Embed Size (px)
Citation preview

1
PocketParamedic.org [email protected]
Pocket Paramedic 2013
By Jason Houghton
A collaboration of useful guidelines In a quick reference pocket book;
tailored for pre-hospital care.

2
Pocket Paramedic 2013 “An elegant solution to a simple problem” A collaboration of useful guidelines in a quick reference pocket book tailored for pre-hospital care. This handy pocket book resulted from my quest to consolidate the most relevant and useful guidance into a single source; something that can be carried in your pocket at all times - whenever you may need it. Pocket Paramedic is 100% non-profit. Sold at cost. Hopefully, this will mean more people can benefit from it. Download the FREE electronic edition from: PocketParamedic.org I hope you find it useful. Jason Houghton - Paramedic [email protected]

3
Contents
Adults Algorithms and Charts
4
Paediatrics Algorithms and Charts
19
Obstetrics Useful Information and Charts
32
Equipment Instructions and Guidance
37
Assessment & History Taking Aid memoirs, Acronyms and Diagnosis
45
Trauma & Medical Emergencies Useful Information and Charts
53
Anatomy Diagrams and Terminology
62
ECG & ETCO2 Interpretation Examples and Explanations
68
Major Incidents Acronyms and Plan of Action
77
Infection Prevention & Control Useful Information
91
Key Contacts Phone Numbers
96
Notes Extra Space
97
References Credits and Information Sources
99

4
Adults Algorithms and Charts
Adult Basic Life Support 5
Adult Advanced Life Support 6
Adult Cardiac Arrest 7
Adult Bradycardia 8
Adult Tachycardia (With Pulse) 9
Adult Chocking Treatment 10
In Hospital Resuscitation 11
AED Algorithm 12
Adult Glasgow Coma Scale 13
Adult Normal Ranges & Drug Dosages 14
Normal Peak Flow Readings 15
Normal Peak Flow Readings Chart - Men 16
Normal Peak Flow Readings Chart - Women 17
Adult Analgesic Ladder 18

5
Adult Basic Life Support 10
Ad
ult
s

6
Adult Advanced Life Support 10 A
du
lts

7
Adult Cardiac Arrest 10
Ad
ult
s

8
Adult Bradycardia 10 A
du
lts

9
Ad
ult
s
A
du
lt Tachyca
rdia (W
ith P
ulse
) 10

10
Adult Choking Treatment 10 A
du
lts

11
In Hospital Resuscitation 10
Ad
ult
s

12
AED Algorithm 10 A
du
lts

13
Adult Glasgow Coma Scale
Eyes
Verbal
Motor
4 Opens Eyes Spontaneously
3 Opens Eyes in Response to Voice
2 Opens Eyes in Response to Painful Stimuli
1 Does Not Open Eyes
5 Oriented, Converses Normally
4 Confused, Disoriented
3 Utters Inappropriate Words
2 Incomprehensible Sounds
1 Makes No Sounds
6 Obeys Commands
5 Localizes Painful Stimuli
4 Flexion / Withdrawal to Painful Stimuli
3 Abnormal Flexion to Painful Stimuli (Decorticate)
2 Extension to Painful Stimuli (Decerebrate)
1 Makes No Movements
Ad
ult
s

14
Adult Normal Ranges & Dosages
Parameter Unit Value
Heart Rate BPM 60 - 100
Respiratory Rate BPM 12 - 19
SpO2 % ≥ 95
BP Systolic mmHg 100 - 170
BP Diastolic mmHg 60 - 80
Blood Glucose (BM) mmol/L 5 - 10.9
Energy 1st Shock Joules 200
Energy 2nd Shock Joules 300
Energy 3rd Shock Joules 360
Adrenaline 1:10000 mg (ml) 1 (10)
Amiodarone mg (ml) 300 (10)
Amiodarone (Refractory VF/VT) mg (ml) 150 (5)
Ad
ult
s

15
Normal Peak Flow Readings 8 EU/EN13826 PEF Meters Only
Ad
ult
s

16
Ad
ult
s
No
rmal
Pe
ak F
low
Re
adin
gs C
har
t -
Me
n 8

17
Ad
ult
s
N
orm
al Pe
ak Flow
Re
adin
gs Ch
art - Wo
me
n 8

18
Adult Analgesic Ladder (12 Years and Older)
Pain Score Medical Pain
Trauma, Orthopaedic,
Musculoskeletal & Soft tissue Pain
0 – 3 Mild Pain
Consider Entonox +/-
Ibuprofen 400MG
Consider Entonox +/-
Ibuprofen 400MG
4 – 6 Moderate Pain
Consider Entonox +/-
Morphine 2.5 to 5mg
(Max 20mg)
Consider Entonox +/-
Ibuprofen 400MG
7 – 10 Severe
Pain
Consider Entonox +/-
Morphine 2.5 to 5mg
(Max 20mg)
Consider Entonox +/-
Ibuprofen 400MG +/-
Morphine 2.5 to 5mg
(Max 20mg)
For Cardiac Related Chest Pain Morphine Should be Considered in the First Instance
Ad
ult
s

19
Paediatrics
Paediatric Basic Life Support 20
Paediatric Advanced Life Support 21
Paediatric Cardiac Arrest 22
Newborn Advanced Life Support 23
Paediatric Chocking Treatment 24
Paediatric Glasgow Coma Scale 25
Paediatric Arrest Calculations 26
Paediatric Normal Ranges & Arrest Dosages 27
Normal Peak Flow Readings Chart - Paediatric 28
Pain Assessment Faces 29
FLACC Scale Pain Assessment 30
Paediatric Analgesic Ladder 31

20
Paediatric Basic Life Support 10 P
aed
iatr
ics

21
Paediatric Advanced Life Support 10
Pa
edia
tric
s

22
Paediatric Cardiac Arrest 10 P
aed
iatr
ics

23
Newborn Life Support 10
Pa
edia
tric
s

24
Paediatric Choking Treatment 10 P
aed
iatr
ics

25
Paediatric Glasgow Coma Scale
Eyes
Verbal
Motor
4 Opens Eyes Spontaneously
3 Opens Eyes in Response to Speech
2 Opens Eyes in Response to Painful Stimuli
1 Does Not Open Eyes
5 Smiles, Orients to Sounds, Objects, Interacts
4 Cries but Consolable, Inappropriate Interactions
3 Inconsistently Inconsolable, Moaning
2 Inconsolable, Agitated
1 No Verbal Response
6 Infant Moves Spontaneously or Purposefully
5 Infant Withdraws from Touch
4 Infant Withdraws from Pain
3 Abnormal Flexion to Pain for Infant (Decorticate)
2 Extension to Pain (Decerebrate)
1 No motor response
Pa
edia
tric
s

26
Paediatric Arrest Calculations 10 WEIGHT
ENERGY
TUBE SIZE
FLUID
ADRENALINE AMIODARONE
GLUCOSE
Age Formula 0 – 12 Months Weight (kg) = (Age in Months x 0.5) + 4 1 – 5 Years Weight (kg) = (Age in Years x 2) + 8 6 – 12 Years Weight (kg) = (Age in Years x 3) + 7
Age Formula 0 – 12 Years Joules = Weight (kg) x 4j
Age Formula Pre Term 2.5mm Neonates 3 – 3.5mm
1 – 10 Years Internal diameter (mm) = (Age/4) + 4 Length (cm) = (Age/2) + 12
Type Formula (0 – 12 Years) Medical Bolus (ml) = Weight (kg) x 20ml Trauma Bolus (ml) = Weight (kg) x 10ml Concealed Haem Bolus (ml) = Weight (kg) x 5ml
Formula (1:10,000) (0 – 12 Years) Formula (300mg in 10ml) (0 – 12 Years)
Dose (mcg) = Weight (kg) x 10mcg (0.1ml)
Dose (mg) = Weight (kg) x 5mg …Then ml’s = Dose (mg) / 30)
Age Formula 0 – 12 Years Dose (ml) 10% Glucose = Weight (kg) x 2ml
Resuscitation Council UK 2010
Pa
edia
tric
s

27
Age
HR
(BP
M)
RR
(PM
) B
P (Systo
lic) W
eigh
t (kg)
Ene
rgy (Jo
ule
s) Tu
be
(mm
) Flu
ids
(ml)
Ad
ren
aline
(ml) (m
cg) A
mio
daro
ne
(ml) (m
g) G
luco
se (m
l) B
irth 1
10
-16
0 3
0-4
0 7
0-9
0 4
20
3 8
0 0
.40
(40
) 0
.67
(20
) 8
1 M
1
10
-16
0 3
0-4
0 7
0-9
0 4
.5 2
0 3
90
0.4
5 (4
5)
0.7
5 (2
2.5
) 9
3 M
1
10
-16
0 3
0-4
0 7
0-9
0 5
.5 2
5 3
.5 1
10
0.5
5 (5
5)
0.9
2 (2
7.5
) 1
1 6
M
11
0-1
60
30
-40
70
-90
7 4
0 4
14
0 0
.70
(70
) 1
.17
(35
) 1
4 9
M
11
0-1
60
30
-40
70
-90
8.5
40
4 1
70
0.8
5 (8
5)
1.4
2 (4
2.5
) 1
7 1
2 M
1
10
-15
0 2
5-3
5 8
0-9
5 1
0 4
0 4
.5 2
00
1.0
(10
0)
1.6
7 (5
0)
20
18
M
10
0-1
50
25
-35
80
-95
11
50
4.5
22
0 1
.1 (1
10
) 1
.83
(55
) 2
2 2
Yr
95
-14
0 2
5-3
0 8
0-1
00
12
50
5 2
40
1.2
(12
0)
2.0
0 (6
0)
24
3 Y
r 9
5-1
40
25
-30
80
-10
0 1
4 6
0 5
28
0 1
.4 (1
40
) 2
.30
(70
) 2
8 4
Yr
95
-14
0 2
5-3
0 8
0-1
00
16
70
5 3
20
1.6
(16
0)
2.6
6 (8
0)
32
5 Y
r 8
0-1
20
20
-25
90
-10
0 1
8 8
0 5
.5 3
60
1.8
(18
0)
3.0
0 (9
0)
36
6 Y
r 8
0-1
20
20
-25
80
-11
0 2
5 8
0 6
50
0 2
.5 (2
50
) 4
.20
(12
5)
50
7 Y
r 8
0-1
20
20
-25
90
-11
0 2
8 1
00
6 5
60
2.8
(28
0)
4.6
7 (1
40
) 5
6 8
Yr
80
-12
0 2
0-2
5 9
0-1
10
31
10
0 6
.5 6
20
3.1
(31
0)
5.1
2 (1
55
) 6
2 9
Yr
80
-12
0 2
0-2
5 9
0-1
10
34
12
0 6
.5 6
80
3.4
(34
0)
5.6
7 (1
70
) 6
8 1
0 Y
r 8
0-1
20
20
-25
90
-11
0 3
7 1
30
7 7
40
3.7
(37
0)
6.1
7 (1
85
) 7
4 1
1 Y
r 8
0-1
20
20
-25
90
-11
0 4
0 1
40
7 8
00
4.0
(40
0)
6.6
7 (2
00
) 8
0
P
aed
iatric No
rmal R
ange
s & A
rrest D
rug D
osage
s 2
01
3
Pa
edia
tric
s

28
N
orm
al P
eak
Flo
w C
ha
rt -
Pae
dia
tric
s 8
Pa
edia
tric
s

29
Pae
diatric P
ain A
ssessm
en
t Faces
Pa
edia
tric
s

30
Cri
teri
a 0
1
2
Face
N
o p
arti
cula
r ex
pre
ssio
n o
r sm
ile
Occ
asio
nal
gri
mac
e o
r fr
ow
n,
wit
hd
raw
n, u
nin
tere
sted
Fr
equ
ent
to c
on
stan
t q
uiv
erin
g ch
in, c
len
ched
jaw
Legs
N
orm
al p
osi
tio
n o
r re
laxe
d
Un
easy
, res
tles
s, t
ense
K
icki
ng,
or
legs
dra
wn
up
Acti
vity
Ly
ing
qu
ietl
y, n
orm
al
po
siti
on
, mo
ves
easi
ly
Squ
irm
ing,
sh
iftin
g b
ack
and
fo
rth
, ten
se
Arc
hed
, rig
id o
r je
rkin
g
Cry
N
o c
ry (
awak
e o
r as
leep
) M
oan
s o
r w
him
per
s;
occ
asio
nal
co
mp
lain
t C
ryin
g st
ead
ily, s
crea
ms
or
sob
s, f
req
uen
t co
mp
lain
ts
Co
nso
lab
ility
C
on
ten
t, r
elax
ed
Rea
ssu
red
by
occ
asio
nal
to
uch
ing,
hu
ggin
g o
r b
ein
g ta
lked
to
, dis
trac
tib
le
Diffi
cult
to
co
nso
le o
r co
mfo
rt
FL
AC
C S
cale
P
aed
iatr
ic N
on
-Ver
ba
l Pa
in A
sses
smen
t To
ol
Pa
edia
tric
s

31
Paediatric Analgesic Ladder (Under 12 Years)
Pain Score Medical Pain
Trauma, Orthopaedic,
Musculoskeletal & Soft tissue Pain
0 – 3 Mild Pain
Consider Entonox +/-
Ibuprofen &/or Paracetamol
Consider Entonox +/-
Ibuprofen &/or Paracetamol
4 – 6 Moderate
Pain
Consider Entonox +/-
Morphine
Consider Entonox +/-
Ibuprofen &/or Paracetamol
7 – 10 Severe
Pain
Consider Entonox +/-
Morphine
Consider Entonox +/-
Ibuprofen &/or Paracetamol
+/- Morphine
For Cardiac Related Chest Pain Morphine Should be Considered in the First Instance
Pa
edia
tric
s

32
Obstetrics Algorithms and Charts
APGAR Score for Newborns 33
Mechanics of Normal Birth 34
Shoulder Dystocia 35
Breech Birth Delivery 36

33
APGAR Score for Newborns Appearance
Pulse
Grimace
Activity
Respiration
1 Blue or Pale All Over
2 Blue at Extremities, Body Pink
3 No Cyanosis, Body and Extremities Pink
1 Absent
2 <100
3 ≥100
1 No Response to Stimulation
2 Grimace/Feeble Cry when Stimulated
3 Cry or Pull Away when Stimulated
1 None
2 Some Flexion
3 Flexed Arms and Legs that Resist Extension
1 Absent
2 Weak, Irregular, Gasping
3 Strong, Lusty Cry
Ob
stet
rics

34
Mechanics of Normal Birth 5 O
bst
etri
cs

35
Shoulder Dystocia 4
The McRoberts' manoeuvre is a procedure performed to release a baby's impacted shoulder during shoulder dystocia. The mother's legs are held back in a flexed position and pulled to her chest to further open the pelvis and allow the baby's shoulder to be released. At the same time suprapubic pressure is applied to the mother's lower abdomen over the pubic bone.
Ob
stet
rics

36
Breech Birth Delivery 5
1
4
2
5
3
6
Ob
stet
rics

37
Equipment Instructions and Guidance
Laerdal Suction Unit 38
ParaPAC Operation 39
Fitting a Collar 40
Fitting a Donway 41
Fitting a Donway Continued 42
Fitting a KED 43
Fitting a KED Continued 44

38
Laerdal Suction Unit 6
Procedure for Daily Test. 1 Ensure that tubing is unwound and un-occluded
2 Ensure the suction catheter adapter is removed from the holder (if applicable)
3 Ensure the canister lid, T-bar, angled connector and tubing are securely fastened.
4
To run the test, press and hold the test button while setting the operating switch to 500+mmHg. Do not release the test button until a minimum of 2 seconds after the operating switch has been set to 500mmHg. The test will start immediately.
5
As soon as LED 2 from the bottom of the battery status indicator comes on (takes approximately 1 second) fully occlude the patient suction tubing until all 4 LED’s have illuminated and LED 1 lights up again.
6 Keep the tubing blocked while LED 2, 3 and 4 lights up. 7 Release the tubing when LED 1 comes on again. 8 Evaluate the test results.
9 After evaluating the test results, turn the operating switch to “0” to exit the device test.
Equ
ipm
ent

39
ParaPA
C O
pe
ratio
n 1
1
Equ
ipm
ent

40
Fi
ttin
g a
Ce
rvic
al C
olla
r 9
Equ
ipm
ent

41
Fittin
g a Do
nw
ay 9
Equ
ipm
ent

42
Fi
ttin
g a
Do
nw
ay C
on
tin
ue
d 9
Equ
ipm
ent

43
Fittin
g a KED
9
Equ
ipm
ent

44
Fi
ttin
g a
KED
Co
nti
nu
ed
9
Equ
ipm
ent

45
Assessment & History Taking Aid memoirs, Acronyms and Diagnosis
Patient Assessment Triangle 46
Body Assessment - DCAPBTLS 47
Neurological Assessment - 5Ps 47
Chest Assessment - TWELVEFLAPS 48
Chest Assessment – ATOMFC 49
Chest Trauma 49
Chest Pain - History Taking 50
Abdominal Pain - History Taking 51
Abdominal Pain Locations 52

46
Patient Assessment Triangle
Airway &
Appearance
Circulation/Skin
Breathing
Effort
General Impression (First View of Patient)
Normal Abnormal
A
Normal cry or speech. Responds to parents or to environmental stimuli such as lights, keys, or toys. Good muscle tone. Moves extremities well.
Abnormal or absent cry or speech. Decreased response to parents or environmental stimuli. Floppy or rigid muscle tone or not moving.
B
Breathing appears regular without excessive respiratory muscle effort or audible respiratory sounds.
Increased/excessive (nasal flaring, retractions or abdominal muscle use) or decreased/absent respiratory effort or noisy breathing.
C Colour appears normal for racial group of child. No significant bleeding.
Cyanosis, mottling, paleness/pallor or obvious significant bleeding.
Initial Assessment (Primary Survey)
Normal Abnormal
A Clear and maintainable. Alert on AVPU scale.
Obstruction to airflow. Gurgling, stridor or noisy breathing. Verbal, Pain or Unresponsive on AVPU scale.
B Easy, quiet respirations. Respiratory rate within normal range. No central cyanosis.
Presence of retractions, nasal flaring, stridor, wheezes, grunting, gasping or gurgling. Respiratory rate outside normal range. Central cyanosis.
C
Colour normal. Capillary refill at palms, soles, forehead or central body ≤2 sec. Strong peripheral and central pulses with regular rhythm.
Cyanosis, mottling, or pallor. Absent or weak peripheral or central pulses; Pulse or systolic BP outside normal range; Capillary refill > 2 sec with other abnormal findings.
Ass
essm
ent

47
Body Assessment
Body Assessment
DCAPBTLS
D Deformity
C Contusions
A Abrasions
P Penetrations
B Burns
T Tenderness
L Lacerations
S Swelling
5Ps
P Pain
P Paralysis (Movement)
P Paraesthesia (Sensation)
P Pulses and Capillary Refill
P Pallor (Skin Colour and Temperature)
S Swelling
Ass
essm
ent
48
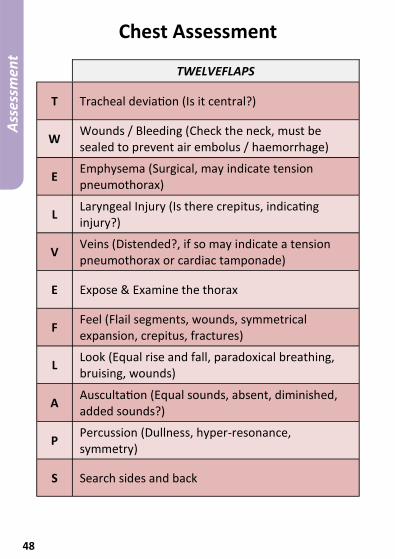
Chest Assessment
TWELVEFLAPS
T Tracheal deviation (Is it central?)
W Wounds / Bleeding (Check the neck, must be sealed to prevent air embolus / haemorrhage)
E Emphysema (Surgical, may indicate tension pneumothorax)
L Laryngeal Injury (Is there crepitus, indicating injury?)
V Veins (Distended?, if so may indicate a tension pneumothorax or cardiac tamponade)
E Expose & Examine the thorax
F Feel (Flail segments, wounds, symmetrical expansion, crepitus, fractures)
L Look (Equal rise and fall, paradoxical breathing, bruising, wounds)
A Auscultation (Equal sounds, absent, diminished, added sounds?)
P Percussion (Dullness, hyper-resonance, symmetry)
S Search sides and back
Ass
essm
ent

49
Chest Assessment
ATOMFC
A Airway obstruction (Tongue, trauma, foreign object, vomit etc)
T Tension Pneumothorax
O Open sucking wound (Open Pneumothroax)
M Massive Haemorrhage (Haemothroax)
F Flail Chest
C Cardiac Tamponade
Chest Trauma
Differential Diagnosis
Condition Chest
Expansion Trachea Percussion
Breath Sounds
Pneumothorax Decreased Unchanged Resonant Reduced
Tension Pneumothorax
Hyper expanded
Deviated away from tension
Hyper Resonant
Absent of affected side
Haemothorax Possibly reduced
Undeviated Dullness Reduced or absent
Collapse / consolidation
Reduced
May deviate towards collapse
May be dull Reduced or bronchial breathing
Pleural effusion Possibly reduced
Undeviated Dullness Reduced or absent
Ass
essm
ent

50
Chest Pain - History Taking
SOCRATES
S Site - Where is the pain or discomfort? Can you point to the area with one finger?
O Onset - What were you doing when the pain first started? What do you think may have caused this pain or discomfort?
C Character - Can you describe the type of pain? Is it: dull ache, sharp, stabbing, cramping, tearing, tightness, crushing, burning? Is it there all the time or does it in waves?
R Radiating - Does the pain stay in one place or does it radiate? Does it follow a certain pattern?
A
Associated Symptoms - Pale, clammy, dyspnoea, tachypnoea, SOB, dizzy, syncope, lethargy, confusion, vomiting, haemoptysis, productive cough, fever, haematemesis, pulse abnormalities, impending doom. Have you had a recent cough or been vomiting? When did you last eat? Have you had any difficulty swallowing?
T Time - How long have you had the pain? Has it been there ever since? Have you ever had a similar episode like this before?
E
Exacerbate / Relieve - Does anything ease the pain? (Analgesia, patient positioning, resting. Does anything make the pain worse? (Walking, leaning forward, lying down, coughing, movement, inhalation or expiration.
S Severity - If you were to score the pain out of 10, 1 being no pain and 10 being the worst imaginable, what would you score it?
Previous History - Recent trauma, chest infection or coughing, asthma, angina, COPD, heart failure, dyspepsia, dysphagia,
Risk Factors - Family history, smoker, overweight, heavy drinker, sedentary life style, hypertension, hypercholesterolemia, long travel / pregnancy, diabetes.
Ass
essm
ent

51
Abdominal Pain - History Taking
SOCRATES
S Site - Where is the pain or discomfort? Can you point to the area with one finger?
O Onset - What were you doing when the pain first started? What do you think may have caused this pain or discomfort?
C Character - Can you describe the type of pain? Is it: dull ache, sharp, stabbing, cramping, tearing, tightness, crushing, burning? Is it there all the time or does it in waves?
R Radiating - Does the pain stay in one place or does it radiate? Does it follow a certain pattern?
A
Associated Symptoms - Pale, clammy, dyspnoea, tachypnoea, SOB, dizzy, syncope, lethargy, confusion, nausea, vomiting, diarrhoea? Have you noticed anything abnormal when passing water? For example: Increased or reduced frequency, dark or off colour urine. Does it have a strong odour, burning sensation? Have you noticed anything abnormal when passing a bowel motion? Increased or reduced frequency, pain, loose or hard stools, dark coloured or bright red.
T Time - How long have you had the pain? Has it been there ever since? Have you ever had a similar episode like this before?
E
Exacerbate / Relieve - Does anything ease the pain? (Analgesia, patient positioning, resting, applying pressure, passing wind or bowel motion?) Does anything make the pain worse? (Lying down, coughing, movement, inhalation, expiration, palpation, passing water or bowel motion?)
S Severity - If you were to score the pain out of 10, 1 being no pain and 10 being the worst imaginable, what would you score it?
Birth Bearing Age - Any chance you could be pregnant? Are there any changes to your menstruation cycle: early, late, abnormal colour, odours, increased pain? Have you had any vaginal discharge?
Previous History - Recent trauma, chest infection or coughing, asthma, angina, COPD, heart failure, dyspepsia, dysphagia,
Risk Factors - Family history, overweight, heavy drinker, sedentary life style, hypertension, hypercholesterolemia, long travel / pregnancy, diabetes.
Ass
essm
ent

52
Abdominal Pain Locations 1
Ass
essm
ent
53
Trauma & Medical Emergencies Useful Information and Charts
Rule of Nines 54
Submersion/Immersion Drowning 55
Key Points - Submersion/Immersion 55
Shock Comparison 56
Stages of Shock 57
Catastrophic Haemorrhage Tourniquet 58
Removing a Helmet 59
Fitting a Triangular Bandage 60
Routes of Drug Administration 61

54
Rule of Nines Paediatric & Adult
Tra
um
a &
Med
ica
l

55
Submersion/Immersion Drowning
The pulse may be extremely slow if hypothermia is present, and external cardiac compression may be required. Bradycardia often responds to improved ventilation and oxygenation. Drugs such as adrenaline and atropine are less effective in HYPOTHERMIA, and must not be repeatedly used. These drugs may pool in the static circulation of the drowned casualty, and then, after re-warming and circulation has been restored, act as a dangerous bolus of drug as they are circulated. In hypothermic cardiac arrest, defibrillation will be unsuccessful where the core temperature remains low. At 28C the ventricle may spontaneously fibrillate. Defibrillation may not succeed until the core temperature rises above 30-32C.
Tra
um
a &
Med
ica
l
Key Points – Submersion/Immersion
Ensure own personal safety
Successful resuscitations have occurred after prolonged submersion/immersion.
Near drowning is often associated with hypothermia.
Special considerations in cardiac arrest treatment in the presence of hypothermia.
Severe complications may develop several hours after submersion/immersion.

56
Tra
um
a &
Med
ica
l
Typ
e
RR
H
R
BP
C
ap R
efill
Sk
in
Hyp
ovo
laem
ia
>2
Se
con
ds
Pal
e
Cla
mm
y Sw
eaty
Car
dio
gen
ic
>2
Se
con
ds
Pal
e
Cla
mm
y Sw
eaty
Sep
tic
<2
Se
con
ds
Flu
shed
H
ot
Swea
ty
An
aph
ylac
tic
<2
Se
con
ds
Flu
shed
H
ot
Swea
ty
Ne
uro
gen
ic
----
<2
Se
con
ds
Flu
shed
H
ot
Swea
ty
Sh
ock
Co
mp
aris
on

57
Tra
um
a &
Med
ica
l
Stage
s of Sh
ock
Stage
Blo
od
Loss
ml
Signs an
d Sym
pto
ms
1
<15
%
75
0
No
rmal B
loo
d P
ressure &
Resp
Rate,
Slight P
allor &
An
xiety
2
15
- 30
%
75
0 - 1
50
0
Tachycard
ia, Increased
Resp
Rate &
D
iastolic P
ressure, N
arrow
Pu
lse P
ressure, Sw
eatin
g, Mild
ly An
xiou
s/R
estless
3
30
- 40
%
15
00
- 2
00
0
Marked
Tachycard
ia >12
0 b
pm
&
Tachyp
no
ea >30
bp
m, D
ecreased
Systo
lic Pre
ssure, A
ltered M
en
tal Statu
s, Sweati
ng, C
oo
l & P
ale Skin
4
>40
%
>20
00
Extreme Tach
ycardia &
Tachyp
no
ea, W
eak Pu
lse, Decreased
LOC
& Systo
lic B
P <7
0, Skin
is Sweaty, C
oo
l and
Pallo
r
58
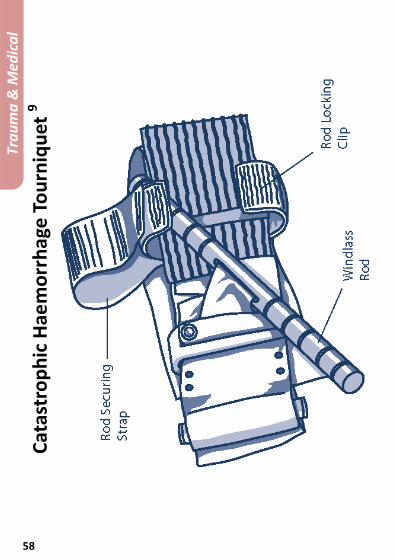
C
atas
tro
ph
ic H
aem
orr
hag
e T
ou
rniq
uet
9
Tra
um
a &
Med
ica
l

59
Re
mo
ving a H
elm
et 9
Tra
um
a &
Med
ica
l

60
Fi
ttin
g a
Tria
ngu
lar
Ban
dag
e 9
Tra
um
a &
Med
ica
l

61
Routes of Drug Administration
Code Route Description
BUC Buccal Administration directed toward the cheek, from within the mouth.
ET Endotracheal Administration down the ET tube.
IM Intramuscular Administration within a muscle.
INH Inhaled Administration by breathing.
IO Intraosseous Administration within the bone marrow.
IV Intravenus Administration within or into a vein or veins.
NASAL Nasal Administration to the nose; administered by way of the nose.
NEB Nebulised Administration in the form of mist.
PO Oral Administration to or by way of the mouth.
PR Rectal Administration to the rectum.
SC Subcutaneous Administration beneath the skin; hypodermic.
SL Sublingual Administration beneath the tongue.
TOPIC topical Administration to a particular spot on the outer surface of the body.
Tra
um
a &
Med
ica
l

62
Anatomy Diagrams and Terminology
Palpable Pulse Locations 63
Bones - General 64
Bones – Spinal Colum 65
Anatomical Terms of Location 66
Patient Positioning 67

63
Palpable Pulse Locations
An
ato
my

64
Bones - General A
na
tom
y

65
Bones – Spinal Colum
An
ato
my

66
Anatomical Terms of Location
Term Definition
Anterior Posterior
From front (Anterior) to back (Posterior).
Dorsal Ventral
From top (Dorsal) to bottom opposite end of body (Ventral).
Lateral (Left) Lateral (Right)
From left to right side of the body.
Medial (Left/Right)
From centre of organism to one or other side
Proximal Distal
from tip of an appendage (distal) to where it joins the body (proximal)
An
ato
my

67
Patient Positioning 7
An
ato
my

68
ECG & ETCO2 Interpretation Examples and Explanations
ECG Lead Placement 69
Normal ECG 70
ECG Assessment Guide 71
ECG Arrhythmias 1 72
ECG Arrhythmias 2 73
ECG Arrhythmias 3 74
ECG Arrhythmias 4 75
Interpretation of ETCO2 Waveform 76

69
ECG Lead Placements 9
ECG
& E
TCO
2

70
Normal ECG 3
I Lateral aVR V1 Septal V4 Anterior
II Inferior aVL Lateral V2 Septal V5 Lateral
III Inferior aVF Inferior V3 Anterior V6 Lateral
Interval Time in Seconds
PR Interval 0.12 to 0.22
QRS Complex 0.08 to 0.12
QT Interval 0.35 to 0.42
ECG
& E
TCO
2

71
ECG Assessment Guide 3 Point Description
What is the rhythm? Regular, Irregular
What is the Rate? Fast, Normal, Slow
Are there P Waves Present?
YES - Atrial Foci NO - Junctional or Ventricle Foci
Are all the P Waves the Same?
YES - Then Same Foci No - Then Different Foci
Is there a P Wave before each QRS?
YES - Atrial Foci NO - Junctional or Ventricle Foci
Is there a QRS after every P Wave?
NO - Ventricular Standstill or Possible Heart Block
Is the P-R Interval Normal?
YES - 0.12 to 0.20 Seconds (3-5 small squares) NO - If >0.0 seconds its First Degree Heart Block
Is the QRS Normal? YES - 0.04 to 0.12 secconds (1-3 small squares) NO – Bundle Branch Block
Is the ST Segment Isoelectric?
If Elevated its Myocardial Infarction If Depressed its Ischemia or Angina
Is the T Wave Normal?
YES – 3 Times the Height of the P Wave NO – Inverted?
ECG
& E
TCO
2

72
ECG Arrhythmias 1 3
Normal Sinus
1st Degree Heart Block
Missing QRS Complex
2nd Degree Heart Block
Type 1
Multiple Missing QRS Complexes
2nd Degree Heart Block
Type 2
3rd Degree Heart Block
ECG
& E
TCO
2

73
ECG Arrhythmias 2 3
ECG
& E
TCO
2
Atrial Fibrillation
Atrial Flutter
Asystole
Bundle Branch (Determine
Left/Right from 12 Lead)
Sinus Bradycardia

74
ECG Arrhythmias 3 3 EC
G &
ETC
O2
Idioventricular Rhythm
Junctional Rhythm
Multifocal Premature Ventricular Contraction
Compensatory Pause
Premature Atrial
Contraction
Paced Rhythm

75
ECG Arrhythmias 4 3
Compensatory Pause
Premature Junctional
Contraction
Super Ventricular Tachycardia
Unifocal Premature Ventricular Contraction
Ventricular Fibrillation
Ventricular Tachycardia
ECG
& E
TCO
2

76
Interpretation of ETCO2 Waveform
Sudden loss of waveform, ETCO₂ near zero. ET Tube,
disconnected, dislodged, kinked or obstructed.
Loss of circulatory function.
Decreasing ETCO₂ with loss of plateau. ET tube cuff leak or deflated cuff ET tube in
hypopharynx Partial obstruction
CPR Assessment. Attempt to maintain
minimum of 10mmHg
Sudden Increase in ETCO2. Return of
spontaneous circulation
ECG
& E
TCO
2
77
Major Incidents Acronyms and Plan of Action
Approach - Think STEP 123 78
Approach - Scene Assessment - CSCATTT 78
Dynamic Operational Risk Assessment 79
Plan of Action - SitRep - METHANE 80
Plan of Action - Briefing Structure - IIMARC 80
Primary Triage 81
Triage Categories 82
Pre-Alert - ASHICE 83
Handover - Trauma MIST 84
Handover –Medical MIST 84
EH20 Escape Hood 85
NAAK Presentation 86
NAAK Indications 87
NAAK Directions for Use 88
Electronic Personal Dosimeter (EPD) 89
EPD Alarm Descriptions 90
78
Approach
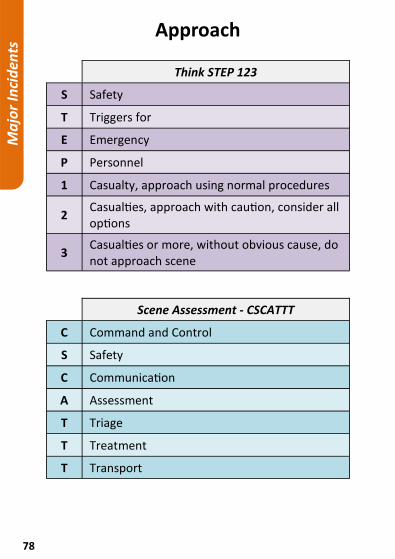
Think STEP 123
S Safety
T Triggers for
E Emergency
P Personnel
1 Casualty, approach using normal procedures
2 Casualties, approach with caution, consider all options
3 Casualties or more, without obvious cause, do not approach scene
Scene Assessment - CSCATTT
C Command and Control
S Safety
C Communication
A Assessment
T Triage
T Treatment
T Transport
Ma
jor
Inci
den
ts
79
Dynamic Operational Risk Assessment
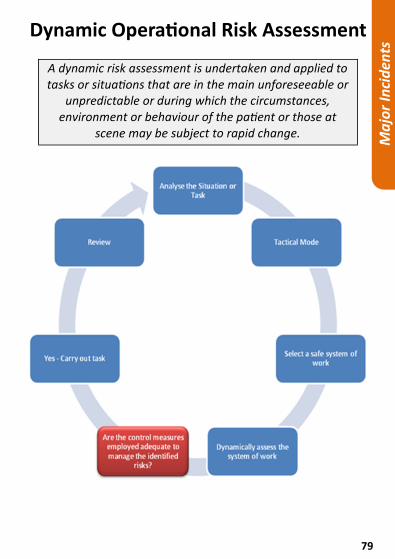
A dynamic risk assessment is undertaken and applied to tasks or situations that are in the main unforeseeable or
unpredictable or during which the circumstances, environment or behaviour of the patient or those at
scene may be subject to rapid change.
Ma
jor
Inci
den
ts

80
Plan of Action
Situation Report to Control - METHANE
M Major Incident – Standby or Declared
E Extraction Location
T Type of Incident
H Hazards (Present and Potential)
A Access (Egress)
N Number of Casualties
E Emergency Services (On Scene or Required)
Briefing Structure - IIMARC
I Information – Overview of incident, location, what is involved and when it happened
I Intention – What are we going to do
M Method – How are we going to achieve it
A Administration – What records are required
R Risks – DORA, hazards, Minimising them and contingency plans
C Talk groups, mobile phones, de-brief arrangements
Ma
jor
Inci
den
ts
81
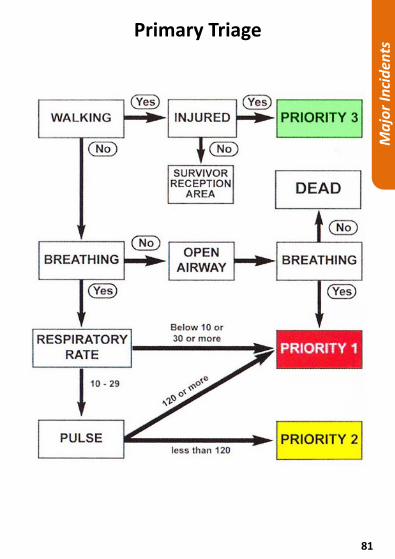
Primary Triage
Ma
jor
Inci
den
ts
82
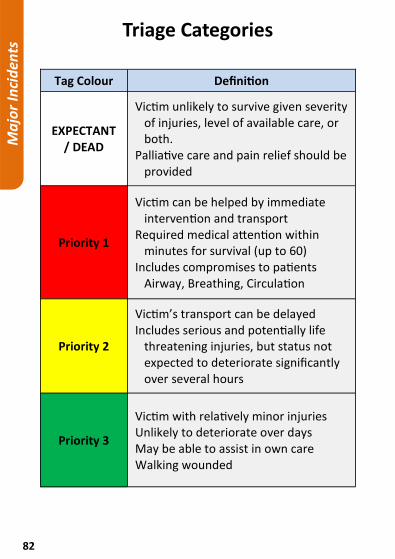
Triage Categories
Tag Colour Definition
EXPECTANT / DEAD
Victim unlikely to survive given severity of injuries, level of available care, or both.
Palliative care and pain relief should be provided
Priority 1
Victim can be helped by immediate intervention and transport
Required medical attention within minutes for survival (up to 60)
Includes compromises to patients Airway, Breathing, Circulation
Priority 2
Victim’s transport can be delayed Includes serious and potentially life
threatening injuries, but status not expected to deteriorate significantly over several hours
Priority 3
Victim with relatively minor injuries Unlikely to deteriorate over days May be able to assist in own care Walking wounded
Ma
jor
Inci
den
ts

83
Pre-Alert
ASHICE
A Age
S Sex
H History
I Illness / Injuries / Intervention
C Condition – HR, RR, SpO2 Air / O2, BP, BM, Temp, GCS, ECG.
E Estimated Time of Arrival
RED
Cardiac Arrest. Peri-Arrest. Any patient eliciting MTC outcome using Major Trauma Pathfinder. Currently fitting. GCS 12 or less. PPCI.
AMBER
Cardiac chest pain New Stroke (regardless of symptom time). Any other clinical concern.
Ma
jor
Inci
den
ts

84
Handover
Trauma - MIST
M Mechanism of Injury
I Injuries
S Signs (Vitals)
T Treatment
Medical - MIST
M Medical History (PMH/Allergies)
I Illnesses (PC/HPC)
S Signs (Vitals)
T Treatment
Ma
jor
Inci
den
ts

85
EH20 Escape Hood 2
For use when the crew believe that they have been potentially exposed to a form of hazardous contamination. One size fits all. It will provide 20 minutes of respiratory protection to escape the scene.
Ma
jor
Inci
den
ts

86
NAAK Presentation
Services carry a supply of 10 packs of Nerve Agent Antidote Kits on every Emergency ambulance for self-administration by the crew in the event of accidental exposure to nerve agents.
They consist of 2 prefilled automatic intramuscular injection devices linked by a plastic clip and housed in a foam pouch. Atropen containing 2.0mg of Atropine and a Combopen containing 600mg Pralidoxime Chloride.
Ma
jor
Inci
den
ts

87
NAAK Indications
The Nerve Agent Antidote Kit (NAAK) should be self-administered or assisted by their crew mate if they are incapacitated on occasions where they suspect that they have been accidentally exposed to nerve agents such as Organo Phosphates (deliberate or accidental release), and are suffering the effects listed below.
Clinical Diagnosis:
History of exposure Miosis Respiratory distress Bronchorrhoea Depressed level of consciousness Bronchospasm Muscle Twitching Convulsion
Including one or more of the following:
Bronchorrhoea Bronchospasm Severe Bradycardia (<40 bpm)
User may experience the following side effects:
Impairment of psychomotor function Disorientation Loss visual accommodation Photophobia Transient bradycardia then tachycardia
Palpitations Arrhythmias CNS depression Circulatory/respiratory failure
Ma
jor
Inci
den
ts

88
NAAK Directions for Use
1
Remove Pen No 1 marked ATROPINE from the plastic holder this removes the safety cap and extreme care must be taken.
2
Place the GREEN cap of the auto injector against the upper quadrant of the thigh making sure that that it is clear of anything in the trouser pocket. Press hard until the injector functions, count to ten slowly and then withdraw. Bend the needle on any hard surface until it breaks off. Record time of administration.
3
Remove Pen No 2 marked PRALIDOXIME from the plastic holder this removes the safety cap and extreme care must be taken.
4
Place the BLACK cap of the auto injector against the upper quadrant of the thigh making sure that that it is clear of anything in the trouser pocket. Press hard until the injector functions, count to ten slowly and then withdraw. Bend the needle on a hard surface until it snaps off. Record time of administration. Hold both injectors in your hand until help arrives.
Ma
jor
Inci
den
ts

89
Electronic Personal Dosimeter (EPD)
An Electronic Personal Dosimeter (EPD) is a small pager sized device that will monitor for the presence of ionising radiation. It is designed to allow for normal every day background levels of radiation, but should it detect a rise in levels of radiation in the vicinity of the wearer it will activate an internal audible alarm to alert the wearer to look at the display and take action according to the reading and the perceived local circumstances.
Default Screen
This example shows the Dose Rate on the display screen in micro-Sieverts/hour (µSv/h).
Test Display Screen
At the beginning of every shift the wearer should perform a confidence test. From the default display screen press and hold the operating button until “TEST” is displayed.
Confidence Test Display
Double press the operating button to initiate the confidence test, which confirms operation of visual display and the visual and audible alarms. The display screen will show all icons at once, the audible alarm will sound and the visual indicator will flash.
Ma
jor
Inci
den
ts

90
EPD Alarm Descriptions Alert Description Low Battery Warning
There is a low battery warning, which is an intermittent slow tone. This indicated there is about ten hours battery life left. This will be the most common warning heard (the data in the EPD will be stored for about a month without a battery).
Alarm 1 Primary Alert Signal
The first tone or Primary Alert Signal is an intermittent double “fast” chirp and the LED will illuminate RED and indicates the presence of a level of radiation just above background. This tone will also sound whenever the battery is replaced and is a function of the auto test process. It also acts as a reminder of the alerts for the wearer. The user should be aware of this facility and is NOT to change batteries at incident sites. The Primary Alert Signal should be the only activation alarm the wearer will ever hear whilst performing their duties, the most common will be the low battery warning.
Alarm 2 Secondary Alert Signal
The second tone, the Secondary Alert Signal is a slow two-tone alarm and indicated a level of radiation approximately equivalent to that received annually by normal means. Under normal circumstances where this level of radiation is present, Ambulance staff will not be deployed forward to assist casualties.
Alarm 3 Tertiary Alert Signal
The third alert tone, the Tertiary Alert Signal is a continuous single high tone. This tone indicated that the wearer has been exposed to a potentially significant or high dose.
Ma
jor
Inci
den
ts

91
Infection Prevention & Control Useful Information
Mops and Buckets 92
Hand Washing Technique 93
Hand Hygiene 94
Protective Clothing 94
Sharp/Splash Injury Procedure 95

92
Mops and Buckets
Mops and their corresponding colour coded buckets must not be interchanged. If any mop becomes contaminated with blood or body fluids, then the head should be discarded as clinical waste and a replacement fitted immediately. All mop heads should be routinely replaced every month.
Infe
ctio
n C
on
tro
l

93
Hand Washing Technique 12
Good and efficient hand hygiene is the single most important factor in the prevention and control of the spread of infection.
Second to hand washing, consistent use of barrier methods, especially wearing gloves, is the most important step in preventing cross-contamination of staff and patients.
Infe
ctio
n C
on
tro
l

94
Hand Hygiene 12 Use the hand washing technique:
Protective Clothing Circumstance/Activity Appropriate PPE
Circumstance/Activity Appropriate PPE
Circumstance/Activity Appropriate PPE
Exposure to blood/body fluids anticipated, but low
risk of splashing.
Wear gloves, plastic apron and sleeve protectors.
Wear gloves, plastic apron and sleeve protectors.
Wear gloves, plastic apron and sleeve protectors.
Infe
ctio
n C
on
tro
l

95
Sharp/Splash Injury Procedure Inoculation/blood splash injuries include any sharp
object that pierces the skin, bites or any other exposure to blood or body fluids.
Bleed it – Apply pressure, but “DO NOT” suck the wound.
Wash it – Wash with soap under warm running water for 2 minutes.
Dry it – Do not scrub the injury or pat it dry.
Dress it – Cover the injury with a dressing.
For splashes to the eyes – Irrigate with saline or water.
For splashes to the mouth – Rinse with copious amounts of water and wash your face. Donor – Identify and document the source of the inoculation injury include: Name, DOB and home address if possible.
Inform – Contact EOC and inform them of the situation.
Attend – Go to the nearest Emergency Department without delay.
Report it – Report the incident to occupational health as soon as possible. Telephone your local Occupational health service. Write Numbers Below:
Infe
ctio
n C
on
tro
l

96
Key Contacts Phone Numbers and Addresses

97
Notes

98
Notes

99
1. Ansari, P (2012) Acute Abdominal Pain [Online] URL: http://www.merckmanuals.com/professional/gastrointestinal_disorders/acute_abdomen_and_surgical_gastroenterology/acute_abdominal_pain.html
2. Avon Protection Systems (2011) EH20 Data Sheet, Melksham/England: Avon Protection Systems.
3. Evans, S (2004) A Guide Through the Maze of ECGs, 3rd Edition, Somerset/England: Association of Professional Ambulance Personnel.
4. Fikac, L (2000) Shoulder Dystocia [Online] URL: http://www.capefearvalley.com/outreach/outreach/peapods/obemergencies/shoulderdystocia.htm
5. Kochenour, N (1997) The Mechanism of Normal Labor [Online] URL: http://library.med.utah.edu/kw/human_reprod/lectures/physiology_labor/#2
6. Laerdal (2013) Laerdal Suction Unit: Instruction Manual, Kent/England: Laerdal Medical Limited
7. Medtrng (2012) Postures and Direction of Movement [Online] URL: http://www.medtrng.com/posturesdirection.htm
8. Peak Flow (2004) Mini-Wright Peak Flow Meter: Predictive Normal Values (Nomogram, EU scale), Essex/England: Clement Clarke International.
9. Queensland Ambulance Service (2011) Clinical Practice Manual [Online] URL: http://www.ambulance.qld.gov.au/medical/CPM.asp
10. Resuscitation Council UK (2010) Resuscitation Guidelines 2010, London/England: RCUK.
11. Smiths Medical (2008) Emergency Transport and Ventilation [Online] URL: http://www.smiths-medical.com/Upload/products/product_relateddocs/EmergencyTransport.pdf
12. World Health Organisation (2009) Clean Care is Safer Care: Clean Your Hands, Geneva/Switzerland: WHO.
References and Credits

100
Handover
A collaboration of useful guidelines in a quick reference pocket book tailored for pre-
hospital care.
This handy pocket book resulted from my quest to consolidate the most relevant and useful
guidance into a single source; something that can be carried in your pocket at all times -
whenever you may need it.
Download the FREE electronic edition from: PocketParamedic.org
Thank you to everyone that has allowed their content to be included in Pocket Paramedic.
For more information visit PocketParamedic.org
Pocket Paramedic is a non profit venture. When Available, the A6 hard copies are sold at cost. For Information Purposes Only. Pocket Paramedic.org, and Jason Houghton, take absolutely zero responsibility for how you, as an individual, choose to make use of Pocket Paramedic.. The contents of this pocket book can in no way be guaranteed to be accurate and/or up to date. No credit is taken for the intellectual property of others highlighted in the references.
Where applicable, consent has been granted to reproduce all copyrighted material. Information provided in Pocket Paramedic may differ from other guidelines, protocols and
procedures; you must never use Pocket Paramedic as a substitute for them.
Version 1.1