Embed Size (px)
Citation preview

04/15/23 1
An approach to jaundiceAn approach to jaundice
Dr. M. S. Prasad

04/15/23 2
ObjectivesObjectives
• By end of this period, you will be able to explain the clinical and pathological approach to a patient suffering from jaundice.

04/15/23 3
DefinitionDefinition
• Jaundice is defined as yellowish discolouration of skin, conjunctivae, sclerae and mucous membrane due to increased level of bilirubin in blood.
• Syn:– Icterus,– Hyperbilirubinaemia (Hyperbil)

04/15/23 4
IntroductionIntroduction
• French word, ‘jaune’ means yellow.
• Serum Bilirubin levels < 2 mg/dl (30 μmol/ liter) in adults does not cause jaundice.
• Serum Bilirubin level < 5 mg/dl (75 μmol/L) in newborn does not cause jaundice.

04/15/23 5

04/15/23 6

04/15/23 7
Differential DiagnosisDifferential Diagnosis• Carotenemia:
– Palms and soles are yellow,– Skin may also be yellow, but– Sclera is never yellow,– Not found in newborn.
• Chloroquine (?).
• Turmeric application.
04/15/23 8

04/15/23 9
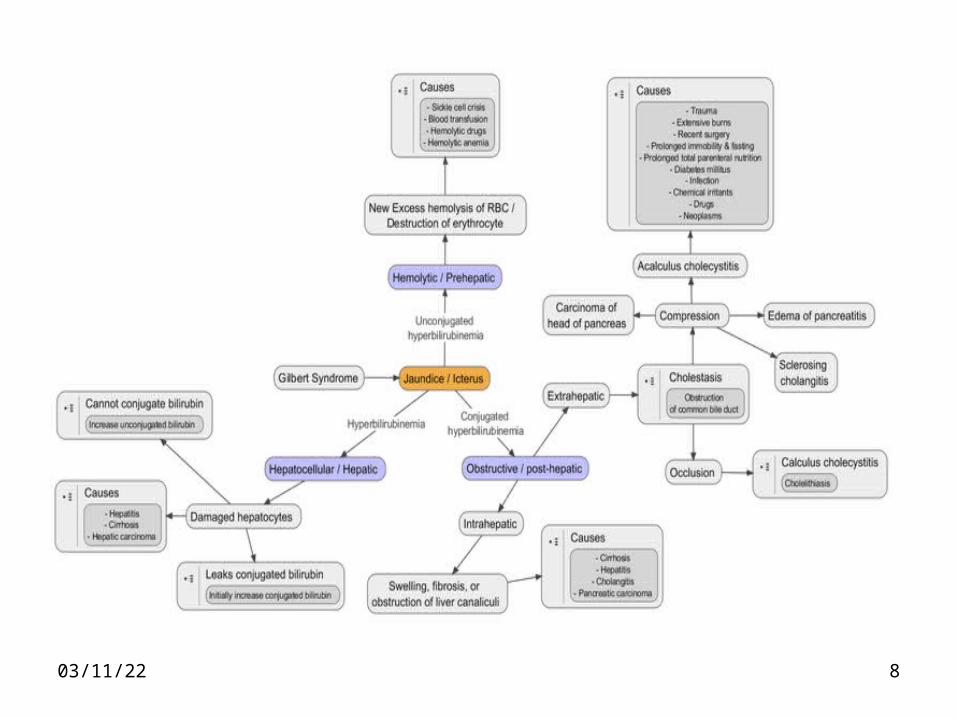
CategoriesCategories
• Pre-hepatic/haemolytic,
• Hepatic/hepatocellular,
• Post-hepatic/cholestatic.

04/15/23 10
Pre-hepatic CausesPre-hepatic Causes• Congenital Haemolytic Anaemias:
– ABO/Rh incompatibilty,– Hereditary spherocytosis,– Thalassemia,– Sickle cell anaemia,– G6PD deficiency.
• Defects in bilirubin metabolism:– Gilbert’s syndrome,– Crigler-Najjar Syndrome.

04/15/23 11
Pre-hepatic ……….Pre-hepatic ……….
•HUS,
•Malaria.

04/15/23 12
Hepatic/hepatocellularHepatic/hepatocellular
• Physiologic Jaundice of Newborn,
• Intra-hepatic Congenital Biliary Atresia (CBA),
• Hepatitis,
• Hepatotoxicity,
• Cirrhosis of liver,
• Leptospirosis.

04/15/23 13
Post-Hepatic/cholestatic
• Extra-hepatic CBA,
• Choledochal cyst,
• Pancreatitis,
• Pancreatic cyst,
• Gall stones.

04/15/23 14
Some clues to diagnosis
• Fever, pain abdomen, vomiting, acute onset, tender hepatomegaly with jaundice:– Acute Viral Hepatitis.
• Chronic jaundice, low grade fever or afebrile, features of liver failure with or without features of portal hypertension:– Chronic Liver Disease (CLD)

04/15/23 15
Clues:Clues:
• Mild jaundice (lemon yellow) with severe pallor with splenomegaly, sometimes hepatomegaly also, typical facial features:– Congenital Haemolytic Anaemia.
• Preceding h/o diarrhoea, pallor, jaundice, oliguria or even anuria:– HUS.

04/15/23 16
CluesClues
• Biphasic course with fever, mild jaundice, haemorrhages, meningitis and h/o rats in kitchen or access to food stored in house:– Leptospirosis.

04/15/23 17
Neonatal Neonatal HyperbilirubinaemiaHyperbilirubinaemia
Neonatal Neonatal HyperbilirubinaemiaHyperbilirubinaemia

04/15/23 18
How to look for jaundice?
• To look for jaundice, press the infant’s skin over the forehead with your fingers to blanch, remove your fingers and look for yellow discolouration under natural light.
• If there is yellow discoloration, the infant has jaundice.
• To assess severity, repeat the process over chest, abdomen, thighs, legs and palms and soles.

04/15/23 19
Clinical Assessment of Jaundice
6
9
12
15
18-20
6
9
12
15
18-20

04/15/23 20
According to age of According to age of appearance of jaundiceappearance of jaundice

04/15/23 21
According to age of appearance of jaundice
• Early Jaundice (< 10 days):– First 24 hours,– After 24 hours.
• Prolonged Jaundice (> 10 days):– Prolonged unconjugated hyperbilirubinaemia– Prolonged conjugated hyperbilirubinaemia

04/15/23 22
Early JaundiceEarly Jaundice
• First 24 hrs:– Rh/ABO incompatibility,– Congenital Hereditary Spherocytosis,– RBC enzyme defects.
• After 24 hrs:– Physiologic jaundice,– Cephalhematoma,– Sepsis,– Galactosemia,– Polycythemia.

04/15/23 23
Early JaundiceEarly JaundiceCauseCause ConfirmationConfirmation
Rh/ABO incompatibility
1. DCT
2. MBG
3. BBG
G6PD deficiency1. Family History
2. G6PD estimation
Spherocytosis1. Blood Film
2. Full Blood Count
Sepsis Sepsis screening.

04/15/23 24
Prolonged JaundiceProlonged Jaundice• Breast Milk Jaundice,
• Hypothyroidism,
• CBA,
• Neonatal Hepatitis,
• Galactosemia,
• Crigler-Najjar Syndrome,
• Gilbert Syndrome,
• Sepsis

04/15/23 25
Jaundice persisting beyond one month of age
• CBA,
• Neonatal Hepatitis,
• Hypothyroidism.

04/15/23 26
Approach to the newborn with jaundiceApproach to the newborn with jaundice
Jaundice inin a termNeonate
< 24 hours old > 24 hours old
• Rule out hemolysis.• No discharge.• Appropriate Therapy• Close monitoring.
DiagnosisTreatment
AAP guideline Disposition

04/15/23 27
Approach Approach (continued)
Diagnosis
Conjugatedbilirubinaemia
UnconjugatedHyperbilirubinaemia
Non-haemolytic Haemolytic

04/15/23 28
IMNCI ApproachIMNCI Approach

04/15/23 29
And if the infant has jaundice
And if the infant has jaundice
SIGNS CLASSIFY AS
• Palms and soles yellow or
• Age < 24 hours or
• Age 14 days or more.
SEVERE SEVERE JAUNDICEJAUNDICE
•Palms and soles not yellow JAUNDICE

04/15/23 30
Need of investigation• Check if,
– Onset of jaundice is within 24 hrs of life, or– Baby is more than 14 days of age, or– Jaundice is below abdomen on clinical
assessment.
• If any of the above is ‘yes’ then do the investigations.

04/15/23 31
InvestigationsInvestigations
• Serum bilirubin (total/direct/indirect)
• Hemoglobin/hematocrit
• Blood groups of baby and mother
• Other investigations as needed.

04/15/23 32
Conjugated Conjugated HyperbilirubinaemiaHyperbilirubinaemia

04/15/23 33
Conjugated HyperbilirubinaemiaConjugated Hyperbilirubinaemia
• Pale stools,
• Dark urine,
• Hepatomegaly,
• Dysmorphism,

04/15/23 34
Causes of conjugated bilirubinaemiaCauses of conjugated bilirubinaemia
• Sepsis,
• Inborn Errors of Metabolism,
• Biliary Atresia,
• Hypothyroidism.

04/15/23 35
Clinical Features and Recommended Tests for
Genetic Syndromes presenting with ConjugatedConjugated
Hyperbilirubinaemia

04/15/23 36
Cystic FibrosisCystic Fibrosis
• Features:– Pancreatic insufficiency,– Pulmonary diseases,– Meconium ileus,– Infertility
• Tests:– Sweat analysis,– CFTR common mutation panel and full
sequence analysis.

04/15/23 37
GalactosemiaGalactosemia• Features:
– Hyperbilirubinaemia,– Hypoglycaemia,– Bleeding diathesis,– Oedema,– Ascites, and – Cataract.
• Tests:– Galactose 1 Phosphatase level,– GALT enzyme activity,– GALT DNA analysis.

04/15/23 38
UnconjugatedUnconjugatedHyperbilirubinaemiaHyperbilirubinaemia

04/15/23 39
Unconjugated HyperbilirubinaemiaUnconjugated Hyperbilirubinaemia
Non-hemolytic
• DCT negative,• Stable haemoglobin,• Normal reticulocyte
• Bruising,• Poor stooling,• Hypothyroidism,• Criggler Najjar

04/15/23 40
Unconjugated HyperbilirubinaemiaUnconjugated Hyperbilirubinaemia
Haemolysis
Physiological Pathological
• Well appearing,• DCT negative,• Peaks at day 3,• Disappears by day 5,• Peak < 12 mg/dl.
• ABO/Rh incompatibility,• RBC defects,• Enzyme defects

04/15/23 41
Clinical Features and Recommended Tests for Genetic Disorders with UnconjugatedUnconjugated Hyperbilirubinaemia.

04/15/23 42
Crigler Najjar Type ICrigler Najjar Type I• Features:
– Severe lifelong jaundice with high risk of kernicterus,
– No haemolysis or significant hepatocellular dysfunction.
• Tests:– UGT1A1 enzyme assay in liver.

04/15/23 43
Gilbert SyndromeGilbert Syndrome• Features:
– Chronic mild fluctuating unconjugated hyperbilirubinaemia,
– No haemolysis or hepatocellular dysfunction.
• Tests:– UGT1A1 targeted mutation analysis.

04/15/23 44
G6PD deficiencyG6PD deficiency
• Features:– Haemolytic anaemia,– Frequently precipitated by illness or
oxidizing drugs.
• Tests:– Quantitative G6PD analysis.

04/15/23 45
Pyruvate Kinase deficiencyPyruvate Kinase deficiency
• Features:– Haemolytic anaemia of variable severity.
• Tests:– Pyruvate kinase isoenzyme analysis.

04/15/23 46
Indicators of HaemolysisIndicators of Haemolysis
• Rapidly rising bilirubin,
• Falling hemoglobin.

04/15/23 47
History and Physical Examination• Note adequacy of feeding, passing stools, and
voiding (risk factors for increased enterohepatic circulation of bilirubin).
• Examine for the following:– Well being (no sepsis),– Growth parameters,– Bruising and cephalhematoma (increased bilirubin
production),– Pallor, oedema, and hepatosplenomegaly (indicators
of haemolysis and CHF).
04/15/23 48
Growth ParametersGrowth Parameters
• SGA infants are likely to be plethoric resulting in higher bilirubin and requiring earlier phototherapy.
• This may be symptomatic of intrauterine infection and hence likely conjugated jaundice.

04/15/23 49
Prolonged JaundiceProlonged Jaundice

04/15/23 50
DefinitionDefinition
Jaundice persisting in newborn beyond 10 (14) days of life is said to be prolonged.

04/15/23 51
Types of Prolonged JaundiceTypes of Prolonged Jaundice
• Unconjugated Hyperbilirubinaemia.
• Conjugated Hyperbilirubinaemia.
04/15/23 52
Causes of ProlongedCauses of ProlongedUnconjugated HyperbilirubinaemiaUnconjugated Hyperbilirubinaemia
• Breast Milk Jaundice.
• Hypothyroidism.
• Intestinal Stasis.
• Hemolytic causes.

04/15/23 53
Breast Milk JaundiceBreast Milk Jaundice• Most common cause of prolonged
unconjugated Hyperbilirubinaemia.
• Total Serum Bilirubin usually < 200 mcg/L
• Conjugated bilirubin < 20% (Normally > 25%)

04/15/23 54
Breast Milk JaundiceBreast Milk Jaundice (continued)
Beta glucuronidase present in Breast Milk
Bilirubin diglucuronide
UC Bilirubin Glucuronic Acid
Absorbed from GIT
Hyperbilirubinaemia(Unconjugated)

04/15/23 55
Breast Milk Jaundice Breast Milk Jaundice (continued)
• Baby well,
• No treatment required,
• Settles by 6 weeks
(occasionally up to 4 months.

04/15/23 56
Lucy Driscoll SyndromeLucy Driscoll Syndrome
• Inhibitors of bilirubin glucuronide is present in the mother’s milk.
• Sometimes severe enough to require exchange transfusion.

04/15/23 57
HypothyroidismHypothyroidism
• A heavy weight, sluggish baby with feeding difficulty and prolonged jaundice s/o congenital hypothyroidism.
• Investigation:– Thyroid Function Test.

04/15/23 58
Intestinal StasisIntestinal Stasis
• 2nd most common cause of prolonged unconjugated hyperbilirubinaemia.
• Due to increased enterohepatic circulation of bilirubin.

04/15/23 59
MechanismMechanism
• Normally 75% of conjugated bilirubin is excreted in feces and 25% of is broken down to unconjugated form in duodenum and is absorbed into circulation.
• When there is stasis, the break-down to unconjugated form increases significantly to cause hyperbilirubinaemia.

04/15/23 60
Causes of Intestinal StasisCauses of Intestinal Stasis• Hirschsprung disease.
• Intestinal atresia.
• Pyloric Stenosis.
• Meconium ileus of Cystic Fibrosis.

04/15/23 61
ProlongedProlongedConjugatedConjugated
HyperbilirubinaemiaHyperbilirubinaemia

04/15/23 62
Causes of prolonged Causes of prolonged conjugated hyperbilirubinaemiaconjugated hyperbilirubinaemia
• Cholestasis syndrome– Intrahepatic cholestasis
• Neonatal Hepatitis• Intrahepatic biliary atresia.
– Extrahepatic cholestasis• Congenital Biliary Atresia.
04/15/23 63
InvestigationsInvestigations
• Serum Bilirubin:– Total– Direct (conjugated)– Indirect (Unconjugated)
• Hepatobiliary ultra-sound study or
• Technetium-99 HIDA cholescintigraphy.
• Percutaneous liver-biopsy.

04/15/23 64
Stool ColourStool Colour
• Stool partially pale or intermittently pale + IUGR = Neonatal Hepatitis (intrahepatic cholestasis).
• Stool completely and persistently pale and lasting longer that 2 weeks + hard liver or unconjugated hyperbilirubinaemia = Extrahepatic cholestasis (congenital biliary atresia)





























