Embed Size (px)
Citation preview

New Articles onEmergency Airway Management
John Fowler, MD
Kent Hospital
İzmir, Türkiye

Conflicts of Interest: none

Topics
• Pre-Prehospital (public access)
• Prehospital (ambulance)
• Equipment
• Technique
• Adjuncts

Public access airways?!
• 2013, Eur J Emerg Med:“Laryngeal tube placement on manikin bylaypersons: is there a possibility for 'publicaccess airway management'?”
• Visitors and patients at a military hospital
• Picture cards with and without words
• Card was shown – placement of LT in manikin –demonstration – placement of LT again
• Time from card to first breath



Laryngeal tube placement on manikin bylaypersons: is there a possibility for
'publicaccess airway management'?
• 71 participants,mean age 43
• Shown one card
• First attempt
• Given demonstration
• Shown the other card
• Second attempt
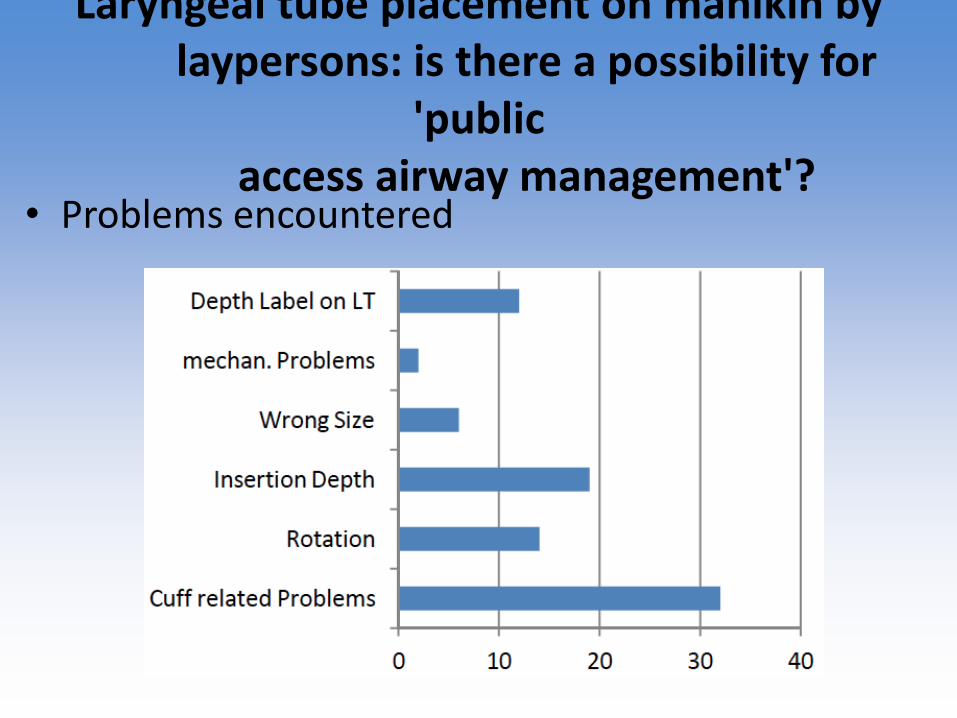
Laryngeal tube placement on manikin bylaypersons: is there a possibility for
'publicaccess airway management'?
• Problems encountered

Disadvantages of standard C-collars
• Airway maneuvers difficult
• Uncomfortable
• Hinder venous return?

• Head/neck fixation
• No pressure onjugular vein
• Comfortable
• Easy to apply
• Airway maneuversnot hindered
2014 EMJ “The ‘Necksafe’ head articulation control system: a novel cervical immobilisation device”

2013, JEM “Videolaryngoscopy With Glidescope Reduces Cervical Spine Movement In Patients With Unsecured Cervical Spine”
• in the OR on healthy patients• Detailed measuring of displacement/angulation

2013, JEM “Videolaryngoscopy With Glidescope Reduces Cervical Spine Movement In Patients With Unsecured Cervical Spine”
Glidescope: less movementcompared to standardlaryngoscopy with aMacintosh blade

Traumatic Brain Injury
• Keep patients from experiencing
– hypoxia
– hypotension
– hypercarbia / hypocarbia
– hyperthermia

2013 AnnEM “Incidence of Hypoxemia During Rapid Sequence Intubation of Head-Injured Patients in theEmergency Department”
• Prospective, 5-year observational study• 435 underwent RSI, 350 had O2 sats recorded
• What percent had more than a 10% fall in O2 saturation?

2013 AnnEM “Incidence of Hypoxemia During Rapid Sequence Intubation of Head-Injured Patients in theEmergency Department”
• Prospective, 5-year observational study• 435 underwent RSI, 350 had O2 sats recorded
• What percent had more than a 10% fall in O2 saturation? 20% !

2013 AnnEM “Incidence of Hypoxemia During Rapid Sequence Intubation of Head-Injured Patients in theEmergency Department”
• Prospective, 5-year observational study• 435 underwent RSI, 350 had O2 sats recorded
• What percent had more than a 10% fall in O2 saturation? 20% !
• A reminder to do apneicoxygenation during RSI

2014 EMJ “Prehospital use in emergency patients of a laryngeal mask airway by ambu. paramedics is a safe and effective alternative for endotracheal intubation”
• NL, intubation failure rate was 12%.
• After training, LMA-S was used 50 times in 9 months (33 cardiac arrests, etc.)
• 2/3 had prior attempts to intubate

2014 EMJ “Prehospital use in emergency patients of a laryngeal mask airway by ambu. paramedics is a safe and effective alternative for endotracheal intubation”
• NL, intubation failure rate was 12%.
• After training, LMA-S was used 50 times in 9 months (33 cardiac arrests, etc.)
• First attempt successful in 49 pts
• Second attempt successful in 1 pt
• All had adequate oxygenation

2014 EuJEM “Emergency airway management by paramedics: comparison between standard endo-
tracheal intubation, laryngeal mask airway, and I-gel”
• 72 paramedics, randomly intubated manikinwith iGel or LMA or ETT
• Outcomes
– success (lungs inflate when BVM used)
– time from insertion to cuff inflation

2014 EuJEM “Emergency airway management by paramedics: comparison between standard endo-
tracheal intubation, laryngeal mask airway, and I-gel”
• 72 paramedics, randomly intubated manikinwith iGel or LMA or ETT

2014 Resuscitation “Intubating LMA placement by non-physician healthcare providers in
management out-of-hospital cardiac arrests”
• Formal protocol for iLMA placementby ambulance nurses (France)
• Observational study
• 302 iLMA attempts, successfulventilation in 96% (n: 290)
• Intubation attempted through iLMA in 265, successful in 96% (n: 254)

2014, EuJEM “Bag-mask ventilation and direct laryngoscopy versus intubating LMA: a manikin study
of hands-on times during CPR
• Manikin study
• Paramedics and CPR-trained medical students
• All did four scenarios, in random order
– iLMA and BVM-DL ± normal airway and difficult airway

2014, EuJEM “Bag-mask ventilation and direct laryngoscopy versus intubating LMA: a manikin study
of hands-on times during CPR
• Manikin study
• Paramedics and CPR-trained medical students
• All did four scenarios, in random order
– iLMA and BVM-DL ± normal airway and difficult airway

2014, EuJEM “Bag-mask ventilation and direct laryngoscopy versus intubating LMA: a manikin study
of hands-on times during CPR
• All did four scenarios, in random order
– iLMA and BVM-DL ± normal airway and difficult airway

2014, EuJEM “Bag-mask ventilation and direct laryngoscopy versus intubating LMA: a manikin study
of hands-on times during CPR
• All did four scenarios, in random order
– iLMA and BVM-DL ± normal airway and difficult airway
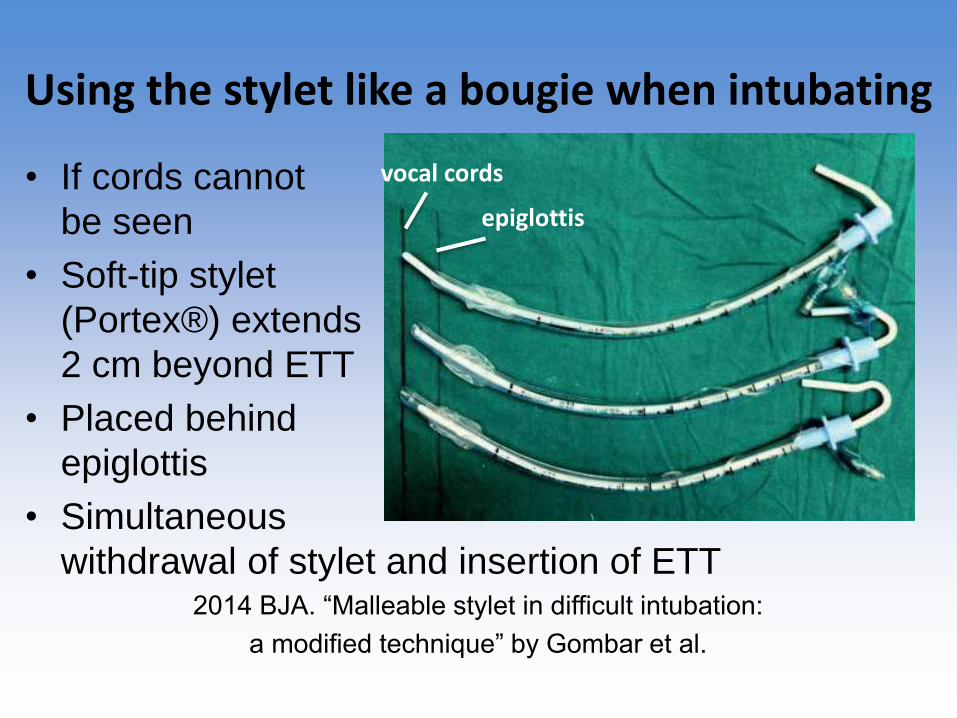
Using the stylet like a bougie when intubating
• If cords cannot
be seen
• Soft-tip stylet
(Portex®) extends
2 cm beyond ETT
• Placed behind
epiglottis
• Simultaneous
withdrawal of stylet and insertion of ETT2014 BJA. “Malleable stylet in difficult intubation:
a modified technique” by Gombar et al.
epiglottis
vocal cords

2014, AnnEM, “A Comparison of Two Open Surgical Cricothyroidotomy Techniques by Military Medics
Using a Cadaver Model”
• 15 US Army medics, on cadavers
• Standard surgical cricothyrotomy vs CricKey®
• Outcome measures
– first-pass success
– procedural time (incision – first ventilation)

2014, AnnEM, “A Comparison of Two Open Surgical Cricothyroidotomy Techniques by Military Medics
Using a Cadaver Model”
• 15 US Army medics, on cadavers
• Standard surgical cricothyrotomy vs CricKey®

2014, AnnEM, “A Comparison of Two Open Surgical Cricothyroidotomy Techniques by Military Medics
Using a Cadaver Model”
• 15 US Army medics, on cadavers
• Standard surgical cricothyrotomy vs CricKey®

2014, AnnEM, “A Comparison of Two Open Surgical Cricothyroidotomy Techniques by Military Medics
Using a Cadaver Model”
• 15 US Army medics, on cadavers
• Standard surgical cricothyrotomy vs CricKey®
First-pass success 66% 100%
Time until first ventilation 72 sec. 35 sec.

2014, JEM “A Dual-use Laryngoscope to Facilitate Apneic Oxygenation”
• Manikin study with a test lung/pharynx
• No O2, nasal O2, laryngoscope O2, intratracheal O2
15 L/min 15 L/min 15 L/min

2014, JEM “A Dual-use Laryngoscope to Facilitate Apneic Oxygenation”
• Manikin study with a test lung/pharynx
• No O2, nasal O2, laryngoscope O2, intratracheal O2
15 L/min 15 L/min 15 L/min

2014, JEM “A Dual-use Laryngoscope to Facilitate Apneic Oxygenation”
• No O2, nasal O2, laryngoscope O2, intratracheal O2

Sonographic confirmation ofendotracheal intubation
• As the tube passes into the trachea
• Lung sliding
• Diaphragm movement

2014 J Ultrasound Med “Sonographic Confirmation of Intub.: Comparison of 3 Methods in a Pig Model”
• Animal study, 25 pigs
• Randomly intubated trachea or esophagus
– As the tube passes into the trachea
– Lung sliding
– Diaphragm movement

2014 J Ultrasound Med “Sonographic Confirmation of Intub.: Comparison of 3 Methods in a Pig Model”
• Animal study, 25 pigs
• Randomly intubated trachea or esophagus
– As the tube passes into the trachea 12.5 sec
– Lung sliding 14.0 sec
– Diaphragm movement 21.0 sec

2014 J Ultrasound Med “Sonographic Confirmation of Intub.: Comparison of 3 Methods in a Pig Model”
• Animal study, 25 pigs
• Randomly intubated trachea or esophagus
– As the tube passes into the trachea 12.5 sec
– Lung sliding 14.0 sec
– Diaphragm movement 21.0 sec
• Accuracy similar with all techniques

Depth of endotracheal tube placement?
• Ideally, the cuff of the ETT should lie underneath the suprasternal notch
2014 Resuscitation, “Tracheal rapid ultrasound saline test (T.R.U.S.T.) for confirming correct endotracheal tube depth in children” by Tessaro…
• 42 elective pediatric cases at an outpt surg. center

Depth of endotracheal tube placement?

Depth of endotracheal tube placement?
• 6 sec. videoclip was taken, just above suprasternal notch
– before intubation
– with the ETT in the right mainstem bronchus (then cuff filled with saline)
– with the ETT in the trachea, (then cuff filled with saline)
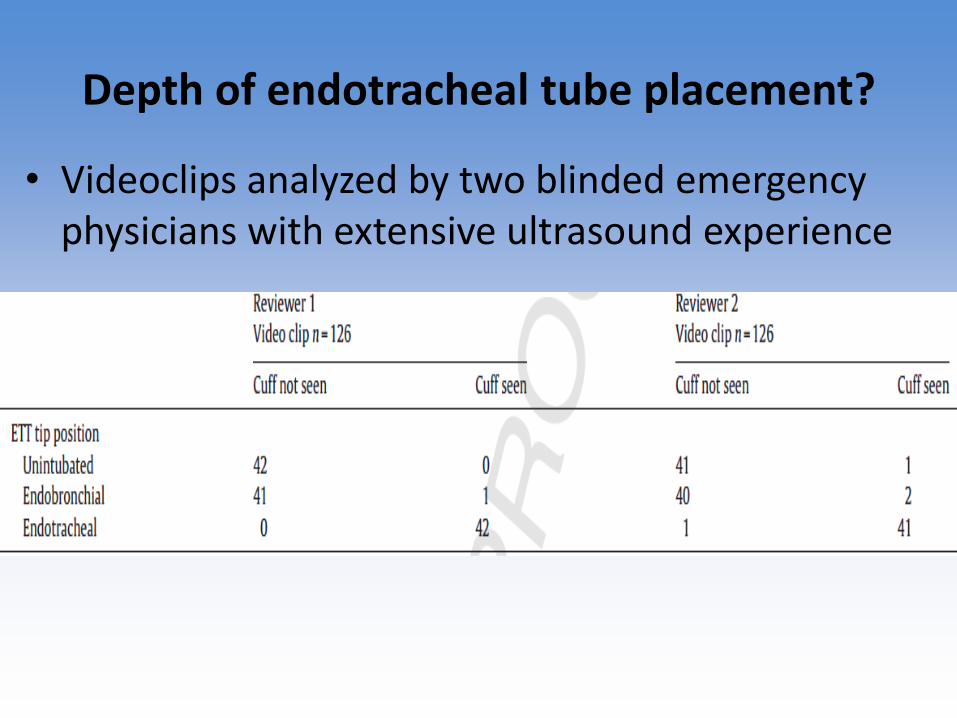
Depth of endotracheal tube placement?
• Videoclips analyzed by two blinded emergency physicians with extensive ultrasound experience

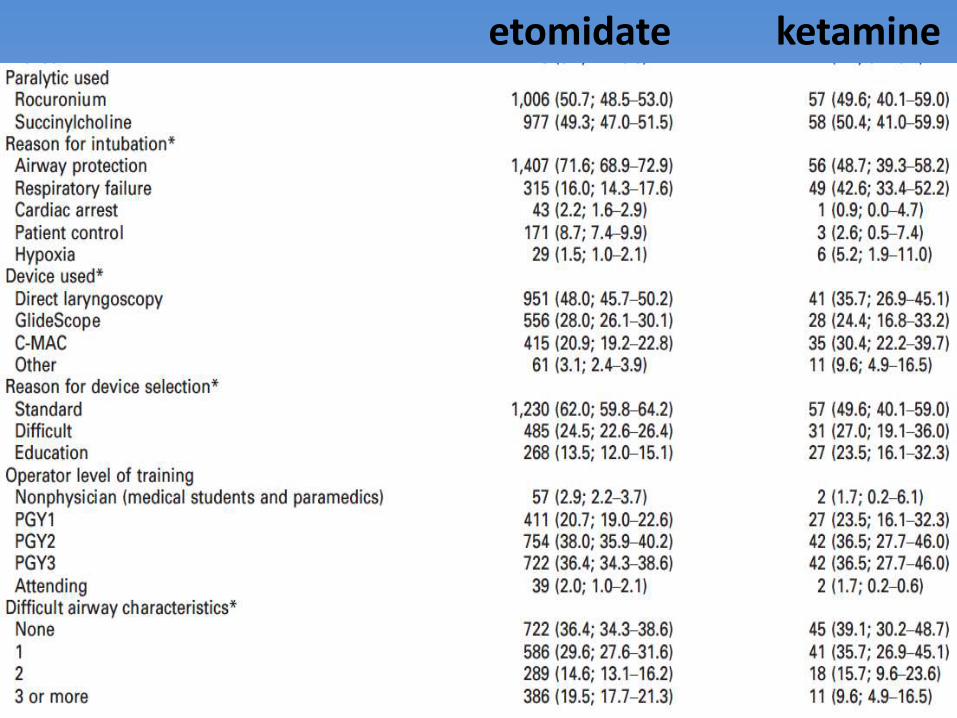
2014 AcadEM “Retrospective Analysis of Etomidate vs Ketamine for First-pass Intubation
Success in an Academic ED”
• Review of 5-years of prospectively collected data
• Outcome: first-pass success of ET tube
• RSI with
– etomidate n= 1,983
– ketamine n= 115
etomidate ketamine
• Review of 5-years of prospectively collected data
• Outcome: first-pass success of ET tube
• RSI with
– etomidate n= 1,983 first pass success 77%
– ketamine n= 115 first pass success 79%

2014 AcadEM “Retrospective Analysis of Etomidate vs Ketamine for First-pass Intubation
Success in an Academic ED”
• RSI with
– etomidate n= 1,983 first pass success 77%
– ketamine n= 115 first pass success 79%

2013 EMJ “Pharmacologically assisted laryngealmask insertion: a consensus statement”
• PALM: for whom?
– low GCS, airway compromise/soiling
– EtCO2 monitoring mandatory
• PALM: what?
– midazolam or ketamine, then supraglottic airway
• if PALM fails, next choice is surgical airway
• need checklist and data regarding this approach

2014, JEM “Trauma Airway Management”
• General approach
• Difficult airway algorithm

2014 Sept; Scand J Trauma Resus EM“Development of a standard operating
procedure and checklist for rapid sequence
induction in the critically ill”

2014 Sept; Scand J Trauma Resus EM“Development of a standard operating
procedure and checklist for rapid sequence
induction in the critically ill”• SOP and checklists… just like pilots

2014 Sept; Scand J Trauma Resus EM“Development of a standard operating
procedure and checklist for rapid sequence
induction in the critically ill”• Evaluate the airway beforehand
• Patient position
• Optimize physiology
• Monitoring the patient
• Equipment
• IVs – drugs - fluids

2014 Sept; Scand J Trauma Resus EM“Development of a standard operating
procedure and checklist for rapid sequence
induction in the critically ill”• Evaluate the airway beforehand
• Patient position
• Optimize physiology
• Monitoring the patient
• Equipment
• IVs – drugs – fluids Time Out

• Am I likely to encounter a:
• difficult laryngoscopy?
• difficult facemask ventilation?
• difficult supraglottic airway?
• difficult cricothyrotomy?
2014 Sept; Scand J Trauma Resus EM“Development of a standard operating
procedure and checklist for rapid sequence
induction in the critically ill”

• Patient positioning
2014 Sept; Scand J Trauma Resus EM“Development of a standard operating
procedure and checklist for rapid sequence
induction in the critically ill”

• Optimizing the patient’s physiology
• NG tube
• pre-oxygenation (give ketamine if agitated)
• if SaO2 is below 97% use NIPPV or high-flow nasal O2
• apneic oxygenation (15L/min O2 via nasal prongs)
• optimize intravascular volume (preinduction fluid bolus…)
2014 Sept; Scand J Trauma Resus EM“Development of a standard operating
procedure and checklist for rapid sequence
induction in the critically ill”

2014 Sept; Scand J Trauma Resus EM“Development of a standard operating
procedure and checklist for rapid sequence
induction in the critically ill”• Monitorization: EKG, BP, SaO2, EtCO2, (art. line…)
• Equipment (see dump sheet figure)
• O2 x 2, suction tip under pillow, OPA, NPA, LMA
• laryngoscope x 2, ET tube x 2, gel, bougie, syringe, tie
• cric kit (scalpel, finger, 10F bougie, 6.0 ETT; or Melker)
• IVs – Medications
• IV x 2 (IO?), ketamine ± opioid, paralytic, other (epi, atropine, fluids, metaraminol)
Time Out

“SOP and checklist for
rapid sequenceinduction
in the critically ill”

“SOP and checklist for
rapid sequenceinduction
in the critically ill”

Use pediatric BVMs for ventilating adults
• Results in a lower incidence of hypocarbia

Airway Safety Lines
• 2013, from the Vortex folks in Australia
• http://monashanaesthesia.org/difficultairway

Airway Safety Lines
• Extend the time to critical desaturation withpreoxygenation, proper patient positioning, etc.
• Shorten the time to performance of a non-surgical airway through preparation, training, etc.

Standard mask ventilation vs NuMask®
• s
Abstract
Objective: To compare a novel intra-oral
mask (IOM) to standard mask (SM)
ventilation
Methods: The study is designed as a
single blinded, cross-over study using a
fresh (un-embalmed) edentulous cadaver
and a convenience sample of 19 novice to
experienced allied health providers. A
tracheotomy was performed with a
retrograde technique using an 8 mm
endotracheal tube (ETT). A ventilator was
attached to the masks studied and set on
volume control, rate of 20, with tidal
volumes (Vt) of 0.5 L, 1.0L, and 1.5 L.
Results: One hundred and fourteen
(n=114) ventilation episodes were
recorded, fifty-seven (57) of each mask.
The mean leak measured at the respective
volumes for the SM and the IOM were 0.13
L vs. 0.11 L (p=0.10), 0.40 L vs0.31 L
(p<0.05), 0.84 L vs 0.50 L (p,0.01).
Conclusions: The novel intraoral mask is
equivalent to standard mask in ability to
maintain a seal as measured in a cadaver
model at the 0.5 L Vt. At the 1.0 and 1.5 L
volumes the IOM was superior to standard
Mask
Fresh (unembalmed) edentulous cadaver
Warmed for 4.5 hrs
Tracheotomy with retrograde insertion of
8.0 ETT connected to a lung analog and in-
line Wrights Spirometer
Convenience sample of 19 novice to
experienced allied health providers
ventilated with Intra-oral or Standard Mask
for 2 minutes at each of 3 ventilator
settings
Methods Results
Total 114 (n=114) ventilation episodes
SM n=57, IOM n=57
At the 500mL ventilator output volume,
the BVM and IOM mean tidal volumes ±
S.D. were 380 ± 60 mL and 380 ± 70 mL,
respectively (P =.10; Fig. 1).
At the 1 L ventilator volume, the BVM
and NuMask tidal volumes were 600 ± 120
mL and 670 ± 150 mL, respectively (P <
0.1; Fig. 2).
At the 1.5 L, the BVM and NuMask tidal
volumes were 720 ± 220 mL and 950 ±
160 mL, respectively (P < 0.001; Fig. 3).
Conclusion
Using a cadaver model, a novel intra-oral
mask is equivalent to standard mask in its
ability to obtain and maintain a seal at Vt of
0.5 L. At a Vt of 1.0L and 1.5 L the intra-
oral mask was superior to standard mask.
Since the IOM (NuMask ®) is dependant
on the mucosal surface to obtain a seal – it
may offer advantages over standard mask,
especially if higher pressures are required
for ventilation such as CPAP.
Comparison of a Novel Intra-oral Mask (NuMask®)
to Standard Mask Ventilation Using a Cadaver ModelPhillip L. Coule, MD1; Andrew J. Mazzoli PhD1; James M. Todaro MS12
1. Department of Emergency Medicine and School of Allied Health Sciences, Medical College of Georgia. Augusta, Georgia
2. Columbia University College of Physicians and Surgeons, New York, New York.
Medical College of Georgia Department of Emergency Medicine Printed by
Newport HT50 Ventilator set at rate of 20
and set to deliver Vt of 0.5 L, 10 L and 1.5
L for each mask and for each volunteer
20 breaths delivered with each mask and
at each ventilator setting
Minute ventilation and leak were
calculated for each setting and mask
0
200
400
600
800
1000
1200
1400
Tid
al V
olu
me
(m
L)
Figure 3. Delivered Tidal Volume at1.5 L Set Ventilator Volume
Standard Mask Intra Oral Mask
0
100
200
300
400
500
600
Tid
al V
olu
me
(m
L)
Figure 1. Delivered Tidal Volume at500ml Set Ventilator Volume
Standard Mask Intra Oral Mask
0
100
200
300
400
500
600
700
800
900
1000
Tid
al V
olu
me
(m
L)
Figure 2. Delivered Tidal Volume at1 L Set Ventilator Volume
Standard Mask Intra Oral Mask

NuMask®: a clinical study is needed…
• s

NuMask vs standard mask: cadaver study
2012, “Workload Comparison of Intraoral Mask to Standard Mask Ventilation Using a Cadaver Model”
• Used both techniques on cadavers then answered a workload-ease of use questionnaire
Standard mask NuMask

NuMask vs standard mask: cadaver study
• Performance was similar
• NuMask was a bit easier to use

2013, AnnEM, “Trauma Intubation Protocol Success Before and After Acquisition of Video Laryngoscopy”
• Academic ED, 2007-2009 – VL – 2009-2012
• Protocol (pre- and post-VL)
– First attempt by senior resident or attending
– Second attempt by senior resident or attending
– Third attempt by anesthesiologist

2013, AnnEM, “Trauma Intubation Protocol Success Before and After Acquisition of Video Laryngoscopy”
• Success on first or second attempt
– Pre-VL: 90% Post-VL: 95%
• Intubations by anesthesiologist
– Pre-VL: 3.4% Post-VL: 0.8%
• Full view of vocal cords
– Pre-VL: 49% Post-VL: 60%

2013, Anesth Analg “Thyromental Height: A New Clinical Test for Prediction of Difficult Laryngoscopy”
• 314 patients in the OR
• Compared actual laryngoscopic view (Cormack and Lehane grade) with prediction scores
– modified Mallampati
– thyromental distance
– sternomental distance
– thyromental height

2013, Anesth Analg “Thyromental Height: A New Clinical Test for Prediction of Difficult Laryngoscopy”
• Compared actual laryngoscopic view (Cormack and Lehane grade) with prediction scores
– modified Mallampati
– thyromental distance
– sternomental distance
– thyromental height

2013, Anesth Analg “Thyromental Height: A New Clinical Test for Prediction of Difficult Laryngoscopy”
• Compared actual laryngoscopic view (Cormack and Lehane grade) with prediction scores
– modified Mallampati
– thyromental distance
– sternomental distance
– thyromental height >50 mm

2014, Indian J Anaesth “Nasopharyngeal airway as a diagnostic and therapeutic tool in difficult airway”
• Don’t forget to use a nasal airway, to optimize oxygenation.
• Oxygen can be given directlythrough the airway
• Fiberoptic scope can beplaced through the airwayif necessary

2014, Resuscitation “The clinical significance of a failed initial intubation attempt during ED resusci-tation of out-of-hospital cardiac arrest patients”
• Retrospective, 4-years of data
435 pts without, 77 with failed initial intub.
ROSC 60% 43%
Time to ROSC 10 min. 12 min.
Surv. to discharge 8% 10%

2014, Resuscitation “The clinical significance of a failed initial intubation attempt during ED resusci-tation of out-of-hospital cardiac arrest patients”

Why not abandon direct laryngoscopy completely for videolaryngoscopy?

Why not abandon direct laryngoscopy completely for videolaryngoscopy?
This is why!

2014, Peds Emerg Care “Alternative Airways for the Pediatric Emergency Department”
• Supraglottic airways
– laryngeal mask
– air-Q mask laryngeal
– iGel
– laryngeal tube








![The Emergency Airway Algorithmsdocuments.theairwaysite.com/documents/Manual of Emergency Airway...The Emergency Airway Algorithms 2 Ron M. Walls GRBQ375-3620G-C02[8-22].qxd 01/24/2008](https://img.dokumen.tips/doc/110x75/5af0cfa37f8b9abc788da848/the-emergency-airway-of-emergency-airwaythe-emergency-airway-algorithms-2-ron.jpg)





















