Embed Size (px)
Citation preview
Editorial Slides VP Watch, October 23, 2002, Volume 2, Issue 42
Hot Plaque; Cool It, Kill It, Or Crush It?
Ward Casscells, M.D.John Edward Tyson Distinguished Professorship of Medicine
University of Texas-Houston and Texas Heart InstituteHouston, Texas
Detection of vulnerable plaques has become the holy grail of cardiology.
Atherosclerosis is an inflammatory disease. Therefore it can be sought by signs of inflammation.1
Cardinal Signs of Inflammation
Pain
Redness
HEAT
Swelling
Inflammation
Casscells et al. have hypothesized
that vascular inflammation and plaque vulnerability can be identified by the heat released from activated macrophages in the plaque.2

It is known that macrophages are metabolically very active with a high turn-over rate of total ATP content.
Newsholme P. Biochem J. 1989;261:211-8
This high metabolic rate can lead to increased heat production in areas of macrophage accumulation while it cannot be observed in areas of smooth muscle cell accumulation in the absence of inflammatory cell infiltration.
Bjornheden T. Arteriosclerosis. 1987;7:238-47
• In 1996, Casscells, Willerson, et al measured the intimal surface temperatures at 20 sites in each of 50 samples of carotid artery taken at endarterectomy from 48 patients.2
• They found several regions in which the surface temperatures varied reproducibly by 0.2-0.3 degrees C, but 37% of plaques had substantially warmer regions. While macrophage/monocytes density was related to higher temperature, such a relation was not seen with smooth muscle cell density. 2

Temperature Heterogeneity on the Surface of An Endartherectomized Carotid Plaque
Casscells W et al. Lancet. 1996;347:1447-51
• They were also able to show temperature heterogeneity of the surface of human carotid plaques ex vivo by infrared camera. 2
• Later on, Naghavi et al. using a thermosensor catheter showed in vivo temperature heterogeneity of atherosclerotic arteries in dogs and rabbits. Also he found ex vivo that areas with high temperature have low pH.3

Infrared Thermography Confirmed Temperature Heterogeneity of Atherosclerotic Plaques
Dog model of atherosclerosis develops marked lesions in its coronary arteries (left panel). Willerson et al observed significant temperature heterogeneity along the coronary arteries of these dogs using an infrared camera (right panel). 4An infrared camera image
shows marked temperature heterogeneity over the surface of an atherosclerotic carotid plaque
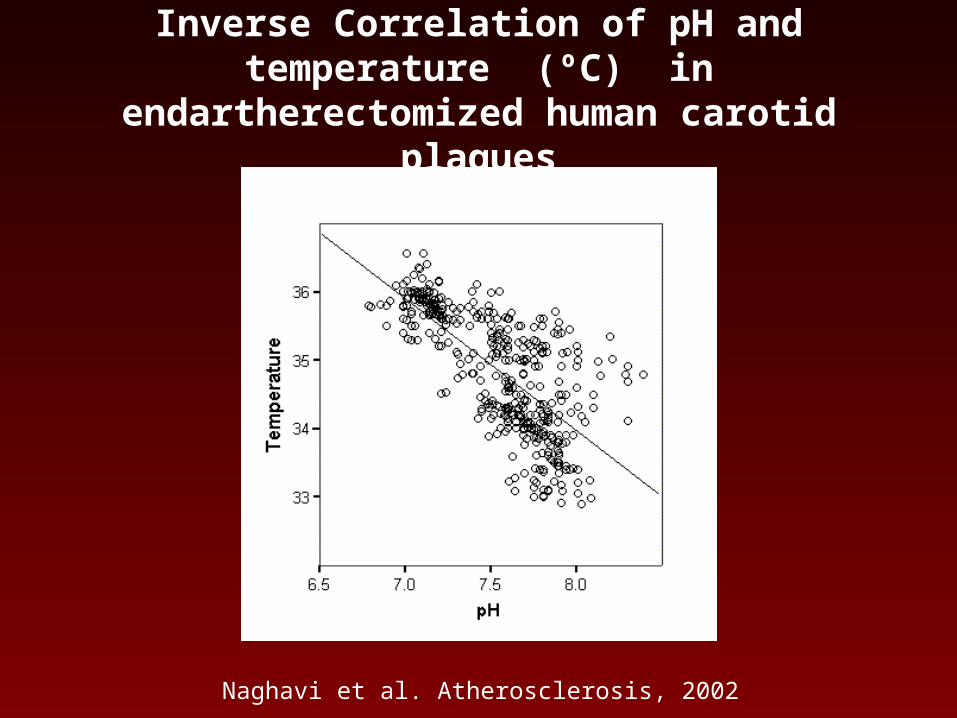
Inverse Correlation of pH and temperature (ºC) in endartherectomized human carotid plaques
Naghavi et al. Atherosclerosis, 2002
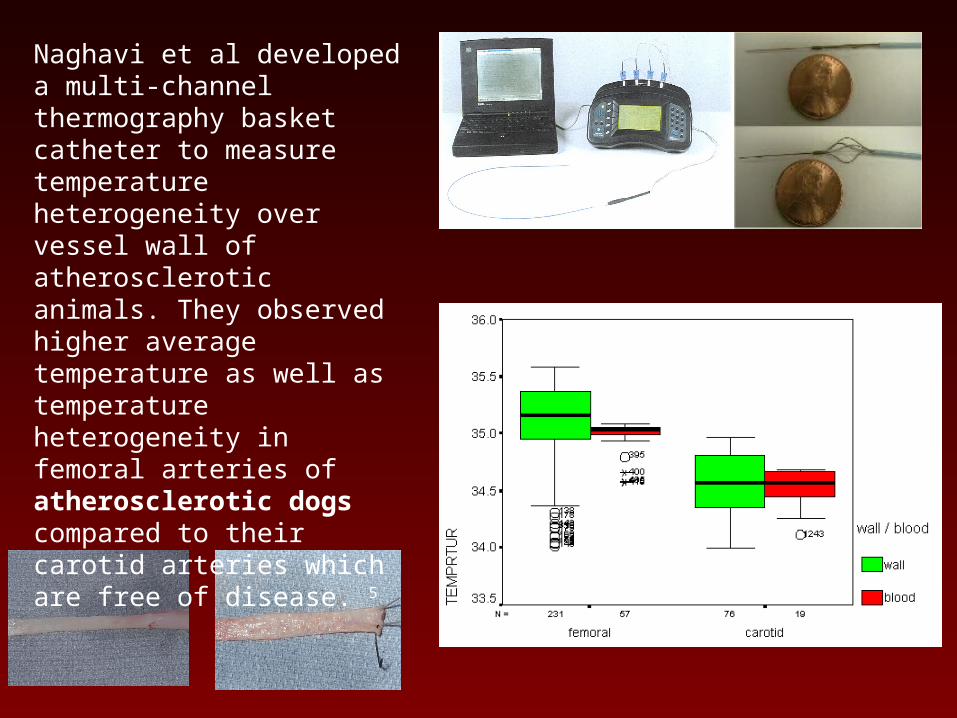
Naghavi et al developed a multi-channel thermography basket catheter to measure temperature heterogeneity over vessel wall of atherosclerotic animals. They observed higher average temperature as well as temperature heterogeneity in femoral arteries of atherosclerotic dogs compared to their carotid arteries which are free of disease. 5
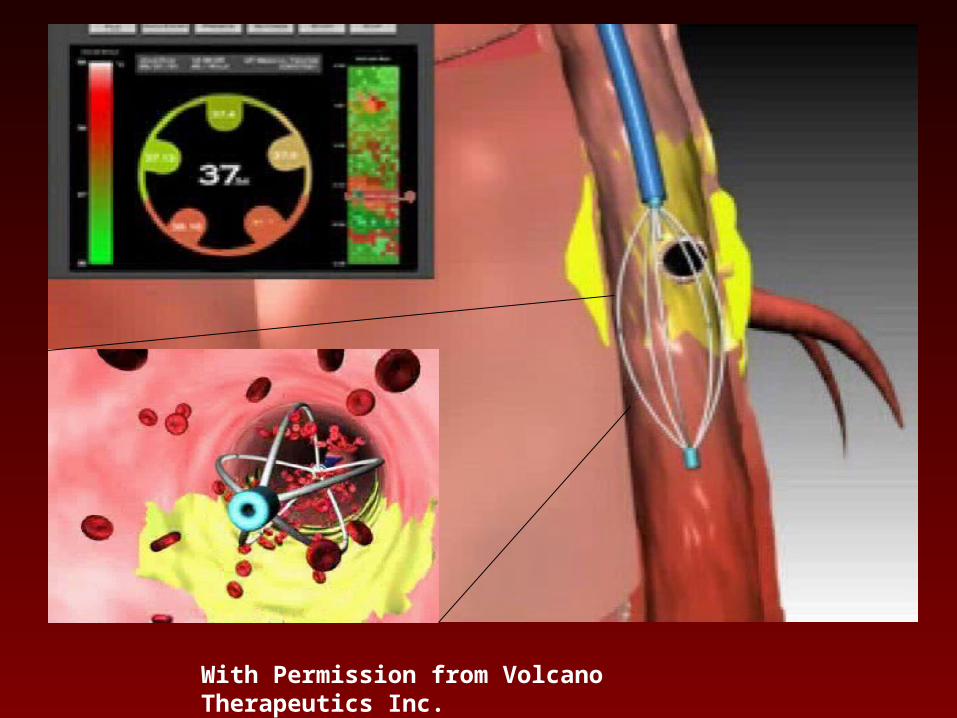
With Permission from Volcano Therapeutics Inc.
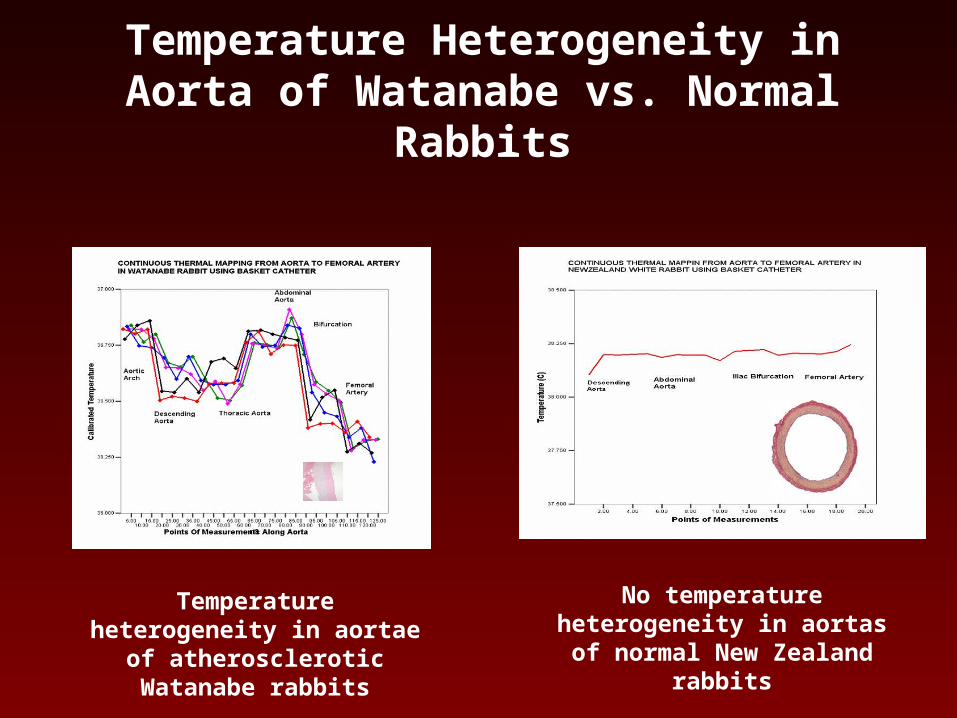
Temperature Heterogeneity in Aorta of Watanabe vs. Normal Rabbits
Temperature heterogeneity in aortae of atherosclerotic
Watanabe rabbits
No temperature heterogeneity in aortas of normal New
Zealand rabbits
• Stefanadis and colleagues from Athens later used a thermography catheter to demonstrate in vivo thermal heterogeneity in human atherosclerotic coronary arteries.
• They observed that temperature was constant within the arteries of the control subjects, whereas most atherosclerotic plaques showed higher temperature compared with the healthy vessel wall.
• Temperature differences between atherosclerotic plaque and healthy vessel wall increased progressively from patients with stable angina to those with acute myocardial infarction. 6
Thermal Heterogeneity – Clinical SyndromeThermal Heterogeneity – Clinical Syndrome

Circulation. 1999;99:1965-71

• In subsequent studies, Stefanadis, Diamantopoulos, and colleagues studied 60 patients with coronary heart disease (CHD) and 20 sex- and age-matched controls without CHD.
• They found strong correlations between C-reactive protein (CRP) and serum amyloid A (SAA) with the temperature differences.7

• Toutozas, Stefanadis and colleagues also reported a strong correlation between remodeling index and temperature difference (DT) between the atherosclerotic plaque and the healthy vessel wall in patients with acute coronary syndromes. 8
• They also showed that serum MMP-9 concentration is correlated with temperature difference in patients with acute coronary syndromes. 9
• In another set of clinical studies on 86 patients undergoing a successful percutaneous intervention, Stefanadis et al found that during a follow-up period of 17.88 +/- 7.16 months, temperature difference between the atherosclerotic plaque and the healthy vessel wall was a strong predictor of adverse cardiac events. 10
• Of clinical importance, Stefanadis et al. found patients on statins show significantly less temperature heterogeneity comparing to those who did not receive statins. 11

As reported in this issue of VP Watch, Stefanadis et al reported the effect of statin therapy on plaque temperature. 12
They measured the temperature differences between the atherosclerotic plaque and the proximal vessel wall using a thermography catheter. 12
The statistical analysis showed that the mean value of temperature differences was higher in the untreated group compared to those who treated with statin. 12
• Stefanadis and colleagues also showed a progressive increase in temperature difference by type of clinical syndrome:
- Statin group• effort angina: 0·24±0·15• unstable angina: 0·26±0·26• acute MI: 0·40±0·28
P<0·05
-Untreated group- effort angina: 0·41±0·26- unstable angina: 0·44±0·28- acute MI: 0·84±0·52

Conclusion:• Intravascular thermography is a novel approach
for detection of inflamed vulnerable plaques.
• Patients on statin treatment produce less heat from the culprit coronary plaque than those not treated.
• Statins have a favorable effect on heat release from hot plaques.
Questions:• How accurate is the measurement of vessel wall
temperature in the presence of flowing blood?
• Is thermography per se enough to make clinical decision or it has to be combined with other anatomical imaging information about plaque?
• Once a “hot plaque” is found, how can we know if it is an inflamed plaque at risk of rupture or an inflamed plaque which is already ruptured?
• What would be the treatment of choice once “hot plaques” are found? Stenting with drug-eluting stent? Heating? Cooling? Killing macrophages with PDT? or aggressive systemic therapy?

References
1. Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med. 1999;340:115-26.
2. Casscells W, Hathorn B, David M, Krabach T, Vaughn WK, McAllister HA, Bearman G, Willerson JT. Thermal detection of cellular infiltrates in living atherosclerotic plaques: possible implications for plaque rupture and thrombosis. Lancet. 1996;347:1447-51.)
3. Naghavi et al. pH Heterogeneity of human and rabbit atherosclerotic plaques; a new insight into detection of vulnerable plaque.Atherosclerosis. 2002 Sep;164(1):27-35.
4. Thermography: A Novel Approach to Identify Plaques at Risk of Rupture and/or Thrombosis. Mohammad Madjid, Morteza Naghavi, James T. Willerson, Ward Casscells, In “The Vulnerable Atherosclerotic Plaque: Understanding, Identification and Modification” edited by Valentin Fuster, Futura Co., NY, 2002
5. Gul K, O'Brien T, Siadaty S, Madjid M, Mohammadi RM, Tewatia T, Willerson JT, Casscells W, Naghavi M. Coronary thermosensor basket catheter with thermographic imaging software for thermal detection of vulnerable atherosclerotic plaques. J Am Coll Cardiol. 2001;37:18A.
6. Stefanadis C, Diamantopoulos L, Vlachopoulos C, Tsiamis E, Dernellis J, Toutouzas K, Stefanadi E, Toutouzas P. Thermal heterogeneity within human atherosclerotic coronary arteries detected in vivo: A new method of detection by application of a special thermography catheter. Circulation. 1999;99:1965-71.
7. Stefanadis C, Diamantopoulos L, Dernellis J, Economou E, Tsiamis E, Toutouzas K, Vlachopoulos C, Toutouzas P. Heat production of atherosclerotic plaques and inflammation assessed by the acute phase proteins in acute coronary syndromes. J Mol Cell Cardiol. 2000;32:43-52.
8. Toutouzas MK, Stefanadis CM, Vavuranakis MM, Tsiamis ME, Tsioufis MC, Pitsavos CM, P.M. T. Arterial remodeling in acute coronary syndromes: correlation of IVUS characteristics with temperature of the culprit lesion. Circulation. 2000;102:II-707.
9. Toutouzas K, Stefanadis C, Tsiamis E, Vavuranakis M, Tsioufis C, Tsekoura D, Vaina S, P. T. The temperature of atherosclerotic plaques is correlated with matrix metalloproteinases concentration in patients with acute coronary syndromes. J Am Coll Cardiol. 2001;37:356A.
10. Stefanadis C, Toutouzas K, Tsiamis E, Stratos C, Vavuranakis M, Kallikazaros I, Panagiotakos D, Toutouzas P. Increased local temperature in human coronary atherosclerotic plaques: an independent predictor of clinical outcome in patients undergoing a percutaneous coronary intervention. J Am Coll Cardiol. 2001;37:1277-83.
11. Stefanadis C, Toutouzas K, Tsiamis E, Vavouranakis M, Kallikazaros I, Toussoulis D, Vaina S, Voutsas A, Pitsavos C, Toutouzas P. Patients with coronary artery disease under statin treatment have decreased heat release from culprit lesions: new insights in the nonlipid effects of statins. Eur Heart J. 2001;22:28 C.
12. C. Stefanadis et al. Statin treatment is associated with reduced thermal heterogeneity in human atherosclerotic plaques; European Heart Journal 2002;23(21):1664-1669