Embed Size (px)
Citation preview

Vitamin A deficiency in eye
Many ocular manifestations are results from prolonged and severe lack of vitamin A, usually combined with general malnutrition.
This may manifest as severe clinical deficiency after a precipitating illness,which is most commonly measles or respiratory tract infection or severe diarrhea.
VitaminA is required for vision , maintenance of the integrity of epithelial linings,growth and immunity. Deficiency leads to ocular manifestations.
INTRODUCTION

Vitamin A deficiency is a major cause of childhood mortality and morbidity in India and other developing countries.
-> The ocular manifestations of vitamin A are collectively called xerophthalmia and range from conjunctival xerosis to severe blinding complications such as keratomalacia.
->Deficiency can be diagnosed by the ocular manifestations such as Bitot's spots, serum retinol levels

-> Vitamin A is a fat-soluble vitamin ingested in the diet in two forms-as retinol itself from animal sources, such as milk, meat, fish, liver, and eggs -> or as provitamin carotene from plant sources such as green leafy vegetables, yellow fruits
Vitamin A

In the eye, vitamin A has a pivotal role in the functioning of the retina and the conjunctiva.
->Vitamin A is the backbone of the visual pigments for the rods and the cones
->In the conjunctiva, vitamin A is necessary for the maintenance of the specialized epithelial surface
Vitamin A in eye

The WHO classification of vitamin A deficiency is as follows:
XN Night blindness
X1A Conjunctival xerosis
X1B Bitot's spot
X2 Corneal xerosis
X3A Corneal ulceration/keratomalacia involving one-third or less of the cornea
X3B Corneal ulceration/keratomalacia involving one-half or more of the cornea
XS
XF
Corneal scar
Xerophthalmic fundus

Because of the essential role of vitamin A in photoreceptor function, defective dark adaptation is the most characteristic early clinical feature, resulting in night blindness. -> Night blindness is the earliest clinical symptom and in children it presents as inability to find their way in dim light.
->Its occurrence reflects a failure of rod cells in the retina to maintain peripheral vision under dim light.
->Patient cannot read or drive a car in poor light..
Night blindness

Normal vision Night blindness

Conjunctival xerosis ->Vitamin A deficiency leads to a loss of mucus-secreting goblet cells and eventually to squamous cell metaplasia of the conjunctival epithelial cells.
->Conjunctiva becomes dry, thick, and wrinkled. It gets keratinized, loses its normal transparency, and acquires a smoky appearance
Conjunctival manifestations
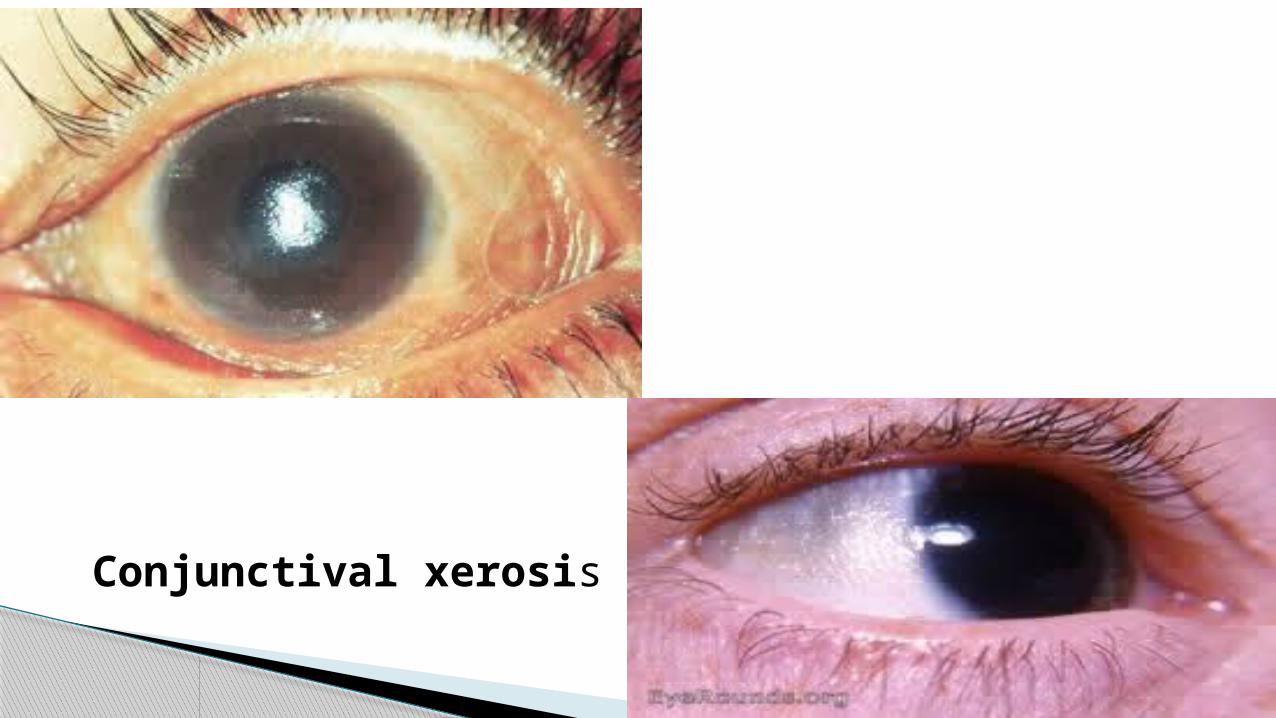
Conjunctival xerosis

Bitot's spots -> Bitot's spots appear as greyish-white triangular
plaques, firmly adherent to the conjunctiva due to increased thickness of conjunctiva in certain areas
-> They respond well to Vitamin A

Keratomalacia Corneal manifestations
The earliest corneal manifestation of xerophthalmia is instability of the precorneal tear film, which can lead to a dull and lustreless corneal appearance.
If xerophthalmia persists for a long time, it progresses to keratomalacia (a full-thickness liquefactive necrosis of the cornea).

These ulcers are small, partial, or of full thickness, located in the periphery in the early stages.
With progression, they can extend to obscure the pupillary axis and develop secondary bacterial infection

KERATOMALACIA

Corneal scar resulting from corneal ulceration due to vitamin A deficiency could potentially lead to blindness.
In severe cases, there can be total loss of vision due to formation of anterior staphyloma (weakening and bulging of cornea lined anteriorly by epithelium and posteriorly by iris)
Corneal scar

Corneal scar

DiagnosisClinical: -> Vitamin A deficiency can be diagnosed clinically by the above-mentioned corneal and conjunctival signs.
-> Night blindness and xerosis are the initial signs of vitamin A deficiency, followed by formation of Bitot's spot.Serum levels of vitamin A:
-> Serum retinol levels can also be assessed to determine vitamin A deficiency.
-> The national prevalence of marginal vitamin A deficiency is defined by serum retinol <20 μg/dl and severe retinol deficiency as <10 μg/dl

Treatment
Oral therapy
Parenteral therapy

Oral therapy:
->The oral regimen of vitamin A is 200,000 IU on day of presentation, next day, and 2-4 weeks later. -> Repeat 200,000 IU every 6 months up to 6 years of age to prevent recurrence.
Parenteral therapy:
-> If the patient has severe disease, is unable to take oral feeds, or has malabsorption, the preferable dose is 100,000 IU of vitamin A given intramuscularly.

Dietary
-> Increasing vitamin A intake from available and accessible foods, achieved through nutritional education, social marketing, home or community garden programs, supplementation:
-> Providing supplementation to high-risk group, particularly to preschool-aged children, on a periodic basis and to mothers within 6-8 weeks after childbirth.
Prevention

Thank u