Embed Size (px)
Citation preview

Evidence-informed Health Care for Rare Diseases
Beth Potter, Associate Professor Julian Little, Professor & Director
School of Epidemiology, Public Health & Preventive Medicine University of Ottawa
CORD Rare Disease Day Conference
March 9, 2016

From: International Rare Disease Research Consortium (IRDiRC), www.irdirc.org.
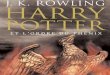
Rarediseaseresearchprogress
# Rare diseases for which a genetic test is available (data from Orphanet)
Cumulative # of medicinal products with orphan designation & marketing approval in Europe and US (data from EMA/FDA)

• Clinical interventions: o Screening tests o Orphan drugs and supplements o Surgery (e.g. organ replacement) o Physical therapy o Diet and lifestyle modifications
• System of care: o Identification/diagnosis (e.g. newborn screening,
diagnostic care) o Organization & coordination of care – multidisciplinary
team care, regionalized treatment centres o Programs to provide access to therapies
Interven2onsforrarediseases

Whystudythesystemofcare?• The effectiveness
gap: outcomes in highly controlled trials (efficacy) often different than outcomes experienced by patients in real world settings (effectiveness)
• To achieve effectiveness, new treatments must be implemented in high quality health care systems
From: Khoury et al, Am J Public Health 2012;102:34-37.

Howdowestudythesystemofcare?
From: Khoury et al, Am J Public Health 2012;102:34-37.
“T2” translational research: studies to evaluate efficacy and effectiveness of interventions (phase III & IV clinical trials; observational studies; systematic reviews)

From: Khoury et al, Am J Public Health 2012;102:34-37.
“T3” translational research: studies to inform the successful integration of interventions into existing systems of care
Howdowestudythesystemofcare?

From: Khoury et al, Am J Public Health 2012;102:34-37.
“T4” translational research: studies that evaluate longer term outcomes of interventions and their impact on population health
Howdowestudythesystemofcare?

ChallengesinstudyingrarediseasecareHierarchyofevidence1. RCT2. Controlledobserva2onalstudies3. Uncontrolledstudies4. Expertopinion
“Itisunfortunatethatscien3stsandcliniciansdealingwiththeveryrarediseaseso7enseemtobelockedintothebo;omrunofthishierarchy”(Wilcken2001)

• Limited knowledge of epidemiology and natural history: are treatments leading to changes in disease progression?
• Defining “effectiveness”: what are the right outcomes? what is a meaningful change?
• Designing evaluative studies that are scientifically sound and feasible in a rare disease setting (i.e., with few patients)
• Working together across geographic boundaries and stakeholder communities (patients/families, providers, policy-makers, researchers) is key to addressing these
Challengesinstudyingrarediseasecare

Rarediseaseresearchnetworks

THE CHANGING FACE OF EPIDEMIOLOGY
Editors’ note: This series addresses topics that affect epidemiologists across a range ofspecialties. Commentaries are first invited as talks at symposia organized by the Editors.This paper was originally presented at the 2006 Congress of Epidemiology in Seattle.
The Emergence of Networks in Human GenomeEpidemiology
Challenges and OpportunitiesDaniela Seminara,* Muin J. Khoury,† Thomas R. O’Brien,‡ Teri Manolio,§ Marta L. Gwinn,†
Julian Little,! Julian P. T. Higgins,#¶ Jonine L. Bernstein,** Paolo Boffetta,†† Melissa Bondy,‡‡Molly S. Bray,§§ Paul E. Brenchley,!! Patricia A. Buffler,¶¶ Juan Pablo Casas,##
Anand P. Chokkalingam,*** John Danesh,††† George Davey Smith,‡‡‡ Siobhan Dolan,§§§Ross Duncan,!!! Nelleke A. Gruis,¶¶¶ Mia Hashibe,†† David Hunter,¶¶¶
Marjo-Riitta Jarvelin,###**** Beatrice Malmer,†††† Demetrius M. Maraganore,‡‡‡‡Julia A. Newton-Bishop,§§§§ Elio Riboli,†† Georgia Salanti,¶ Emanuela Taioli,!!!! Nic Timpson,†††
Andre G. Uitterlinden,¶¶¶¶ Paolo Vineis,####### Nick Wareham,***** Deborah M. Winn,*Ron Zimmern,# and John P. A. Ioannidis†††††‡‡‡‡‡ for the Human Genome Epidemiology Network
and the Network of Investigator Networks
Large-scale “big science” is advocated as an approach to complex research problems inmany scientific areas.1 Epidemiologists have long recognized the value of large
collaborative studies to address important questions that are beyond the scope of a studyconducted at a single institution.2 We define networks (or, interchangeably, consortia) asgroups of scientists from multiple institutions who cooperate in research efforts involving,but not limited to, the conduct, analysis, and synthesis of information from multiplepopulation studies. Networks, by virtue of their greater scope, resources, population size,and opportunities for interdisciplinary collaboration, can address complex scientificquestions that a single team alone cannot.3
There is a strong rationale for using networks in human genome epidemiologyparticularly. Genetic epidemiology benefits from a large-scale population-based approachto identify genes underlying complex common diseases, to assess associations betweengenetic variants and disease susceptibility, and to examine potential gene–environmentinteractions.4–6 Because the epidemiologic risk for an individual genetic variant is likelyto be small, a large sample size is needed for adequate statistical power.7 Power issues areeven more pressing for less common disease outcomes. Replication in different popula-tions and exposure settings is also required to confirm and validate results. The adoptionof common guidelines for the conduct, analysis, reporting, and integration of studiesacross different teams is essential for credible replication. Transparency in acknowledgingand incorporating both “positive” and “negative” results is necessary to direct subsequentresearch. Furthermore, newer and more efficient genotyping technologies must be inte-grated rapidly into current and planned population studies.8,9 Networks can supportstudies with sample sizes large enough to achieve “definitive” results, promote spinoff
Supported by the Intramural Research Program of the NIH, National Cancer Institute, Division of Cancer Epidemiology and Genetics and the National CancerInstitute Extramural Program, Division of Cancer Control and Population Sciences, Epidemiology and Genetics Research Program.
The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services nor does mention of tradenames, commercial products, or organizations imply endorsement by the U.S. Government.
Editors’ note: Related papers appear on pages 9, 13, and 18.Correspondence: Daniela Seminara, Epidemiology and Genetics Research Branch, Division of Cancer Control and Population Sciences, National Cancer
Institute, NIH, EPN Bldg., Rm. 5142, MSC 7393, 6130 Executive Blvd., Bethesda, MD 20892. E-mail: [email protected] © 2006 by Lippincott Williams & WilkinsISSN: 1044-3983/07/1801-0001DOI: 10.1097/01.ede.0000249540.17855.b7
Epidemiology • Volume 18, Number 1, January 2007 1

ChallengesFacedbyInves2gatorNetworks
• Resourcesforestablishingtheini2alinfrastructure,suppor2ngconsor2aimplementa2on,andaddingnewpartners
• Coordina2on:minimizeadministra2ontomaximizescien2ficprogressandavoidconflicts
• Selec2onoftargetprojects• Variabledataandbiospecimenqualityfrompar2cipa2ng
teams• Handlingofinforma2onfromnonpar2cipa2ngteamsandof
nega2veresults• Collec2on,management,andanalysisofcomplexand
heterogeneousdatasetsSeminaraetal.,2007

ChallengesFacedbyInves2gatorNetworks
• Anticipating future needs • Communication and coordination • Scientific credits and career development • Access to the scientific community at large and
transparency • Peer review • Informed consent
Seminaraetal.,2007

Networks• BoXomup• Topdown

• The Canadian Inherited Metabolic Diseases Research Network (CIMDRN): ~50 investigators (multidisciplinary), 14 pediatric metabolic centres
• Funding: CIHR Emerging Team Grant (2012-17) • Goal: generate evidence to improve care & outcomes
for pediatric inherited metabolic diseases (IMD)
• Interest in outcomes across the “triple aim”: clinical outcomes, patient and family experiences, health system impacts
• “Practice-based research”: collect observational data about existing treatments & outcomes to make inferences about patterns of care that work best
CIMDRN

• Consent-based enrollment of children born 2006-2015 and receiving care for one of ~30 IMD at a participating centre (>420 families enrolled so far)
• Research (several completed/ongoing studies): o Clinical interventions and outcomes (data abstracted
from charts with families’ permission)
o Patient and family-reported experiences (qualitative interviews, survey)
o Health system impacts (health services use data)
• Successes: engaged investigators, enthusiastic participation of families, high quality data
• Challenges: administration of multi-centre research, sustainability
CIMDRN

RareDiseasesClinicalResearchNetwork
(RDCRN-USNa&onalCenterforAdvancingTransla&onalSciences)• TheRDCRNfacilitatesclinicalresearchinrarediseases
throughsupportfor:• Collabora2veac2vi2es,includingmul2sitelongitudinal
studiesofindividualswithrarediseases,and/orclinicaltrials• Trainingofclinicalinves2gatorsinrarediseasesresearch• Pilotanddemonstra2onprojects• Uniformdatacollec2onprotocols• Accesstoinforma2onaboutrarediseasesforbasicand
clinicalresearchers,academicandprac2cingphysicians,pa2ents,andthepublic

RCDRN• 22clinicalresearchconsor2a• Eachconsor2um
o focusesonatleastthreerelatedrarediseaseso par2cipatesinmul2sitestudieso incorporatespa2entadvocacygroupsasresearchpartners
• DataManagementandCoordina2ngCenterintendedtoenableuniformcollec2onandanalysis,andfacilitateinforma2onsharingacrossthenetwork
• Overallabout2,600researchersathundredsofclinicalsitesinterna2onallyinvolved
• Since2003,nearly29,000par2cipantsenrolledinnetworkclinicalstudies
• Fundingandscien2ficoversightprovidedbyNCATS,10otherNIHen22es,andbypa2entadvocacyorganiza2ons

Pa2ent-CenteredOutcomesResearchIns2tute
• PCORI’sauthorizinglawcallsforafocusonrarediseases(condi2onsthataffectfewerthan200,000peopleinUS)
• specialpooloffunding• Fundedprojectstocomparetreatmentsforureacycledisorders,
non-cys2cfibrosisbronchiectasis,&syringomyelia• PCORIrequiresthatallstudiescomparetwodifferenceapproaches
forpreven2on,diagnosis,treatmentorcaredelivery• interestedinfundingcomparisonsofreal-worldclinicalop2ons,
proposedstudieswillnotqualifyiftherearenoefficacydataortheproposedinterven2onsarenotconsideredaclinicalop2onforindividualswithagivenraredisease

Europeannetworksofreferenceforrarediseases
• MainaddedvalueofEuropeanReferenceNetworks(ERN)andassociatedCentresofReferenceistofacilitateimprovementsinaccesstodiagnosisanddeliveryofhigh-quality,accessibleandcost-effec2vehealthcareforpa2entswhohaveamedicalcondi2onrequiringapar2cularconcentra2onofexper2seorresources,par2cularlyinmedicaldomainswhereexper2seisrare
• ERNfocalpointsformedicaltrainingandresearch,informa2ondissemina2onandevalua2on
• Centresintendedtoserveasresearchandknowledgefoci,upda2ngandcontribu2ngtothelatestscien2ficfindings,trea2ngpa2entsfromotherMemberStatesandensuringtheavailabilityofsubsequenttreatmentfacili2eswherenecessary

Europeannetworksofreferenceforrarediseases
• AmongMemberStatesthathaveestablishedsuchcentres,nocommondefini2on!
• processforiden2fying,selec2nganddesigna2ngcentresofreferencevariesmarkedlybetweenUK,France,Italy&Denmark
• Twomainpurposes:1. provideara2ngschemethatenablesconsumerstoiden2fytheappropriatehealth-care
resource2. toenablehealth-caremanagersiden2fywherebesttoallocatefinancialresources
• EuropeanUnionCommiXeeofExpertsonRareDiseases(EUCERD)hasmade45Recommenda2onsonQualityCriteriaforCentresofExper2seo MissionandScope;Designa2onCriteria;ProcessofDesigna2onandEvalua2on;European
Dimension
• ~12projectsfunded

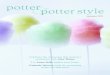
Pa2ent/familyengagement
Figure 2, Shippee et al, Health Expectations 2013;18:1151-1166
• Engaging with patients/families recognized as key to research that aims to inform care
• Patient-oriented research occurs on a continuum: patients/families as participants, consultants, collaborators, partners, or leaders of research

Pa2entinvolvementinrarediseaseresearch• Providing patient-centred care
requires that outcomes of importance to patients are prioritized in research
• Patients with rare diseases and their families are frequently experts about health care needs
• Rare disease organizations are leading the way (e.g., PCORnet patient-powered research networks)

• Our group has undertaken two qualitative studies to understand the experiences and needs of families of children with rare inherited metabolic diseases (IMD) related to the system of care:
1. Study recommended by patients/family members on our network advisory board: perspectives of patient advocacy organizations on families’ experiences and needs
2. Study of parents/caregivers of children with IMD
Examplesofpa2entperspec2vesoncare
Funding from CIHR & the Rare Disease Foundation • Khangura et al., JIMD 2016;139-47 • Siddiq, MSc thesis

• Families are often experts about care and act as educators/advocates; they report mixed experiences with providers: o “I think parents can be fantastic resources, and I think
doctors… are very receptive to hearing from patients…”(study 1, participant 12)
o “…not all physicians are willing to accept that usually the mom and dad know more about this particular [disease]…” (study 1, participant 16)
o “When we go to the ER in crisis…we know what to say, we know what's going to work… we've come up against a couple of doctors in the ER that don't appreciate that, they want to be the ones to when they walk into the room, everyone looks to them for the answers…” (study 2, participant 21)
Selectedfindings

• In this patient population, parents/caregivers are generally happy with the care their child receives from the specialist metabolic clinic team: o “...our experience is amazing. We have a fantastic
doctor and a fantastic dietitian. The backup dietitian and the backup doctor are equally as knowledgeable.” (study 2, participant 15)
o "Oh, when she was diagnosed it was great because [metabolic physician] and [dietitian] would come in together and we got a chance to see both. We have an option to see them separately. So yah, there is definitely a good coordination between them." (study 2, participant 1)
Selectedfindings

• But families frequently experience challenges with care and its coordination outside the specialist clinic: o “…I think everybody who has a child with a complex
medical condition like this would benefit from having more coordination. You know, being able to go into a clinic and see several specialists in one day… And that really doesn’t happen right now….the burden of getting to all these appointments is huge.” (study 1, participant 3)
o “… I just have a lot of stress around mostly around the health care that we received there [emergency department] because I can't say that it's consistent at all…I feel like almost like I have to prove that they are sick…" (study 2, participant 2)
Selectedfindings

• Challenges with care often manifest as single negative encounters, which accumulate and are an important source of stress: o “…like in a matter of three days that [hospital] room
had become my home, you know? And that was where I’d stay, and I never left my son’s bedside. And then when they’d tell me we were moving, like, my heart would just sink and I’d almost be in tears over it because I couldn’t handle any more change… and that was very, very difficult as a family… (study 1, participant 6)
o "…we were told not to use medication from home ...but the pharmacy, when she was in Emerg that afternoon, they were going to send up her meds from pharmacy, which they didn't…" (study 2, participant 05)
Selectedfindings

• There is a need for patient- and family-oriented health services research to complement the exciting advances in the diagnosis and development of new therapies for rare diseases
• This research will ensure that these treatments are implemented in high quality systems that can maximize their effectiveness
• This research should incorporate lessons that the rare disease community has learned about working together across boundaries, both geographic and disciplinary
Conclusions


RCDRNConsor2a1. AmyotrophicLateralSclerosisandRelatedDisorders2. AutonomicRareDiseases3. BrainVascularMalforma2on4. BriXleBoneDisorders5. ChronicGranVersusHostDisease6. DevelopmentalSynaptopathiesAssociatedwithTSC,PTENandSHANK3Muta2ons7. Dystonia8. EosinophilicGastrointes2nalDisease9. FrontotemporalLobarDegenera2on10. Gene2cDisordersofMucociliaryClearance11. InheritedNeuropathies12. LysosomalDisease13. MitochondrialDisease14. NephrolithiasisandKidneyFailure:TheRareKidneyStoneConsor2um15. Nephro2cSyndrome16. Porphyrias17. PrimaryImmuneDeficiency18. RareLungDiseases(MolecularPathway-DrivenDiagnos2csandTherapeu2cs)19. ReXSyndrome,MECP2Duplica2onsandReX-RelatedDisorders20. SterolandIsoprenoid21. UreaCycleDisorders22. Vasculi2s

ERNforrarediseases–fundedprojects
1. Cys2cfibrosis2. Dysmorphology3. Alpha-1an2trypsindeficiency4. Porphyria5. RareBleedingDisorders6. paediatricHodgkin’slymphoma7. RarePaediatricNeurologicalDiseases(NEUROPED)8. Langerhanscellhis2ocytosisandassociatedsyndrome9. SevereGenodermatoses10. RareAnaemias11. Refractoryepilepsyandepilepsysurgery(E-PILEPSY)12. ExpertPaediatricOncologyReferenceNetworkforDiagnos2csand
Treatment(ExPO-r-NeT)

BMJ | 1 MAY 2010 | VOLUME 340 963
RESEARCH METHODS & REPORTING
1School for Health and Related Research, University of Sheffield, Sheffield2Department of Health Sciences, University of York, Heslington, York3School of Healthcare, University of Leeds, LeedsCorrespondence to: C Relton [email protected]: 16 November 2009
Cite this as: BMJ 2010;340:c1066doi: 10.1136/bmj.c1066
Pragmatic trials are important for informing routine clinical practice, but current designs have shortcomings. Clare Relton and colleagues outline the new “cohort multiple randomised controlled trial” design, which could help address the problems associated with existing approaches
Rethinking pragmatic randomised controlled trials: introducing the “cohort multiple randomised controlled trial” designClare Relton,1 3 David Torgerson,2 Alicia O’Cathain,1 Jon Nicholl1
Randomised controlled trials are generally held to be the “gold standard” for establishing how well an intervention works. Trials that aim to determine the efficacy of a treat-ment by using a double blind, placebo controlled design (that is, explanatory trials) are, however, sometimes criti-cised. For example, although the design of explanatory tri-als results in strong internal validity—we can depend upon the results of a given trial—such trials may have limited external validity: we can’t be confident that we can apply the results to routine clinical practice. Pragmatic trials,1 2 which aim to inform healthcare decision making in prac-tice, have been offered as a solution in that they retain the rigour of randomisation (thus eliminate selection bias) but retain the characteristics of normal clinical practice.
The implementation and interpretation of both prag-matic and explanatory randomised controlled trials are associated with significant problems. This article describes a trial design that helps address these prob-lems—the “cohort multiple randomised controlled trial” approach.
Problems with randomised controlled trialsExisting clinical trial designs can have shortcomings in four areas: recruitment; ethics; patient preferences; and treatment comparisons.
RecruitmentThe majority of randomised controlled trials have difficulty recruiting sufficient numbers of patients. For example, one investigation found that less than a third of 114 multicen-tre, publicly funded UK trials recruited their original target number of patients within the time originally specified.3 Failure to recruit to target may have implications for the power and generalisability of trial results.
Moreover, many clinical trials exclude hard to reach groups and ethnic minorities,4 resulting in disparities between the “with need” (reference) population and the trial population.5 6 Measures of real world effectiveness are vital for analyses of benefit, harm, and cost effectiveness. If the reference population is not adequately represented in a trial and effectiveness is variable, then such analyses cannot accurately inform real world decisions.
EthicsThe most common reason given by patients (and clini-cians) for not participating in clinical trials is “concerns with information and consent.”7 In routine real world health care, patients are rarely told of treatments that their clinicians cannot with certainty provide,8 nor are patients told their treatment will be decided by chance. On the other hand, in clinical trials providing this type of “full” information before randomisation is regarded as an ethical requirement.
Patient preferencesStandard “open” (unblinded) pragmatic trials often com-pare an intervention with treatment as usual. Where the “standard care” on offer is available outside the trial, however, the only incentive for the patient to participate (apart from altruism) is to receive the new intervention. If a patient is allocated to treatment as usual, he or she may withdraw from the trial (attrition bias) or exhibit disap-pointment bias when reporting outcomes.9
Treatment comparisonsA common research scenario is addressing a clinical problem with many potential treatments. Yet often each
SUMMARY POINTSThe “cohort multiple randomised controlled trial” (cmRCT) design tackles some of the problems associated with pragmatic trial designs, such as recruitmentThe cmRCT design has several innovative features: a large observational cohort of patients is recruited and used as a multiple trials facility; each randomised controlled trial uses random selection of some participants (not random allocation of all); and “patient centred” information and consent is appliedThe cmRCT design is best suited to: open trials where “treatment as usual” is compared with the offer of treatment; easily measured and collected outcomes; conditions where many trials will be conducted; and trials of desirable or expensive interventionsFurther research is required to address a range of analysis, implementation, and ethical questions related to the cmRCT design
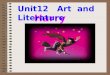
Large observational cohort (N)
Regular outcome measurement
Eligible patients identified (NA)
Random selection of some eligible patients (nA) and outcomes compared with those receiving usual care (NA–nA)
Eligible patients identified (NB)
Random selection of some eligible patients (nB) and outcomes compared with those receiving usual care (NB–nB)

Using the cohort multiple randomised controlled trial design
966 BMJ | 1 MAY 2010 | VOLUME 340
RESEARCH METHODS & REPORTING
for patients who comply with the protocol (albeit usually with loss of power), unlike per protocol or on treatment analysis.
Secondly, we could try to avoid some potential non-com-pliance by presenting cohort patients with a list of possible interventions at enrolment and asking which they would consider agreeing to use if offered. This process identi-fies the potential compliers in advance and consequently reduces dilution effects; however, care must be taken to avoid false expectation of future treatment and the loss of feature VII, patient centred information and consent.
In researching interventions already available in routine health care, it will be necessary to identify and monitor which patients use or have used these.
Furthermore, discrete trials are currently supported by private and public funding infrastructures and institutional frameworks, to the tune of £100 000 per trial. Existing infrastructures and frameworks might struggle to deter-mine a funding approach for cmRCTs.
Examples of the cmRCT designCampbell and colleagues18 recently adapted the ran-domised consent (Zelen) method and developed an approach in which patients consented to an observational study and were then all randomly allocated to either intervention or control in a randomised controlled trial.
Although this method shares several features with the cmRCT design (features I, II, IV, and VII), it does not have the capacity for multiple randomised controlled trials (feature III) or use random selection of some instead of random allocation of all (features V and VI).
We have obtained ethical approval for and have con-ducted a pilot study of the cmRCT design.21 In this pilot, a large observational cohort of 856 women aged 45-64 was recruited and their outcomes measured. A total of 72 women reported frequent or severe menopausal hot flushes, or both. Of these 72 women, 48 were eligible for the trial treatment (NA) and 24 were randomly selected to be offered the treatment (nA). The outcomes of the ran-domly selected patients were then compared with the outcomes of those eligible patients not randomly selected (NA − nA) using both intention to treat analysis and CACE analysis.20 Patients were not told about the treatments that they were not randomly selected to be offered.
The clinical outcomes of this pilot will be reported sepa-rately. However, a post hoc evaluation of the design found that the design was acceptable to patients, clinicians, and the NHS Research ethics committee. The concept of multi-ple trials within a single cohort of patients (feature III) has not yet been tested.
The cmRCT design is currently being used to address questions in the management of obesity (http://clahrc-sy.nihr.ac.uk/theme-obesity.html). The 20 year study is pro-jected to recruit a cohort of 20 000 adults aged 16 years or more, and multiple trials will be embedded within this cohort. To maximise the long term benefits of this study, it is planned that the cohort will be “open” and will be replenished with new recruits (16 and 17 year olds) every two years.
SummaryThe cmRCT design appears to be a workable and useful approach to pragmatic research questions that aim to inform healthcare decisions within routine practice. The design is best suited to circumstances that require open (rather than blinded) trials where “treatment as usual” is compared with the offer of study treatment, and to questions with outcomes that can be easily measured in the whole cohort (for exam-ple, patient reported outcomes). Clinical conditions where many clinical trials will be conducted and trials of desirable or expensive interventions are also well suited to the cmRCT approach.
There are challenges to the cmRCT design. Further research is required to address a range of analysis and implementation questions related to the design and the ethics of patient centred informed consent for pragmatic randomised controlled trials.
In his Harveian oration at the Royal College of Physicians, London, Professor Michael Rawlins, chair of the National Institute for Health and Clinical Excellence, called for “investigators to continue to develop and improve their methodologies in order to help decision makers appraise the evidence.”22 We hope that the cmRCT design goes some way towards addressing the problems associated with exist-ing approaches. If these problems are addressed, then per-haps the most important problem of all will be resolved—the non-implementation of the results of clinical research.
Using the cohort multiple randomised controlled trial design
Most suited to: Settings
Open trials with “treatment as usual” as the comparatorStudies that aim to inform healthcare decisions in routine practice (pragmatic trials)Research questions that address easily measured and collected outcomes
PopulationsStable populationsEasily identified populations
Clinical conditionsClinical conditions for which many trials will be conducted; for example, obesity, diabetes, chronic pain Chronic conditionsConditions for which previous trials have struggled with recruitment
TreatmentsTreatments highly desired by patientsExpensive treatments
Least suited to:Settings
Closed trial designs with masking or a placebo armStudies that aim to further knowledge as to how and why a treatment works (efficacy trials) Research questions that address hard to measure and hard to collect outcomes
PopulationPopulations with high attritionUnstable patient populationsDifficult to identify populations
Clinical conditionsAcute or short term conditions
TreatmentsTreatments not highly desired by patients
966 BMJ | 1 MAY 2010 | VOLUME 340
RESEARCH METHODS & REPORTING
for patients who comply with the protocol (albeit usually with loss of power), unlike per protocol or on treatment analysis.
Secondly, we could try to avoid some potential non-com-pliance by presenting cohort patients with a list of possible interventions at enrolment and asking which they would consider agreeing to use if offered. This process identi-fies the potential compliers in advance and consequently reduces dilution effects; however, care must be taken to avoid false expectation of future treatment and the loss of feature VII, patient centred information and consent.
In researching interventions already available in routine health care, it will be necessary to identify and monitor which patients use or have used these.
Furthermore, discrete trials are currently supported by private and public funding infrastructures and institutional frameworks, to the tune of £100 000 per trial. Existing infrastructures and frameworks might struggle to deter-mine a funding approach for cmRCTs.
Examples of the cmRCT designCampbell and colleagues18 recently adapted the ran-domised consent (Zelen) method and developed an approach in which patients consented to an observational study and were then all randomly allocated to either intervention or control in a randomised controlled trial.
Although this method shares several features with the cmRCT design (features I, II, IV, and VII), it does not have the capacity for multiple randomised controlled trials (feature III) or use random selection of some instead of random allocation of all (features V and VI).
We have obtained ethical approval for and have con-ducted a pilot study of the cmRCT design.21 In this pilot, a large observational cohort of 856 women aged 45-64 was recruited and their outcomes measured. A total of 72 women reported frequent or severe menopausal hot flushes, or both. Of these 72 women, 48 were eligible for the trial treatment (NA) and 24 were randomly selected to be offered the treatment (nA). The outcomes of the ran-domly selected patients were then compared with the outcomes of those eligible patients not randomly selected (NA − nA) using both intention to treat analysis and CACE analysis.20 Patients were not told about the treatments that they were not randomly selected to be offered.
The clinical outcomes of this pilot will be reported sepa-rately. However, a post hoc evaluation of the design found that the design was acceptable to patients, clinicians, and the NHS Research ethics committee. The concept of multi-ple trials within a single cohort of patients (feature III) has not yet been tested.
The cmRCT design is currently being used to address questions in the management of obesity (http://clahrc-sy.nihr.ac.uk/theme-obesity.html). The 20 year study is pro-jected to recruit a cohort of 20 000 adults aged 16 years or more, and multiple trials will be embedded within this cohort. To maximise the long term benefits of this study, it is planned that the cohort will be “open” and will be replenished with new recruits (16 and 17 year olds) every two years.
SummaryThe cmRCT design appears to be a workable and useful approach to pragmatic research questions that aim to inform healthcare decisions within routine practice. The design is best suited to circumstances that require open (rather than blinded) trials where “treatment as usual” is compared with the offer of study treatment, and to questions with outcomes that can be easily measured in the whole cohort (for exam-ple, patient reported outcomes). Clinical conditions where many clinical trials will be conducted and trials of desirable or expensive interventions are also well suited to the cmRCT approach.
There are challenges to the cmRCT design. Further research is required to address a range of analysis and implementation questions related to the design and the ethics of patient centred informed consent for pragmatic randomised controlled trials.
In his Harveian oration at the Royal College of Physicians, London, Professor Michael Rawlins, chair of the National Institute for Health and Clinical Excellence, called for “investigators to continue to develop and improve their methodologies in order to help decision makers appraise the evidence.”22 We hope that the cmRCT design goes some way towards addressing the problems associated with exist-ing approaches. If these problems are addressed, then per-haps the most important problem of all will be resolved—the non-implementation of the results of clinical research.
Using the cohort multiple randomised controlled trial design
Most suited to: Settings
Open trials with “treatment as usual” as the comparatorStudies that aim to inform healthcare decisions in routine practice (pragmatic trials)Research questions that address easily measured and collected outcomes
PopulationsStable populationsEasily identified populations
Clinical conditionsClinical conditions for which many trials will be conducted; for example, obesity, diabetes, chronic pain Chronic conditionsConditions for which previous trials have struggled with recruitment
TreatmentsTreatments highly desired by patientsExpensive treatments
Least suited to:Settings
Closed trial designs with masking or a placebo armStudies that aim to further knowledge as to how and why a treatment works (efficacy trials) Research questions that address hard to measure and hard to collect outcomes
PopulationPopulations with high attritionUnstable patient populationsDifficult to identify populations
Clinical conditionsAcute or short term conditions
TreatmentsTreatments not highly desired by patients
Relton C et al. BMJ 2010;340:c1066