Embed Size (px)
DESCRIPTION
s
Citation preview

ByDr. Asmaa Sobhy Abd-ellah
Lecturer of Anesthesia and Intensive CareAlzahraa university hospital
Al-Azhar university3/21/2013

Bariatric surgery is a surgical subspecialty that perform operations to treat morbid obesity.
Over 100,000 laparoscopic Bariatric procedures were performed in the US in 2004
Most of the patho-physiology & medical conditions associated with extreme Obesity are reversible with sustained weight loss following Bariatric surgery.

• BMI > 40 kg/ m2 • BMI > 30 kg/ m2
with co-morbidities
• Failed medical treatment
Unstable angina Inflammatory diseases of
the gastrointestinal tract upper gastrointestinal
bleeding (varices); chronic pancreatitis; laparoscopic surgery may
be technically difficult in patients weighing >180 kg and this may be considered a relative contraindication.
Indications
Indications
Contraindications
Contraindications

A-Vertical-banded gastroplasty,
B-Adjustable laparoscopic gastric banding
A- Jejunoileal bypass
B- Biliopancreatic diversion.
C - Gastric bypass
1-Restrictive procedures 2- Malabsorptive procedures
involves the creation of a small gastric pouch to cause early satiety;
Involve bypass of a portion of the small intestine. With the drawbacks of relative technical complexity and a risk of malnutrition and vitamin deficiencies, along with the need for close follow-up.
Surgical approaches designed to treat obesity can be classified as restrictive or malabsorptive

Ch. Metabolic disorder that is primarily caused by over consumption of caloric substances
AHA defines obesity by BW> 30% of IBW
Definitions :

Ideal Weight = Height – 100 or 105 (Brocca)
Body Mass Index = weight (kg)/ height ( m)2
BMI = 25 kg/m2 – NORMAL
BMI > 30 – 49.9 kg/m2 OBESE subdivided into classes
BMI >50 kg/m2 super-obese
Health risks increase with the degree of obesity and with increased abdominal distribution of weight.
Men with a waist measurement of 40 in. and
women with a waist measurement of 35 in. are at increased health risk.

Quality of life issues: depression, social incompetence
NIDDM HTN
CV disease
OSA
Liver & Gallbladder diseases
Arthritis
Risk of sudden death
Colon and breast cancer
obesity

LV dysfunction is often present in young asymptomatic patient
high cardiac output and an increased circulating volume
HTN
Increased Pre-load & After-load Increased PAP (dyspnea, fatigue,
syncope).
Fatty Infiltration of conductive system
Risk of arrhythmias
1. CV System
2- Respiratory system
O2 consumption & CO2 production increased
WOB increased
Chest wall compliance low
FRC<CC
Decrease lung volumes
Obesity- hypovetilation syndrome

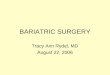
Flow-volume loops from healthy obese female, aged 35 yr, BMI = 43 kg/m2,

NW OB
FEV1, liters (%predicted) 1.33 ± 0.64 (59 ± 17) 1.26 ± 0.21 (60 ± 13)
FVC, liters (%predicted) 3.10 ± 1.18 (95 ± 16) 2.80 ± 0.60 (92 ± 20)
FEV1/FVC,% 42 ± 8 47 ± 12
PEFR, l/s (%predicted) 4.4 ± 1.4 (68 ± 16) 4.4 ± 0.7 (73 ± 16)
FEF50, l/s (%predicted) 0.5 ± 0.4 (12 ± 8) 0.5 ± 0.2 (14 ± 6)
TLC, liters (%predicted) 7.44 ± 1.97 (124 ± 15) 6.35 ± 1.66 (109 ± 30)
IC, liters (%predicted) 2.24 ± 0.86 (81 ± 18) 2.18 ± 0.35 (84 ± 15)
FRC, liters (%predicted) 5.20 ± 1.37 (158 ± 27) 4.18 ± 1.51 (130 ± 38)
RV, liters (%predicted) 3.83 ± 1.04 (170 ± 43) 3.42 ± 1.29 (154 ± 53)
RV/TLC, % 52 ± 11 52 ± 9
ERV, liters (%predicted) 1.37 ± 0.69 (134 ± 50) 0.76 ± 0.42 (80 ± 38)
sRaw, cmH2O·s (%predicted) 22.5 ± 9.3 (544 ± 218) 21.5 ± 11.8 (512 ± 270)
DLCO, ml ·min−1 ·mmHg−1 (%predicted) 13.9 ± 6.5 (75 ± 26) 14.6 ± 5.0 (67 ± 20)
DLCO/VA, ml ·min−1 ·mmHg−1 l−1(%predicted) 2.86 ± 0.69 (77 ± 16) 3.45 ± 0.88 (93 ± 23)
MIP, cmH2O (%predicted) −67 ± 22 (89 ± 30) −76 ± 16 (108 ± 38)
MEP, cmH2O (%predicted) 121 ± 28 (75 ± 17) 125 ± 46 (77 ± 24)
CLst, l/cmH2O 0.37 ± 0.13 0.29 ± 0.12
PLst, cmH2O (%predicted) 21.3 ± 5.9 (77 ± 37) 27.4 ± 8.1 (97 ± 25)
Coefficient of retraction, cmH2O/l 3.1 ± 1.4 4.5 ± 1.5
Sniff Pes, cmH2O −64 ± 18 −65 ± 11
Sniff Pdi, cmH2O† 114 ± 27 127 ± 25
Cough Pga, cmH2O† 137 ± 66 177 ± 69
Pulmonary function and static respiratory mechanical measurements

1.Hypercapnia
2.Severe hypoxemia
3.Periodic breathing
4.ventricular enlargement
5.Dependent edema.
6.Polycythemia.
7.Pulmonary edema.
Obesity- Hypoventilation Syndrome Pickwickian syndrome:

a) Limitation of extension and flexion of the C-spine.
b) Restricted mouth opening from submental fat.
c) Large tongue.
d) Redundant intra oral tissue.
e) small Thyromental distance.
f) Infantile type anterior laryngeal opening.
3. Airways

Gastroparesis as obese persons have NIDDM . Increase incidence of reflux, haiatal hernia
and increase abdominal pressure Fatty Liver w or w/o liver dysfunction is
common. Gall bladder disease is also common
4 -GI System.
Renal clearance of drugs is increased in obesity because of increased renal blood flow and glomerular filtration rate (GFR)
5 –Renal System


History of previous surgeries and their anesthetic challenges and need for ICU admission
cardio-respiratory & airway
Co-morbidities:

Assessed for use of weight reducing substances, herbal supplements, and anorexiant drugs (drugs that acting on the brain to reduce the appetite).
Chronic use of noradrenergic and serotonergic therapy can produce hypertension, tachycardia, anxiety, psychosis, and catecholamine depletion
Patient scheduled for surgery following previous Bariatric surgery may have chronic metabolic changes

CBC bl. Sugar Electrolytes Liver and renal functions Coagulation profile ABG (hypoxia & hypercarbia) ECG (LVH- low QRS amplitude -ischemia)
Chest x-ray PFTs Sleep study ( polysomniography) OSA /0SHA

Explanations of anticipated events during preoperative preparation (multiple venipunctures, central and arterial lines insertions, awake intubation, pain management) and protection of the patient’s privacy will relieve anxiety

Medication for chronic HTN
No diabetic medication on the morning of surgery
Avoid sedation.
Antibiotics
DVT prophylaxis (heparin –compressive stocks –inferior vena cava filter)
Prophylaxis for aspiration

NIBP can be obtained from the wrist or ankle
End-tidal co2 monitoring
A-line highly recommended for invasive BP monitoring and ABG sampling.
CV lines especially if difficult peripheral IV line or supermoribid obese
Urinary catheter
Nerve stimulator: needle electrodes are recommended (surface electrode)

Table It is mandatory to arrange a surgical
table with an adequate weight limit, and appropriate support for body parts and cushions for Protection from nerve injury
Strapping patient to operating table help keep from falling off table
Transfer
Sufficient manpower must be available to help transfer the patient from a bed to the operating table, and special inflation mattresses have been designed for this purpose.

Equipment for difficult airway management ,including laryngeal mask and fibroptic bronchoscope should be available and surgical airways should be considered
Since mask ventilation can be difficult, a second person
It is possible that no difference between laryngoscopy and intubation in normal and obese if paying attention for proper patient positioning

Adequate pre-oxygenation is vital for obese patient usually using 45 degree head-up
Use of 10 cm H2O CPAP during pre-oxygenation results in high pao2 after intubation and decrease the incidence of atelectasis
Four vital capacity breaths with 100% oxygen within 30sec have been suggested as superior to the usually recommended 3 min of 100% oxygen in obese patient

Less lipophilic drugs not affected by vd in obese
Lipophilic drugs (i.e. benzodiazepines, thiopental, sufentanyl) have a greater volume of distribution and longer elimination half-life in obese patients, although the clearance rate is similar to that in non-obese patients
Anesthetic drugs should be tailored according to their lipid solubility and knowledge of their lingering depressive effects on respiration calculated according to IBW or more accurately on LBW

Drug Dosing Comments
Propofol (LBW) Preferable induction agent. Titrate dosing to effect
Thiopental TBW Increased Vd. Increased blood volume, cardiac output, and muscle mass Increased absolute
dose. Prolonged duration of action
Midazolam LBW Central Vd increases in line with body weight. Increased absolute dose. Prolonged sedation
because larger initial doses are needed to achieve adequate serum concentrations
Succinylcholine TBW Plasma cholinesterase activity increases in proportion to body weight. Increased absolute dose
Vecuronium LBW Recovery may be delayed if given according to TBW because of increased Vd and impaired
hepatic clearance
Rocuronium LBW Faster onset and longer duration of action. Pharmacokinetics and pharmacodynamics are not altered in obese subjects
Atracurium Cisatracurium
LBW Absolute clearance, Vd, and elimination half-life do not change. Unchanged dose per unit
body weight without prolongation of recovery because of organ- independent elimination
Fentanyl LBW Increased Vd and elimination half-time, which correlates positively with
Sufentanil LBW the degree of obesity. Distributes as extensively in excess body mass as in lean tissues. Dose should account for total body mass.
Remifentanil IBW Systemic clearance and Vd corrected per kilogram of TBW—significantly smaller in the
obese. Pharmacokinetics are similar in obese and nonobese patients
Neostigmine LBW Reversal of muscle relaxants may be slower than in non -obese patients.

Ramped position “stacking”

Neuromuscular recovery time is similar in obese & non-obese patient with Atracurium &CIS-ATRACURIUM (NIMBEX)
Obese patients may require larger doses of succinylcholine because of greater levels of pseudocholinesterase than in non-obese patients.
Any of the commonly available intravenous induction agents may be used after taking into consideration problems pecular to individual patients

Bariatric procedures are usually performed laparoscopically unless there is a contraindication such as previous extensive abdominal surgery.
Therefore, patients are usually placed in a steep reverse Trendelenburg position,
Although offering a slight respiratory advantage, this position, however, exacerbates venous pooling in the limbs, decreasing venous return and contributing to the high risk of venous thromboembolism.

Pneumoperitoneum causes systemic changes during laparoscopy. The gas most often used for this purpose is carbon dioxide. Positioning, such as Trendelenburg, can worsen the systemic changes of pneumoperitoneum
Systemic vascular resistance is increased with increased intraabdominal pressure (IAP). The degree of IAP determines its effects on venous return and myocardial performance
There is a biphasic cardiovascular response to increases
in IAP.

Continuous infusion of short-acting ,such as propofol or any inhalational agents or a combination may be used to maintain anesthesia
Desflurane, sevoflurane and isoflurane are minimally
metabolized and are therefore useful agents in the obese
patient. Desflurane possibly providing better hemodynamic
stability and faster washout

Combined epidural and general balanced anesthesia has been advocated to allow better titration of anesthetic drugs, use of a larger oxygen concentration, and optimal muscle relaxation for upper abdominal surgery in the obese
short-acting opioids combined with a low-solubility inhalational anesthetic, facilitate a more rapid emergence without increasing opioid-related side effects
short-acting NDMR is a better choiced for maintenance of anesthesia

VT – 10-12 mL/Kg IBW
FiO2 up to 1.0 may be needed
RR 12- 14 bpm
High PiP will be needed
PEEP = 5cm H2O or more but …
N2O is avoided

Fluid requirements are usually larger to prevent postoperative acute tubular necrosis
Patients usually require up to twice the calculated maintenance fluid requirement plus the calculated deficit based on a 12-h fasting for the first hour by using the 4-2-1 formula
The next hour usually requires the same amount of crystalloid,
After which the amounts are reduced to approximately half the calculated maintenance requirement, based on LBM, For the next 12 h

Position:
beach chair: Upper body elevated 30-45 degree.
Neuromuscular blockade : must be fully reversed and adequate muscle strength has to be returned before patient is extubated
Oxygenation: Restoration of normal pulmonary function after abdominal surgery may take several days.
Nasal cannula or face mask O2. Nasal CPAP BiPAP Spirometry

Avoid IM injection
Analgesia can be provided through:
An IV opioid via PCA dosed on the basis of IBW IV opioid Epidural analgesia with local anesthetic or
opioids Local infiltration of the incision with local
anesthetic NSAIDs as an adjunctive to opioids and local
infiltration

For regional anesthesia , special equipments in terms of longer needles or special ultrasound probes may be needed
Care should be exercised in dosing
Laparoscopy can be difficult in super-morbid obese patient
Remove all endogastric tubes completely before gastric division
After RYGB pouch is created, the anesthiologist should not blindly insert the NG tube

Overall, each type of surgery was safe, with the more complex surgeries carrying a greater risk of morbidity and mortality.
Mortality ranged from a; low of 0.1% for restrictive procedures to 1.3% for biliopancreatic diversion/duodenal switch.
oDiabetes resolved in 76.8% of cases,
o lipid profiles improved in70.0%,
oHypertension resolved in 61.7%, and
o obstructive sleep apnea resolved in 85.7%.
Effect on co-morbidities

Bariatric surgery is fraught with complexities that need careful consideration.
All members of the multidisciplinary team must be involved throughout all stages of assessment, surgery, and follow up.
Weight loss surgery is associated with a decrease in obesity related co-morbidities, which often are not seen in lifestyle changes alone.
Patients must be fully counselled on the operative and postoperative sequelae of surgery so that they understand the risks.
Ensuring that patients are fully optimized before their surgery and receive the appropriate levels of care during and after their operations is paramount.

THANK YOU