Update of radiosurgery at the Royal AdelaideHospitalDE Roos,1 BP Brophy,2 MK Bhat3 and ES Katsilis4
Departments of 1Radiation Oncology, 2Neurosurgery, 3Medical Physics and 4Radiation Therapy, Royal Adelaide Hospital, Adelaide,
South Australia, Australia
SUMMARY
This is an update of the Royal Adelaide Hospital radiosurgery experience between November 1993 and December
2004 comprising 165 patients with 168 intracranial lesions. Including re-treatment, there were 175 treatment epi-
sodes (163 radiosurgery and 12 stereotactic radiotherapy) at an average of 1.3 per month. The commonest lesions
were acoustic neuroma (65), arteriovenous malformation (58), solitary brain metastasis (23) and meningioma (14).
The clinical features, treatment details and outcome are described. Our results continue to be well within the
range reported in the published work. Radiosurgery provides an elegant, non-invasive alternative to neurosurgery
and conventional external beam radiotherapy for many benign and malignant brain tumours.
Key words: brain; linac; radiosurgery; stereotactic radiotherapy.
INTRODUCTION
Radiosurgery (RS) is the use of single large doses of highly
focused ionizing radiation to treat small lesions localized by
stereotactic technology. All nine Australasian units are linac
based (there are no gamma knife or charged particle acceler-
ator systems at the time of writing). The Royal Adelaide Hos-
pital (RAH) commenced RS in 1993 using a German-designed
Fischer–Leibinger system (now Stryker–Leibinger), the only one
of its type in Australasia. Treatment has been restricted to
intracranial pathology, although RS is now commonly used
elsewhere for head and neck, and trunk tumours. Because of
resource constraints, fractionated RS, so-called stereotactic
radiotherapy (SRT), only commenced at the RAH in 2001.
An audit of our results for the first 65 treated lesions and a
subsequent update of 16 solitary brain metastasis patients
both confirmed outcomes consistent with those reported in
the published work to that time.1,2
The purpose of the current study is to review the overall
RAH RS/SRT experience up to December 2004. Data at pre-
sentation and follow up were prospectively gathered in our
weekly RS clinic, supplemented where necessary by phone or
written contact with the patients and their referring specialist or
general practitioner.
MATERIALS AND METHODS
Radiosurgery was initially carried out on a Siemens KD2 linac
(Siemens Medical Systems, Concord, CA, USA), but from
1998, a Varian 6/100 linac (Varian Medical Systems, Palo Alto,
CA, USA) was used. The procedure is as previously described.1
Briefly, the patient is admitted to the neurosurgical ward on the
morning of RS for fixation of the stereotactic head ring, followed
by angiography (for arteriovenous malformations (AVM) only)
and CT imaging of the brain for computer planning (all patients).
If MRI is required, this is usually arranged the preceding week,
with CT–MRI fusion carried out on the day of RS. Computer
planning is completed by late morning, and treatment takes
place mid to late afternoon (for logistics reasons) after which
the head ring is removed. Patients are generally observed over-
night, with discharge the following morning. Although not
essential for RS, inpatient management is convenient in view
DE Roos BSc(Hons), MD, FRANZCR; BP Brophy FRACS; MK Bhat MSc, M App Sc, Dip Rad Phys; ES Katsilis MIR.
Correspondence: Dr Daniel E Roos, Department of Radiation Oncology, Royal Adelaide Hospital, North Terrace, Adelaide, SA 5000, Australia.
Email: [email protected]
Submitted 9 February 2005; accepted 24 November 2005.
doi: 10.1111/j.1440-1673.2006.01560.x
RadiationOncology Australasian Radiology (2006) 50, 158–167
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists

of the above scheduling. For patients having SRT, a relocatable
rigid fibreglass head cast is constructed during the preceding
week and treatment is on an outpatient basis.
The default beam arrangement is six equally dose-weighted,
non-coplanar arcs per isocentre using 140� gantry rotation per
arc and equal angular separation (30�) between the arcs. This
produces a spherical dose distribution that can be modified by
omitting arcs, varying their separation, gantry rotation or dose
weighting to conform to the lesion contour. Sometimes, a com-
bination of circular collimator sizes is used. The available colli-
mators have 80% isodose curve diameters at isocentre ranging
from 4 to 55 mm. Irregular lesions may require the use of more
than one isocentre, which can have different collimator sizes
and different dose weightings to optimize conformity. We do not
currently have the option of micromultileaf collimation.
Between November 1993 and December 2004, 165 patients
with 168 lesions were treated. Six AVM and one brain meta-
stasis required re-treatment. Hence, there were 175 treatment
episodes (RS 163 and SRT 12) at an average of 1.3 per month.
Table 1 summarizes the clinical characteristics and treat-
ment details for the four commonest tumour types. Follow-up
data extends to September 2005.
Acoustic neuroma
There were four patients with bilateral acoustic neuroma (AN)
due to neurofibromatosis type 2 (NF2). Their median age was
28 years (range 19–40 years), characteristically younger than
the 61 unilateral (sporadic) cases (median 62 years, range
21–81 years). Six of the sporadic cases had RS for recurrence
after surgery that was carried out a median of 11.5 years pre-
viously (range 2.5–32 years). Two of these recurrences were
detected on follow-up imaging, the other four were symptom-
atic. Three of the 59 de novo tumours were picked up inci-
dentally on scans carried out for other reasons; the commonest
symptoms for the other 56 were hearing loss (51 patients),
tinnitus (46), disequilibrium (34) and trigeminal neuropathy
(eight).
Of interest, for the sporadic cases, there was an excess
of left-sided lesions (39:22 = 1.77). This difference was statis-
tically significant (P = 0.04).
Follow-up MRI and audiometry were carried out at
12 months, yearly for 2–3 years, then two yearly thereafter
unless there were clinical indications to vary this schedule.
Maximum dimensions mediolaterally (including contrast-
enhancing extension into the internal auditory meatus), antero-
posteriorly (usually obliquely) and superoinferiorly were
recorded. Because of the difficulties inherent in measurements
from sequential imaging (e.g. interpolation from the centimetre
scale; variable slice width and angulation on successive scans),
sustained changes �2 mm were deemed significant.
Arteriovenous malformation
Each of the 56 patients had solitary AVM except a 13-year-
old woman with Rendu–Osler–Weber disease (familial haemor-
rhagic telangiectasia) and a 43-year-old man, both of whom had
RS for two AVM. Five patients had prior treatment elsewhere
Table 1. Summary of the clinical features and treatment details for the four commonest tumour types
Acoustic neuroma Arteriovenous malformation Metastasis Meningioma
No. patients 65 56 22 14
No. lesions treated 65 58 23 14
No. treatments 65 64 24 14
Age (years)
Range 19–81 5–69 36–83 14–75
Median 61 36.5 64 47.5
Male:female 38:27 24:32 12:10 5:9
Largest diameter (mm)
Range 11–40 5–70 3–34 17–35
Median 22 23 19 24.5
Site Left = 39† Cerebral hemisphere = 42 Cerebral hemisphere = 20 Base of skull = 10
Right = 22† Thalamocapsular = 7 Thalamus = 1 Tentorial = 1
Cerebellum = 5 Cerebellum = 1 Parasagittal = 1
Brainstem = 2 Brainstem = 1 Optic nerve sheath = 1
Basal ganglia = 2 Lateral ventricle = 1
Marginal dose (Gy), RS cases only
Range 12–14 12–23 15–23 14–18
Median 12 18 19 15
Isocentres (1:2:3) 54:11:0 55:9:0 22:2:0 11:2:1
Prescription isodose curve (%)‡
Range 70–90 70–90 60–90 70–90
Median 85 80 75 80
†Sporadic (unilateral) cases only (n = 61). ‡Single isocentre technique only. RS, radiosurgery.
RAH RADIOSURGERY UPDATE 159
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists

(embolization plus RS, two; conventional external beam radio-
therapy (RT) plus gamma knife, one; RS alone, one and partial
excision, one). Eleven AVM were discovered incidentally on
imaging (six at the time of intracranial haemorrhage from other
lesions). The commonest presentations otherwise were haem-
orrhage from the AVM (19 patients), seizures (15), headache
(10) and neurological deficit (six); some patients had a com-
bination of these features.
Eight paediatric patients (age 5–15 years) required a gen-
eral anaesthetic lasting 5.5–12 h (median 9 h) for planning and
treatment.
Seven of the biggest lesions (40–60 mm) were treated with
SRT (30 Gy in 5 or 6 fractions); one other patient with a 70-mm
AVM was offered ‘volume fractionation’ but failed to attend after
two of the three components had been treated.
Our policy was to monitor AVM regression with 12 monthly
MRI. Angiography was carried out as the gold standard to con-
firm apparent obliteration on MRI, or in any case at approxi-
mately 3 years (this being the time when re-treatment needs
to be considered in the event of nonobliteration because of the
continuing risk of haemorrhage).
Metastasis
Details for the first 16 patients have been previously de-
scribed.1,2 Six more have been treated subsequently, all with
MRI confirmed solitary (presumed) brain metastases. One
patient had RS for two metachronous lesions and another
had re-treatment of a brainstem metastasis at the time of symp-
tomatic recurrence. Thus, there were 24 RS treatments in all.
The commonest primaries were lung (12 patients) and mela-
noma (three), and the commonest presenting symptoms were
hemiparesis (10), headache (six) and visual field defect (five).
When classified by Radiation Therapy Oncology Group recur-
sive partitioning analysis (RPA) prognostic class (based upon
Karnofsky performance status, age and extracranial disease
status),3 four patients were in class 1, 16 in class 2 and two in
class 3.
Two patients had RS 12 and 31 months following excision
plus whole-brain radiotherapy (WBRT) for solitary brain meta-
stases at a different site. Of the other 20 patients, eight had
adjuvant WBRT (30 Gy in 10 or 36 Gy in 18 fractions) at the
time of the RS, two had subsequent WBRT for distant brain
relapse and one had focal (conventional) brain RT for local
relapse. The other nine patients (41%) did not receive conven-
tional brain RT in their remaining lifespan.
Meningioma
One meningioma was discovered incidentally on brain MRI car-
ried out for other reasons. Presenting symptoms for the other
13 patients were cranial neuropathy (10 patients), headache/
pain (five) and seizures (one). Ten patients had no prior treat-
ment, two had adjuvant RS after surgical debulking and two had
RS on progression 6 and 5 years after surgery (the latter also
had repeat surgery and conventional RT 3 years before the
RS). Nine patients had RS and the other five SRT (30 Gy in 6
fractions to 52.2 Gy in 29 fractions).
Miscellaneous
The clinical features and treatment details for eight patients with
various other lesions are summarized in Table 2.
RESULTS
Non-specific acute side-effects
The majority of patients experienced no acute side-effects.
Vomiting was recorded for six patients only (3.6%). In some
cases, analgesia and/or anaesthesia may have contributed.
This low incidence may reflect our policy of routine premedica-
tion with dexamethasone 8 mg i.v. and metoclopramide 10 mg
i.v. A few patients developed minor toxicity related to the head
ring pins (haematoma, infection, transient focal scalp tingling or
numbness). Many showed temporary 1- to 1.5-cm patches of
alopecia at the two posterior pin sites, thought to be due to
pressure ischaemia of the adjacent hair follicles. This was of
no cosmetic consequence as it was obscured by surrounding
hair. Reversible circular or ellipsoidal alopecia also developed
predictably in the case of subcranial lesions because of un-
avoidable irradiation of the overlying scalp. Several patients
reported lethargy for a week or two after the RS. One patient
with a medullopontine AVM developed facial flushing and fever
(38–39�C) the morning after RS. There was no obvious infec-
tion, and the symptoms settled conservatively.
Treatment outcome and site-specific side-effects are as
follows.
Acoustic neuroma
One patient died at 5 months from an unrelated cause and two
others await their first follow-up scan and audiometry at the time
of writing, leaving 62 evaluable patients.
A transient increase in tumour size associated with central
necrosis was observed in nine patients (16%) at a median of
12 months from RS (range 4–25 months). This typically per-
sisted for 1–2 years. The median increase was 4 mm (range
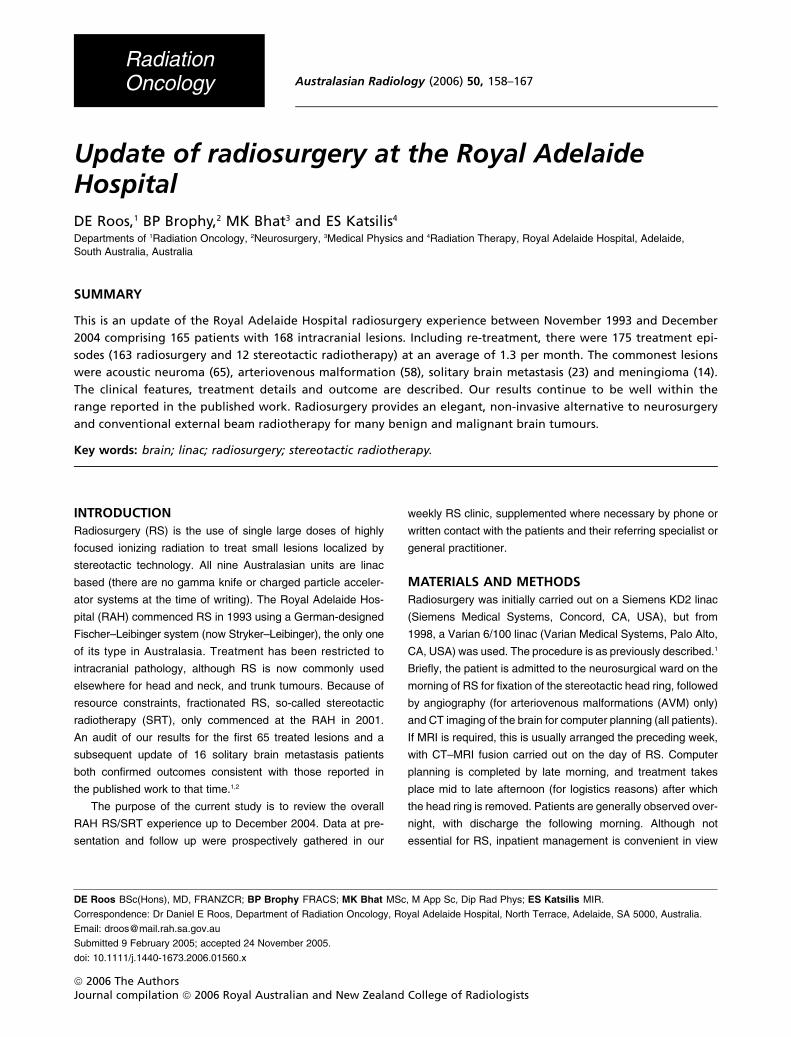
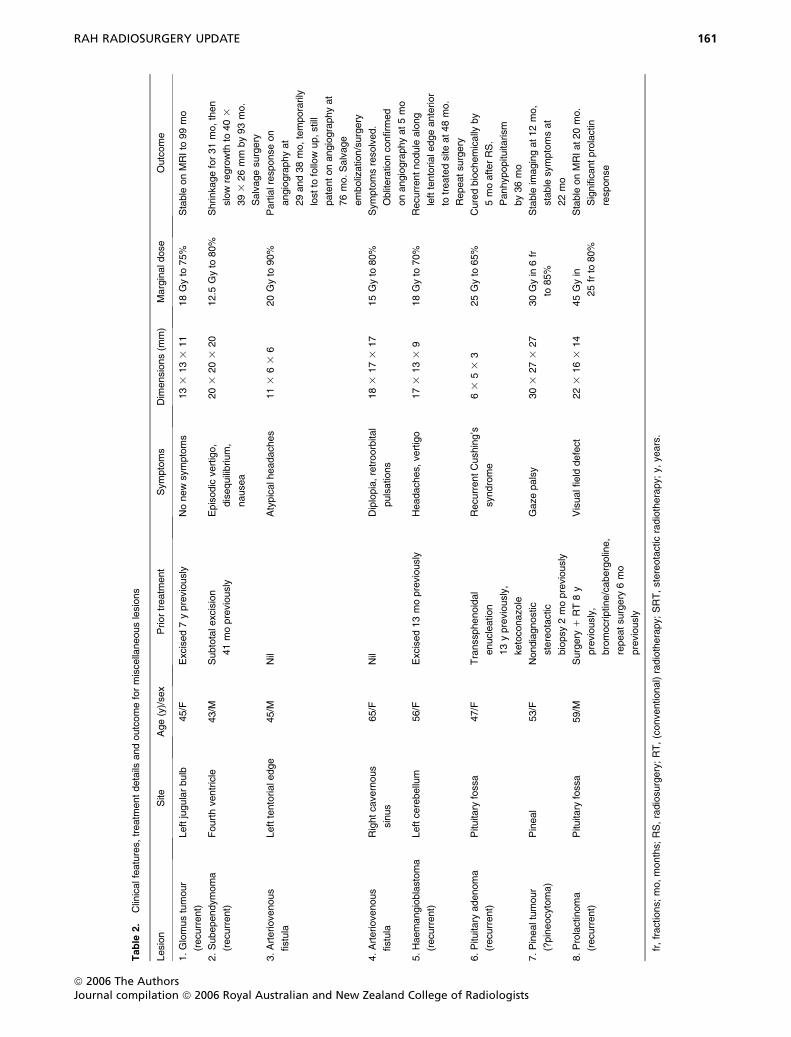
2–5 mm) (Fig. 1b).
Tumour control (defined as stable or reduced dimensions
on follow-up imaging relative to baseline) was achieved in 59 of
the 62 evaluable patients (95%) over a median observation
period of 48 months (range 12–134 months). Seventeen tumours
were stable over 12–85 months; 42 decreased by 2–12 mm
(median 4 mm) over 13–134 months (Fig. 1c). One of the three
patients whose tumour progressed had palliative RS to part
of a recurrent multicystic AN excised 32 years previously. The
cystic component increased at 26 months after RS, associated
with further distortion of the brainstem, but this has not required
surgical intervention after a further 7 years. The second had
160 DE ROOS ET AL.
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists
Table
2.
Clinicalfeatures,treatm
entdetails
andoutcomeformiscellaneouslesions
Lesion
Site
Age(y)/sex
Priortreatm
ent
Symptoms
Dim
ensions(m
m)
Marginaldose
Outcome
1.Glomustumour
(recurrent)
Leftjugularbulb
45/F
Excised7ypreviously
Nonewsymptoms
133
133
11
18Gyto
75%
Stable
onMRIto
99mo
2.Subependymoma
(recurrent)
Fourthventricle
43/M
Subtotalexcision
41mopreviously
Episodic
vertigo,
disequilibrium,
nausea
203
203
20
12.5
Gyto
80%
Shrinkagefor31mo,then
slowregrowth
to403
393
26mm
by93mo.
Salvagesurgery
3.Arteriovenous
fistula
Lefttentorialedge
45/M
Nil
Atypicalheadaches
113
63
620Gyto
90%
Partialresponseon
angiographyat
29and38mo,temporarily
lostto
follow
up,still
patentonangiographyat
76mo.Salvage
embolization/surgery
4.Arteriovenous
fistula
Rightcavernous
sinus
65/F
Nil
Diplopia,retroorbital
pulsations
183
173
17
15Gyto
80%
Symptomsresolved.
Obliterationconfirm
ed
onangiographyat5mo
5.Haemangioblastoma
(recurrent)
Leftcerebellum
56/F
Excised13mopreviously
Headaches,vertigo
173
133
918Gyto
70%
Recurrentnodule
along
lefttentorialedgeanterior
totreatedsiteat48mo.
Repeatsurgery
6.Pituitary
adenoma
(recurrent)
Pituitary
fossa
47/F
Transsphenoidal
enucleation
13ypreviously,
ketoconazole
RecurrentCushing’s
syndrome
63
53
325Gyto
65%
Curedbiochemically
by
5moafterRS.
Panhypopituitarism
by36mo
7.Pinealtumour
(?pineocytoma)
Pineal
53/F
Nondiagnostic
stereotactic
biopsy2mopreviously
Gazepalsy
303
273
27
30Gyin
6fr
to85%
Stable
imagingat12mo,
stable
symptomsat
22mo
8.Prolactinoma
(recurrent)
Pituitary
fossa
59/M
Surgery
1RT8y
previously,
bromocriptine/cabergoline,
repeatsurgery
6mo
previously
Visualfield
defect
223
163
14
45Gyin
25frto
80%
Stable
onMRIat20mo.
Significantprolactin
response
fr,fractions;mo,months;RS,radiosurgery;RT,(conventional)radiotherapy;SRT,stereotacticradiotherapy;y,years.
RAH RADIOSURGERY UPDATE 161
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists
salvage RS for recurrence 4.5 years after excision but developed
symptomatic progression 2 years following the RS. Pathology
at reoperation confirmed (benign) AN. The third patient’s
tumour was stable for 3 years after primary RS but increased
by 2–3 mm over the next 3 years without new symptoms. This
appears to be a delayed recurrence but further follow up will be
needed for confirmation. The current rate of freedom from sur-
gical salvage for patients treated with primary RS is thus 100%
and for the whole series 64/65 (98.5%).
With respect to hearing outcome, two of the four NF2
patients were functionally deaf before RS. The other two had
some hearing on the treated side but lost this by 2 months
Fig. 1. Coronal MRI images showing an enhancing left acoustic neuroma. (a) Before radiosurgery with pre-existing ventriculomegaly. (b) At
11 months, central necrosis associated with transient 3-mm enlargement. (c) At 24 months, progressive hydrocephalus requiring elective shunting.
(d) At 45 months, 5-mm shrinkage with resolution of the hydrocephalus.
162 DE ROOS ET AL.
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists

(14 Gy) and 8 months (12 Gy). All six of the patients with post-
operative recurrences were deaf on that side. Of the other 55
(sporadic) cases, 19 (35%) had no useful ipsilateral hearing at
presentation (defined as pure tone average .50 dB or patient
report to that effect where audiometry was borderline). At the
time of writing, two of the 36 patients with initially useful hearing
await first follow-up audiogram. This leaves 34 assessable
patients, of whom 18 (53%) lost useful hearing by 8–77 months
(median 24 months), whereas 16 (47%) retained it over 20–
108 months (median 60 months) of follow up.
Nausea was reported by five patients after RS, lasting for
1.5–4 weeks. This was associated with vomiting in one patient
and vertigo requiring bedrest in another who developed a pul-
monary embolus at 2.5 weeks. Worsened disequilibrium also
occurred in five patients at 1, 2, 4, 5 and 7 months each requir-
ing temporary corticosteroids and brief admission for two of
them.
Mild/partial trigeminal neuropathies developed in seven
patients (two of whom also developed facial neuropathies).
Four of these were new (numbness, dysaesthesia or hyper-
aesthesia) at 4, 6, 12 and 20 months; the other three patients
developed trigeminal neuralgia in a distribution of pre-existing
numbness at 2, 6 and 41 months. Mild facial neuropathies
developed in four patients (facial weakness in three and
impaired ipsilateral taste in one). Three of these were new at
4, 6 and 7 months (one associated also with minor hemifacial
spasms reported at 42 months) and the other was transient
worsening of pre-existing facial nerve weakness at 4 months.
Significantly, when considered together, these V and VII neu-
ropathies affected four of eight patients (50%) receiving 14 Gy
but affected only five of the 57 patients (9%) receiving 12 Gy.
Ventriculoperitoneal shunting for hydrocephalus was re-
quired in three patients at 5, 6 and 27 months. However, in
two of these, ventriculomegaly preceded treatment and it is
unclear whether RS contributed to the natural history of this
known complication of untreated AN (Fig. 1c). The rate of de
novo hydrocephalus after RS was thus 1/63 (1.6%).
No second tumour has occurred at the treated site, but six
patients so far have developed distant neoplasms 6–56 months
after the RS, three fatal, namely contralateral parietal glio-
blastoma multiforme, contralateral suprasellar meningioma,
squamous cell carcinoma (SCC) of the lung, uterine leiomyo-
sarcoma, disseminated adenocarcinoma (unknown primary)
and ipsilateral metastatic parotid SCC (skin primary). None of
these would satisfy the criteria for radiation-induced tumours.
Arteriovenous malformation
Of the five previously treated AVM, angiography confirmed
obliteration in three at 27, 31 and 57 months (the latter patient
failing to pursue earlier angiography); one poorly compliant
patient had a persistent diffuse vascular abnormality at
6.5 years but declined selective angiogram and further follow
up thereafter; the other has had a partial response on MRI after
2 years.
Fifty-three AVM were treated with primary RS (47) or SRT
(six). Six patients failed to continue follow up or declined con-
firmatory angiography, and 13 patients await 3-year angio-
graphy at the time of writing, leaving 34 assessable AVM.
Obliteration without any further treatment was confirmed in 25
of these (74%) at 12–56 months (median 26 months). Five
of the partially obliterated AVM went on to have repeat RS or
SRT at a median of 40 months after initial treatment (range 37–
47 months). Subsequent obliteration has so far been confirmed
in one of these 19 months after re-treatment; another had inde-
terminate angiograms (stable dysplastic vessels without early
draining vein) at 14, 25 and 36 months after re-treatment
(coded conservatively as nonobliteration). Hence, the crude
‘cure’ rate with primary RS/SRT (one or two treatments) stands
at 26/34 (76%). Two partially obliterated AVM required surgery,
one for haemorrhage at 36 months and the other for radionec-
rosis at 63 months.
There were three complications of angiography (haemor-
rhage at groin puncture site, presumed femoral artery throm-
bosis and vertebral artery occlusion), each of which resolved
conservatively without sequelae.
Two patients, both of whom were already on anticonvul-
sants for grand mal epilepsy, had partial seizures within a few
days of the RS, whereas a third had increased frequency and
severity of pre-existing hemisensory seizures during the first
few weeks after RS; one patient had a first generalized seizure
at 2 months, with, in retrospect, a history of partial seizures for
7–8 years before the RS; another developed complex partial
seizures from about 6 months, which subsequently became
intractable (related to radionecrosis) but had initially presented
with temporal lobe haemorrhage associated with one grand mal
and several focal seizures. Thus, there has been no case of
post-RS seizures developing in the absence of a history of
seizure disorder.
Six patients required dexamethasone for 1–4 months be-
cause of symptomatic oedema around the AVM at a median
of 6.5 months (range 6–20 months) after RS. Of interest, four of
these had been treated with a two isocentre technique (which
is associated with higher central dose). Two patients with
large, deeply seated AVM (left thalamic 47 mm, right basal
ganglia 60 mm) developed progressive hemiparesis from about
6 months after SRT but have been able to continue working
2–3 years later. One paediatric patient with a midbrain/thalamic
AVM required shunting for hydrocephalus at 21 months, al-
though it is unclear whether this was a complication of the RS.
Two patients (4%) have had nonfatal haemorrhages at the
site of the treated AVM, one at 36 months (mentioned above),
the other 9 years after initial RS elsewhere, and 58 and
59 months after repeat RS despite angiographically confirmed
obliteration at 57 months.
RAH RADIOSURGERY UPDATE 163
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists
Metastasis
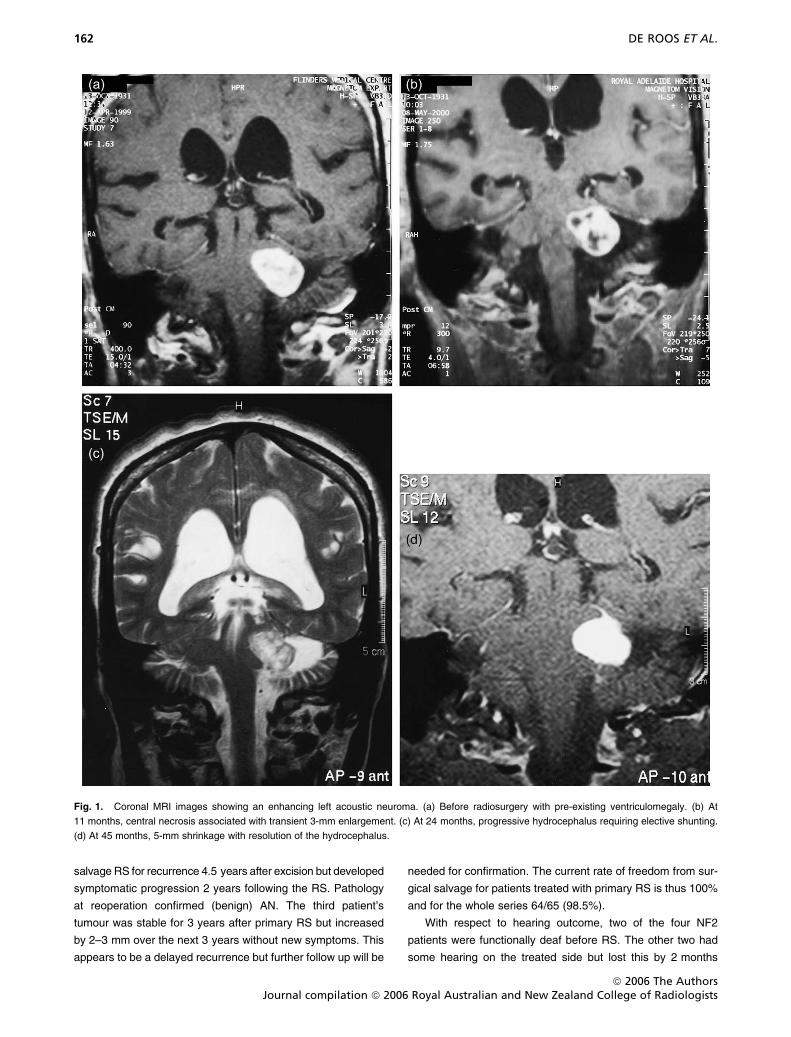
The estimated median survival from RS for the 22 patients was
10.1 months (95% CI 2.4–34.7 months), with the estimated
2-year survival being 35% (95% CI 18–58%). The actuarial
overall survival curve is shown in Figure 2a, and by RPA class
in Figure 2b. Despite the small number of patients, there was
a statistically significant difference in survival by RPA class
(P = 0.013, log–rank test). As far as could be determined, the
cause of death for the 17 deceased patients was central
nervous system disease (seven), systemic disease (five) and
both (five).
Meningioma
Thirteen of the 14 patients have had at least one MRI scan to
assess response. At a median radiologic follow up of 36 months
(range 7–123 months), six lesions have regressed (median
shrinkage 5.5 mm, range 2–10 mm), six have remained stable
and one has progressed. The latter patient had two operations
and conventional external beam RT for a parietal meningioma
within 5 years before the RS, which was given with palliative
intent to the solid component of a mixed cystic/solid recurrence.
He required further surgery after 9 months, pathology confirm-
ing transformation to atypical meningioma and he died at
19 months because of complications from his tumour. Another
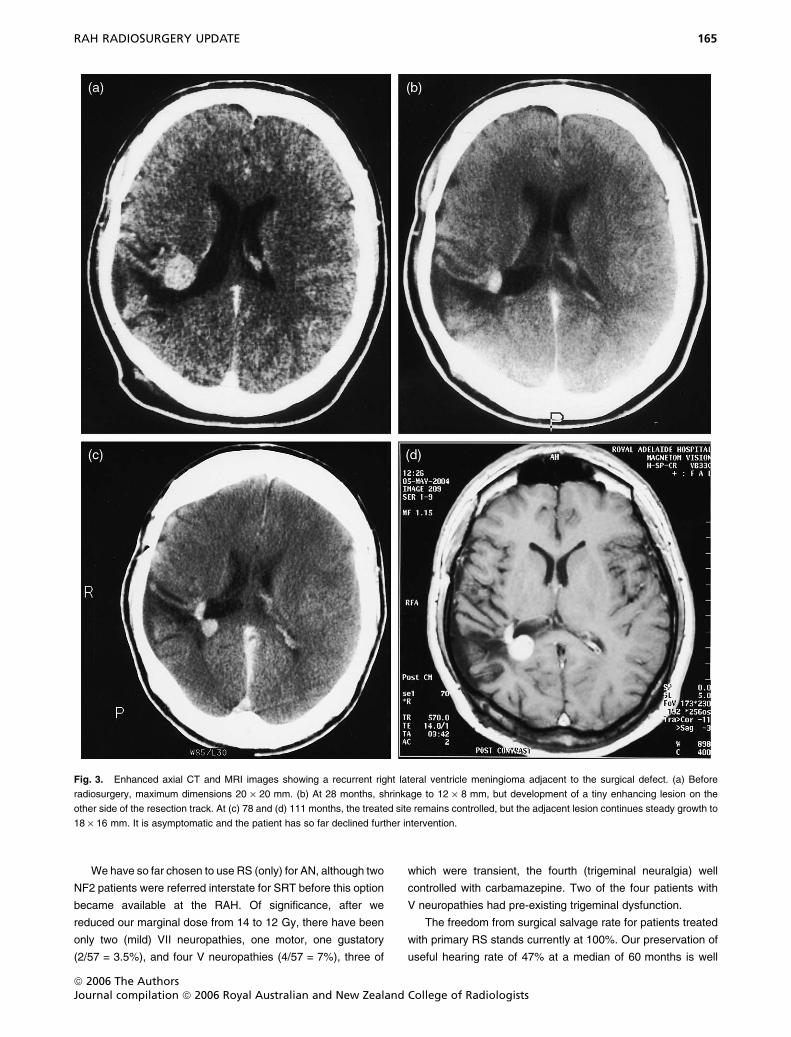
patient who had RS for a recurrent lateral ventricle meningioma
excised 5 years previously developed a new site of disease
on the other side of the resection track (outside the high dose
region) at 28 months. He is asymptomatic at 10 years, but
although the treated site remains controlled, the new lesion
continues to grow (Fig. 3).
Five patients developed side-effects attributable to the treat-
ment: transient worsening of ipsilateral facial paraesthesiae
from a cavernous sinus meningioma at 18 months; partial
ipsilateral VI nerve palsy from a petroclival meningioma at
14 months (corrective eye surgery had to be revised subse-
quently because of recovery); transient contralateral hemisen-
sory loss from a parietal meningioma at 6 months; decreased
visual acuity during SRT for an optic nerve sheath meningioma
resolving with steroids, subsequent intermittent steroids for epi-
sodes of visual blurring and orbital pain; worsening ipsilateral
trigeminal neuralgia from a cerebellopontine angle meningioma
at 3 months resolving with steroids. These cases presumably
reflect temporary oedema due to the radiation.
Miscellaneous
Outcomes for the remaining eight patients are shown in
Table 2. Two patients with lesions within or adjacent to the
brainstem (cases 2 and 5) required dexamethasone because
of transient oedema following RS, but subsequently recovered
to pretreatment level of functioning. At the time of writing, five of
these lesions remain controlled with RS.
DISCUSSION
Acoustic neuroma
The optimal management of small to moderate-sized AN
(�3 cm) is controversial because of the absence of randomized
trials. Radiosurgery is certainly a viable alternative to micro-
surgery, but debate continues in the published work about the
relative merits of RS versus SRT, with a wide range of fraction-
ation schedules reported for the latter (20 Gy in 4–5 fractions up
to 45–59.4 Gy in 25–33 fractions).4,5 Tumour control rates are
similar with all three treatment options (.90–95%), and the
unacceptably high incidence of V and VII neuropathies reported
in early RS series has greatly improved as doses have progres-
sively decreased to ,14 Gy.6 Hearing preservation rates vary
enormously between series reflecting differing selection factors
(age, tumour size, degree of loss pretreatment), length of follow
up and definitions of ‘useful’ hearing.
0
20
40
60
80
100(a)
(b)
0 1 2 3 4 5 6 7
Number at risk
0 1 2 3 4 5 6 7
Number at risk
22 9 6 3 2 2 1 0
0
20
40
60
80
100
4162
441
420
300
200
200
100
000
Class 1Class 2Class 3
P = 0.013
Fig. 2. Actuarial survival curves for the 22 solitary brain metastases
patients treated with radiosurgery: (a) overall and (b) by recursive par-
titioning analysis class. ( ), RPA class 1; ( ), RPA class 2; ( ),
RPA class 3.
164 DE ROOS ET AL.
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists
We have so far chosen to use RS (only) for AN, although two
NF2 patients were referred interstate for SRT before this option
became available at the RAH. Of significance, after we
reduced our marginal dose from 14 to 12 Gy, there have been
only two (mild) VII neuropathies, one motor, one gustatory
(2/57 = 3.5%), and four V neuropathies (4/57 = 7%), three of
which were transient, the fourth (trigeminal neuralgia) well
controlled with carbamazepine. Two of the four patients with
V neuropathies had pre-existing trigeminal dysfunction.
The freedom from surgical salvage rate for patients treated
with primary RS stands currently at 100%. Our preservation of
useful hearing rate of 47% at a median of 60 months is well
Fig. 3. Enhanced axial CT and MRI images showing a recurrent right lateral ventricle meningioma adjacent to the surgical defect. (a) Before
radiosurgery, maximum dimensions 20 · 20 mm. (b) At 28 months, shrinkage to 12 · 8 mm, but development of a tiny enhancing lesion on the
other side of the resection track. At (c) 78 and (d) 111 months, the treated site remains controlled, but the adjacent lesion continues steady growth to
18 · 16 mm. It is asymptomatic and the patient has so far declined further intervention.
RAH RADIOSURGERY UPDATE 165
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists

within the 33–81% range found in the major RS and SRT
series.4 Three out of the 65 patients (4.6%) required shunting
for hydrocephalus after RS, but two of these had pre-existing
ventriculomegaly (de novo hydrocephalus rate 1/63 = 1.6%).
These figures are similar to the 2–3% shunting rate typically
reported.6
It is interesting to speculate whether the previously noted
excess of left-sided sporadic lesions (P = 0.04) may be associ-
ated with mobile phone use, either causally or by unmasking
early hearing loss preferentially on that side. Recent Swedish
data showed an increased risk of AN on the side where the
phone is usually held (but not on the other side) after 10 or more
years of analogue mobile phone use. However, in that study,
the excess of tumours and phone use was on the right,7 and in
the context of many previous negative population studies, the
association remains highly uncertain.8 We do not have prospec-
tive data on mobile phone behaviour for our patients, and the
observed left-sided dominance may simply be because of
chance.
Arteriovenous malformation
Similar to the situation with AN, there are no randomized trials
comparing surgery with RS (with or without embolization) for
AVM. Surgery offers the possibility of immediate cure, whereas
obliteration after RS can take 2–3 years, during which time the
risk of haemorrhage persists. Incomplete obliteration requires
further treatment in order to eliminate this risk. However, RS
may be the only option for deep-seated (inoperable) lesions,
and where patients decline surgery or are medically inoperable.
Obliteration rates are typically in the range of 60–90%, and
are a function of marginal dose rather than AVM size per se.9
Large (.3–4 cm) AVM can be treated with (hypofractionated)
SRT10 or ‘staged-volume’ RS where components of the AVM
are sequentially treated with single fractions several months
apart.11
Our overall obliteration rate for assessable patients treated
with primary RS is 76%. Evaluation of the efficacy of our SRT
fractionation is pending as only one of the seven patients has
had follow-up angiography at the time of writing.
Haemorrhage after RS is reported to occur at an annual rate
of 3–4% per year until obliteration, with no statistical alteration
from the natural history of untreated AVM. This typically trans-
lates to an approximately 5% bleeding risk.12 However, there
are case reports of haemorrhage after angiographic obliteration
thought to be because of recanalization of thrombi that have not
evolved to stable scar tissue at the time of the angiogram.13 So
far, two of our patients (3.6%) have had nonfatal bleeds after
RS, one following angiographic obliteration.
Metastasis
The management issues have been addressed previously.2
In brief, there is randomized evidence of survival benefit for
the addition of surgery or RS to WBRT alone, at least for good
prognosis patients with solitary brain metastases. The addition
of WBRT to surgery or RS improves local and distant brain
control, but does not increase survival. There have been no pub-
lished randomized trials directly comparing surgery with RS
(one is in progress at the RAH), although nonrandomized data
suggest similar efficacy but superior cost effectiveness for RS.
We have restricted RS to patients with solitary brain meta-
stases and generally to RPA class 1 or 2 (two class 3 patients
were treated on the above-mentioned randomized trial). The
overall median survival of 10.1 months is typical of recent multi-
institutional reviews.14 Our results also illustrate the prognostic
validity of the RPA concept.3
Meningioma
The role of radiation in any form for benign meningioma is con-
troversial, particularly the issue of timing in the postoperative
setting. Radiosurgery and SRT are no exception to this ob-
servation.15 Accordingly, our indications are broad, including
primary treatment of inoperable lesions (e.g. cavernous sinus,
optic nerve sheath), adjuvant treatment after debulking surgery
where symptomatic progression is likely (e.g. young patient with
base of skull meningioma), or for postoperative recurrence
as an alternative to repeat surgery. Stereotactic radiotherapy
is favoured for large meningiomas (.3–3.5 cm) or because
of proximity to sensitive structures (e.g. optic pathway,
brainstem).16
Control rates of more than 90% are usually reported with
stereotactic radiation techniques.17 However, prolonged fol-
low up (10–20 years) is required for a true indication of tumour
control, so our 100% rate for the 12 assessable lesions trea-
ted with ‘curative’ intent with a median radiological follow up
of 36 months must be regarded as very preliminary. The rate
is 92% if the adjacent recurrence discussed above is counted
as a marginal failure. This case illustrates a disadvantage of
RS relative to conventional RT, namely the risk that highly
focused radiation may inadequately treat nearby microscopic
disease.
Complication rates are a function of tumour volume, dose
and location. Each of the five cases of (probable) treatment-
related toxicity described above were transient and/or episodic.
In only two patients were these symptoms new.
CONCLUSION
Radiosurgery and SRT provide elegant non-invasive alterna-
tives to microsurgery for many benign and malignant intra-
cranial tumours. Our more mature follow-up data confirm
outcomes that continue to be well within the range reported in
the world literature. Subject to provision of the necessary fund-
ing, we are planning to upgrade the current system to one
based upon micromultileaf collimation and including the option
166 DE ROOS ET AL.
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists

of recent advances in stereotactic radiation techniques, namely
intensity-modulated stereotactic RS.
ACKNOWLEDGEMENTS
The support of the Royal Adelaide Hospital physics, radi-
ation therapy, radiology and nursing staff are all gratefully
acknowledged. Many thanks to Dr Jennifer Smith for statistical
analysis of the brain metastasis outcomes.
REFERENCES1. Roos DE, Brophy BP, Zavgorodni SF, Francis JW. Radiosurgery
at the Royal Adelaide Hospital: the first 4½ years’ clinical experi-
ence. Australas Radiol 2000; 44: 185–92.
2. Roos DE, Brophy BP, Zavgorodni SF, Katsilis ES. Radiosurgery
for brain metastases at the Royal Adelaide Hospital: are we treat-
ing the right patients? Australas Radiol 2002; 46: 402–8.
3. Gaspar L, Scott C, Rotman M et al. Recursive partitioning analysis
(RPA) of prognostic factors in three Radiation Therapy Oncology
Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol
Phys 1997; 37: 745–51.
4. De Salles AAF, Frighetto L, Selch M. Stereotactic and microsur-
gery for acoustic neuroma: the controversy continues (Editorial).
Int J Radiat Oncol Biol Phys 2003; 56: 1215–17.
5. Flickinger JC. What is the optimal dose and fractionation for ste-
reotactic irradiation of acoustic neuromas? (Editorial). Int J Radiat
Oncol Biol Phys 2002; 54: 311–12.
6. Lunsford LD, Kondziolka D, Flickinger JC, Bissonette D, Maitz A.
Acoustic neuroma management: evolution and revolution. In:
Kondiolka D (ed.). Radiosurgery 1997, Vol. 2. Karger, Basel,
Switzerland, 1998; 1–7.
7. Lonn S, Ahlbom A, Hall P, Feychting M. Mobile phone use and the
risk of acoustic neuroma. Epidemiology 2004; 15: 653–9.
8. Savitz DA. Mixed signals on cell phones and cancer (Commen-
tary). Epidemiology 2004; 15: 651–2.
9. Flickinger JC, Kondziolka D, Maitz AH, Lunsford LD. An analysis of
the dose-response for arteriovenous malformation radiosurgery
and other factors affecting obliteration. Radiother Oncol 2002;
63: 347–54.
10. Aoyama H, Shirato H, Nishioka T et al. Treatment outcome of
single or hypofractionated single-isocentric stereotactic irradiation
(STI) using a linear accelerator for intracranial arteriovenous mal-
formation. Radiother Oncol 2001; 59: 323–8.
11. Pollock BE, Kline RW, Stafford SL, Fooke RL, Schomberg PJ. The
rationale and technique of staged-volume arteriovenous malforma-
tion radiosurgery. Int J Radiat Oncol Biol Phys 2000; 48: 817–24.
12. Friedman WA. Radiosurgery for arteriovenous malformations. In:
Kondziolka D (ed.). Radiosurgery, Vol. 4. Karger, Basel, Switzer-
land, 2002; 12–18.
13. Szeifert GT, Vandersmissen B, Taib NOB et al. Recurrent haemor-
rhage in a radiosurgically obliterated cerebral arteriovenous mal-
formation. In: Kondziolka D (ed.). Radiosurgery, Vol. 4. Karger,
Basel, Switzerland, 2002; 34–41.
14. Sanghavi SN, Saranarendra SM, Chappell R et al. Radiosurgery
for patients with brain metastases: a multi-institutional analysis,
stratified by the RTOG recursive partitioning analysis method. Int
J Radiat Oncol Biol Phys 2001; 51: 426–34.
15. Mirimanoff R-O. New radiotherapy technologies for meningiomas:
3D conformal radiotherapy? Radiosurgery? Stereotactic radiother-
apy? Intensity-modulated radiotherapy? Proton beam radiother-
apy? Spot scanning proton radiation therapy . or nothing at all?
Radiother Oncol 2004; 71: 247–9.
16. Milker-Zabel S, Zabel A, Schulz-Ertner D, Schlegel W, Wannen-
macher M, Debus J. Fractionated stereotactic radiotherapy in
patients with benign or atypical intracranial meningioma: long-term
experience and prognostic factors. Int J Radiat Oncol Biol Phys
2005; 61: 809–16.
17. Torres RC, De Salles AAF, Frighetto L et al. Long-term follow-up
using linac radiosurgery and stereotactic radiotherapy as aminimally
invasive treatment for intracranial meningiomas. In: Kondziolka D
(ed.). Radiosurgery, Vol. 5. Karger, Basel, Switzerland, 2004;
115–23.
ª 2006 The AuthorsJournal compilation ª 2006 Royal Australian and New Zealand College of Radiologists
RAH RADIOSURGERY UPDATE 167
Recommended

















