Embed Size (px)
Citation preview

Alexander Ghanem & David Leistner
Antegrade Approach – How to start?
Minimalists‘ versus Maximalists‘ Approaches
17. September 2017

Our aim and its Paradigmata
Minimalists‘ view Maximalists‘ view
“The patient is treated in one attempt by the mostexperienced operator fitted to his lesion complexity.“
Patient
Patient
ProcedureProcedure
Outcome
G. Werner

Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography
Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography

Minimalists‘ Appropriateness List
adopted from Prof. G. Werner, Darmstadt
• Selection of the patient with normal LV-EF
– Symptoms, but „asymptomatic“ patients may beadapted to their limitations by a CTO...
– Ischemic territory should be > 10%

Relationship between mortality and extentof myocardial ischaemia, depending on therapy
Montalescot / Sechtem et al., Eur Heart J 2013;34:2949–3003. Hachamovitch et al., Circulation 2003;107:2900–2907.
OMT / Revascularisation

adopted from Prof. G. Werner, Darmstadt
• Selection of the patient with normal LVF
– Symptoms, but „asymptomatic“ patients may beadapted to their limitations by a CTO...
– Ischemic territory should be > 10%
• In patients with akinesia and ischemic CMP
– Presence of viability tested by MRI
– A grey zone of scar tissue extension remains
Minimalists‘ Appropriateness List

Viability is a Continuum
Wilcox et al, JACC 2015

Baks T et al. JACC 2006;47:721-5
Improvement of LV-Function dependson viability of revascularized myocardium

Adapted from Werner et al. JACC 2006;48:51-8
Collateral blood flow is neversufficient...
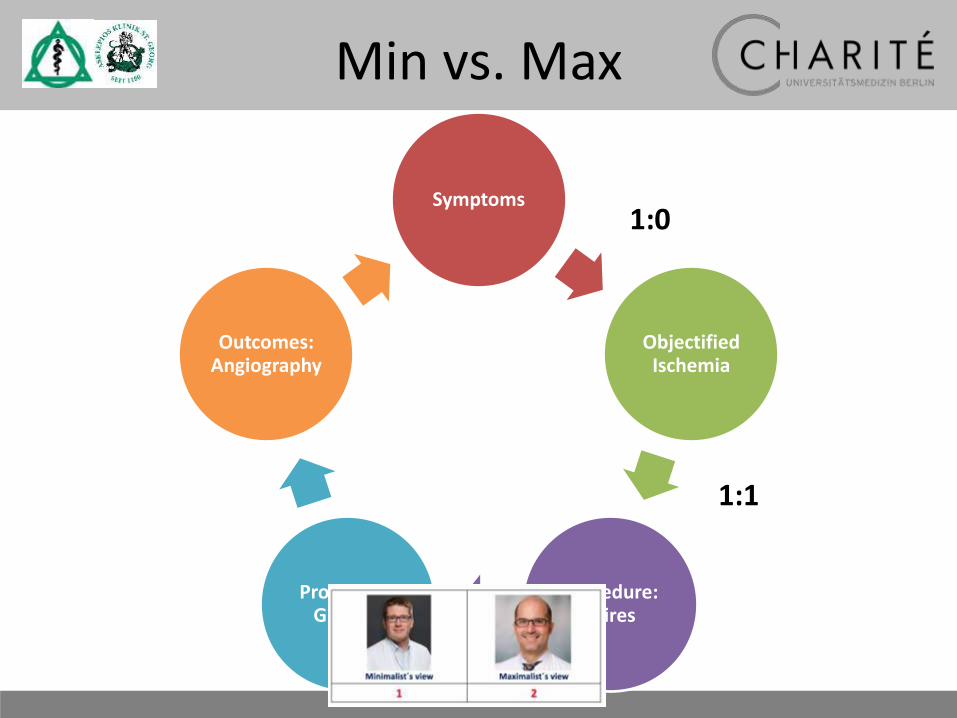
Min vs. Max
Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography

Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography

(Retrograde) CTO PCI reduced markely
symptoms (angina and dyspnea)

Boden et al., NEJM 2007
PCI added to optimal medicaltherapy did not improve outcome
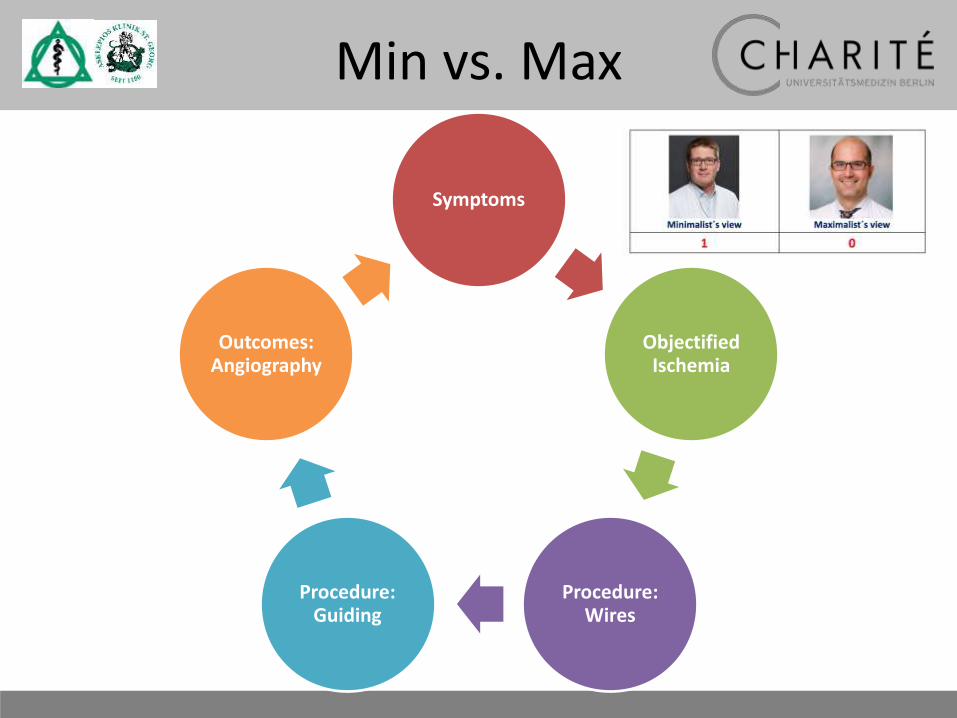
Garcia S et al, JACC 2013;62(16):1421 –31
Outcome after incomplete versus complete revascularisation in MVD

Farooq et al., Circulation. 2013; 128: 141-151
Prognosis is significantly related toresidual SYNTAX-Score

SYNTAX Revascularisation Index
Genereux et al., Am J Cardiology, 2015, DOI: 10.1016/j.amjcard.2015.03.056

Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography
1:0
Min vs. Max
Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography
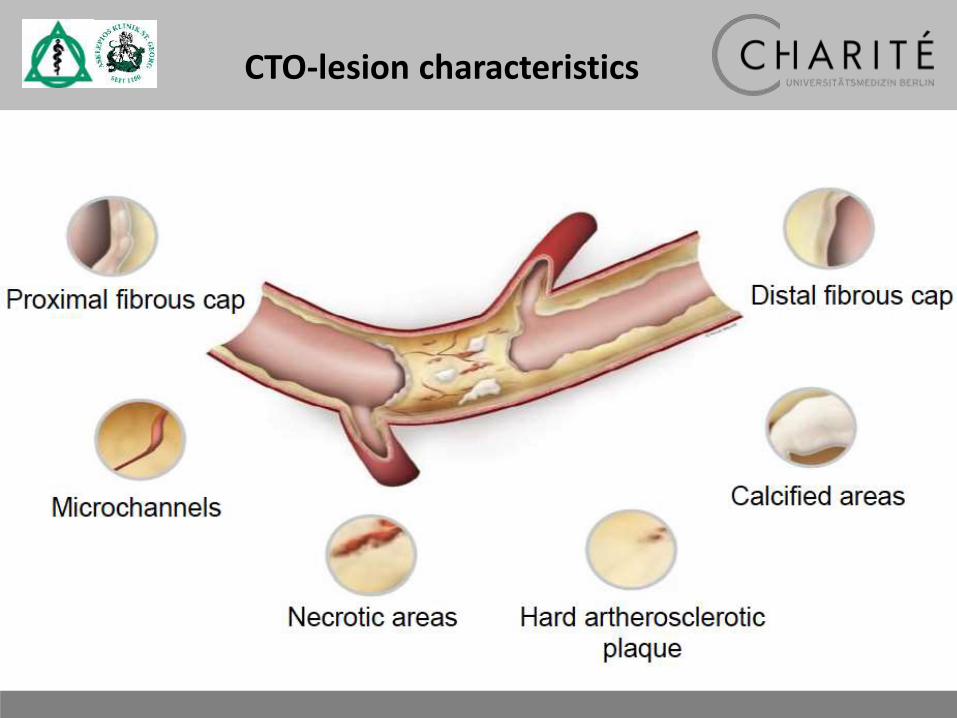
CTO-lesion characteristics
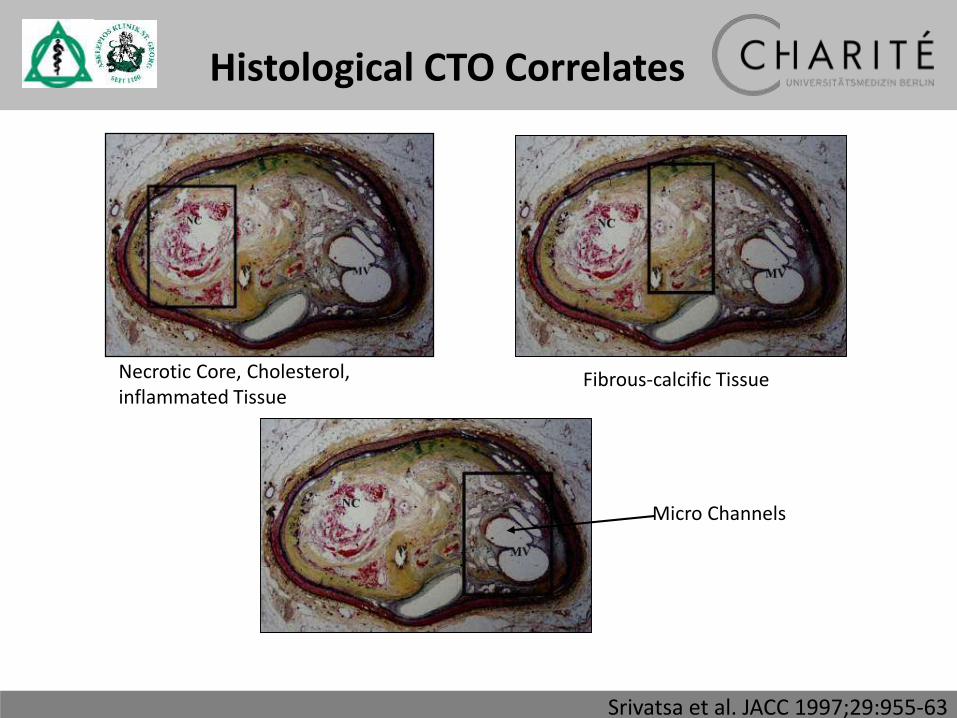
Srivatsa et al. JACC 1997;29:955-63
Necrotic Core, Cholesterol, inflammated Tissue
Fibrous-calcific Tissue
Micro Channels
Histological CTO Correlates
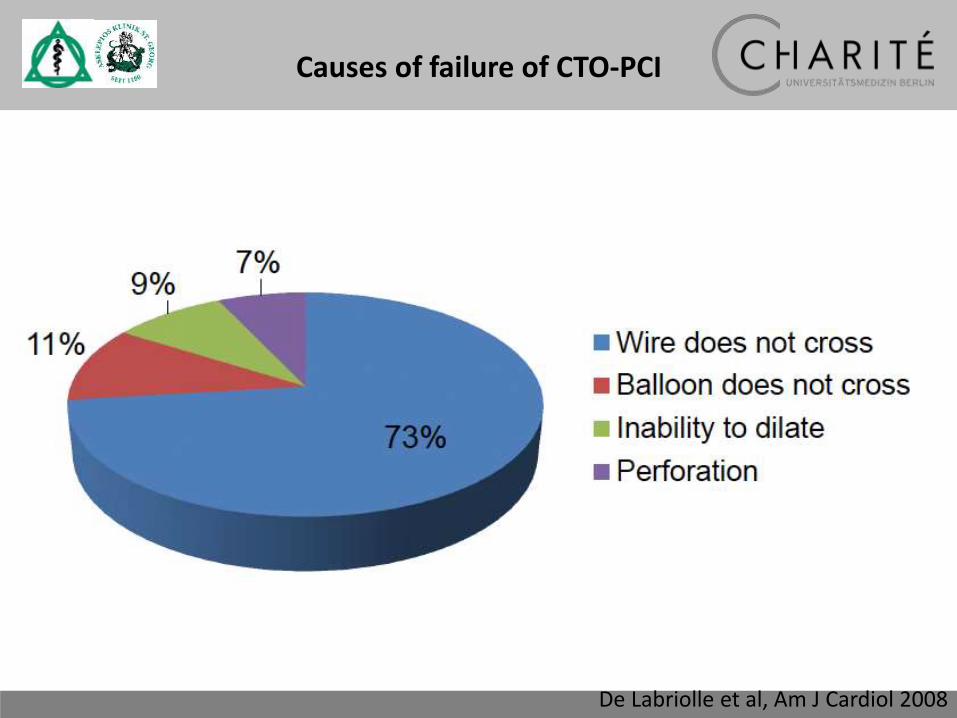
De Labriolle et al, Am J Cardiol 2008
Causes of failure of CTO-PCI
CTO Toyohashi Heart Center
Complex PCI, NYC
Development of CTO-PCI procedure
Miracle
Conquest
Parallel wiring
IVUS guidance
Retrograde approach
1995 2000 2005 2010
Fielder XT
Pilot
Fielder FC
SION
MDCT
Corsair
wire, device
imaging modality
wiring technique
CTO Toyohashi Heart Center
Complex PCI, NYC
Development of CTO-PCI procedure
Miracle
Conquest
Parallel wiring
IVUS guidance
Retrograde approach
1995 2000 2005 2010
Fielder XT
Pilot
Fielder FC
SION
MDCT
Corsair
wire, device
imaging modality
wiring technique
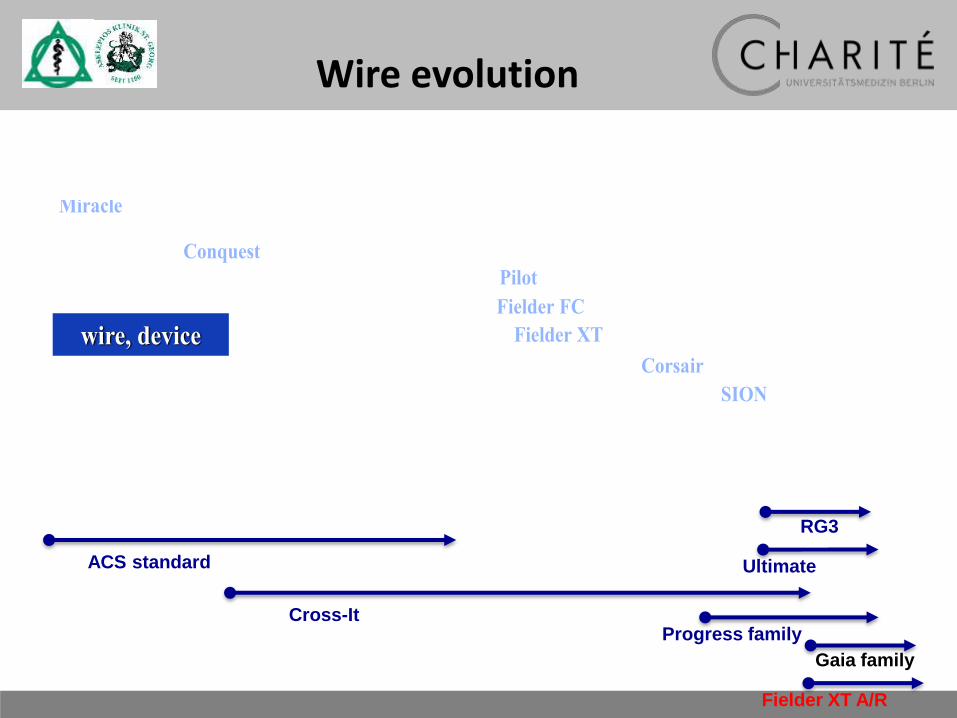
ACS standard
Cross-ItProgress family
RG3
Ultimate
Gaia family
Fielder XT A/R
Wire evolution

CTO Toyohashi Heart Center
Complex PCI, NYC
Development of CTO-PCI procedure
Miracle
Conquest
Parallel wiring
IVUS guidance
Retrograde approach
1995 2000 2005 2010
Fielder XT
Pilot
Fielder FC
SION
MDCT
Corsair
wire, device
imaging modality
wiring technique
Wire evolution

Microcatheter
Finecross

Improve wire pushabilityConcentrate rotating forcefor better wire control
Superior device passage for the next option
1. 2.
3.
Microcatheter
Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography
Min vs. Max
1:1
1:0

Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography
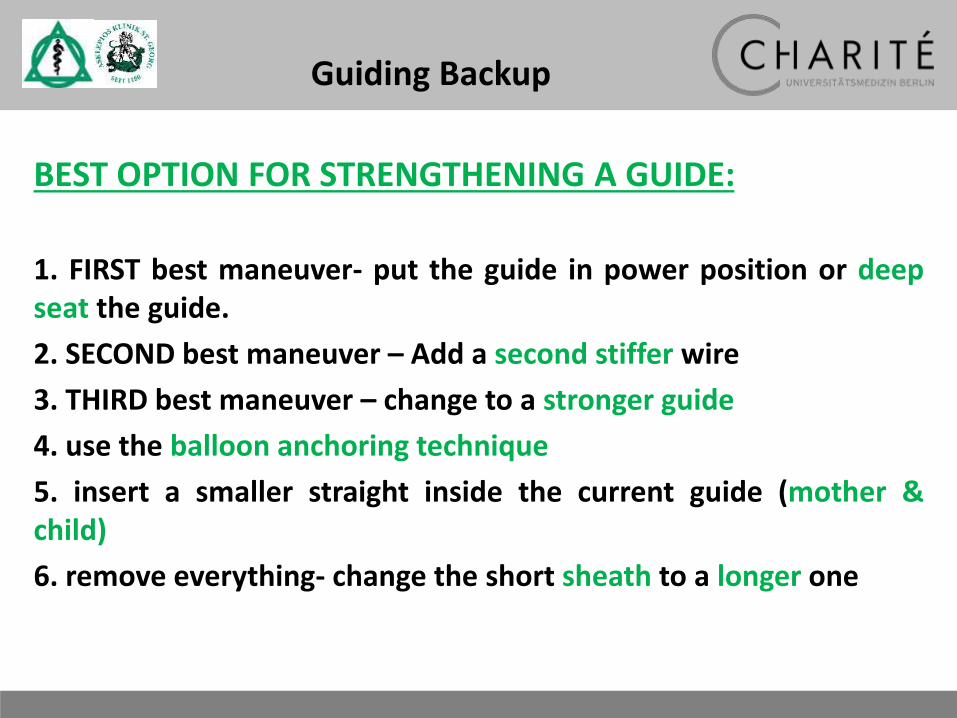
Guiding Backup
BEST OPTION FOR STRENGTHENING A GUIDE:
1. FIRST best maneuver- put the guide in power position or deepseat the guide.
2. SECOND best maneuver – Add a second stiffer wire
3. THIRD best maneuver – change to a stronger guide
4. use the balloon anchoring technique
5. insert a smaller straight inside the current guide (mother &child)
6. remove everything- change the short sheath to a longer one

Guiding Diameter
Ghione et al., Eurointervention 2013

Guiding Diameter
Habit #2: Begin with the End in Mind !

Habit #1: Begin with any End in Mind !
PCI - OPERATORS

Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography
1:1
1:0
1:2
Min vs. Max

Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography

Gasparini et al. JACC INTV, 7 (4), 2014.
Vessel Remodelling
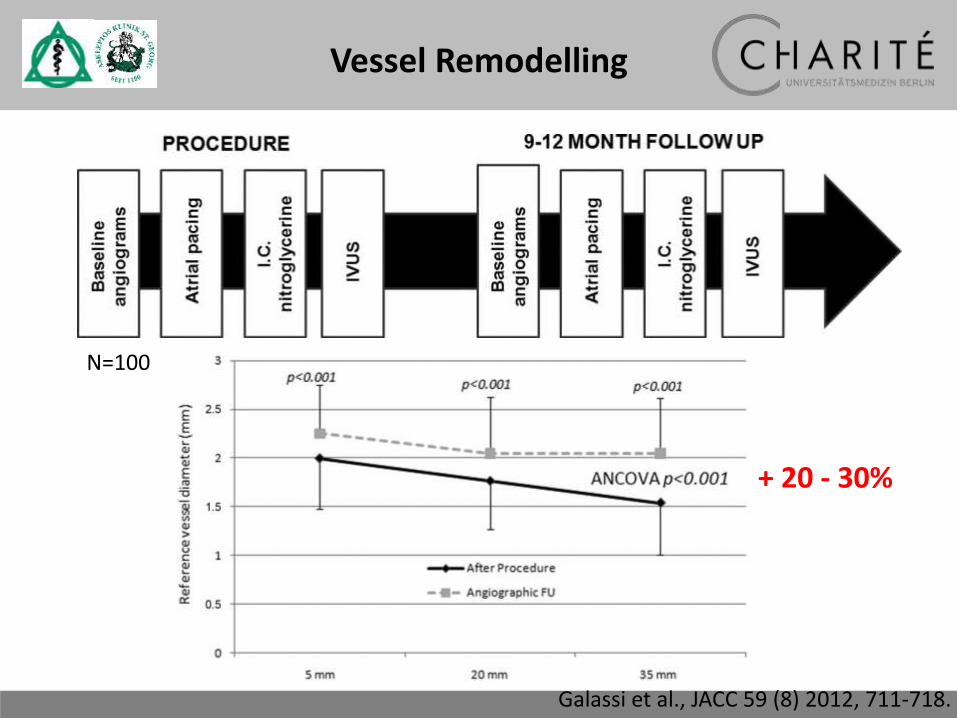
Galassi et al., JACC 59 (8) 2012, 711-718.
N=100
Vessel Remodelling
+ 20 - 30%

Galassi et al., JACC 59 (8) 2012, 711-718.
Vessel Remodelling
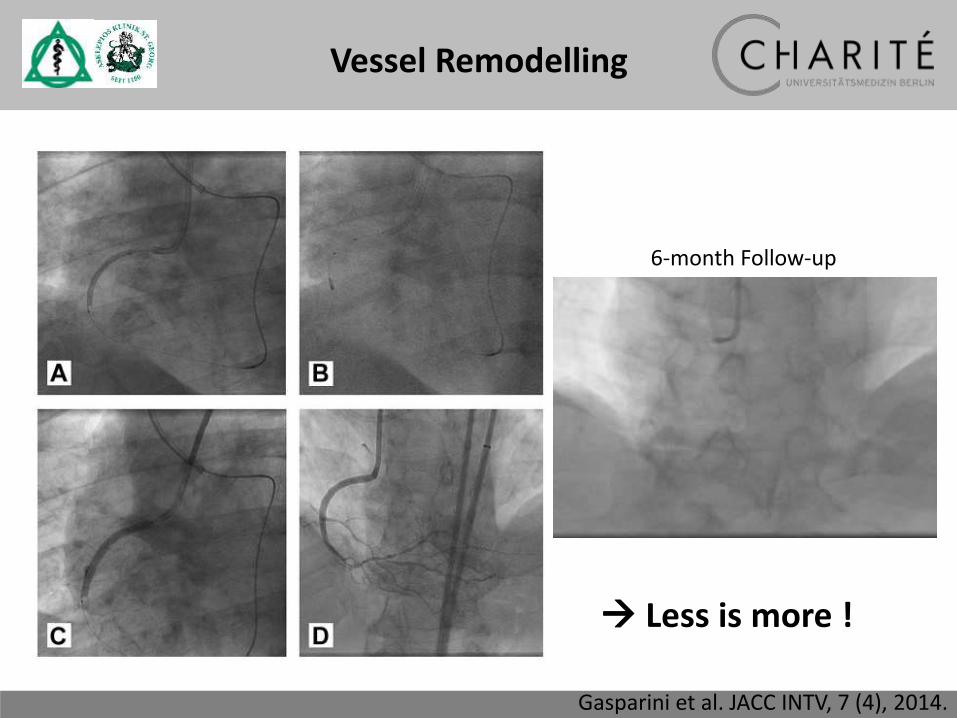
6-month Follow-up
Gasparini et al. JACC INTV, 7 (4), 2014.
Less is more !
Vessel Remodelling
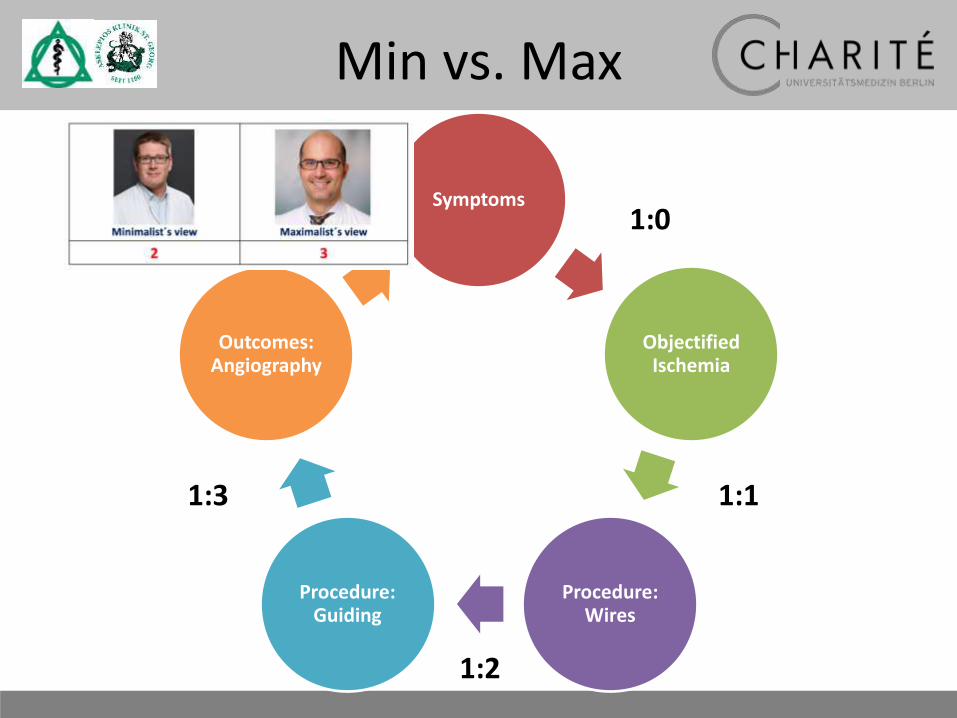
Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography
1:1
1:0
1:2
1:3
Min vs. Max
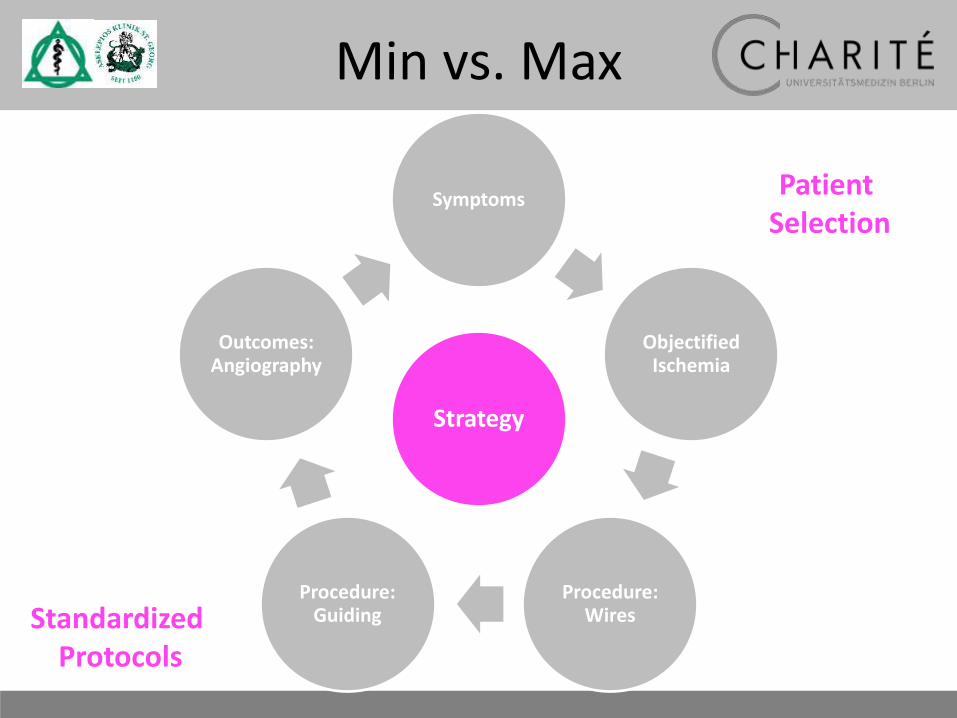
Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography
Strategy
Patient Selection
StandardizedProtocols
Min vs. Max

Strategy is often about whatyou don‘t do!
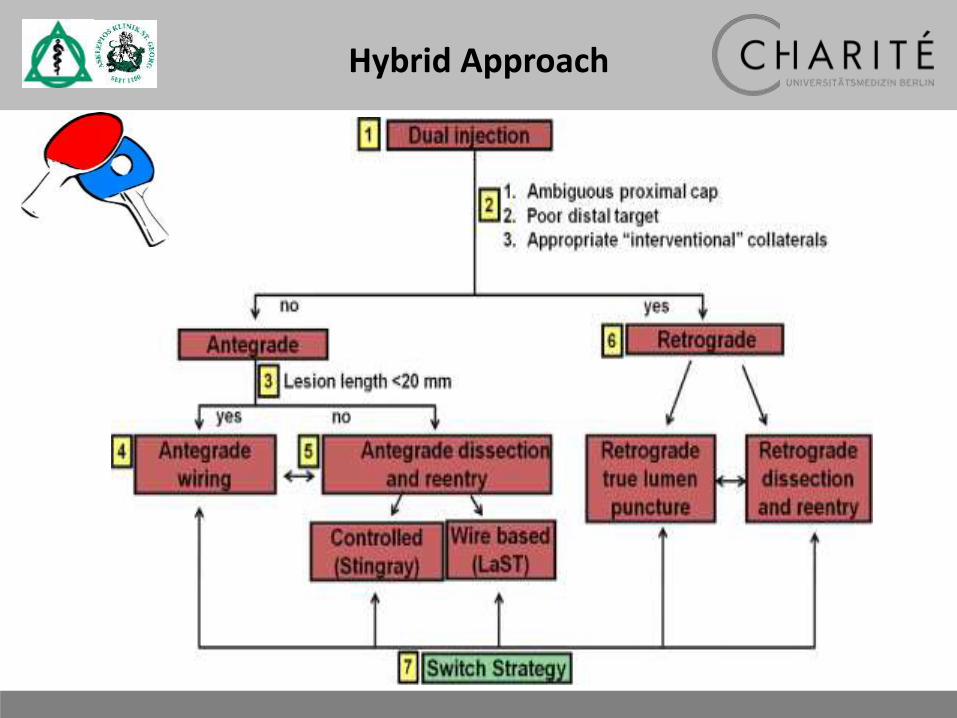
Hybrid Approach

pC
dC
Pl
Hybrid Approach

Hybrid Approach4
5
6 6´ 7
4´
4
B 2







Strategic Options
adopted from Prof. G. Werner, Darmstadt
The apparent length of theocclusion is often shorter
than you think !
Bilateral Injection
Maximum Guide Backup
AntegradeFielder XT/A/R orGaia 1 Gaia 2,
Confienza, Progress
Penetration, thenstep down
AntegradeNo stump
IVUS for guidedpenetration?
Reentry-System
Crossboss / Stingray
Distal good target
Parallel with stiffwire
Retrograde
Feasible collateralpathways

Symptoms
ObjectifiedIschemia
Procedure: Wires
Procedure: Guiding
Outcomes: Angiography
Strategy
Min vs. Max
CTO – PCI always should beplanned and performed
with a maximalist‘s mindset !