Is integrated nursing home care cheaper than traditional care?A cost comparison
Aggie T.G. Paulus *, Arno J.A. van Raak 1, Hans J.A.M. Maarse 2
Care and Public Health Research Institute (CAPHRI), Faculty of Health, Medicine and Life Sciences,
Maastricht University, Department of Health Organization, Policy and Economics (HOPE),
P.O. Box 616, 6200 MD Maastricht, The Netherlands
Received 21 June 2007; received in revised form 23 April 2008; accepted 22 May 2008
www.elsevier.com/ijns
Available online at www.sciencedirect.com
International Journal of Nursing Studies 45 (2008) 1764–1777
Abstract
Background: It is generally assumed that integrated care has a cost-saving potential in comparison with traditional care.
However, there is little evidence on this potential with respect to integrated nursing home care.
Aims and objectives: �To portray the costs of traditional and integrated nursing home care.�To explore the cost-saving potential
of integrated care.
Design/methods/settings/participants: Between 1999 and 2003, formal and informal caregivers of different nursing homes in
the Netherlands recorded activities performed for residents with somatic or psycho-social problems. In total, 23,380 lists were
analysed to determine the average costs of formal and informal care per activity, per type of resident and per nursing home care
type. For formal care activities, the total personnel costs per minute (in Euro) were calculated. For informal care costs, two
shadow prices were used.
Results: Compared to traditional care, integrated care had lower informal direct care costs per resident and per activity and
lower average costs per direct activity (for a set of activities performed by formal caregivers). The total average costs per resident
per day and the costs of formal direct care per resident, however, were higher as were the costs of delivering a set of indirect
activities to residents with somatic problems.
Conclusions: The general assumption that integrated care has a cost-saving potential (per resident or per individual activity)
was only partially supported by our research. Our study also raised issues which should be investigated in future research on
integrated nursing home care.
# 2008 Elsevier Ltd. All rights reserved.
Keywords: Costs; Formal care; Informal care; Integrated care; Nursing home care; Traditional care
* Corresponding author. Tel.: +31 43 3881706;
fax: +31 43 3670960.
E-mail addresses: [email protected] (A.T.G. Paulus),
[email protected] (A.J.A. van Raak),
[email protected] (H.J.A.M. Maarse).1 Tel.: +31 43 3881699; fax: +31 43 3670960.2 Tel.: +31 43 3881571; fax: +31 43 3670960.
0020-7489/$ – see front matter # 2008 Elsevier Ltd. All rights reserved
doi:10.1016/j.ijnurstu.2008.05.005
What is already known about the topic?
� I
.
t is generally assumed that integrated care (delivered by
formal caregivers) has a cost-saving potential in compar-
ison with traditional care.
� O
nly a few studies have explored the costs of traditionaland integrated care. These studies do not include informal
care or nursing home care.

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–1777 1765
What this paper adds
� T
his study indicates that the actual cost-saving potentialof integrated nursing home care (delivered by formal
caregivers) is limited.
� T
his study indicates that integrated nursing home care ischeaper than traditional care with respect to informal care
delivery.
1. Background
In many countries, policy measures are being taken to
promote a (better) integration of health care services (Leich-
senring and Alaszewski, 2004). All measures have in com-
mon that they are aimed at stimulating functional,
organizational or financial integration in order to develop
more complete, coherent and comprehensive structures of
service delivery (Kodner and Spreeuwenberg, 2002; Leich-
senring, 2004; Mur-Veeman et al., 2008). From the perspec-
tive of patients with complex, long-term problems, ‘[t]he
result of such multi-pronged efforts to promote integration
for the benefits of these special patient groups is called
‘integrated care’.’ (Kodner and Spreeuwenberg, 2002).
There are numerous varieties of integrated care (Paulus
et al., 2002; Van Raak et al., 2003), ranging from inter-
organisational arrangements (such as a networks in which
care is provided by multiple organisations) to intra-organi-
sational arrangements in which caregivers within a single
organization focus on the development of inter-professional
relationships (Reed et al., 2005) and multi-disciplinary co-
operation (Paulus et al., 2003). Whatever the variety, the
main purpose of integrated care is to provide a level of
service that is more sensitive to the personal circumstances
and wishes of individual patients and has better results in
terms of efficiency and cost-effectiveness (WHO, 2001). The
characteristics of the patient population and the specific
challenges they face to obtain the most appropriate care
determine the level, type and combinations of the strategies
that can best be used to foster integrated care (Leutz, 1999).
Reed et al. (2005) distinguish between three integration
strategies: macro strategies (at the societal level); mezzo-
strategies (at the organizational level) and micro strategies
(at the individual service level).
In recent years, the attention for integrated care arrange-
ments in nursing homes has been growing (Reed et al., 2005,
2007; Paulus et al., 2006). Older nursing home residents with
somatic or psycho-social problems not only require long-
term care but also different types of services from a host of
formal and informal caregivers (Leichsenring, 2004). The
financial resources to deliver nursing home care, however,
are becoming more and more scarce (Spillman and Lubitz,
2002; Remsburg, 2004). Consequently, because of its
assumed cost-effectiveness, integrated nursing home care
is becoming an important policy goal in many countries.
In the Netherlands, nursing homes have translated this
goal into an integration strategy which is focused on intra-
organisational integrated care arrangements which focus on
changing the mode of service delivery. Following the ter-
minology common in this country, the strategy should result
in a replacement of ‘traditional’ nursing home care with
‘integrated’ nursing home care (Paulus et al., 2003).
Although both types of care are not completely each other’s
opposites, a typical feature of the latter type of care is that the
demand of residents dictates what is delivered (and when,
how often, how long and by whom). Generally, residents
simultaneously need services from a multitude of caregivers,
requiring integrated actions from caregivers. These services
have to be delivered in an environment in which specific
features of the home situation are copied in nursing home
care (Paulus et al., 2005, 2006) Traditional nursing home
care, on the other hand, is supply-oriented (i.e. caregivers
dictate what is delivered, when, how often, how long, et
cetera), mono-disciplinary and requires no integrated actions
from caregivers or adaptations of service delivery to a home-
like environment. In terms of the contextual framework
above, the strategy of nursing homes can be described as
one which assumes a patient-centered notion of integration
(Kodner and Spreeuwenberg, 2002) at the mezzo-level
(Reed et al., 2005) and is aimed at linking parts within a
single institution or level of care (i.e. the nursing home)
through the creation of (intra-organisational) integration
within service delivery (Leichsenring, 2004). When applied
successfully, the strategy should result in integrated nursing
home care which is not only patient-centred but also cost-
effective and more efficient compared to traditional care
(Kodner and Spreeuwenberg, 2002).
Within the literature on integrated care, the emphasis has
been on the development and implementation of integrated
care (Van Raak et al., 2003). However, there is little evidence
on the actual cost-saving potential of integrated care (Von-
deling, 2004). Furthermore, studies with respect to nursing
home care primarily reported the costs of traditional nursing
home care activities delivered by (some) formal caregivers
(e.g. Schlenker et al., 1985; Dorr et al., 2005; Hamrick et al.,
2007). To date, results on the cost-saving potential of
integrated nursing home care, however, have not been
reported (De Bekker-Grob, 2005).
Against this background, the main purpose of this paper
is to describe the costs of an extended set of traditional and
integrated nursing home care activities and to explore the
cost-saving potential of integrated care. Because of its
explorative nature, our study also tries to indicate relevant
directions for future research on this topic. For managers,
local care providers and insurers, such an explorative ana-
lysis can indicate whether the delivery of integrated care
might be cheaper or more expensive than the delivery of
traditional nursing home care and thus whether integrated
care (and its underlying integration strategy) might be an
effective instrument to achieve a more efficient allocation of
scarce resources in nursing home care. Moreover, by focus-
ing on activities, a detailed overview can be provided on
what is delivered, by whom and for whom. This information

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–17771766
is important in order to efficiently allocate nursing time and
make decisions with respect to manpower planning and
resource utilization in nursing home care (Lemonidou
et al., 1996; Weech-Maldonado et al., 2004). Finally, by
linking the cost information from our study to results from
studies in which the impact of integrated care on the quality
of care is investigated, more general information on the cost-
effectiveness of integrated care can be obtained. Such infor-
mation is generally lacking.
2. Methods
2.1. Design
Our cost study was part of a larger study (see Paulus et al.,
2003) in which also the change process and the effects of the
introduction of integrated nursing home care on the quality
of care and the quality of work were investigated. As part of
the larger study, which used a quasi-experimental design
with three measurement periods, we assembled cost data on
traditional and integrated nursing home care delivery in
different nursing homes in the Netherlands. In this
country, there are separate and combined nursing homes
for residents with somatic problems and psycho-social
problems (www.brancherapporten.minvws.nl, accessed
October 18, 2007). Older people with somatic problems
mostly have physical limitations (e.g. due to chronic illness,
heart problems or visibility impairments). They are usually
admitted to a nursing home after receiving hospital care first.
Older people with psycho-social problems usually include
people who need mental care (often besides physical care)
and who suffer from dementia or Alzheimer’s disease.
Before being admitted to a nursing home, they received
home care first or already lived in a home for older people.
The nursing homes were selected on the basis of several
criteria including a stable working environment and motiva-
tion to contribute to the research. Two homes fulfilled all of
the criteria and were therefore purposefully selected for our
cost study. Each home had separate wards for residents with
somatic problems and for residents with psycho-social
problems. Approval to conduct the study was obtained from
the relevant ethics committees in the nursing homes.
Informed consent forms were used and all participants were
informed before, during and after the research.
One of the selected nursing homes (with 121 beds and 4
wards) delivered traditional nursing home care during the
entire research period. The other nursing home (with 88 beds
in total and 3 participating wards (with 28 beds)) introduced
integrated care in March 1998 and continued to deliver this
type of care during the research period. Prior to the intro-
duction of integrated care, this nursing home also offered
traditional care.
Although both types of care were not completely each
other’s opposites, according to the care managers of the
participating homes, there were five main differences
between traditional and integrated care. First, traditional
care delivery was more supply-oriented while integrated
care was more demand-oriented. In practice, the latter
was expressed in the attention that was given by caregivers
to certain individual wishes of residents. For instance,
instead of getting out of bed at the same time each day
(in traditional care), residents could indicate the time they
preferred to get out of bed in integrated care. Secondly,
residents receiving integrated care and their informal care-
givers were engaged in daily activities such as cooking,
cleaning, doing the laundry. In traditional care they were not
and cooking took place in a central kitchen. Thirdly, for
residents receiving integrated care, there were small scale
wards with a limited number of residents (generally, a
maximum of 12 per ward). In traditional care, there were
approximately 30 residents per ward. Most of these residents
also had to share bedrooms. Fourthly, in integrated care, the
delivery of services was more integrated compared to tradi-
tional care. In practice, this was visible in the fact that nurses
also conducted certain activities (e.g. meal activities or
household activities) which were traditionally conducted
by nutrition assistants or household assistants or vice versa.
More coordination with informal caregivers was also part of
integrated care. Finally, in integrated care, to mimic the
home situation, there were more social group activities for
residents.
As part of the larger study, it was tested whether tradi-
tional and integrated nursing home care also actually dif-
fered with respect to these five characteristics. This study
(Vijgen et al., 2003) showed that there were significant
differences between both homes as regards scale, demand-
orientation, engagement of residents in daily activities, and
an integrated delivery of care services (especially as regards
residents with psycho-social problems). Although, there
were various social group arrangements, financial limita-
tions in the integrated nursing home restricted a well-
functioning club structure. In related studies, we also
showed the actual differences between traditional and inte-
grated nursing home care as regards the role of informal
caregivers (Paulus et al., 2005); the performance of activ-
ities by certain caregivers (Paulus et al., 2006) and the
frequency and duration of these activities (Paulus and Van
Raak, 2008). The most important similarities and differ-
ences between both homes are listed in Table 1. The table
shows that there are many similarities such as the average
dependency score of residents, the types of informal care-
givers involved in care delivery, visiting hours and the
average level of personnel costs for many formal caregivers.
However, the type and absolute number of roles involved in
the delivery of formal care differed to some extent. The
related implications of the latter are explored in the dis-
cussion part of this paper.
During the research period, there were waiting lists for
different types of care for older people in the Netherlands. In
2003, for instance, approximately 7000 people were on the
waiting list for nursing home care. Although there were

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–1777 1767
Table 1
Features of the two nursing homes
Features Nursing home offering traditional care Nursing home offering integrated
care
Annual financial turnover
(in 2001; million Euro)
7.4 8.0 (including care offered to
homes for older persons)
Number of wards/groups 4 (2 for residents with somatic problems;
2 for residents with psycho-social problems);
all wards participated in the cost study.
6 (2 for residents with somatic
problems; 4 for residents with
psycho-social problems); 3
wards participated in the
cost study.
Number of residents for whom activities
were recorded
90 per measurement (on average) 24 per measurement (on average)
Average dependency score residents
(with standard deviation)a
9.78 (0.24) 9.58 (0.55)
Number of participating formal caregivers 159 per measurement (on average) 69 per measurement (on average)
Composition/types of formal caregivers
involved in care deliveryb (and their
average gross personnel costs per minute;
average of three time points; in Euro)
Licensed practical nurse (0.216), geriatric
nurse (0.178), registered nurse (0.253), ward
assistant (0.167), evening/night/weekend
manager (0.253), recreational activities
supervisor (0.213), nutrition assistant (0.190),
living room assistant (0.14), student nurse
(0.14), trainee (0.00), volunteer (0.00),
nursing assistant (0.082), nursing care
coordinator (0.238), aid (0.144), kitchen
assistant (0.164).
Licensed practical nurse
(0.210), geriatric nurse (0.191),
registered nurse (0.259),
evening/night/weekend manager
(0.253), recreational activities
supervisor (0.191),
nutrition assistant (0.188),
household assistant (0.181),
student nurse (0.124), trainee
(0.00), volunteer (0.00),
nursing assistant (0.181).
Number of forms filled in by formal caregivers 16238 (in total) 6027 (in total)
Average duration of direct care activities by
formal caregivers for somatic residents
(in minutes, with standard deviation)c
T1: 11.73 (14.02) T1: 14.49 (13.29)
T2: 14.67 (16.82) T2: 10.08 (7.25)
T3: 10.05 (4.92) T3: 9.47 (6.71)
Average duration of direct care activities by
formal caregivers for residents with
psycho-social problems (in minutes,
with standard deviation)c
T1: 14.84 (22.13) T1: 10.14 (5.40)
T2: 17.47 (19.80) T2: 10.78 (10.06)
T3: 14.98 (15.42) T3: 10.05 (5.13)
Types of informal caregivers involved in
care delivery
Mainly partners and sons/daughters, but
also brothers/sisters, other family members,
friends, neighbours.
Mainly partners and sons/
daughters, but also brothers/
sisters, other family members,
friends, neighbours.
Visiting hours Unlimited Unlimited
Number of forms filled in by informal
caregivers
794 (in total) 321 (in total)
T1, T2, T3 = First, second and third measurement point, respectively.a This feature was tested as part of the larger study (Vijgen et al., 2003).b See Paulus et al. (2006) for an elaborate description of all roles.c Based on Paulus and Van Raak (2008).
regional differences, the average waiting time was 9 months
(www.minvws.nl/dossiers/verpleeg–en-verzorgingshuizen/,
accessed October 18, 2007; www.scp.nl, accessed October
18, 2007). Due to this situation, most (potential) residents
could not really choose between nursing homes (with a
specific type of care).
2.2. Cost method and cost perspective
To determine the costs, we used the method of activity-
based costing (ABC). Since integrated care has processual
characteristics (because of continuous changes in care deliv-
ery) and incorporates many coordinating and co-operative

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–17771768
activities (which can produce uncertain outcomes) and is
aimed at tailor-made care for each individual (so standar-
dized outcomes are absent), determination of the costs of
integrated care required a method which could be used
irrespective of the presence of stable, certain and standar-
dized outcomes. Of all existing cost methods, ABC was the
only method which could meet these requirements. ABC
was therefore selected to provide the best cost information to
decision-makers (Paulus et al., 2002).
ABC assumes that a product or service carries costs in
terms of the activities that it incorporates (Kaplan and
Cooper, 1998; Paulus et al., 2002). Cost-determination
therefore entails identification of the relevant activities
and resources needed to perform these activities. After
the final product or service is defined, this information is
used to identify the costs of the product or service (Kaplan
and Atkinson, 1998). Studies show that besides formal
caregivers, also informal caregivers are important resources
which contribute to activities delivered to older persons in
institutionalised settings (Whitlatch and Noelker, 1996;
Lyons and Zarit, 1999; Gaugler et al., 2004; Paulus et al.,
2005; SCP, 2005). Furthermore, since integrated care
focuses more than traditional care on the co-ordination with
informal caregivers and on a more active role of these
caregivers in daily activities, the amount of informal care
is also expected to differ between both care types (Paulus
et al., 2005). Therefore, both formal care and informal care
are part of our cost analysis. By including both types of care
as important cost features, we look at the costs from a
societal perspective (Gold et al., 1996).
2.3. Data-collection
Following the design of the larger study, we collected
data at three measurement periods between September 1999
and February 2003. At each time point, we determined the
costs of traditional and integrated care. By repeating the
same measure we could obtain more data, prevent the well-
known shortcomings of cross-sectional research and
increase the reliability of our study. Moreover, by repeating
the same measure, possible changes in the costs of integrated
care over time could be taken into account. The latter is
considered necessary because the effects of integrated care
on the costs of service delivery over time are largely
unknown (Vondeling, 2004).
Given the final service (care delivery) and the resources
(formal and informal caregivers), the bulk of the data-collec-
tion consisted of assembling information on the activities
conducted by caregivers. We used the method of self-reporting
on the basis of an a priori defined list of activities. Burke et al.
(2000, p. 124) show that for data-collection on nursing
activities in institutional settings this is an accurate method
of data-collection. They state: ‘self-reporting allows . . . to
define a list of activities precisely and to review the activity
definitions carefully with participants. By focusing on a select
list of activities, perceptual differences among participants
and the burden of continuous self-reporting are minimized’. In
this study, we also used a select list of activities. Selections
were made on the basis of a literature study (Minyard et al.,
1986; Schuster and Cloonan, 1989; Hendrikson et al., 1990;
Cardona et al., 1997), interviews with caregivers in nursing
homes throughout the country and observations in nursing
homes that offered traditional or integrated care. To test the
clearness, validity and usefulness of the list, in two of these
homes a pilot study was executed in March 2000. In each
nursing home, a random sample of formal caregivers tested the
lists during 2 days (2 � 24 h). On the basis of the comments
and suggestions of those participating in the pilot (‘expert
opinions’), two final lists were made. One list described direct
care activities (i.e. activities related to individual residents).
The other list described indirect activities (i.e. activities for a
group of residents or for the entire ward). Together, both forms
listed 24 selected activities customary for nursing home care
in the Netherlands. Table 2 gives an overview of these
activities.
At each of the three measurement points, each lasting 14
consecutive days, caregivers recorded information on the
activities they conducted for (a group of) residents. To
minimize self-reporting bias and further increase the validity
and reliability of the study, those who designed the list were
present at all measurements to stimulate a proper recording
or solve any questions with respect to the list of activities.
Formal caregivers represented 15 roles, which ranged
from different types of nurses to nutrition assistants. In
traditional care, on average 159 formal caregivers per mea-
surement point recorded their activities. In integrated care,
this average was 69. Informal caregivers included partners,
brothers and sisters, sons and daughters, neighbours, friends,
and others. In traditional care, on average 242 forms were
filled in by informal caregivers per measurement point. In
integrated care this average was 115. Residents were patients
with physical or psycho-social needs who had an average
dependency score of 9 (on a scale from 1 to 12). This score
represents the care load on the nursing wards and was
measured by the SIVIS-Help Index (SIG, 1994), which is
an instrument used in nursing homes in the Netherlands.
Measured on a 12-point scale, the index measures the
resident’s functioning in daily living. The higher the score,
the higher the care load. For residents receiving traditional
care, activities were registered at the three measurement
points for 84, 89 and 98 residents, respectively. In integrated
care, these numbers were 25, 23 and 26, respectively.
Immediately or shortly after they performed an activity;
formal caregivers marked that activity on the relevant list.
They also indicated the duration of that activity (how many
minutes did the activity take?) and (and how often and) for
whom the activity had been performed. In total, 22,265 forms
from formal caregivers were subjected to data analysis.
For informal caregivers, a simplified form was developed
that listed the same 24 activities. Also informal caregivers
recorded the type, frequency and duration of activities
immediately or shortly after they performed the activity.

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–1777 1769
Table 2
Recorded activities (partly based on Paulus et al., 2003, 2006)
Activities Description
Direct care activities
Morning care Getting residents out of bed, bathing, dressing, shaving, combing hair
Coffee/tea making Making and pouring out coffee and tea, doing the dishes, cleaning up
Medication Recording, distributing and helping with medication
Toileting Helping residents who need to go to the bathroom, changing
incontinence slips, emptying catheters
Afternoon care Bringing residents to bed (and sometimes getting out of bed),
dressing/undressing residents, combing hair
Extra care Giving extra attention to residents through conversations, walking
or shopping, extra pedicure or hair treatment
Evening care Bringing residents to bed, bathing, cleaning teeth and dentures
Meal activities Preparing meals, setting the table, helping residents with eating, doing the dishes
Medical care Taking care of wounds, catheterise, medical treatments, etc.
General activities Preparing and doing activities such as pottering, singing, playing
games with residents and cleaning up afterwards
Club activities Preparing and doing social activities in groups (e.g. a choir or bridge-club)
Transfer and transport Bringing residents to or back from a particular social activities
meeting ward or room for general activities or appointments
Reacting to incidents Taking care of residents in case of extra-ordinary events (e.g. a sudden
change in health, aggressive behaviour towards other residents or staff)
Additional direct activities Activities other than those mentioned above such as: buying extra food
or clothing or doing the laundry for a particular resident
Having chats with residents Socializing with residents (e.g. ordinary day to day talks during a cup
of tea) or talks by informal carers with their family member
Indirect care activities
Consultation Having consultations on and evaluating the course of matters with residents, a
group of residents, caregivers during planned or unplanned meetings
Administration Keeping and readjusting patient’s files; administration
Schooling Participating in courses, training and schooling sessions and attending
meetings relevant for keeping a specific function up to date
Handling supplies Ordering, handling and storing different (consumer) goods (such as
towels, incontinence slips, toilet paper, cleaning products)
Handling food Shopping to buy food, storing food supplies, etc.
Handling medication Ordering and preparing medicines
Cleaning Cleaning/dusting rooms, bathrooms, hallways, beds
Additional indirect activities Activities other than those mentioned above such as: making rounds on wards, etc.
Out of pocket activities Activities by informal carers such as doing the laundry, ironing or
buying make-up for their family member
They filled in a form each time they visited the nursing home
during the measurement period. Each period lasted 14 days. In
the Netherlands, such a time period covers most visits. A
recent study on nursing home care, for instance, shows that
approximately 29% of the residents in nursing homes in this
country get daily visits from informal carers. 48% on average
is visited at least once a week and 12% more than once per
week (SCP, 2005). Both homes had unlimited visiting hours.
Those who designed the list were present in the nursing homes
to stimulate a proper recording. In total, 1115 forms from
informal caregivers were subjected to data analysis.
To determine the costs of activities performed by formal
caregivers, we assembled additional data on the personnel
costs. In the Netherlands, total personnel costs include the
gross wage (including certain bonuses) and additional per-
sonnel costs. The latter costs include, among others, social
insurance premiums, pension contributions and holiday pay.
Guidelines on economic evaluation in the Netherlands indi-
cate that the gross wage plus a surcharge of 35% is a valid
estimation of the total personnel costs (Oostenbrink et al.,
2000). The percentage represents the additional personnel
costs. Using the data on gross wages that we obtained from
the nursing homes and applying the recommended guide-
lines, this allowed a specification of the gross personnel costs
per activity per minute per role (in Euro (s)). Since each
individual resident received a certain number of activities
per day, this also allowed determination of the total and
average costs per resident per day.
Following the findings of a pilot study on the valuation of
informal nursing home care (Vijgen, 2000), we decided to

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–17771770
use two shadow prices to determine the costs of activities
performed by informal caregivers. The first shadow price
reflects the ‘legal worker tariff’ (lwt). This tariff represents
the lowest fee for a specific activity in case it would have
been performed by a professional (formal) caregiver. In the
Netherlands, this fee was equal to s7.941 gross per hour at
the first measurement point (Oostenbrink et al., 2000). The
second shadow price is the ‘average gross personnel costs’
(agpc). It reflects the average total personnel costs per
minute per role taking into account the relative number of
formal caregivers per role per measurement and per nursing
home. Relevant data on the number of caregivers were
provided by the nursing homes and were used to specify
the costs of informal care per activity, per minute and per
resident (in s).
2.4. Data analysis
SPSS 10.0 was used to file and analyse all data. First, we
calculated the (total) average costs of formal and informal
care per resident per day (see Table 3). This average was
determined by adding up the costs at the three separate time
points. Then, this outcome was divided by three in order to
determine the mean value of the costs during the entire
period. Since an average resident received a number of
activities per day, the average costs per direct and indirect
activity (per measurement point, type of caregiver and type
of nursing home care) had to be calculated (see Tables 4 and
5). Since residents had somatic (i.e. physical) or psycho-
social problems, we distinguished between the costs per
activity for these two types of residents. The total average
costs per resident were determined by adding up the average
costs of formal direct care, formal indirect care and informal
direct care. Then the average was calculated as the mean
value of these costs during the research period. Finally, the
costs of traditional and integrated care were compared to
each other. On the basis of descriptive statistics, comparisons
were made per type of resident, per type of caregiver, per
Table 3
Costs per resident per day (in Euro (s))a
Traditional care
Residents with
somatic problems
R
ps
pr
Average costs
Formal direct care 22.30 (2.75) 19
Formal indirect care 16.18 (2.30) 12
Informal direct care (lwt) 20.51 (5.79) 19
Informal direct care (agpc) 34.26 (9.27) 32
Total average costs
Formal + informal care (lwt) 56.96 (6.28) 50
Formal + informal care (agpc) 70.15 (9.26) 63
Lwt = legal worker tariff; agpc = average gross personnel costs.a Calculated as the average of the costs at three measurement points.
activity and per set of activities (direct and indirect care). By
exploring the cost-saving potential of integrated care in this
way, our study intends to produce insights that must be tested
during future research.
3. Results
3.1. Costs per resident per day
Table 3 shows that the delivery of formal direct care to
residents receiving integrated care was more expensive
compared to traditional care. Differences ranged between
s8.00 (residents with somatic problems) and s10.00 (resi-
dents with psycho-social problems) per resident per day. For
residents with psycho-social problems, also the costs of
formal indirect care were higher in integrated care. For
residents with somatic problems, the costs of formal indirect
care were approximately s16.00 per resident in both care
types. For both types of residents, the average costs of
informal direct care were lower in integrated care.
Table 3 also shows that (based on lwt-calculations) the
total average costs per resident per day were higher in
integrated care compared to traditional care. For residents
with psycho-social problems, these costs were s50.66 for
traditional care and s64.99 for integrated care. For residents
with somatic problems, these costs were s56.96 and
s59.28, respectively. Based on agpc-calculations, however,
the total average costs of integrated care for residents with
somatic problems were slightly below those of traditional
care (s68.53 and s70.15, respectively).
In traditional care, the average costs of formal direct and
indirect care for residents with somatic problems were
higher compared to residents with psycho-social problems.
The difference in costs was about s3.50 per resident per day.
For both types of residents, the average costs of informal
direct care (determined on the basis of agpc) outweighed the
costs of formal direct care.
Integrated care
esidents with
ycho-social
oblems
Residents with
somatic problems
Residents with
psycho-social
problems
.90 (1.50) 30.97 (0.32) 29.59 (4.00)
.96 (2.10) 16.62 (2.01) 30.28 (5.19)
.45 (2.92) 13.85 (3.53) 8.23 (1.26)
.61 (5.62) 23.49 (6.11) 13.89 (1.67)
.66 (4.30) 59.28 (2.44) 64.99 (7.30)
.46 (7.38) 68.53 (4.96) 71.07 (8.54)
Standard deviation in brackets.
A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–1777 1771
Table 4
Average costs per activity (formal care) (in Euro (s))a
Traditional care Integrated care
Som PG Som PG
Direct care
Morning care 5.07 (0.75) 4.48 (0.12) 5.67 (0.09) 5.17 (0.51)
Coffee/tea making 5.64 (0.52) 7.32 (0.82) 4.23 (0.80) 3.38 (1.09)
Medication 1.33 (0.25) 1.02 (0.16) 0.85 (0.09) 0.81 (0.17)
Toileting 1.67 (0.22) 1.38 (0.70) 1.39 (0.06) 1.52 (0.87)
Afternoon care 3.09 (0.50) 3.17 (0.22) 2.46 (0.19) 2.72 (0.50)
Extra care 1.97 (0.19) 1.44 (0.38) 1.79 (0.26) 2.0 (0.49)
Evening care 3.59 (0.52) 3.28 (0.38) 3.68 (0.14) 3.45 (0.32)
Meal activities 1.52 (0.33) 1.90 (0.10) 1.77 (0.21) 1.8 (0.21)
Medical care 1.95 (0.54) 1.47 (0.20) 1.54 (0.21) 1.41 (0.38)
General activities 15.51 (6.87) 22.03 (3.60) 4.95 (2.38) 3.91 (0.55)
Club activities 1.56 (1.60) 6.95 (8.22) 5.32 (3.50) 6.34 (4.57)
Transfer and transport 1.38 (0.25) 0.90 (0.04) 0.96 (0.07) 1.29 (0.33)
Reacting to incidents 2.66 (0.16) 3.46 (0.75) 1.67 (0.09) 1.83 (0.30)
Additional direct activities 2.18 (0.71) 1.63 (0.80) 2.24 (1.04) 1.97 (0.52)
Average costs of set of direct care activitiesb 3.51 (0.70) 4.31 (0.67) 2.75 (2.36) 2.68 (0.24)
Indirect care
Consultation 0.84 (0.12) 0.81 (0.12) 1.25 (0.19) 0.82 (0.06)
Administration 1.70 (0.21) 1.04 (0.26) 0.91 (0.13) 0.88 (0.15)
Schooling 8.91 (5.65) 13.59 (8.03) 26.02 (17.80) 25.96 (25.64)
Handling supplies 3.10 (0.40) 2.14 (1.64) 2.36 (0.20) 3.02 (0.79)
Handling food 3.50 (0.25) 2.08 (3.60) 0.13 (0.22) –
Handling medication 5.63 (0.38) 8.23 (4.50) 5.89 (2.71) 5.07 (1.60)
Cleaning 6.97 (1.53) 6.63 (1.04) 5.67 (1.00) 7.25 (0.93)
Additional indirect activities 10.16 (1.47) 13.70 (0.97) 6.41 (2.36) 11.57 (6.30)
Average costs of set of indirect activitiesc 5.09 (0.33) 6.03 (1.34) 6.07 (1.87) 6.82 (2.60)
Som = residents with somatic problems; PG = residents with psycho-social problems.a Calculated as the average of the costs at three measurement points. Standard deviation in brackets.b Calculated as the average of the costs of 14 direct activities (since ‘chats with residents’ was not performed by formal caregivers, this activity
was not included in the calculation).c Calculated as the average of the costs of 8 indirect activities (since ‘out of pocket activities’ were not performed by formal caregivers, this
activity was not included in the calculation).
With respect to integrated care, Table 3 shows that the
delivery of formal indirect care to residents with psycho-
social problems was costlier than the delivery of the same
type of care to somatic residents. The difference in costs
was approximately s14.00 per resident per day. The
average costs of informal direct care for somatic residents
outweighed those made for residents with psycho-social
problems.
3.2. Costs per activity
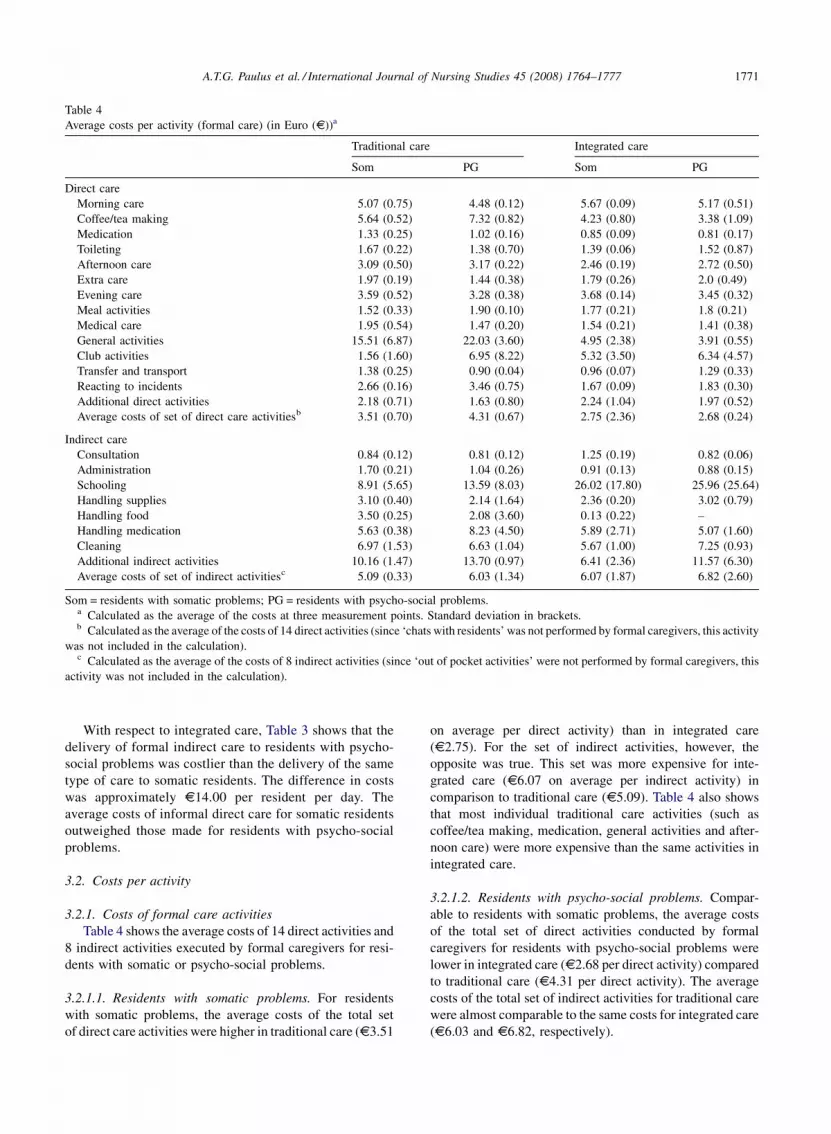
3.2.1. Costs of formal care activities
Table 4 shows the average costs of 14 direct activities and
8 indirect activities executed by formal caregivers for resi-
dents with somatic or psycho-social problems.
3.2.1.1. Residents with somatic problems. For residents
with somatic problems, the average costs of the total set
of direct care activities were higher in traditional care (s3.51
on average per direct activity) than in integrated care
(s2.75). For the set of indirect activities, however, the
opposite was true. This set was more expensive for inte-
grated care (s6.07 on average per indirect activity) in
comparison to traditional care (s5.09). Table 4 also shows
that most individual traditional care activities (such as
coffee/tea making, medication, general activities and after-
noon care) were more expensive than the same activities in
integrated care.
3.2.1.2. Residents with psycho-social problems. Compar-
able to residents with somatic problems, the average costs
of the total set of direct activities conducted by formal
caregivers for residents with psycho-social problems were
lower in integrated care (s2.68 per direct activity) compared
to traditional care (s4.31 per direct activity). The average
costs of the total set of indirect activities for traditional care
were almost comparable to the same costs for integrated care
(s6.03 and s6.82, respectively).
A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–17771772
Table 5
Average costs per activity (informal care) (in Euro (s))a
Traditional care Integrated care
Som PG Som PG
lwt agpc lwt agpc lwt agpc lwt agpc
Direct care
Morning care 0.91 (1.57) 1.58 (2.74) 1.15 (1.35) 1.93 (2.22) – – – –
Coffee/tea making 3.31 (1.46) 5.60 (2.67) 2.24 (0.27) 3.75 (0.56) 2.26 (0.48) 3.41 (1.51) 2.21 (1.76) 3.67 (2.83)
Medication 2.02 (1.79) 3.42 (3.07) 0.66 (0.37) 1.11 (0.66) 1.02 (0.30) 1.69 (0.54) 0.32 (0.44) 0.54 (0.75)
Toileting 1.70 (0.44) 2.85 (0.79) 1.33 (0.33) 2.25 (0.63) 1.22 (2.12) 2.15 (3.72) – –
Afternoon care 1.02 (1.16) 1.74 (2.02) 1.47 (0.84) 2.49 (1.50) 6.1 (7.40) 10.4 (12.48) – –
Extra care 1.74 (0.35) 2.93 (0.66) 4.34 (1.08) 7.25 (1.74) 2.69 (2.33) 4.63 (4.00) – –
Evening care 2.17 (1.33) 3.65 (2.30) 2.24 (0.76) 3.78 (1.38) – – 0.88 (1.53) 1.55 (2.68)
Meal activities 8.98 (4.23) 15.08 (7.26) 4.72 (1.16) 7.93 (2.24) 4.32 (3.94) 7.16 (6.48) – –
General activities 5.16 (1.73) 8.56 (2.65) 7.93 (3.22) 13.31 (5.44) 5.64 (9.77) 9.23 (15.99) – –
Club activities 3.44 (4.25) 5.9 (7.44) 8.11 (8.19) 13.88 (14.2) 8.33 (7.22) 13.85 (12.0) 12.99 (3.65) 16.16 (14.4)
Transfer and transport 4.62 (0.54) 7.72 (0.76) 4.51 (1.64) 7.54 (2.68) 8.11 (8.19) 13.44 (13.8) – –
Reacting to incidents 31.48 (47.6) 51.53 (77.2) 2.14 (2.20) 3.57 (3.63) – – 7.28 (8.34) 6.9 (11.95)
Having chats with
residents
14.22 (2.01) 23.65 (3.83) 12.14 (1.02) 20.34 (2.41) 12.76 (5.88) 16.99 (15.8) 7.54 (0.43) 12.76 (0.39)
Average costs of set
of direct care
activitiesb
6.21 (4.51) 10.91 (7.34) 4.07 (1.12) 6.85 (0.91) 4.04 (1.99) 8.18 (1.29) 2.01 (1.09) 2.33 (1.17)
Indirect care
Consultation 4.70 (2.07) 7.94 (3.81) 1.96 (0.60) 3.30 (0.79) 4.19 (1.63) 7.13 (2.99) 1.48 (2.56) 2.5 (4.33)
Cleaning 0.32 (0.34) 0.55 (0.60) 1.35 (1.37) 2.31 (1.39) 1.93 (0.91) 3.26 (1.48) 2.73 (4.73) 4.62 (8.0)
Out of pocket activities 5.23 (1.14) 8.77 (7.34) 7.66 (1.35) 12.80 (2.12) – – – –
Average costs of set
of indirect
activitiesc
3.42 (1.14) 5.75 (2.13) 3.65 (0.82) 6.14 (0.21) 2.04 (0.72) 3.08 (0.85) 1.40 (2.43) 2.37 (4.11)
Som = residents with somatic problems; PG = residents with psycho-social problems; Lwt = legal worker tariff; agpc = average gross personnel
costs.a Calculated as the average of the costs at three measurement points. Standard deviation in brackets.b Calculated as the average of the costs of 13 direct activities (since medical care and additional direct activities were not performed by formal
caregivers, these activities were not included in the calculation).c Calculated as the average of the costs of 3 indirect activities (the remaining activities were not performed by informal caregivers).
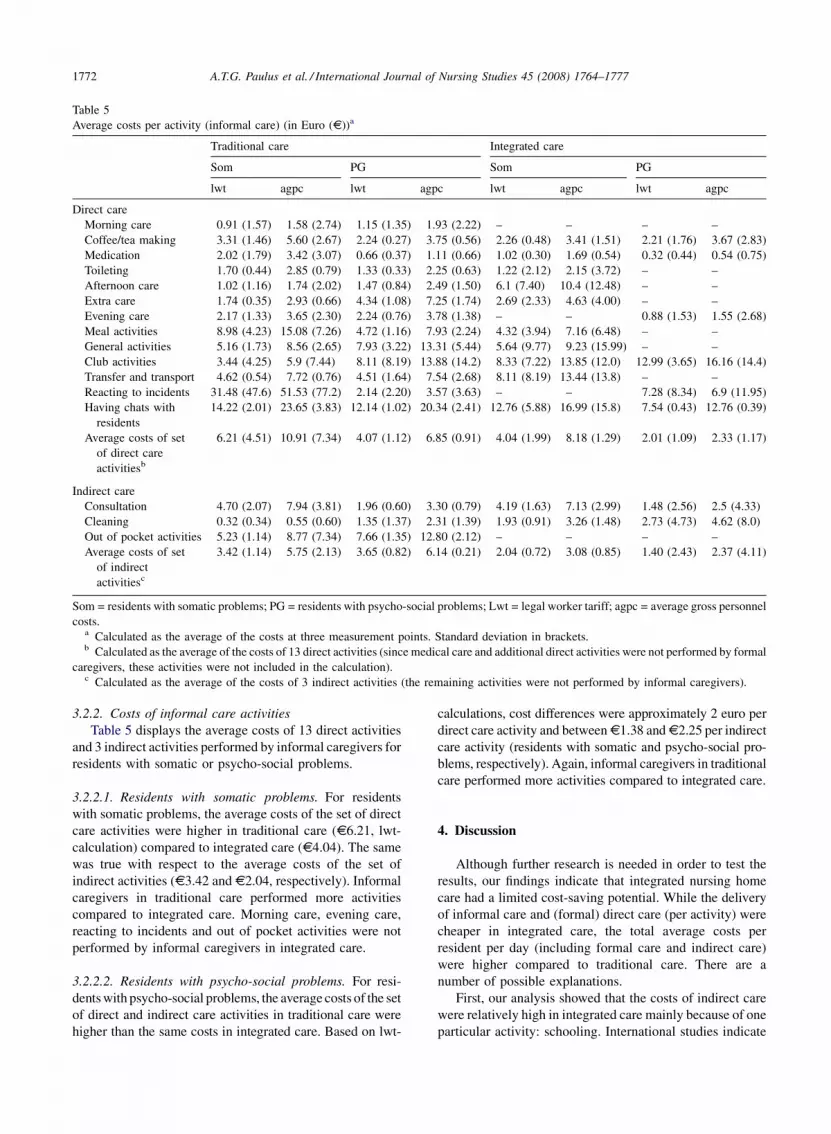
3.2.2. Costs of informal care activities
Table 5 displays the average costs of 13 direct activities
and 3 indirect activities performed by informal caregivers for
residents with somatic or psycho-social problems.
3.2.2.1. Residents with somatic problems. For residents
with somatic problems, the average costs of the set of direct
care activities were higher in traditional care (s6.21, lwt-
calculation) compared to integrated care (s4.04). The same
was true with respect to the average costs of the set of
indirect activities (s3.42 and s2.04, respectively). Informal
caregivers in traditional care performed more activities
compared to integrated care. Morning care, evening care,
reacting to incidents and out of pocket activities were not
performed by informal caregivers in integrated care.
3.2.2.2. Residents with psycho-social problems. For resi-
dents with psycho-social problems, the average costs of the set
of direct and indirect care activities in traditional care were
higher than the same costs in integrated care. Based on lwt-
calculations, cost differences were approximately 2 euro per
direct care activity and between s1.38 and s2.25 per indirect
care activity (residents with somatic and psycho-social pro-
blems, respectively). Again, informal caregivers in traditional
care performed more activities compared to integrated care.
4. Discussion
Although further research is needed in order to test the
results, our findings indicate that integrated nursing home
care had a limited cost-saving potential. While the delivery
of informal care and (formal) direct care (per activity) were
cheaper in integrated care, the total average costs per
resident per day (including formal care and indirect care)
were higher compared to traditional care. There are a
number of possible explanations.
First, our analysis showed that the costs of indirect care
were relatively high in integrated care mainly because of one
particular activity: schooling. International studies indicate

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–1777 1773
that schooling in general and interprofessional learning in
particular is a necessity for an integrated delivery of services
(Colyer, 2004). This may explain why the costs of indirect
care in integrated care were higher compared to traditional
care. Our analysis also made clear that in integrated care
fewer activities were delivered by informal caregivers.
Consequently, the costs of informal care were lower com-
pared to traditional care. The total average costs per resident
per day (including formal care), however, were higher in
integrated care. One possible explanation is substitution, i.e.
a process in which formal caregivers undertake activities
usually performed by informal caregivers. Such a process
would stimulate a shift from informal to formal care costs.
This explanation, however, is not compatible with the find-
ings from other studies on care for older people. These
suggest higher contributions by informal caregivers (e.g.
Aneshensel et al., 1995; Bass et al., 1996; Robinson, 1997;
Arno et al., 1999; Wimo et al., 2002; Van Raak et al., 2003).
It is therefore recommended to further investigate factors
which can explain cost-shifts in integrated care.
Secondly, it can be questioned whether our findings were
influenced by the fact that there was no full match between
some features of formal caregiving in both homes. Table 1
shows that, while there were matches with respect to resi-
dents and informal caregivers, the type and absolute number
of roles involved in the delivery of formal care differed to
some extent. In traditional care, there were 15 different roles.
Five of these roles (ward assistant; living room assistant,
nursing care coordinator, aid and kitchen assistant) were not
present in integrated care. The latter three roles were
involved in a majority of the activities (see Paulus et al.,
2006). In integrated care, there were 11 different roles. One
of these roles (household assistant) was not present in
traditional care and was unique for integrated care. Also
this role was involved in a majority of the activities (Paulus
et al., 2006). To what extent the presence of more and
different roles in traditional care affected the costs of direct
and indirect care is unknown. Further investigation is there-
fore recommendable. Table 1 also presents the wage levels
of formal caregivers. Although most levels were compar-
able, there were considerable differences between the wage
level of the nursing assistant in both homes (s0.082 per
minute in traditional care; s0.181 per minute in integrated
care). In a related study we showed that this assistant was
involved in more activities (and mostly to a larger extent) in
integrated care compared to traditional care (Paulus et al.,
2006). This may explain part of the higher costs per resident
which are associated with the delivery of integrated care.
Table 1 also presents the average duration of direct care
activities in both traditional and integrated care. Although
there were relatively large standard deviations, it is clear that
the average duration of these activities for residents with
psycho-social problems was considerably lower in inte-
grated care compared to traditional care. This may explain
why the average costs per direct activity were lower in
integrated care.
The fact that there was no full match between some
formal caregivers’ characteristics is a limitation of this study.
There are other methodological limitations as well. To
obtain information on (the duration of) activities, we used
the method of self-reporting. Besides the burden of report-
ing, it is sometimes argued that self-reporting may also result
in a bias: participants may not tell the truth about their
activities or record socially desirable or self-perceived rather
than actual job performances. Furthermore, conceptual dif-
ferences between participants of what constitutes an activity
may lead to under- or overestimation of the number of
activities (Burke et al., 2000). Different caregivers may also
have different perceptions of activities and record (the
duration of) activities differently (e.g. because of different
personal characteristics). This also poses questions with
respect to the reliability of the self-reporting method. Burke
et al. (2000) make clear that the reliability of the self-
reporting method would increase if the outcomes would
approximate the outcomes provided by an alternative
method (such as observations or interviews). Our research
is limited in the sense that we did not investigate this. The
duration and sample size of the research did not allow
conducting a comparable number of observations and inter-
views. Furthermore, it has to be noted that alternative
methods such as the observation method also have some
well-known shortcomings. Continuous time observations,
for instance, can result in observer-induced bias: caregivers
may change their behavior when being observed. Secondly,
observations may be costly: each caregiver has to be
observed during a certain period of time. The use of obser-
vations is therefore usually restricted to a limited number of
participants or a short observation period. Obviously, the
duration and scale of our study did not match with these
conditions. Because of this, the biases of self-reporting may
be no greater than the biases of observations, as Burke et al.
(2000) show in their study. For our cost study, the application
of the self-reporting method provided us with more than
23,000 forms with detailed information on activities, the
duration (and frequency) thereof and by whom they were
performed. Obtaining the same number and detailed level of
information (needed to determine the costs of nursing home
care and compare it to traditional care) by way of interviews
was practically and financially infeasible. Moreover, the
retrospective nature of such interviews could have resulted
in a recall bias. In conclusion: given our aims, we used the
most appropriate method to collect our data. Further valida-
tion of the a priori lists that we used for self-reporting is
recommended for future research. Future research on the
impact of certain characteristics of caregivers on the regis-
tration (and duration) of these activities and their perceptions
thereof is also recommended.
On the basis of descriptive statistics, we reported cost
differences between traditional and integrated care.
Although the cost information we provided was far more
detailed compared to most cost studies, we did not use
statistical methods to test the significance of these differ-

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–17771774
ences. Instead we described these differences because we
wanted to explore the cost-saving potential of integrated
care. Since so little is known about the costs of this type of
care (while many stakeholders and scholars automatically
assume that it has a cost-saving potential), we wanted to
open part of the current black box. Our study indicates that
(irrespective of significance testing), providing an answer to
the question ‘is integrated care cheaper or not?’ is not that
simple. Integrated care can be cheaper or more expensive at
the same time, depending on the types of costs, activities and
residents included. Since there is no general agreement on
this, our study intended to produce insights which can be
used during future research. For future cost comparisons, it
is recommendable to actually test the cost-saving potential
provided that particular methodological challenges have
been met. By definition, integrated nursing home care is
aimed at small scale arrangements. Comparisons with tradi-
tional care (with large scale arrangements) therefore always
have to deal with the problem of ‘numbers’ (see Table 1
which illustrates this problem in our study with respect to the
number of residents and formal caregivers included in this
study). Furthermore, due to its demand-orientation and
underlying integration strategy, integrated care delivery
(and the associated roles and informal–formal care relation-
ships) develops and changes continually in response to the
demands from users. Comparisons with a more ‘static’ usual
care arrangement can therefore present formidable metho-
dological challenges. In our cost study, we tried to capture
the ‘dynamics’ of integrated care delivery by repeating the
same measure at different time points and using the out-
comes to determine the mean value of the costs. In this way,
we tried to present a more realistic picture of the costs. It is
recommended to further explore these and related metho-
dological challenges in future research.
On the basis of 23,380 lists on which a range of formal and
informal caregivers reported the activities they conducted
during 42 days, we investigated the costs of traditional and
integrated nursing home care in the Netherlands. Most of these
activities are routine activities in nursing home care in many
countries (Paulus et al., 2006). Moreover, our finding that
integrated care has a limited cost-saving potential (especially
for formal care) is comparable with the results from interna-
tional studies such as Wan et al. (2001), Newhouse et al.
(2003) and Segal et al. (2004). These features indicate some
potential for generalization. It has to be noted, however, that
there also studies which indicate that integrated care leads to
cost savings (Bernabei et al., 1998; Hernandez et al., 2003;
Johri et al., 2003; Gross et al., 2004; Leung et al., 2004). Here
the problem arises that these studies refer to different types of
integrated care for older persons, various integration strategies
and a variety of costs. Integrated nursing home care as defined
in our research is not part of these studies. In this sense, our
study is quite unique.
Our findings suggest that integrated care leads to cost
savings in some care delivery activities (such as informal care
activities and a set of formal direct care activities) and to
additional costs in others (such as certain formal indirect care
activities and the average total costs per resident). For the
practice and development of care delivery, these findings
suggest that integrated care can principally be a viable option
in case decision-makers can control the costs of indirect care
as well as the costs per resident. Controlling the costs of
schooling and training for formal caregivers (as part of indirect
care) and choosing an efficient size of the group of residents to
which integrated care has to be delivered seem particularly
important in this respect. Otherwise, decision-makers should
take into account that the introduction of integrated care leads
to shifts and/or increases in the costs rather than to cost
savings. In that case, integrated care seems a viable option
only as long as these costs are evenly matched with the
relevant benefits. As Kodner and Kyriacou (2000) indicate,
fully integrated models of care may improve the delivery of
health and social care for older people. Possible benefits
include better patient outcomes and improvements in the
quality of care or the quality of work (Weech-Maldonado
et al., 2006). Our study is limited in the sense that we did not
assess these or other potential benefits of integrated care.
However, as we explained in the methods section of our paper,
our cost study was part of a larger study in which other
researchers investigated the impact of integrated care on
the quality of work and the quality of care. The findings of
the latter study are reported in Vijgen and Boumans (2003).
The authors indicate that especially particular elements of the
quality of care, as experienced by the family members of
residents who received integrated nursing home care, were
higher in comparison to traditional care. Elements include the
living environment, possibilities for residents to relax, treat-
ment of residents and involvement of family members in
decisions on care delivery. The effects on the quality of work
are reported in Boumans et al. (2008). This study shows that
the effects of integrated nursing home care on quality of work
are limited. Our findings and recommendations, combined
with these outcomes, provide a first step in providing infor-
mation that can be used for the development of more cost-
effective care arrangements for older people in nursing homes.
5. Conclusions
The general assumption that integrated care has a cost-
saving potential (per resident or per individual activity) was
only partially supported by our research. Only with respect
to informal care delivery and a set of formal direct care
activities, integrated care was cheaper in comparison with
traditional care. For the practice of care delivery this means
that there may be reasons not to be overly positive about the
cost-saving potential of integrated care. If only because of
this, cost savings should not serve as the sole reason to
promote or implement integrated care. After all, it is always
quality which should come first.
Further researchon integratednursinghomecare isneeded.
Our study indicated that, besides in-depth analyses of the

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–1777 1775
associated costs (including informal care), also the benefits
and underlying integration strategy should be investigated.
Additionally, the factors which can explain possible cost shifts
(such as changing informal–formal care relationships and the
presence of different roles) should be included in future
research. Finally, research on the development of methods
which can capture the dynamic and (methodologically) chal-
lenging features of integrated care is recommendable.
Funding
We obtained financial sources of support from the Dutch
Ministry of Health; The Province of Limburg; VGZ Insurers;
the Boncura Foundation/Care Group ‘Noord-Limburg’; the
Foundation Stimulating Scientific Research on Nursing
Home Care. The resources allowed us to conduct our
research. These financial supporters did not have any role
in determining the study design; the collection, analysis and
interpretation of the data; the writing of the report or the
decision to submit this paper for publication.
Ethical approval
Approval to conduct the study was obtained from the
relevant ethics committees in the nursing homes. Informed
consent forms were used and all participants were informed
before, during and after the research. [The nursing homes did
not use a reference number].
Acknowledgements
The authors would like to thank Femke Keijzer for her
contribution to the data-collection. Furthermore we are
grateful for the financial sources of support that we obtained
from the Dutch Ministry of Health; The Province of Lim-
burg; VGZ Insurers; the Boncura Foundation/Care Group
‘Noord-Limburg’; the Foundation Stimulating Scientific
Research on Nursing Home Care. We are also grateful for
the suggestions and comments provided by the reviewers.
Conflict of interest
None of the authors has been engaged in any relationship
that could have inappropriately influenced this work. There
is no conflict of interest.
References
Aneshensel, C.S., Pearlin, L.I., Mullan, J.T., Zarit, S.H., Whitlatch,
C.J., 1995. Profiles in Caregiving: The Unexpected Career.
Academic Press, San Diego.
Arno, P.S., Levine, C., Memmott, M.M., 1999. The economic value
of informal caregiving. Health Affairs 18 (2), 182–188.
Bass, D.M., Noelker, L.S., Rechlin, L.R., 1996. The moderating
influence of service use on negative caregiving consequences.
The Journals of Gerontology (series B) 51 (3), 121–131.
Bernabei, R., Landi, G., Gambassi, A., Sgadari, A., Zuccala, G., Mor,
V., Rubenstein, L.Z., Carborin, P., 1998. Randomised trial of
impact of model of integrated care and case management for older
people living in the community. BMJ 316 (7141), 1348–1351.
Boumans, N.P., et al., 2008. The effects of integrated care on quality
of work in nursing homes: A quasi-experiment. International
Journal of Nursing Studies 45 (8), 1122–1136.
Burke, T., McKee, J., Wilson, H., Donahue, R., Batenhorst, A.,
Pathak, D., 2000. A comparison of time-and-motion and self-
reporting methods of work measurement. Journal of Nursing
Administration 30 (3), 118–125.
Cardona, P., Tappen, R., Terrill, M., Acosta, M., Eusebe, M., 1997.
Nursing staff time allocation in long-term care: a work-sampling
study. Journal of Nursing Administration 27 (February (2)), 28–
36.
Colyer, H.M., 2004. The construction and development of health
professions: where will it end? Journal of Advanced Nursing 48
(4), 406–412.
De Bekker-Grob, E., 2005. Cost-effectiveness of Integrated Care for
the Elderly: A Systematic Review. Universiteit Maastricht,
Maastricht.
Dorr, D.A., Horn, S.D., Smout, R.J., 2005. Cost analysis of nursing
home registered nurse staffing times. Journal of the American
Geriatrics Society 53 (4), 840–845.
Gaugler, J.E., Anderson, K.A., Zarit, S.H., Perlin, L.I., 2004. Family
involvement in nursing homes: effects on stress and well-being.
Aging and Mental Health 8 (1), 65–75.
Gold, M.R., Siegel, J.E., Russell, L.B., Weinstein, M.C. (Eds.),
1996. Cost-effectiveness in Health and Medicine. Oxford
University Press, Oxford/New York.
Gross, D.L., Temkin-Greener, H., Kunitz, S., Mukamel, D.B., 2004.
The growing pains of integrated health care for the elderly:
lessons from the expansion of PACE. The Milbank Quarterly 82
(2), 257–282.
Hamrick, I., Nye, A.M., Gardner, C.K., 2007. Nursing home med-
ication administration cost minimization analysis. Journal of the
American Medical Directors Association 8 (3), 173–177.
Hendrikson, G., Doddato, T., Kovner, C., 1990. How do nurses use
their time? Journal of Nursing Administration 20 (3), 31–37.
Hernandez, C., et al., 2003. Home hospitalisation of exacerbated
chronic obstructive pulmonary disease patients. The European
Respiratory Journal 21 (1), 58–67.
Johri, M., Beland, F., Bergman, H., 2003. International experiments
in integrated care for the elderly: a synthesis of the evidence.
International Journal of Geriatric Psychiatry 18 (3), 222–235.
Kaplan, R.S., Atkinson, A.A., 1998. Advanced Management
Accounting, 3rd ed. Prentice Hall.
Kaplan, R.S., Cooper, S., 1998. Cost & Effect: Using Integrated Cost
Systems to Drive Profitability and Performance. Harvard Busi-
ness School Press, Boston.
Kodner, D.L., Spreeuwenberg, C., 2002. Integrated care: meaning,
logic, applications, and implications—a discussion paper. Inter-
national Journal of Integrated Care, October–December (e-jour-
nal: retrieved from: http://www.ijic.org).
Kodner, D.L., Kyriacou, C.K., 2000. Fully integrated care for frail
elderly: two American models. International Journal of Inte-
A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–17771776
grated Care 1 (November) (e-journal: retrieved from: http://
www.ijic.org/).
Leichsenring, K., 2004, Developing integrated health and social care
services for older persons in Europe. International Journal of
Integrated Care (September) (e-journal: retrieved from: http://
www.ijic.org).
Leichsenring, K., Alaszewski, A. (Eds.), 2004. Providing Integrated
Health Care and Social Care for Older Persons. A European
View of Issues at Stake. Ashgate Publishing Limited, Aldershot/
England (Public Policy and Social Welfare Series, Volume 28,
European Centre Vienna).
Lemonidou, C., Plati, C., Brokalaki, H., Mantas, J., Lanara, V., 1996.
Allocation of nursing time. Scandinavian Journal of Caring
Sciences 10 (3), 131–136.
Leung, A., Liu, C., Chow, N.W., Chi, I., 2004. Cost-benefit analysis
of a case management project for the community-dwelling frail
elderly in Hong Kong. Journal of Applied Gerontology 23 (1),
70–85.
Leutz, W.N., 1999. Five laws for integrating medical and social
services: lessons from the United States and the United King-
dom. The Milbank Quarterly 77 (1) 77–110, iv-v.
Lyons, K.S., Zarit, S.H., 1999. Formal and informal support: the
great divide. International Journal of Geriatric Psychiatry 14 (3),
183–192 (discussion 192–196).
Minyard, K., Wall, J., Turner, R., 1986. RNs may cost less than you
think. Journal of Nursing Administration 16 (5), 28–34.
Mur-Veeman, I., van Raak, A., Paulus, A., 2008. Comparing inte-
grated care policy in Europe: Does policy matter? Health Policy
85 (2), 172–183.
Newhouse, R., Mills, M., Johantgen, M., Pronovost P., 2003. Is there
a relationship between service integration and differentiation
and patient outcomes? International Journal of Integrated Care 3
(November) (e-journal retrieved from: http://www.ijic.org).
Oostenbrink, J.B., Koopmanschap, M.A., Rutten, F.F.H., 2000. Han-
dleiding voor kostenonderzoek. Methoden en richtlijnen voor
economische evaluaties in de gezondheidszorg (Guide for cost
research. Methods and guidelines for economic evaluation of
health care) College voor Zorgverzekeringen, Amstelveen.
Paulus, A., van Raak, A., Keijzer, F., 2002. ABC: the pathway to
comparison of the costs of integrated care. Public Money and
Management 22 (3), 25–32.
Paulus, A., Boumans, N., Keijzer, F., Vijgen, S., Mur, I., 2003.
Geıntegreerde vraaggestuurde verpleeghuiszorg. Een longitudi-
naal en transversaal onderzoek naar de effecten, kosten en het
proces van verandering van aanbod- naar geıntegreerde vraag-
gestuurde vormen van verpleeghuiszorg (Integrated demand-
oriented nursing home care. A longitudinal and transversal
research of the effects, costs and process of changing from
supply-oriented towards integrated demand-oriented types of
nursing home care). University of Maastricht, Maastricht.
Paulus, A., Van Raak, A., Keijzer, F., 2005. Informal and formal
caregivers’ involvement in nursing home care activities: impact of
integrated care. Journal of Advanced Nursing 49 (4), 354–366.
Paulus, A., Van Raak, A., Keijzer, F., 2006. Nursing home care:
whodunit? Journal of Clinical Nursing 15 (11), 1426–1439.
Paulus, A.T.G., Van Raak, A.J.A., 2008. The impact of integrated
care on direct nursing home care. Health Policy 85 (1), 45–59.
Reed, J., Cook, G., Childs, S., McCormack B., 2005. A literature
review to explore integrated care for older people. International
Journal of Integrated Care 5 (January) (e-journal retrieved from:
http://www.ijic.org).
Reed, J., Childs, S., Cook, G., Hall, A., McCormack, B., 2007.
Integrated care for older people: methodological issues in con-
ducting a systematic literature review. Worldviews on Evidence-
based Nursing 4 (2), 78–85.
Remsburg, R.E., 2004. Pros and cons of using paid feeding assistants
in nursing homes. Geriatric Nursing 25 (3), 176–177.
Robinson, K.M., 1997. Family caregiving: who provides the care,
and at what cost? Nursing Economics 15 (5), 243–247.
Schlenker, R.E., Schaughnessy, P.W., Yslas, I., 1985. Estimating
patient-level nursing home costs. Health Services Research 20
(1), 103–128.
Schuster, G., Cloonan, P., 1989. Nursing activities and reimburse-
ment in clinical care management. Home Health Care Nursing 7
(5), 10–15.
SCP: Sociaal en Cultureel Planbureau, 2005. Ouderen in instellin-
gen. Landelijk overzicht van de leefsituatie van oudere tehuis-
bewoners (Older persons in institutions. An overview of the
living situation of older persons in institutions) Sociaal en
Cultureel Planbureau, Den Haag.
Segal, L., Dunt, D., Day, S.E., Day, N.A., Robertson, I., Hawthorne,
G., 2004. Introducing co-ordinated care (1): a randomised trial
assessing client and cost outcomes. Health Policy 69 (2), 201–213.
SIG, 1994. Gebruikershandboek Gegevensverwerking Verpleeghui-
zen SIVIS (Users’ guide to data processing in nursing homes
SIVIS). Stichting Informatiecentrum voor de Gezondheidszorg,
Utrecht.
Spillman, B.C., Lubitz, J., 2002. New estimates of lifetime nursing
home use: have patterns of use changed? Medical Care 40 (10),
965–975.
Van Raak, A., Mur-Veeman, I., Hardy, B., Steenbergen, M., Paulus,
A. (Eds.), 2003. Integrated Care in Europe. Description and
Comparison of Integrated Care Delivery and its Context in Six
EU Countries. Reed Business Information, Maarssen, The Neth-
erlands.
Vijgen, S.M.C., 2000. Economische evaluatie van informele ver-
pleeghuiszorg. Een vergelijking in zorggroep en patientgroep
(Economic evaluation of informal nursing home care. A com-
parison of care and patient groups) Universiteit Maastricht,
Maastricht.
Vijgen, S., Boumans, N., 2003. Resultaten product deelonderzoek 1:
Effectkenmerken (Results product research project 1: Effect
characteristics). In: Paulus, A., Boumans, N., Keijzer, F., Vijgen,
S., Mur, I., 2003. Geıntegreerde vraaggestuurde verpleeghuis-
zorg. Een longitudinaal en transversaal onderzoek naar de
effecten, kosten en het proces van verandering van aanbod- naar
geıntegreerde vraaggestuurde vormen van verpleeghuiszorg
(Integrated demand-oriented nursing home care. A longitudinal
and transversal research of the effects, costs and process of
changing from supply-oriented towards integrated demand-
oriented types of nursing home care). University of Maastricht,
Maastricht, pp. 147–190 (chapter 6).
Vijgen, S., Tolen, V., Boumans, N., van Mil, A., 2003. Resultaten
product deelonderzoek 1: Ontwerpkenmerken (Results product
research project 1: Design/Implementation characteristics). In:
Paulus, A., Boumans, N., Keijzer, F., Vijgen, S., Mur, I., 2003.
Geıntegreerde vraaggestuurde verpleeghuiszorg. Een longitudi-
naal en transversaal onderzoek naar de effecten, kosten en het
proces van verandering van aanbod- naar geıntegreerde vraag-
gestuurde vormen van verpleeghuiszorg (Integrated demand-
oriented nursing home care. A longitudinal and transversal
research of the effects, costs and process of changing from

A.T.G. Paulus et al. / International Journal of Nursing Studies 45 (2008) 1764–1777 1777
supply-oriented towards integrated demand-oriented types of
nursing home care). University of Maastricht, Maastricht, pp.
113–146 (chapter 5).
Vondeling, H., 2004. Economic evaluation of integrated care: an
introduction. International Journal of Integrated Care 4 (March)
(e-journal retrieved from: http://www.ijic.org).
Wan, T.T.H., Ma, A., Lin, B.Y.J., 2001. Integration and theperformance
of healthcare networks: do integration strategies enhance effi-
ciency, profitability, and image? International Journal of Integrated
Care 1 (June) (e-journal retrieved from: http://www.ijic.org).
Weech-Maldonado, R., Meret-Hanke, L., Neff, M., Mor, V., 2004.
Nurse staffing patterns and quality of care in nursing homes.
Health Care Management Review 29 (2), 107–116.
Weech-Maldonado, R., Shea, D., Mor, V., 2006. The relationship
between quality of care and costs in nursing homes. American
Journal of Medical Quality 21 (1), 40–48.
Whitlatch, C.J., Noelker, L.S., 1996. Caregiving and caring. Ency-
clopedia of Gerontology 1, 253–268.
WHO, 2001 (European Office for Integrated Health Care Services).
Integrated care: A position paper of the WHO European office
for integrated health care services. International Journal of
Integrated Care 1 (June) (e-journal retrieved from: http://www.
ijic.org).
Wimo, A., Von Strauss, E., Nordberg, G., Sassi, F., Johansson, L.,
2002. Time spent on informal and formal caregiving for persons
with dementia in Sweden. Health Policy 61 (3), 255–268.
Recommended

















