Embed Size (px)
DESCRIPTION
Citation preview
Clinical Pharmacology of Anesthetic drugs
Dr. Ahsan K. Siddiqui

General Anesthesia
• Definition – Induced, Reversible, controlled, loss of sensation
• Components:
1. Analgesia
2. Muscle relaxation
3. Amnesia
4. Suppression of excessive autonomic
responses
• Practical Conduct :
Pre Anesthetic check up
Just preoperative monitoring
Induction
Maintenance
Recovery
Post operative Care
•

Monitoring
Maintenance
Induction Recovery
Pre op. Check Post op. Care
• Anesthesiologist Tools
Drugs : Hypnotics, Analgesics, Muscle
relaxants & others
Gases : Oxygen, Nitrous Oxide
Vapors: Halothane, Isoflurane, Sevoflurane
Equipments : Anesthetic Machine - Breathing
Circuits, Monitors…….
Others: iv access, Infusion fluid, Airway
equipments……..,…..

Premedication
Reasons for administration of premedications
1. Reduction of fear and anxiety
catecholamine , risks
2. Reduction of saliva secretion
3. Prevention of vagal reflexes (caused by surgical stimulation like squint op., stretching of anal sphincter,
or associated with medication e.g., B –blockers
4. As part of anesthetic technique e.g. use of narcotics

5. To produce amnesia
- Hyoscine ( Scopolamine)
- Benzodiazepines - anterograde amnesia
- Diazepam -hyoscine – in 75% pts complete amnesia
6. For specific therapeutic effects
- Transdermal glyceryl nitrate patches for angina pts,
- Steroids
- B – blockers
(anterograde amnesia- inability to form new memories, Impairment of memory for events occurring after the onset of amnesia)

Drugs : 1. Anxiolysis\ Amnesia: BNZ, Hyosc., Antihist. (H1 Blochers) 2. Analgesia: Opiates
3. Adjuvant to GA : BNZ & Ketamine
4. Anti-emetic : Metoclopramide, Antihist.
5. Antacids : H2 blockers, Antihist., Na Citrate

6. Antihist. : Promethazine,Diphinhydramine
7. Antivagal \ Antisialagogues: Atrop, Hyos.,AntiH
8. Antitromb. / Anticoag.: Heparin, Stockings
9. Antibiotics: Infective Endocarditis Prophylaxis
10: Attention to pre-existing medications:
Continue: unless otherwise
Stop : MAOI, Contraceptive pills
Change : Insulin, oral hypogly., Steroids
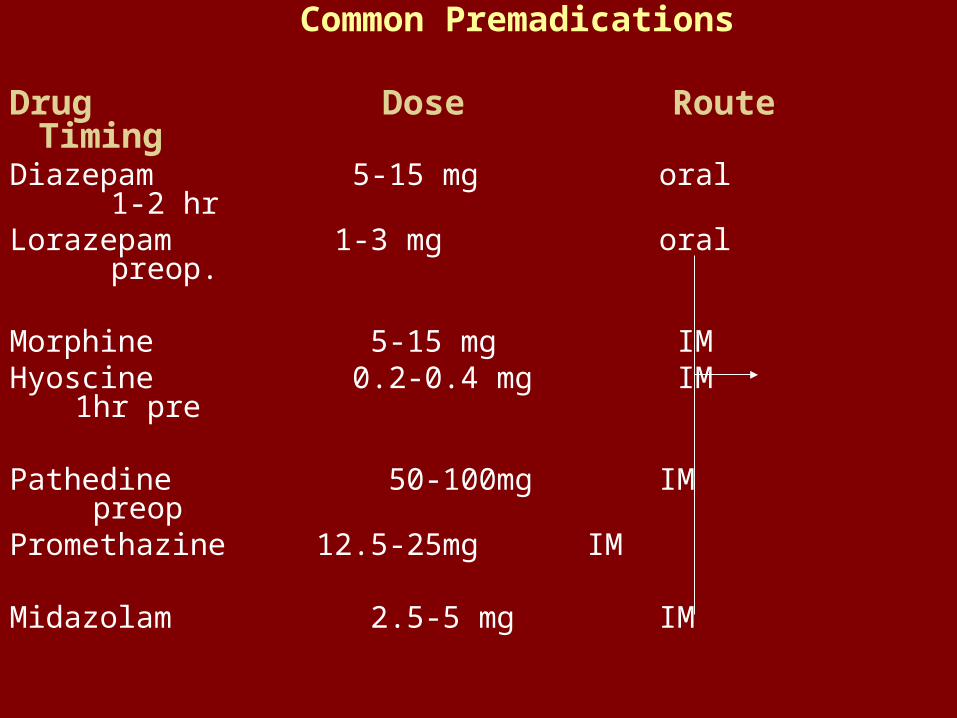
Common Premadications
Drug Dose Route TimingDiazepam 5-15 mg oral 1-2 hrLorazepam 1-3 mg oral preop.
Morphine 5-15 mg IM Hyoscine 0.2-0.4 mg IM 1hr pre
Pathedine 50-100mg IM preopPromethazine 12.5-25mg IM Midazolam 2.5-5 mg IM
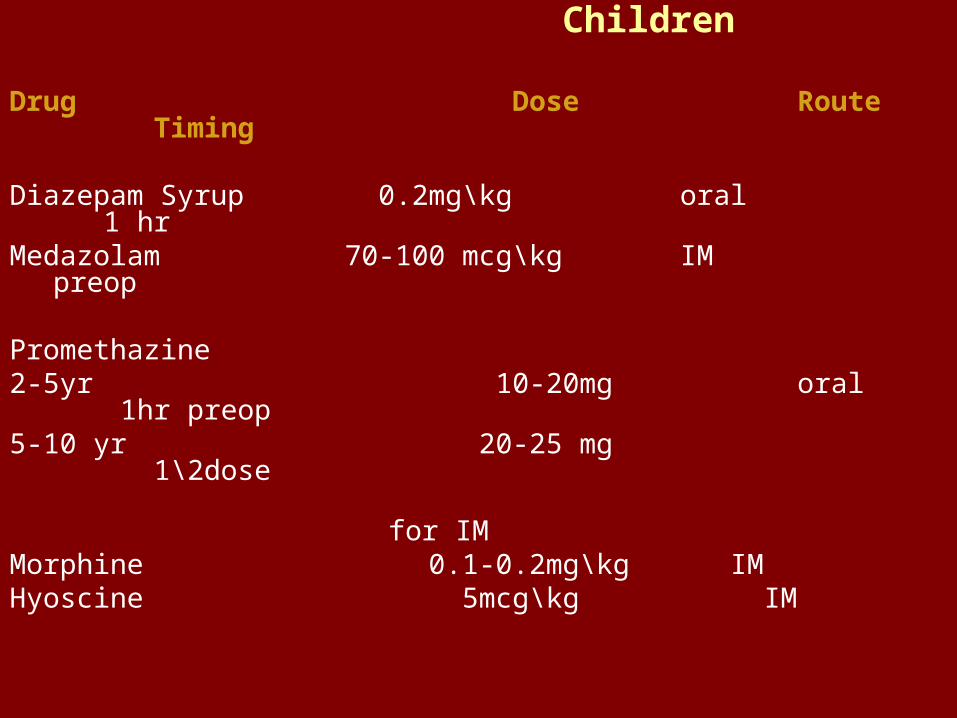
Children
Drug Dose Route Timing
Diazepam Syrup 0.2mg\kg oral 1 hr Medazolam 70-100 mcg\kg IM preop
Promethazine2-5yr 10-20mg oral 1hr preop5-10 yr 20-25 mg 1\2dose for IMMorphine 0.1-0.2mg\kg IMHyoscine 5mcg\kg IM
Side effect of premadications :
Delayed recovery and interaction of Specific drugs
Opioids
• Act on opioid receptors located through out CNS
• Identified as mu - mu1 & mu2
keppa (k)
delta (d)
sigma
• Most effective as producing analgesia
• They provide some degree of sedation

IV opiatesDrugs Dose Onset Duration
Morphine 0.1-0.2mg\kg slowest long
Pathedine 1-2 mg\kg slow long
Fentanyl 1-2mcg\kg rapid short
Alfentanil 10-20mcg\kg v. rapid v. short
Sufentanil 0.2-0.4mcg\kg rapid short
Induction
Check: pt \ machine\ Monitors
Monitoring:
Basic Monitoring:
Anesthetics, clinical, Air way
EKG,NIBP,SpO2, Capnography
Add.: PNS\Temp.\ CVP
Agent for induction : IV vs. Inhalational
Analgesia: Opiates

IV Induction Agents
• The ideal intrav. Agent reliably and pleasantly induces full anesthesia within one arm-brain circulation time
- is free of side effects
- completely wears off in a few minutes
- it must be capable of infusion to maintain
anesthesia without problems.
• I.V. anesthetic agents may be used for
1. Induction of anesthesia
2. As a sole agent for operation (TIVA)
3. To supplement volatile anesthesia or regional
anesthesia
4. For sedation
IV Induction Agents
Propofol – - Mechanism of action – facilitation of inhibitory
neurotransmission mediate by GABA - Not water soluble- 1% solution aqueous solution is available for IV
use as an oil-in-water emulsion containing - soybean oil - egg lecithin - glycerol
• Only for IV administration
• Rapid on set ( one arm brain circulation time)
- 1\2 life 2-8 min. ( recovery rapid, no hangover)
- V. high clearance rate( 10 time that of thiopentone)
• Conjugation in liver results in inactive metabolites
• Excretion – in urine
• Can be used in Chr. Renal F, hepatic ds.

Thiopent. Propofol Ketamine barbiturate phenol
phencyclidine
Pain - - + - -
Phleb. Less more less
Rapid onset ++ +++ +
BP decrease decrease increase
Analgesia -- -- +
Bronch ppt Asthma -- +
Mech. GABA GABA Desociat.
of act.

Recovery Hang over clean headed Emerg.
Delir.
PONV + - Antiemetic +
antipruritic
Duration 10 min 10 min < 10min
Route iv i.v i.v \ i.m
Thiopent. Propofol Ketamine
Commul. ++ - -

• Life Support During Induction
A. Airway : Support: manual \ Atrif. Airway
B. O2 FM + circuit +- An. Agent
Chest expansion\ bag \ monitor
C. Circulatory Support
D. Definitive Airway : Guedel`s Airway
Laryngeal Mask Airway
ETT MR + Circuit + IPPV
MAINTENANCE
Anesthesia ( Tetrad) :
Unconsciousness : Inhal. Vs TIVA
Analgesia : N2O + Opioids / LA
Relaxation : M.R.
Autonomic : Pares. : Anticholin.
: Symp. : GA
Opioids
CVS drugs
Inhalational Anesthetics
• The greater the uptake of anesthetic agent, the greater the difference b \ w the inspired and alveolar conc. And slower the rate of induction.
• Three factors affect anesthetic uptake
1. Solubility in the blood
2. Alveolar blood flow
3. partial pressure difference b\w alveolar gas
and venous blood.
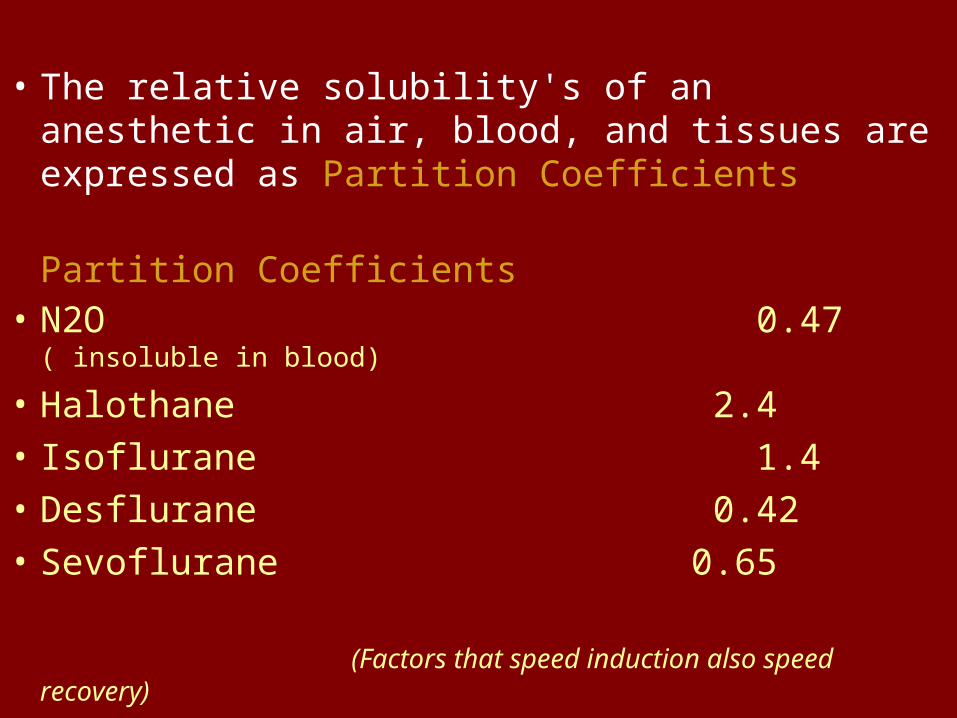
• The relative solubility's of an anesthetic in air, blood, and tissues are expressed as Partition Coefficients
Partition Coefficients• N2O 0.47 ( insoluble in blood)
• Halothane 2.4
• Isoflurane 1.4
• Desflurane 0.42
• Sevoflurane 0.65
(Factors that speed induction also speed recovery)
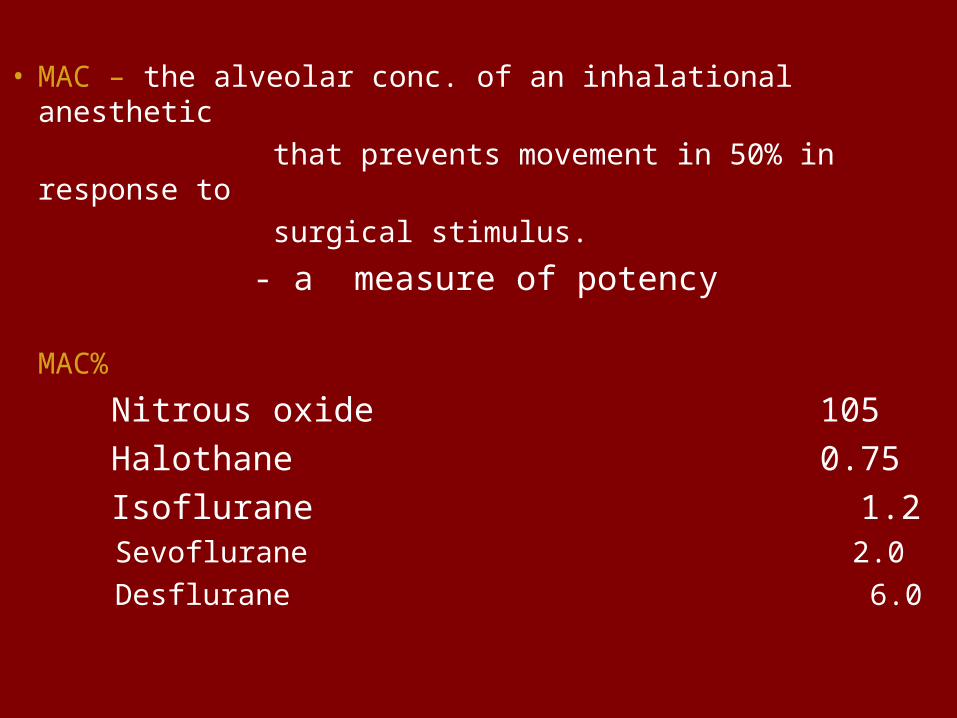
• MAC – the alveolar conc. of an inhalational anesthetic
that prevents movement in 50% in response to
surgical stimulus.
- a measure of potency
MAC%
Nitrous oxide 105
Halothane 0.75
Isoflurane 1.2 Sevoflurane 2.0
Desflurane 6.0
• ISOFURANE – dilates coronary arteries ( but less potent than nitroglycerine or adenosine).
- Can cause (coronary steal syndrome) regional myocardial ischemia)
• DESFLURANE – Low solubility of desflurane in blood and tissues causes a very rapid wash in and wash out of anesthetic.
• SEVOFLURANE – Excellent choice for rapid and smooth inhalational induction.
( b\c of non pungency and rapid increases in alveolar anesthetic conc.)

VOLATILE ANESTHETICS
Halothane Isoflurane Sevoflurane
hydrocarbon -----------halogenated ether-------------
Pleasant ++ -- +_
Smell
MAC 0.75% 1.2% 2%
HR No change
arrhythmia minimal
SVR +_ - - - -
Contractility - minimal - minimal
BP - - - - -
CO +_ or +_ or
minimal minimal

Halothane Isoflurane Sevoflurane
Catachol. + + + - -
sensitisation
Bronchi Dilatation less less
Uterus Relaxation less less
Hepatic Tox. + - - - -
Renal Tox. -- - +

• Neuromuscular Blocking Agents( Ms relaxants) ( no anesthesia, amnesia or analgesia)
• Depolarizing Nondepolarizing Acetyl-choline competitive antagonist receptor agonist
Nondepolarizing Muscle relaxants are not significantly metabolized ( except mivacurium metabolized by pseudocholinestrase & atracurium – metabolized by hofmann elimination and ester hydrolysis )
Need reversal agents ( Cholinesterase inhibitors) that inhibit acetylecholinesterase enzyme activity.

Muscle Relaxants
Sux Dtc. Panc. Vecur. Atrac.
Type Depol ------Non --- Depolarising----------
Onset 30 S. ---3-5 min---- --------2-3 min----
Dur. V. Short ----Long ----- --intermediate --- (3-5 min) ( 30-60min) ( 20-30min)
Dose 1 0.2-0.4 0.6-0.1 0.05-0.1 0.25-.5 ( mg\kg)
Hist. Min. +++ - - +
G.B. - ++ - - -
Vagal - - + - -
Block

Sux Dtc. Panc. Vecur. Atrac
Symp. - - + - -
HR or +_ +_
BP ? +_ +_ +_
Elim. Ps. Ch Es. ----kidney\liver- –liver-- Hoff + esterNotes; Sux. apnoea, K/ ICL/IOP,
Dysrhythmia, MH+, Myalgea ( fasciculation)

Reversal Agents
• Cholinesterase inhibitors ( Anticholinesterse)
• Characteristics of cholinergic receptors
Nicotinic Muscarinic• Location Autonomic Ganglia Glands ( Lacrimal
Sympathetic & salivary, gastric)
parasympathetic Smooth muscle
ganglia (Bronchial, GIT,
Skeletal muscle bladder, bld vessels)
Heart(SA node,AV node)• Agonists Acetylcholine Acetylcholine
Nicotine Muscarine• Antagonist N D P M relaxants Antimuscarinics ( Atropine, Scopolamine,
Glycopyrrolate)
• RECOVERY :
Titrate : Reversal : (Muscle relaxant)
Atropine + Neostegmine
opiate : Nalaxone
Benzodiazepine : flumazinil
Extubation \ Airway
oxygenation
Consciousness

• Pharmacological character of anticholinerg. Dg.
Atropine Scopolamine Glycopyrrolate
Tachycardia +++ + ++
Bronchodilat. ++ + ++
Sedation + +++ 0
Antisialagogue ++ +++ +++
effect
• Post- Operative Care :
R. Room : A. Airway, recovery position
B. O2
C. CVS : Consciousness
Analgesia
MONITORING COMPLECATION IN THE RECOVERY ROOM
HYPOTENTION-HYPERTENSION-ARRHYTHMIA
RESPIRATORY : Airway Obstruction, Hypoxia, Hypoventilation
Delayed recovery
Pain
PONV

• Complication in recovery room
CVS : Hypotension – hypertension – arrhythmia
Respiratory : Airway obstruction, Hypoxia,
Hypoventilation
Delayed Recovery
Pain
PONV
RECOVERY :
Stop Anaesthesia
# Titrate : Reversal : MR : Prostig. + Atropine. Opioids : naloxone
A. Extubation \ Airway B. O2 C. Consciousness

Thank you