Embed Size (px)
Citation preview

In-Hospital Cardiac ArrestIn-Hospital Cardiac ArrestEEvidencevidence B Basedased M Medicineedicine
Stefano Nardi MD,PhD
AZIENDA OSPEDALIERA SANTA MARIA TERNIAZIENDA OSPEDALIERA SANTA MARIA TERNI DIVISION OF CARDIOLOGY DIVISION OF CARDIOLOGY
ARRHYTHMIA, ELECTROPHYSIOLOGIC CENTER ARRHYTHMIA, ELECTROPHYSIOLOGIC CENTER AND CARDIAC PACING UNIT AND CARDIAC PACING UNIT

Definition• Natural Death
(due to CARDIAC CAUSES)
Sudden (Cardiac) Death Sudden (Cardiac) Death
• Preceeding by a sudden loose of coscience until 1 h of start of the ACUTE SYMPTOMS, in a pts W or w/oa note pre-existent CARDIAC DISEASE, in which the die was not considered imminent.
• AGE and modality of DEATH are not prevedible
Myerburg RJ, Castellanos A ’80 Myerburg RJ, Castellanos A ’80 Task-force on Task-force on
SD of ESC. EHJ ’01 SD of ESC. EHJ ’01

Suddenly Suddenly FILIPPIDE FILIPPIDE die immediately after his die immediately after his announcement at Atheniesis the victory ofannouncement at Atheniesis the victory of MARATONAMARATONA
ANCIENT PROBLEM ......

Vittorio GassmanMassimo TroisiBeniamino AndreattaUmberto BossiSergio LeoneClark GableDwight Eisenhower
..... CURRENT PROBLEM !!!!

The only difference between CA and Syncope is that the last one “wake up”

Total DeathTotal Death →→ 557.584 (100%) 557.584 (100%)
Death for CV diseaseDeath for CV disease →→ 242.248 (43%) 242.248 (43%)
Sudden DeathSudden Death →→ 57.000 (10.2%)57.000 (10.2%)
ISTAT source ‘00ISTAT source ‘00
0
50000
100000
150000
200000
250000 Cancro dellaMammellaCancro ColonRettoCancroBronchi/PolmoniIctus
Morte Improvvisa
MalattieCardiovascolari
Mor
ti p
er a
nno
In hospital cardiac arrestMortality Distribution

• Until 20% survival
• Between 30 - 80% of survivals suffer of Anoxic Encephalopaty
Cardiac Arrest Cardiac Arrest Magnitude (annual mortality)• U. S. U. S. →→ 450.000 450.000
• Europe Europe →→ 600.000 600.000
• Germany Germany →→ 80.000 80.000
• ItalyItaly →→ 65.00065.000
Incidence in Italy Incidence in Italy 1 1
case each 9 minutes case each 9 minutes
In hospital cardiac arrest

• 2 peak age-related in which SCD is more prevalent • Between born and 6 mo (sudden infant death syndrome)
• Between 45 and 75 years old
Sudden Cardiac Death Sudden Cardiac Death Relationship with Age
• 1 case each 1 case each 10 10 hours hours (UMBRIA)(UMBRIA)
• 912/850.000 each years912/850.000 each years
• 10 %10 % of all total mortality of all total mortality
• 40 %40 % of all deaths for CARDIAC DISEASE of all deaths for CARDIAC DISEASE

Primary Based on Studies and Clinical Research in a large cohort of pts
Based on Statistical Analisys but strickly linked with Personal Experiences and
common good practise
What is Evidence Based Medicine (EBM)?
Magnitude of Sudden Cardiac Arrest

CLINICAL GOVERNANCE
• National Operative Organized System by which is possible to CTR the Standard references of
QUALITY and the Continuous Educational System
• Merge between Clinical Practice and Health Management
• Efficacy and Effectivness of Local Source
Big Brother

CLINICAL GOVERNANCE
PerformancePerformance Disease Disease Management Management
Evento Evento Sentinella Sentinella
AUDIT AUDIT EBM EBM
Clinical Governance is a cyclical process
GUIDELINES GUIDELINES

• Incidence variable 0.36-1.28/1000 Incidence variable 0.36-1.28/1000 pts in general population pts in general population
• In industrialized pts, the total annual In industrialized pts, the total annual incidence is 1/ 1000 inhabitants incidence is 1/ 1000 inhabitants
• In ITALYIn ITALY: studio FACS (Friuli) : studio FACS (Friuli) incidence of 0.95 cases each incidence of 0.95 cases each 1000/people for yr; LIFE PROJECT 1000/people for yr; LIFE PROJECT of Piacenza (Emilia) 1.10 CA each of Piacenza (Emilia) 1.10 CA each 1000 inhabitants for yr 1000 inhabitants for yr
Sudden Cardiac Death Sudden Cardiac Death Epidemiology
• Until 8/1000 inhabitants between 60 and 69 yrs
EBM

Schein RMH. Chest ’90; Franklin C. Crit Care Med ‘94Smith AF. Resuscitation 1998; Hodgetts TJ. Resuscitation ’02
In-Hospital Cardiac Arrest (CA)In-Hospital Cardiac Arrest (CA)
• 50-80% have “warning” signs
• 66% potentially avoidable
• C.A. Inside Hospital C.A. Inside Hospital 60%60%• C.A. Outside Hospital C.A. Outside Hospital 40%40%

It’s possible to stratifie the patients ?
Mostly subjects that TRY OUT a CARDIAC ARREST
does not Survive to can NARRATE itself
Sudden Cardiac Death Sudden Cardiac Death
Which is the Classes at Risk ?

• Identification of appropriate pt categories
MethodsEvidence Based Medicine (EBM)
In-Hospital Cardiac Arrest In-Hospital Cardiac Arrest
• Identification of solid endpoints
• Definite working hypothesis

Risk Stratification • WIDE Spectrum of
underlying substrate
• Several combination between type of Arrhythmia and SUBSTRATE configure different Clinical Presentation with different profile of RISK
SUBSTRATESUBSTRATE• CAD• Valvular HD• Congenital HD• I-DCM
- reduction of LVEF - NSVT - Syncope
• H(O)CM• ARVD• Brugada syndrome• QTLS• Idiopatic VF • Idiopatic VT

< 30 yrs % > 30 yrs %- Ao stenosis 3-18- Eisenmenger 15- Congenital CM 10- H (O) CM 1-50- ARVD 0-26- Mitral Prolapse 1-24- CAD 3-20
- CAD 85- CM 10- Valvular disease 3- Electrical alternation 2
SUBSTRATES Sudden Cardiac Death Sudden Cardiac Death
Santomauro M, Cardiac Arrhythmias ’05 Santomauro M, Cardiac Arrhythmias ’05

Evidence Based is ruled by Ejecton Fraction (LVEF)(PREVALENT restriction)
Methodologic Introduction
In hospital cardiac arrest

Total Mortality
Ejection Fraction
Considerations
The impact factor of a specific strategy is prevalently based on the reduction the probability of
event “END POINT”
Sudden Cardiac Death Sudden Cardiac Death

PATHOGENESIS Bradiarrhythmias Bradiarrhythmias 15-20%15-20%
VT/VF VT/VF 75-80% 75-80%
EMD EMD 5%5%
Cardiac Rhythm recorded Cardiac Rhythm recorded in pts resuscitate to CA in pts resuscitate to CA
Cummins RO, Annals Emerg Med. ‘89Albert CM. Circulation ‘03
Bayés de Luna A. Am Heart J. ‘89
Which rhythm during CA ?Which rhythm during CA ?

“ Which is the treatments of choice
to Reduce SCD ? “
Zipes DP. Circulation ‘98Pitt B. NEJM ‘03

In both aviation and medicine,
people depend on
technology as the solution…

ALARM DEFIBRILLATION
BLS ACLS
The Chain of Survival

Sequence and TerminologySequence and Terminology
ASSESSMENTASSESSMENTACTIVATE EMSACTIVATE EMSPOSITIONPOSITION1’ AIRWAY1’ AIRWAY1’ BREATHING1’ BREATHING1’ CIRCULATION1’ CIRCULATIONDEFIBRILLATIONDEFIBRILLATION2’ AIRWAY2’ AIRWAY2’ BREATHING2’ BREATHING2’ CIRCULATION2’ CIRCULATIONDDifferential ifferential Diagnosis Diagnosis
BLS
ACLS
1’ SURVEY
2’ SURVEY2’ SURVEY

It’s easy to get good players.
Getting ’em to play together …That’s the hard part.

The ‘Swiss cheese’ model of organizational accidents
Some holes dueTo active failures
Other holes due tolatent conditions
Successive layers of defences
Hazards
Losses
It takes an average of 4.5 errors in the system for a medical accident to result Modified from James
Reason, 1991.

When to call for help?

• Few seconds after CAFew seconds after CA, , the subject loose consciousness the subject loose consciousness and stop to breath.and stop to breath.
• 4-6 minutes after CA4-6 minutes after CA, it’s , it’s clearly evident a significative clearly evident a significative Brain Damage Brain Damage
• More fastly is recovery More fastly is recovery cerebral circulation cerebral circulation more more probability a complete recovery probability a complete recovery of Cerebral Function of Cerebral Function
• 90 % of CA90 % of CA are completely are completely worked out if defibrillation is worked out if defibrillation is applied until 2 minutes applied until 2 minutes
SURVIVAL is Time-dependent SURVIVAL is Time-dependent

20:56:23 II
20:56:35 II
20:56:47 II Medtronic Physio-Control
Print 2

OBJECTIVES
• Identified CA. • Calling Help. • Start CPR (e.g. Mayo)• If appropriate start
with Defibrillation whithin 3’ from loose of consciousness
In hospital cardiac arrest

20:56:47 II
Print 2
20:56:59 II
Charge Complete
20:57:10 II Medtronic Physio-Control
Shock 1, 360 J
II
Postshock Charge Complete

Device able to recognize automatically a VT/VF and delivery a DC shock
1) Automatic Diagnoses
2) Easy and ready to use
In hospital cardiac arrest
AED’s

Time from CA to first
defibrillation (n=2748)
ssuurrvviivvaall
From: Swedish Cardiac Arrest Registry
In-Hospital Cardiac Arrest In-Hospital Cardiac Arrest
• Survival decrease each m of 10%
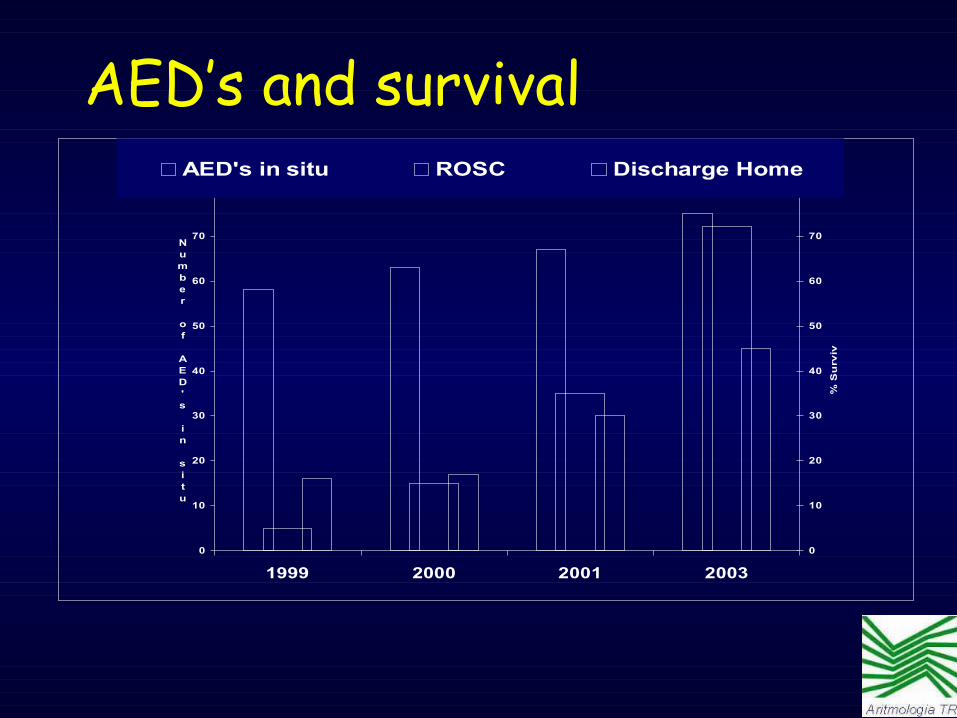
AED’s and survival
0
10
20
30
40
50
60
70
80
1999 2000 2001 2003
Number of AED's in situ
0
10
20
30
40
50
60
70
80
% S
urv
iva
l
AED's in situ ROSC Discharge Home

Audit compliance 2000 - 2004
0
20
40
60
80
100
2000 2001 2002 2003 2004
Year
%
• Systematic analysis of ‘Assistential Quality System’• Comparison between ‘Guided lines’ and ‘Real Word’ proposed new Standard Organizative Models • Implementation of ‘Guided Lines’• Verification of ‘outcomes’ over the time

BRESUS Gwinnutt Peberdy
Year 1992 2000 2003
Number of
arrests
2835 1368 14720
% Survival to discharge
15 17.6 17
SURVIVAL (EBM)
In-Hospital Cardiac Arrest In-Hospital Cardiac Arrest

END POINT mortality is correct ?END POINT mortality is correct ?Cardiac Arrest
Complete recovery
Intervention
Brain Damage, kidney failureBrain Damage, kidney failure
DEATH
Basic
Life
Support
TIME
In-Hospital Cardiac Arrest In-Hospital Cardiac Arrest

* A Brain Damage “Start” 4-6’ after a loss of hemodinamic support (cardiovascular arrest )
* Become “irreversible” after 10’
SURVIVAL is Time-dependent SURVIVAL is Time-dependent
Evidence-Based Medicine
Gathering Medical Information
Evaluating quality of Medical Information
Making Medical decisions using Best Evidence
In-Hospital Cardiac Arrest In-Hospital Cardiac Arrest Evidence Based Medicine (EBM)

Hospital staff should provide a resuscitation service that
exceeds what is available in their local airport, railway station etc
System of Training
In-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest Evidence Based Medicine (EBM)

The Clinical Staff

SERVICE
Educational Organizational
aspects
In-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest RESCUE Services • ~ 575 beds
• ~ 350 MD• ~ 800 staff Nurses• Complex ‘case mix’
of patients
CP Resuscitation does it only work on TV?
• What’s the problem in real life?
• Role of national standards
In-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest

System of TrainingIn-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest
• Who should we teach?
• What do we teach?
• How do we teach it?
• What resources do we use?
• How meaningful is the session?
• How could this teaching be improved?

System of TrainingIn-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest
• Who should we teach?
• What do we teach?
• How do we teach it?
• What resources do we use?
• How meaningful is the session?
• How could this teaching be improved?

Schein RMH. Chest ’90; Franklin C. Crit Care Med ‘94Smith AF. Resuscitation 1998; Hodgetts TJ. Resuscitation ’02
In-Hospital Cardiac Arrest In-Hospital Cardiac Arrest Who should we teach ?
• 50-80% have “warning” signs
• 66% potentially avoidable
• 85% pts recovery in Medical or Surgical Division (Unmonitored Ward Areas – UWA),
die for Sudden Death
• Less then 10% pts recovery in Intensive Care Unit (ICU) die for Sudden Death

• Cardiac Arrest usually is a predictable event NOT caused by primary Cardiac Disease.
• CA follows a period of slow and progressive deterioration (unrecognized or inadequately treated Hypoxemia and Hypotension).
• Rhythm is usually Asystole or PEA
In-Hospital Cardiac Arrest In-Hospital Cardiac Arrest
• Chance of survival is extremely poor.
Unmonitored Ward Areas (UWA)

N= 78Hodgetts TJ. Resuscitation ‘02
Delay in the Diagnosis 77%Error in the Diagnosis 58%Nurse delay informing MD 35%Delayed response of MD Staff 29%Bad evaluation of altered analisys 58%Deficiencies in Acute Care 100%Failure to interpret X-rays 24%
In-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest Reasons for avoidable CA

Hodgetts TJ. Resuscitation ‘02
• Inadequate means (ie defibrillator)• Presence of architectural barriers• Presence of institutional barriers• AED often available in specific divisions• AED often useless for technical reason
(lack of experiences)• Missing of dedicated ‘Emergency Team’• Lengthy delay in CPR
Defibrillation in Italian Hospital occurs ‘OFTEN’ very late Defibrillation in Italian Hospital occurs ‘OFTEN’ very late
Reasons for avoidable CA

• Abnormalities of the A.B.C.
Deficiencies in Acute Care
In hospital cardiac arrest
• MD and Nursing staff with poor acute-care knowledge and skills, with lack of confidence when dealing with problems.
• Incorrect use of O2 therapy and failure to monitor pts
Schein RMH. Chest ’90; Franklin C. Crit Care Med ‘94Smith AF. Resuscitation ’98; Hodgetts TJ. Resuscitation ‘02

CPR Quality during CA
• Chest compressions were not delivered adequately and compressions were too shallow.
• Quality of multiple CPR parameters was inconsistent and often did not meet published guidelines.
Abella BS, Quality of CPR, During In-Hospital Cardiac Arrest. JAMA, ’05
In hospital cardiac arrest

• Pts deterioration is displayed with Common signs (LUNGS, HEART or BRAIN systems)
Recognition of ‘at-risk’ or critically ill pts
In hospital cardiac arrestUnmonitored Ward Areas (UWA)
• Physiological parameters are monitoring and measured less frequently than desirable.
• Monitoring HR, BP, RR may predict CP arrest.

• Significant effects on pt outcome.
• Pts discharged from ICU to GENERAL WARDS during the night have an increased risk of in-hospital death compared to those discharged during the day and those discharged to HIGH-DEPENDENCY UNITS.
• Higher NURSE-Pt Staffing RATIOS are also associated with a reduction in CA rates, as well as rates
of PNEUMONIA, SHOCK and DEATH.
Hospital ProcessDeficiencies in Acute Care
In hospital cardiac arrest

1. FAILURE to use a systematic approach to the
assessment of critically ill pts
2. POOR communication
3. LACK of teamwork
4. INSUFFICIENT use of treatment limitation plans.
Addictional factors Deficiencies in Acute Care
In hospital cardiac arrest

Hodgetts TJ. Resuscitation ‘02
• Inadequate means (ie defibrillator)• Presence of architectural barriers• Presence of institutional barriers• AED often available in specific divisions• AED often useless for technical reason
(lack of experiences)• Missing of dedicated ‘Emergency Team’• Lengthy delay in CPR
Defibrillation in Italian Hospital occurs ‘OFTEN’ very late Defibrillation in Italian Hospital occurs ‘OFTEN’ very late
Reasons for avoidable CA

Which is the RIGHT way ???
UTICCardiochirurg
ia
Medicina Generale
Rianimazione Generale
Chirurgia Generale
PS
Sale Operatorie
Medicina d’ Urgenza

• avoidable CA rate about 2.12/1000 admissions
• CRUDELY extrapolating to the NHS in UK
• There are 23,000 potentially avoidable CA/yr
In-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest
Extrapolating to the whole NHS
• 50-80% have “warning” signs
• 66% potentially avoidable

Evidence-Based Medicine
Gathering Medical Information
Evaluating quality of Medical Information
In-Hospital Cardiac Arrest In-Hospital Cardiac Arrest Evidence Based Medicine (EBM)

Asking questions and finding answers in clinical practice
(and in this room)
• INCLUSION CRITERIA
– Finding knowledge gaps– Asking the right question– Finding an answer– Applying the answer
What are our habits in this respect?

EBM is important because - provides a science-based method for
• Improving physician practice– increase effectiveness / decrease harms (better clinical outcomes / cost-effectiveness)
• Increasing consumer knowledge – understand potential benefits / harms
• Building quality into healthcare systems– using practice guidelines, quality indicators
• Guiding government / employer policies– guide programs / policies on healthcare

Effective Communication’s System

Hammersmith Hospitals Policy
System of TrainingIn-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest
• Teach the right skills
• Teach the right people
• Teach them well
• Positive evaluation and positive feedback
• Empower them to act
• Recall them for ‘refresher’ training
What do we teach?
In-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest
• Introduction to Critical Care course
• Mandatory Skills Update course
• Immediate or Basic Life Support (BLS)
• Advanced (Cardiac) Life Support (ACLS)
• Newborn Life Support Course (NLS)
• Ad hoc sessions
COURSES

In hospital cardiac arrestEarly Warning Scores (EWS)
• EWS is a point system that measure the Routine Vital Sign and their deviation from an arbitrarily ‘NORMAL RANGE”.
• The EWS is used to alert a ward staff or a critical care teams if a pts deteriorate his condition.
• The EWS systems incorporate a ‘CALLING-CRITERIA’ response when one or more measured variables reach an EXTREMELY ABNORMAL VALUE.

• EWS can track changes in physiology and warn of impending physiological collapse (detection of ill
condition at an earlier stage).
In hospital cardiac arrest
• Several studies have identified abnormalities of HR, BP, RR, and conscious level as possible markers
of impending critical events.
Early Warning Scores (EWS)
Recognition of ‘at-risk’ or critically ill pts

Pre-arrest planning Recommendations
1. An EWS system should be in place to identify pts who are critically ill and therefore at risk of CP arrest
2. The institution should have a designated outreach or MET capable of responding to acute clinical crises identified by clinical triggers or other indicators.
3. The institution should have a pt charting system that facilitates the regular measurement and recording of EWS
In hospital cardiac arrest

• Information/Sensitisation of the Staff
• Hospital Staff Training in CPR-D
• Hospital Notification System for Emergencies
• Selection/creation of an Operative Team
• Rational positioning of Emergency Trolley
• Standard procedures for the staff
Key PointKey Point
• Quality CTR system
• Coordination Centre for emergencies
• Retraining of the Staff
In-Hospital Cardiac ArrestIn-Hospital Cardiac Arrest

• Continuous MONITORING of EWS in UWA (high predictive value of CA)
In hospital cardiac arrest
• Increase the frequency of vital sign monitoring.
• FAST and APPROPRIATE response of Medical/Nursing staff to a pt’s abnormal physiology
• A Medical Emergency Team (Medical and Nursing staff from ICU and MD) responds to pts with acute physiological deterioration.
The Role of Education in Cardiac Arrest Response

• MET respects CTR groups reduce CA, deaths and un-anticipated ICU admissions, improved detection of Medical Errors, treatment-limitation decisions, and reduced postoperative ward deaths.
In hospital cardiac arrest
• In UK, a CRITICAL CARE OUTREACH is an integrated system of pre-emptive ward care that reduce ward deaths, postoperative adverse events, ICU admissions and readmissions, and increase survival.
The Role of Education in Cardiac Arrest Response

The Role of Education in Cardiac Arrest Response
• Many CA may be preventable with COURSES specifically designed to prevent physiological deterioration, critical illness, and CA (ALERT Acute Life Threatening Events Recognition and Treatment)
• EBM suggests that they improve knowledge and change attitudes about acute care (BLS, ACLS).
• Training in acute and critical care should commence early. Many countries have established an education programme.
In hospital cardiac arrest

Do outcomes correlate with training?
Survival from ward-based VF/VT CA

• Place critical pts or those at risk of clinical deterioration in areas
where the LEVEL of CARE matched the level of sick.
Recommended strategies for the prevention of avoidable IHCA
• Regularly monitor pt’s vital sign • Match the frequency and type of
observations to the severity of illness of the pt.
• Use an EWS system to identify pts who are critically ill, at risk of clinical deterioration or CA PA or both.

Recommended strategies for the prevention of avoidable IHCA
• A VITAL SIGNS CHART permits the regular measurement and
recording of EWS.
• Ensure that the hospital has a clear policy that requires a clinical response to deterioration in the pt’s clinical condition.• Provide advice on the further clinical management of the pt and the specific responsibilities of MEDICAL and NURSING STAFF.

Recommended strategies for the prevention of avoidable IHCA
• Introducing a clearly identified response to critical illness, that considered a MET able to responding in acute clinical crises.
• The clinical staff should be trained for recognize, monitor and manage the
critical ill pt.
• This MET should be ALERTED using an EWS and must be available 24 hours a day.

• Agree a hospital DNR policy based on national guidelines, and ensure that it is understood by all clinical staff.
• Identify pts for whom CA is an anticipated terminal event for whom CPR would be inappropriate.
Recommended strategies for the prevention of avoidable IHCA
UTICCardiochirurg
ia
Medicina Generale
Rianimazione Generale
Chirurgia Generale
PS
Sale Operatorie
Medicina d’ Urgenza

GRAZIE per la cortese Attenzione






























