23,000 OACinterruptions in 70 studies from 1966 to 2015
CLOTTING AND BLEEDING RISK IN THE PERIPROCEDURAL PERIOD
Arrigo, Messina (Italy) 2016
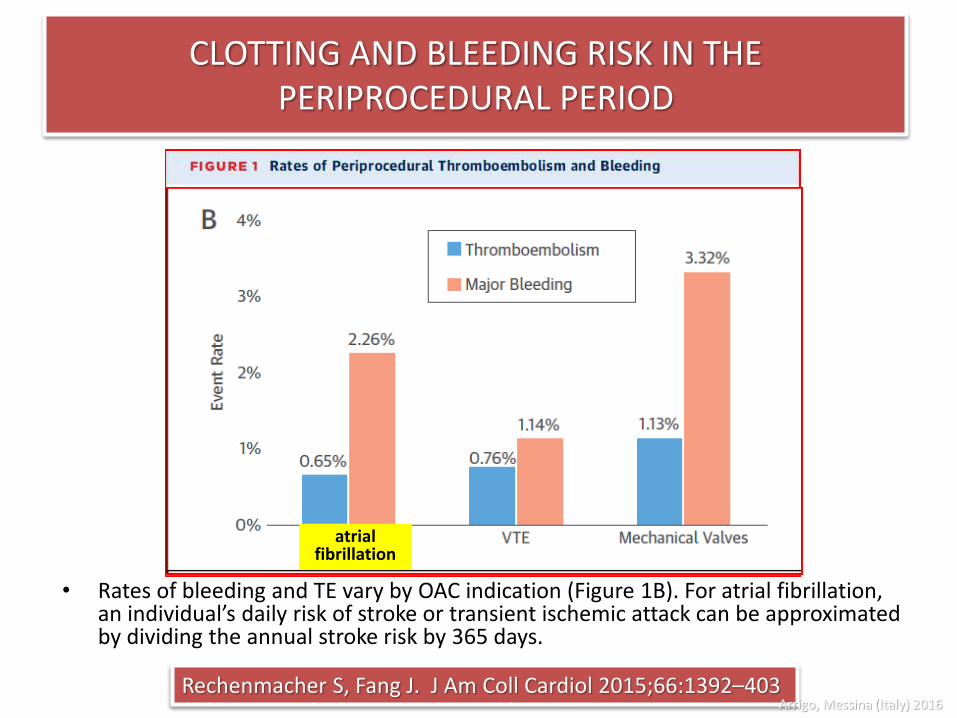
Rechenmacher S, Fang J. J Am Coll Cardiol 2015;66:1392–403
• Rates of bleeding and TE vary by OAC indication (Figure 1B). For atrial fibrillation, an individual’s daily risk of stroke or transient ischemic attack can be approximated by dividing the annual stroke risk by 365 days.
CLOTTING AND BLEEDING RISK IN THE PERIPROCEDURAL PERIOD
atrialfibrillation
Arrigo, Messina (Italy) 2016

Trials e registri
Stent e fibrillazione atriale
Arrigo, Messina (Italy) 2016
Isar TRIPLE TT 6 sett vs 6 mesiWOEST non aspirinaSambola A TT vs DT nell’anzianoThe ROCKET AF Trial (NOAC)The ACTION Registry–GWTG TT vs DAPT
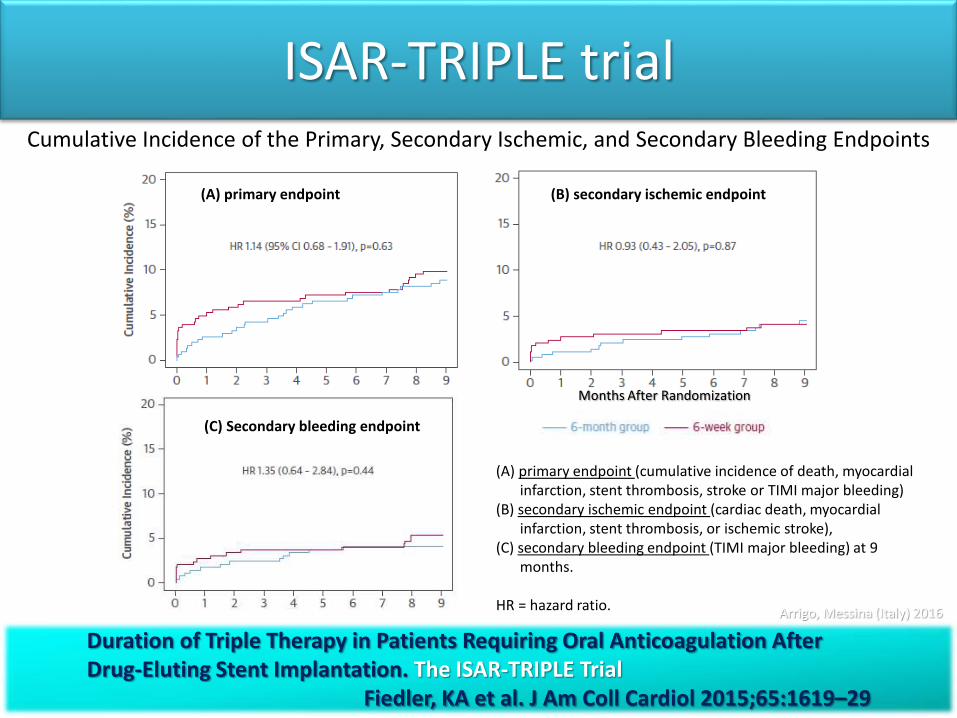
ISAR-TRIPLE trial
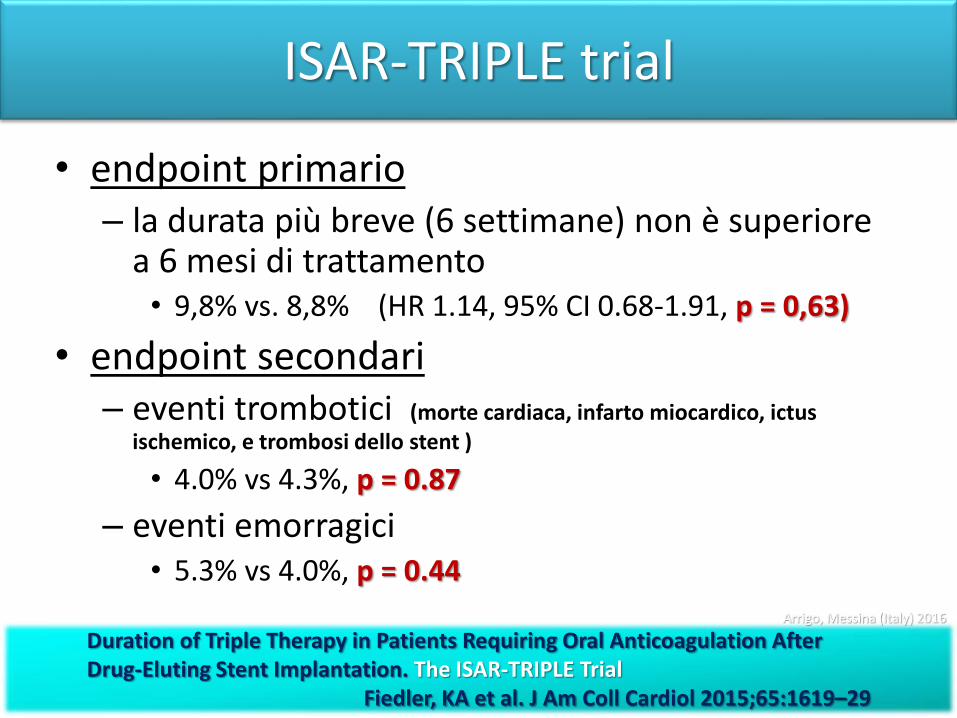
• endpoint primario – la durata più breve (6 settimane) non è superiore
a 6 mesi di trattamento• 9,8% vs. 8,8% (HR 1.14, 95% CI 0.68-1.91, p = 0,63)
• endpoint secondari– eventi trombotici (morte cardiaca, infarto miocardico, ictus
ischemico, e trombosi dello stent )
• 4.0% vs 4.3%, p = 0.87
– eventi emorragici • 5.3% vs 4.0%, p = 0.44
Duration of Triple Therapy in Patients Requiring Oral Anticoagulation After Drug-Eluting Stent Implantation. The ISAR-TRIPLE Trial
Fiedler, KA et al. J Am Coll Cardiol 2015;65:1619–29
Arrigo, Messina (Italy) 2016
ISAR-TRIPLE trial
Duration of Triple Therapy in Patients Requiring Oral Anticoagulation After Drug-Eluting Stent Implantation. The ISAR-TRIPLE Trial
Fiedler, KA et al. J Am Coll Cardiol 2015;65:1619–29
Cumulative Incidence of the Primary, Secondary Ischemic, and Secondary Bleeding Endpoints
(A) primary endpoint (B) secondary ischemic endpoint
(C) Secondary bleeding endpoint
(A) primary endpoint (cumulative incidence of death, myocardial infarction, stent thrombosis, stroke or TIMI major bleeding)
(B) secondary ischemic endpoint (cardiac death, myocardial infarction, stent thrombosis, or ischemic stroke),
(C) secondary bleeding endpoint (TIMI major bleeding) at 9 months.
HR = hazard ratio.
Months After Randomization
Arrigo, Messina (Italy) 2016
Arrigo, Messina (Italy) 2016
Go, A. S. et al. JAMA 2001;285:2370-2375.
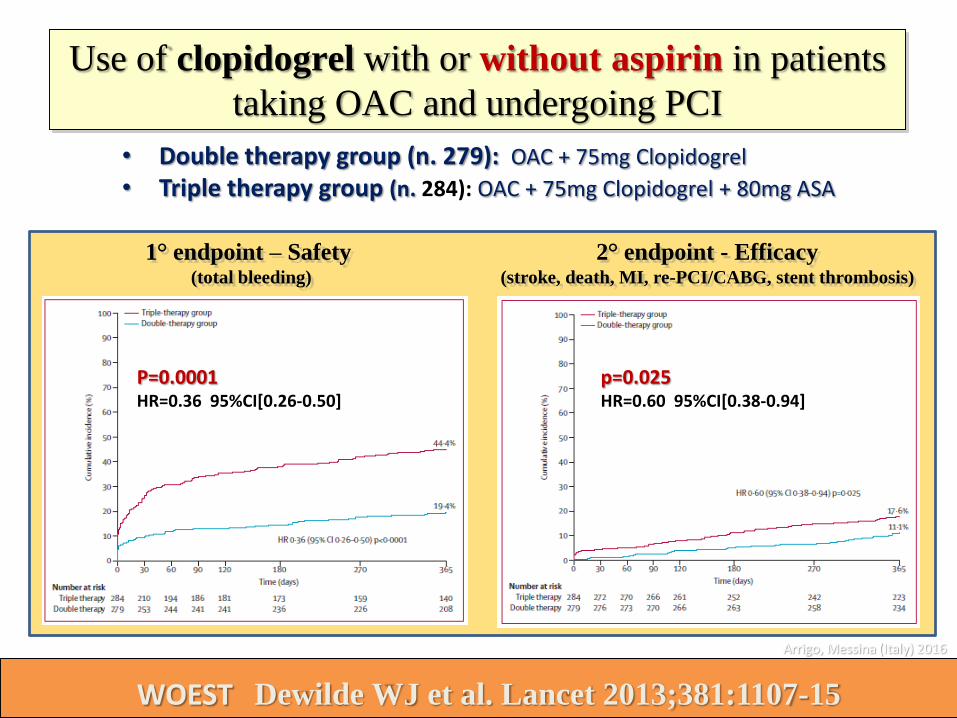
Use of clopidogrel with or without aspirin in patients
taking OAC and undergoing PCI
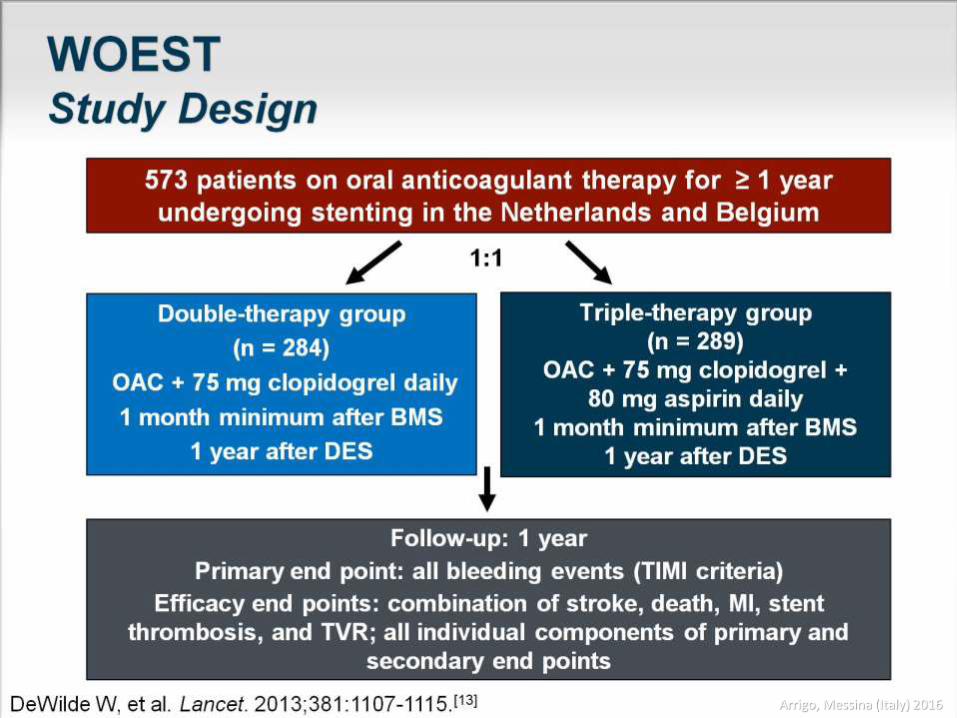
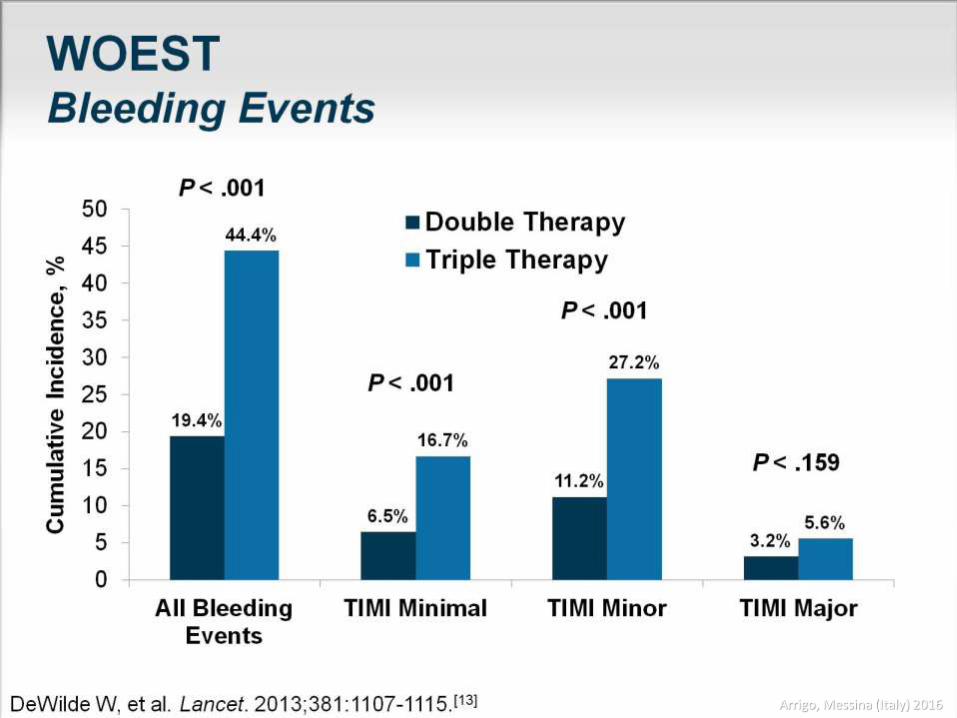
WOEST Dewilde WJ et al. Lancet 2013;381:1107-15
1° endpoint – Safety (total bleeding)
2° endpoint - Efficacy(stroke, death, MI, re-PCI/CABG, stent thrombosis)
• Double therapy group (n. 279): OAC + 75mg Clopidogrel
• Triple therapy group (n. 284): OAC + 75mg Clopidogrel + 80mg ASA
P=0.0001HR=0.36 95%CI[0.26-0.50]
p=0.025HR=0.60 95%CI[0.38-0.94]
Arrigo, Messina (Italy) 2016
Arrigo, Messina (Italy) 2016
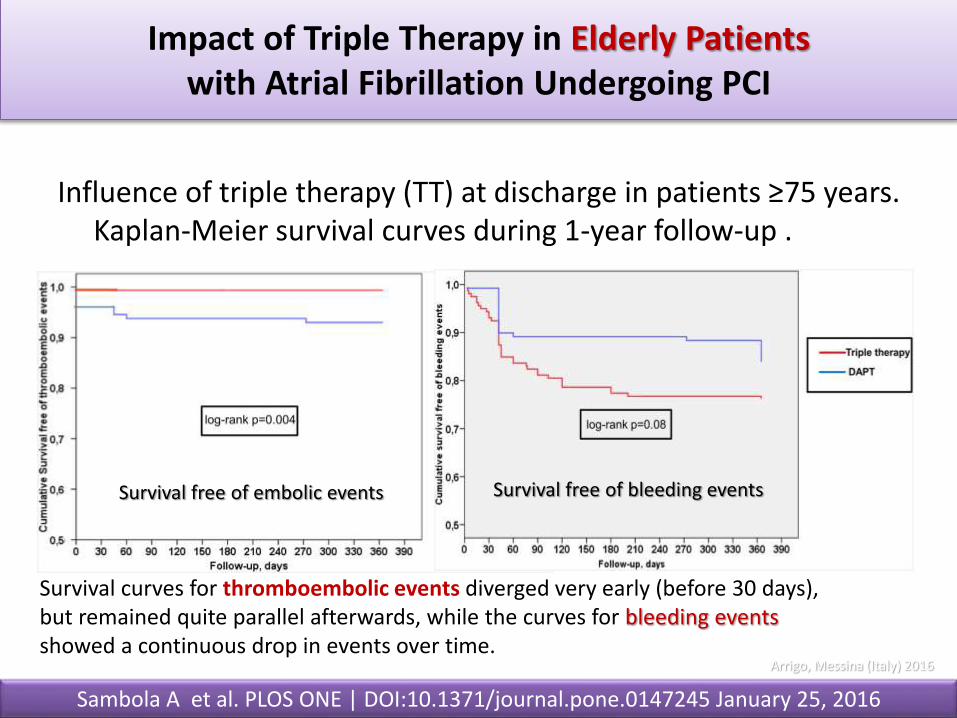
Impact of Triple Therapy in Elderly Patientswith Atrial Fibrillation Undergoing PCI
Sambola A et al. PLOS ONE | DOI:10.1371/journal.pone.0147245 January 25, 2016
Influence of triple therapy (TT) at discharge in patients ≥75 years. Kaplan-Meier survival curves during 1-year follow-up .
Survival free of embolic events Survival free of bleeding events
Survival curves for thromboembolic events diverged very early (before 30 days), but remained quite parallel afterwards, while the curves for bleeding events showed a continuous drop in events over time.
Arrigo, Messina (Italy) 2016
.
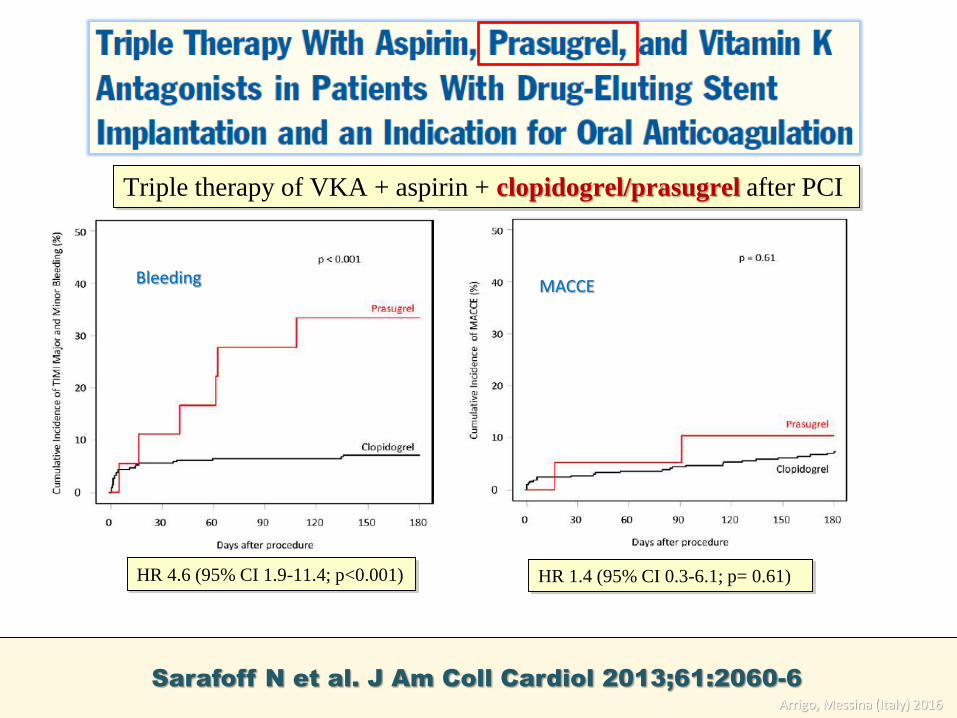
Sarafoff N et al. J Am Coll Cardiol 2013;61:2060-6
HR 1.4 (95% CI 0.3-6.1; p= 0.61)HR 4.6 (95% CI 1.9-11.4; p<0.001)
Triple therapy of VKA + aspirin + clopidogrel/prasugrel after PCI
BleedingBleeding MACCE
Arrigo, Messina (Italy) 2016
• Treatment group of the ROCKET AF trial (Rivaroxabancompared with VKA).
• 153 patients (1.1%) underwent PCI during a median 806 days of follow-up.
• Study drug was continued during PCI in 81% of patients.
Arrigo, Messina (Italy) 2016
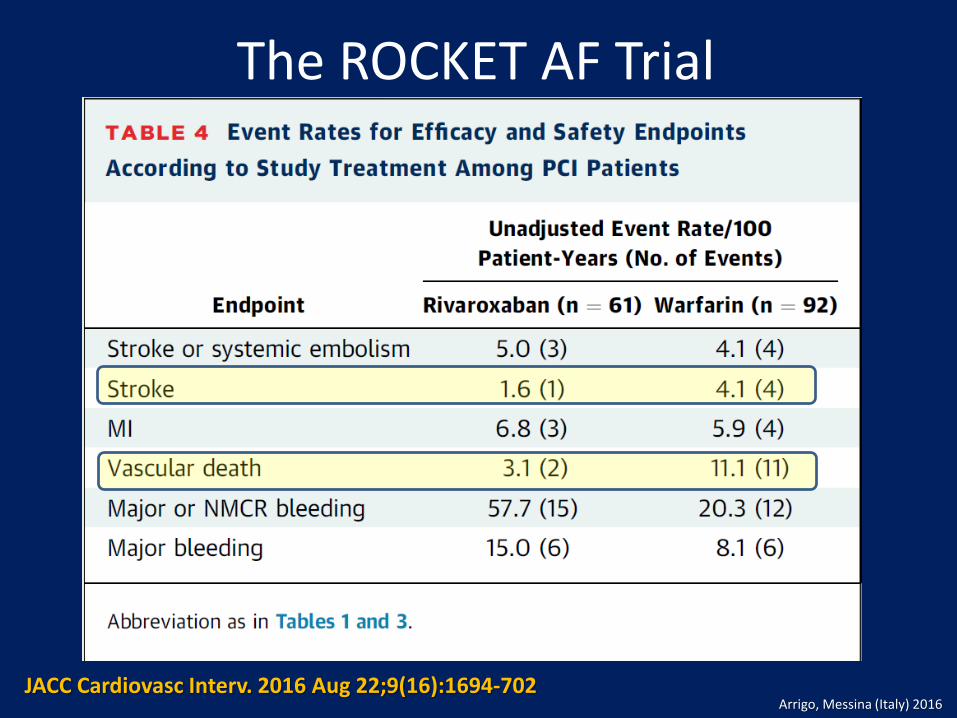
The ROCKET AF Trial
JACC Cardiovasc Interv. 2016 Aug 22;9(16):1694-702Arrigo, Messina (Italy) 2016
Triple Therapy Among Older Pts With AMI and AF. The ACTION Registry–GWTG
• The ACTION Registry–GWTG is a national quality improvement registry capturing data on consecutive MI patients treated at >500 hospitals in the United States.
• Among 4,959 MI patients presenting with a history of AF who were treated with PCI, 27.6% (n = 1,370) were discharged on triple therapy (warfarin + DAPT), and 72.4% (n = 3,589) were discharged on DAPT (aspirin and a P2Y12antagonist)
Hess, C.N. et al. J Am Coll Cardiol. 2015; 66(6):616–27. Arrigo, Messina (Italy) 2016
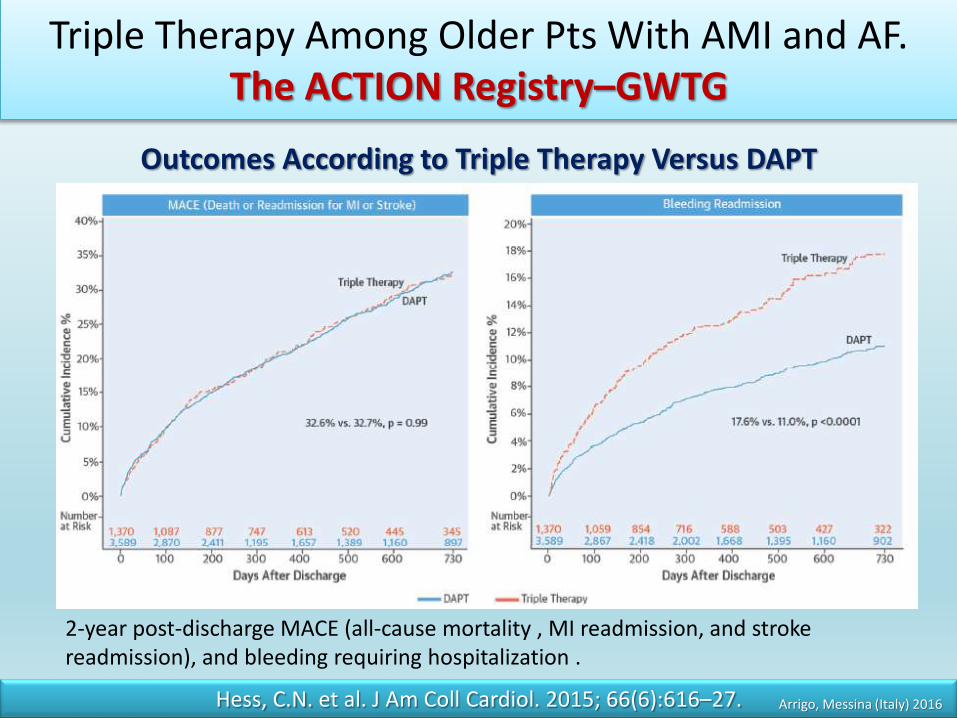
Triple Therapy Among Older Pts With AMI and AF. The ACTION Registry–GWTG
Hess, C.N. et al. J Am Coll Cardiol. 2015; 66(6):616–27.
Outcomes According to Triple Therapy Versus DAPT
2-year post-discharge MACE (all-cause mortality , MI readmission, and stroke readmission), and bleeding requiring hospitalization .
Arrigo, Messina (Italy) 2016
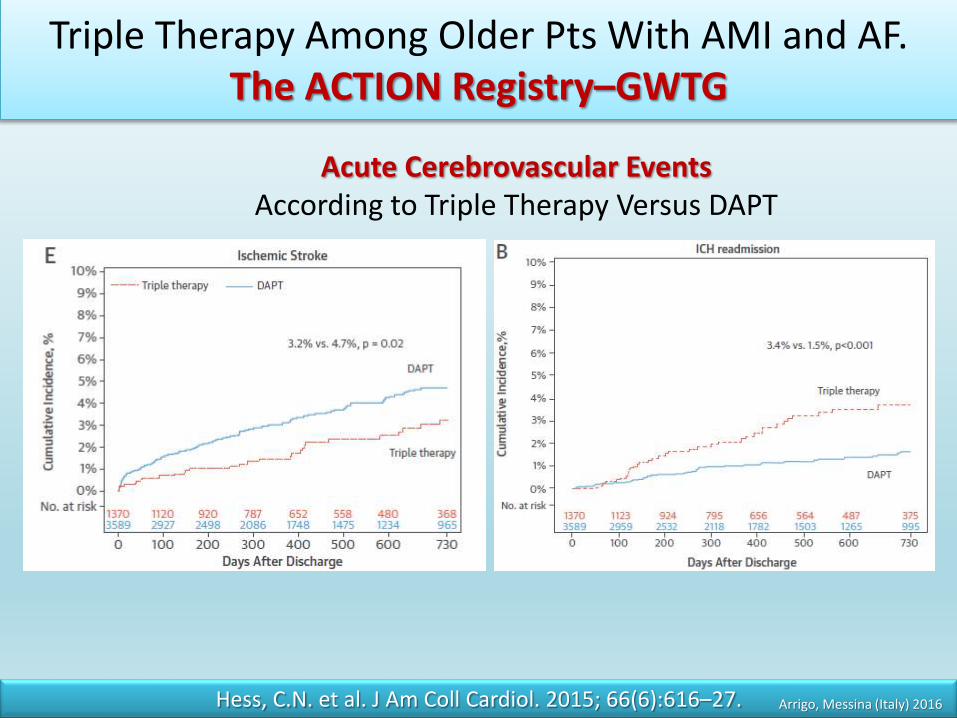
Triple Therapy Among Older Pts With AMI and AF. The ACTION Registry–GWTG
Hess, C.N. et al. J Am Coll Cardiol. 2015; 66(6):616–27.
Acute Cerebrovascular Events According to Triple Therapy Versus DAPT
Arrigo, Messina (Italy) 2016
Bleeding in atrial fibrillation patients following myocardial infarction and coronary intervention: a nationwide cohort study
• Subjects with AF hospitalized for Myocardial Infarction (n. 8775 - 76.4%) or PCI (n. 2705 - 23.6%).
• 1521 (17.3%) patients of the group with MI had a PCI performed within 1 week.
• Inclusion criteria were ongoing antithrombotic treatment in subjects alive 7 days after discharge, and no registration with diagnosis of bleeding, MI or ischemic stroke during the quarantine period.
Lamberts M et al. Circulation 2012;126:1185–1193
Nationwide registries in Denmark 2001 - 2009
Arrigo, Messina (Italy) 2016
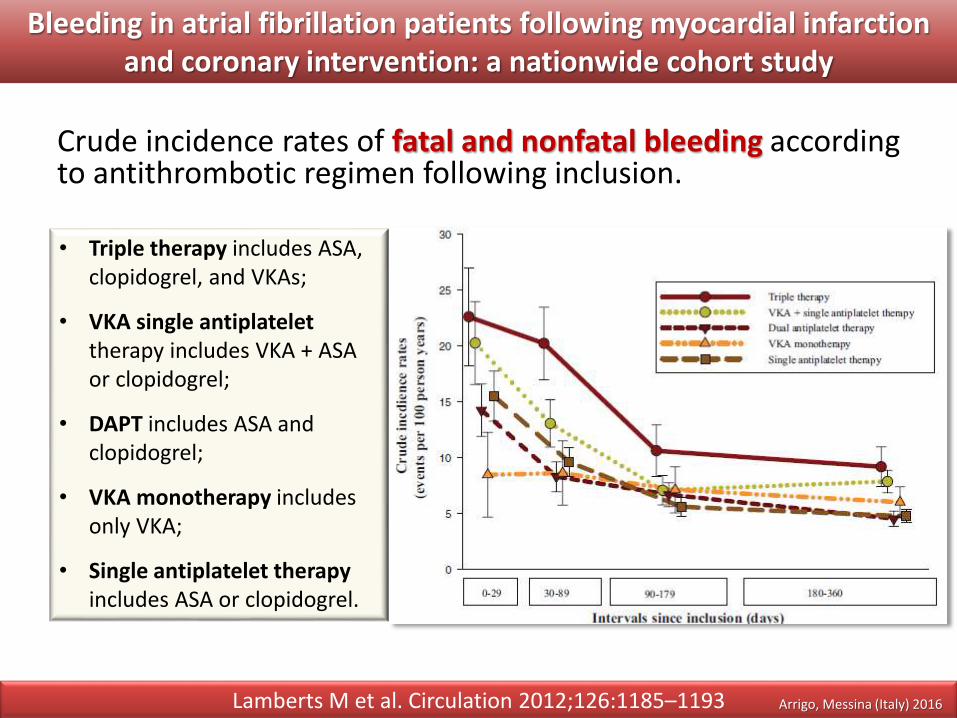
Bleeding in atrial fibrillation patients following myocardial infarction and coronary intervention: a nationwide cohort study
Crude incidence rates of fatal and nonfatal bleeding according to antithrombotic regimen following inclusion.
Lamberts M et al. Circulation 2012;126:1185–1193
• Triple therapy includes ASA, clopidogrel, and VKAs;
• VKA single antiplatelettherapy includes VKA + ASA or clopidogrel;
• DAPT includes ASA and clopidogrel;
• VKA monotherapy includes only VKA;
• Single antiplatelet therapyincludes ASA or clopidogrel.
Arrigo, Messina (Italy) 2016
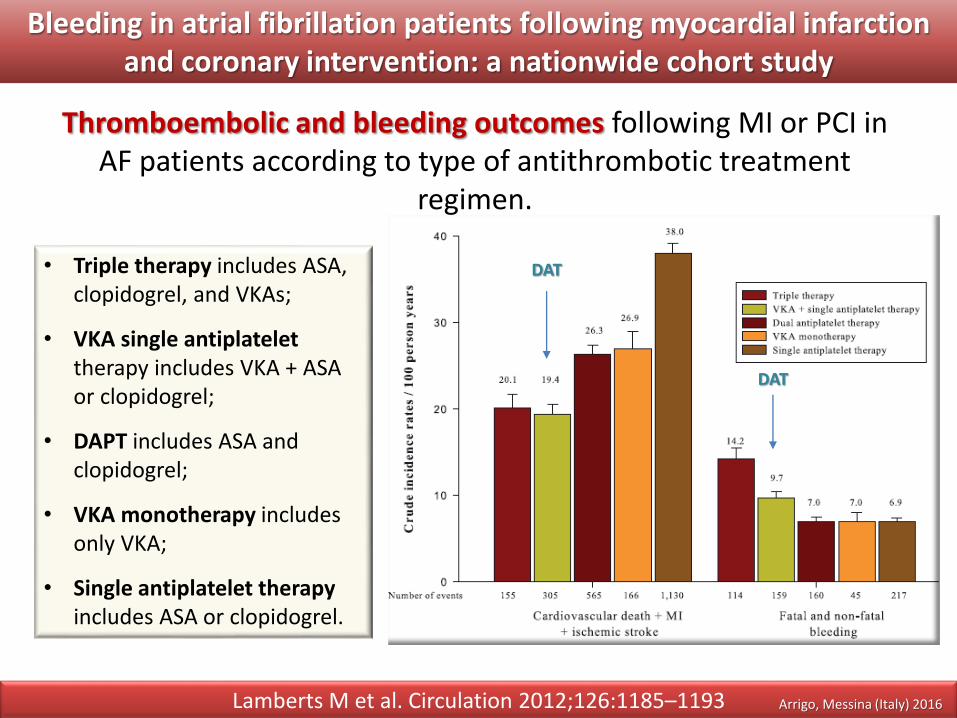
Bleeding in atrial fibrillation patients following myocardial infarction and coronary intervention: a nationwide cohort study
Thromboembolic and bleeding outcomes following MI or PCI in AF patients according to type of antithrombotic treatment
regimen.
Lamberts M et al. Circulation 2012;126:1185–1193
• Triple therapy includes ASA, clopidogrel, and VKAs;
• VKA single antiplatelettherapy includes VKA + ASA or clopidogrel;
• DAPT includes ASA and clopidogrel;
• VKA monotherapy includes only VKA;
• Single antiplatelet therapyincludes ASA or clopidogrel.
DAT
DAT
Arrigo, Messina (Italy) 2016
Arrigo, Messina (Italy) 2016
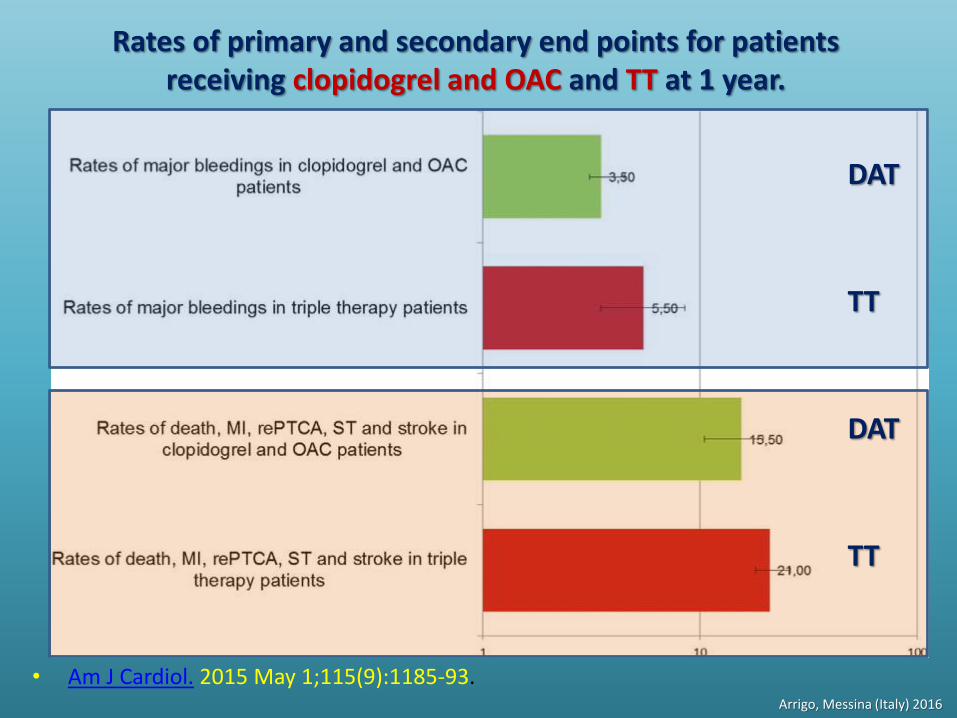
Rates of primary and secondary end points for patients receiving clopidogrel and OAC and TT at 1 year.
• Am J Cardiol. 2015 May 1;115(9):1185-93.
TT
TT
DAT
DAT
Arrigo, Messina (Italy) 2016
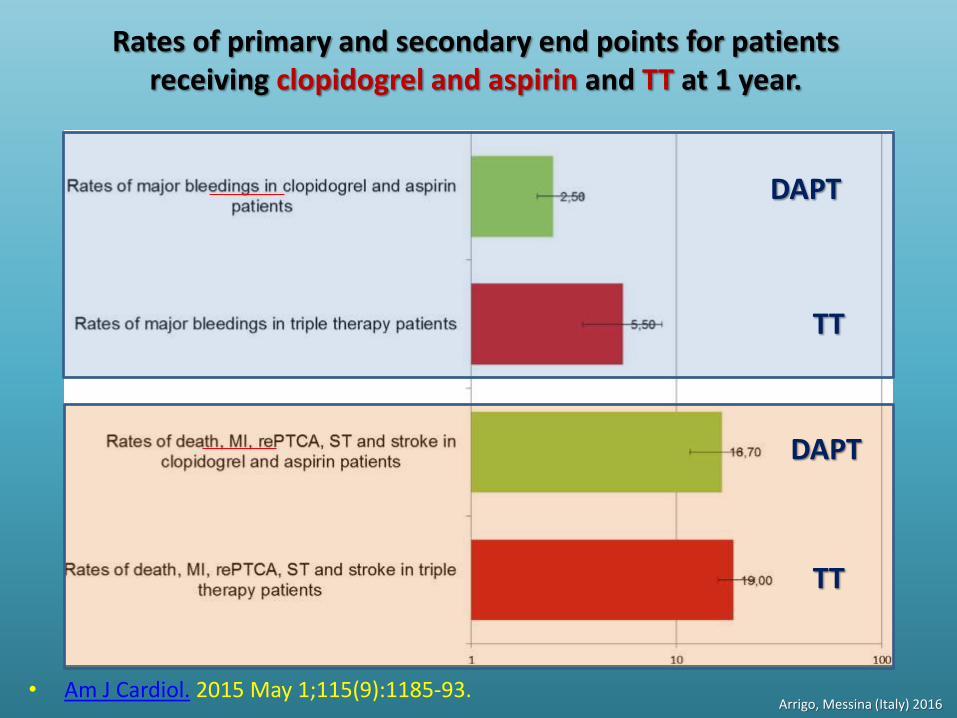
Rates of primary and secondary end points for patients receiving clopidogrel and aspirin and TT at 1 year.
• Am J Cardiol. 2015 May 1;115(9):1185-93.
TT
TT
DAPT
DAPT
Arrigo, Messina (Italy) 2016
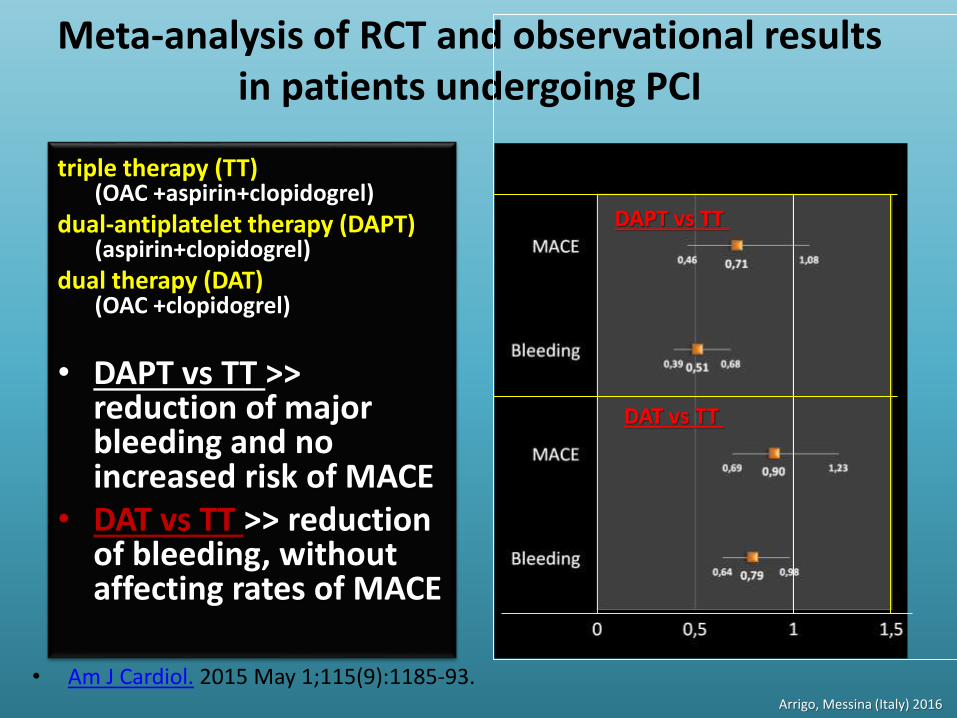
Meta-analysis of RCT and observational results in patients undergoing PCI
triple therapy (TT)(OAC +aspirin+clopidogrel)
dual-antiplatelet therapy (DAPT) (aspirin+clopidogrel)
dual therapy (DAT) (OAC +clopidogrel)
• DAPT vs TT >> reduction of major bleeding and no increased risk of MACE
• DAT vs TT >> reduction of bleeding, without affecting rates of MACE
• Am J Cardiol. 2015 May 1;115(9):1185-93.
DAT vs TT
DAPT vs TT
Arrigo, Messina (Italy) 2016
A proposito di Tripla terapia(OAC +ASA + P2Y12i)
• La doppia terapia (OAC + P2Y12i) è preferibile• riduce significativamente la mortalità per
qualunque causa e i sanguinamenti (WOESTtrial)
• Riduce i sanguinamenti a parità di effetto sugliEventi CV (Metanalisi, ACTION Registry–GWTG)
• la durata della TT per 6 settimane è sufficiente• uguale protezione antitrombotica e tasso di
emorragie nel confronto tra 6 settimane e 6 mesi (ISAR-TRIPLE trial)
Arrigo, Messina (Italy) 2016
La doppia terapia
DAP (OAC + P2Y12i) : il Clopidogrel è preferibile all’aspirina e al
prasugrel in associazione a OAC Sono in corso trials con Ticagrelor e NOAC
DAPT (P2Y12i + aspirina): indicata solo in pazienti a basso rischio
trombotico (CAHDS 0-1)
Arrigo, Messina (Italy) 2016

scenari
Arrigo, Messina (Italy) 2016
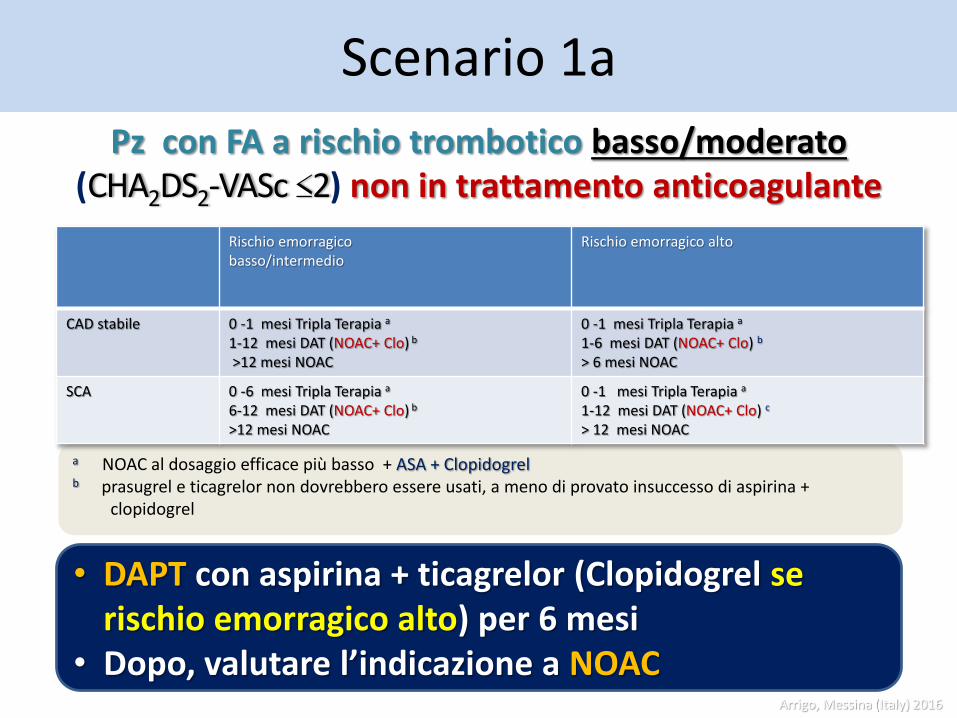
Scenario 1a
a NOAC al dosaggio efficace più basso + ASA + Clopidogrelb prasugrel e ticagrelor non dovrebbero essere usati, a meno di provato insuccesso di aspirina +
clopidogrel
Rischio emorragicobasso/intermedio
Rischio emorragico alto
CAD stabile 0 -1 mesi Tripla Terapia a
1-12 mesi DAT (NOAC+ Clo) b
>12 mesi NOAC
0 -1 mesi Tripla Terapia a
1-6 mesi DAT (NOAC+ Clo) b
> 6 mesi NOAC
SCA 0 -6 mesi Tripla Terapia a
6-12 mesi DAT (NOAC+ Clo) b
>12 mesi NOAC
0 -1 mesi Tripla Terapia a
1-12 mesi DAT (NOAC+ Clo) c
> 12 mesi NOAC
Pz con FA a rischio trombotico basso/moderato (CHA2DS2-VASc ≤2) non in trattamento anticoagulante
• DAPT con aspirina + ticagrelor (Clopidogrel se rischio emorragico alto) per 6 mesi
• Dopo, valutare l’indicazione a NOACArrigo, Messina (Italy) 2016
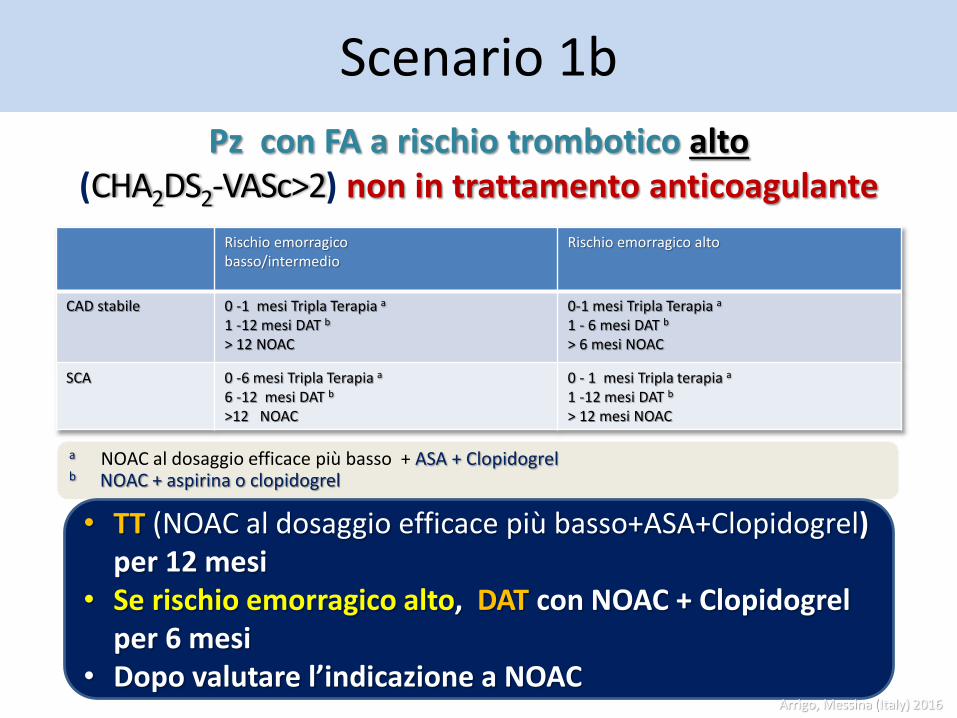
Scenario 1b
a NOAC al dosaggio efficace più basso + ASA + Clopidogrelb NOAC + aspirina o clopidogrel
Rischio emorragicobasso/intermedio
Rischio emorragico alto
CAD stabile 0 -1 mesi Tripla Terapia a
1 -12 mesi DAT b
> 12 NOAC
0-1 mesi Tripla Terapia a
1 - 6 mesi DAT b
> 6 mesi NOAC
SCA 0 -6 mesi Tripla Terapia a
6 -12 mesi DAT b
>12 NOAC
0 - 1 mesi Tripla terapia a
1 -12 mesi DAT b
> 12 mesi NOAC
Pz con FA a rischio trombotico alto (CHA2DS2-VASc>2) non in trattamento anticoagulante
• TT (NOAC al dosaggio efficace più basso+ASA+Clopidogrel) per 12 mesi
• Se rischio emorragico alto, DAT con NOAC + Clopidogrelper 6 mesi
• Dopo valutare l’indicazione a NOACArrigo, Messina (Italy) 2016
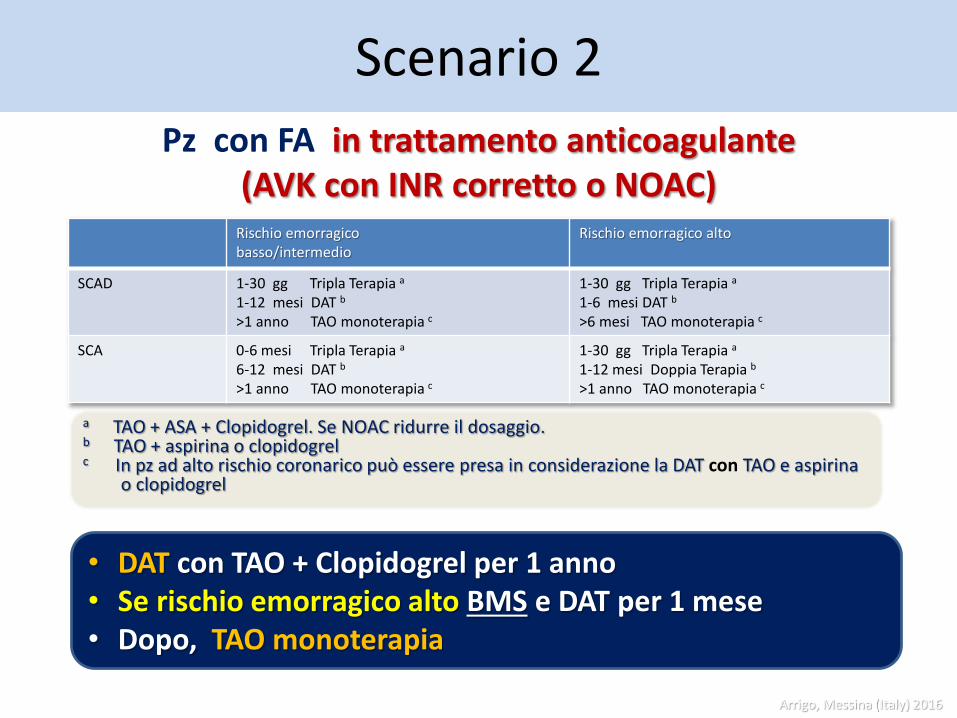
Scenario 2
a TAO + ASA + Clopidogrel. Se NOAC ridurre il dosaggio. b TAO + aspirina o clopidogrelc In pz ad alto rischio coronarico può essere presa in considerazione la DAT con TAO e aspirina
o clopidogrel
Rischio emorragicobasso/intermedio
Rischio emorragico alto
SCAD 1-30 gg Tripla Terapia a
1-12 mesi DAT b
>1 anno TAO monoterapia c
1-30 gg Tripla Terapia a
1-6 mesi DAT b
>6 mesi TAO monoterapia c
SCA 0-6 mesi Tripla Terapia a
6-12 mesi DAT b
>1 anno TAO monoterapia c
1-30 gg Tripla Terapia a
1-12 mesi Doppia Terapia b
>1 anno TAO monoterapia c
Pz con FA in trattamento anticoagulante(AVK con INR corretto o NOAC)
• DAT con TAO + Clopidogrel per 1 anno• Se rischio emorragico alto BMS e DAT per 1 mese• Dopo, TAO monoterapia
Arrigo, Messina (Italy) 2016
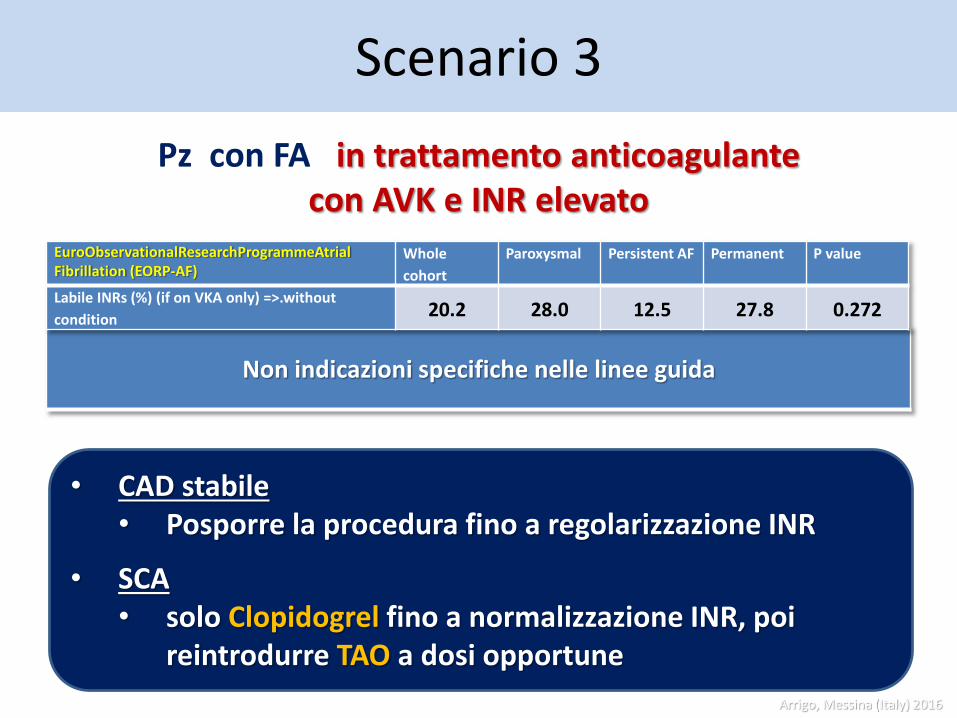
Scenario 3
Non indicazioni specifiche nelle linee guida
Pz con FA in trattamento anticoagulantecon AVK e INR elevato
• CAD stabile • Posporre la procedura fino a regolarizzazione INR
• SCA• solo Clopidogrel fino a normalizzazione INR, poi
reintrodurre TAO a dosi opportune
EuroObservationalResearchProgrammeAtrialFibrillation (EORP-AF)
Whole
cohort
Paroxysmal Persistent AF Permanent P value
Labile INRs (%) (if on VKA only) =>.without
condition 20.2 28.0 12.5 27.8 0.272
Arrigo, Messina (Italy) 2016

Stent e fibrillazione atriale
Quali e quanti farmaci usiamo e per quanto tempo?
Una risposta valida per tutti non esiste e la gestione della terapia antitrombotica è complessa e spesso individuale.
Le principali variabili da considerare sono
• Età
• Sindrome clinica
• Rischio tromboembolico
• Rischio emorragico
• Terapia antitrombotica precedente
• Il tipo di stent
Arrigo, Messina (Italy) 2016
Stent e fibrillazione atriale
La gestione del paziente con fibrillazione atriale e Sindrome Coronarica Acuta (SCA) o intervento coronarico percutaneo (PCI) è una sfida della pratica clinica.
Il punto critico è trovare l’equilibrio ottimale per prevenire gli eventi trombotici, come la trombosi dello stent e lo stroke cardioembolico, senza aumentare il rischio di eventi emorragicimaggiori.
La rapida evoluzione farmacologica e tecnologica rende spesso superati i risultati dei trial clinici di riferimento.
Arrigo, Messina (Italy) 2016

Grazie per l’attenzione
Stent e fibrillazione atriale: singola,
duplice o triplice terapia antitrombotica?
LVIII congresso della sezione
regionale siciliana della Società
Italiana di Cardiologia Roccalumera 17 – 19 novembre 2016
Arrigo, Messina (Italy) 2016
Go, A. S. et al. JAMA 2001;285:2370-2375.
Strategie per evitare il rischio emorragico
1 Ridurre il dosaggio di OAC (target INR 2.0-2.5)
2. Ridurre la durata della Triplice Terapia (1 - 3 mesi)
3.Somministrare di routine farmaci gastroprotettivi
(PPIs)
Arrigo, Messina (Italy) 2016