Embed Size (px)
Citation preview

DENTAL ANOMALIES
UNDER THE GUIDANCE
OF:DR.M.K.JINDAL
PRESENTED BY:
BUSHRA FARHANBDS 2010 BATCH

DENTAL ANOMALIES
NUMBER SIZE
SHAPE STRUCTURE

ALTERATIONS IN NUMBER OF TEETH
Alteration in tooth number occur usually
during initiation or dental lamina stage of
dental development
The alteration may produce extra or
missing teeth

ANODONTIA
HYPODONTIA
OLIGODONTIA
SUPERNUMERARY TEETH
ANODONTIA
•Congenital absence of teeth
because of failure of development
of tooth germs.
•Total anodontia is rare.
•Partial anodontia (hypodontia) is
more common.


SUPERNUMERARY TEETH Supernumerary teeth are additional
number of teeth, over and above the
usual number for the dentition
Mostly seen in
a. Gardner's syndrome,
b. Cleidocranial dysostosis syndrome
c. Cleft palate (or cleft lip)
CLASSIFICATION
CONICAL
SUPPLEMENTAL
TUBERCULATE
ODONTOME
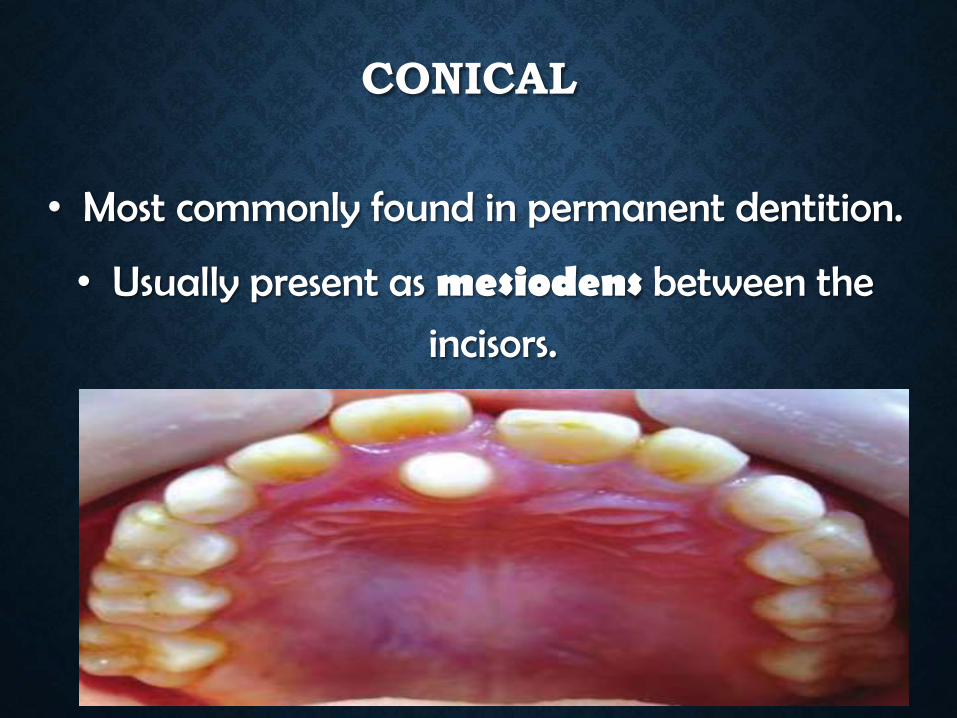
CONICAL
• Most commonly found in permanent dentition.
• Usually present as mesiodens between the
incisors.

TUBERCULATE
• Commonly located on palatal side of
central incisors.
• Possess more than 1 tubercle or cusp.
• Associated with delayed eruption of incisors.

SUPPLEMENTAL
• Duplication of teeth in normal series & found at the end of a tooth series.
• Most commonly found in permanent maxillary lateral incisors.

ALTERATIONS IN SIZE OF TEETH
Alteration in tooth size originate during
the Bell stage or proliferation stage of
tooth development.


MICRODONTIA
• Teeth that are smaller than normal.
• Most commonly affects maxillary lateral
incisors or maxillary third molars.
• Occur in a condition known as pituitary
dwarfism.
• Can cause spacing in primary and
permanent dentition.


MACRODONTIA
• Teeth that are larger than normal
• Hemifacial hypertrophy
• Can cause crowding in primary n
permanent dentition

ALTERATIONS IN SHAPE OF TEETH
•Abnormalities in shape can originate
during the morphodifferentiation stage
of tooth development and are
manifested as alterations in crown and
root form.

FUSION
GEMINATION
CONCRESCENCE
DENS INVAGINATUS(DENS IN DENTE)
DENS EVAGINATUS
TALON CUSP
TAURODONTISM
DILACERATION
HYPERCEMENTOSIS

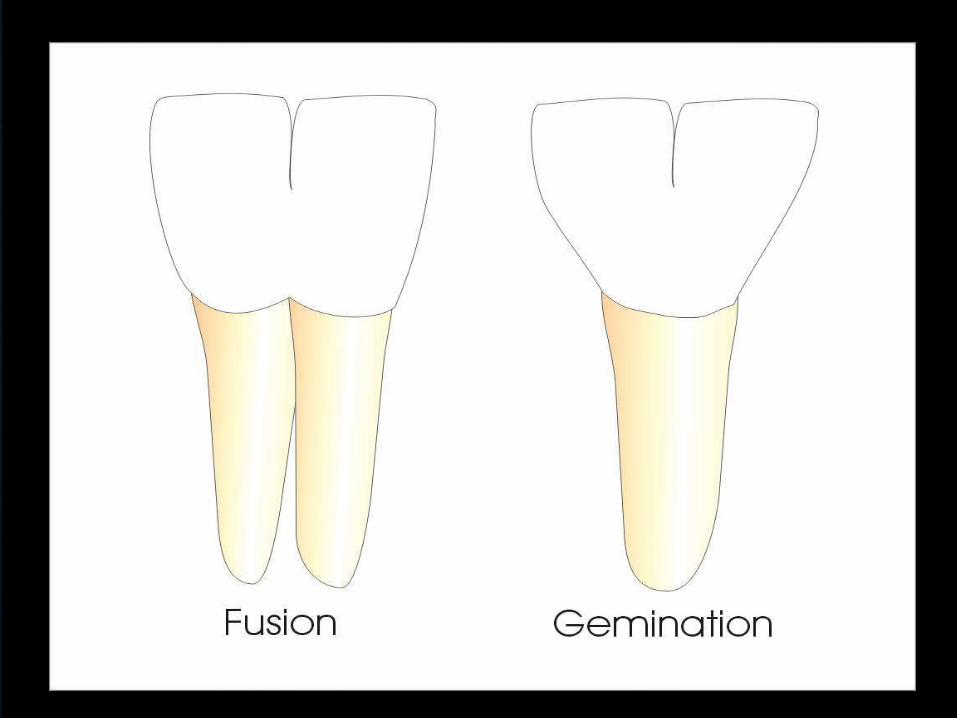
FUSIONUnion of 2 normally separated tooth germs.
Must involve the dentin.
Cause :some physical force or pressure
produces contact of tooth germs.
Early contact: 2 teeth may be completely
united.
Late contact: union of roots only.


GEMINATIONIncomplete attempt of a tooth germ to
divide into two.
Tooth has two crowns or a large crown
partially separated.
Single (common) root and root canal.
Etiology of this condition is unknown


CONCRESCENCEFusion occurring after root formation has
been completed.
Teeth united by their cementum.
Mostly association with the maxillary
second and third molars.
Difficulty in tooth extraction.

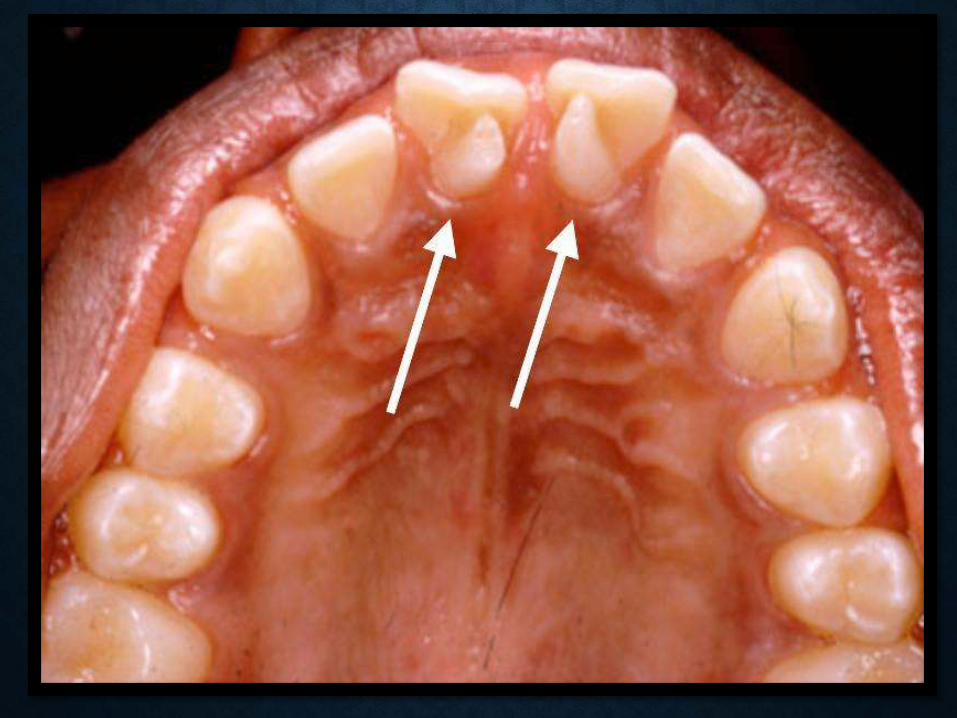
DENS INVAGINATUSInvagination in the surface of tooth crown
before calcification has occurred.
Also called tooth within a tooth.
Can cause development and spread of
dental caries.
Maxillary lateral incisor is the most
frequently affected tooth.


DENS EVAGINATUSTubercle or cusp located in the center of
the occlusal surface.
Affect predominantly premolar and molar
teeth.
Tubercle wears off relatively quickly
causing early exposure of the accessory
pulp horn that extends into the tubercle.



TALON CUSPAccessory cusp located on the lingual
surface of maxillary or mandibular teeth
Pattern resembling an eagle's talon.
Maxillary central or lateral incisor are often
involved

TAURODONTISM Crowns of normal size and shape but have large
rectangular bodies. Pulp chamber is dramatically increased in its
apico-occlusal heights. Apically displaced furcations. Short roots and pulp canals.
Involves molar tooth. Seen in association with amelogenesis imperfecta.Not recognizable clinically but on a radiograph.


DILACERATIONAbnormal bend in the root of a tooth.
Result of trauma to a developing tooth.
Difficulties during extraction or root canal
therapy.


HYPERCEMENTOSISExcessive build-up of cementum around
tooth
Evident on a radiograph
Affects vital teeth
Exact cause not known
Mostly seen in periapical inflammation,
tooth repair and teeth that are not in
occlusion


ALTERATIONS IN STRUCUTRE OF TEETH
AMELOGENESIS IMPERFECTA
DENTINOGENESIS IMPERFECTA
DENTIN DYSPLASIA
ODONTODYSPLASIA
AMELOGENESIS IMPERFECTA• Disturbance in enamel development
•Normal dentin & root
•Etiology: alteration of genes involved in the
process of formation & maturation of the
enamel.
•Three general types


• Defects in matrix formationHYPOPLASTIC
• Defects of matrix structure and of mineral deposition.
HYPOCALCIFIED
• Alterations in enamel rod and rod sheath structures.HYPOMATURE

DENTINOGENESIS IMPERFECTAA hereditary abnormality in the formation of
dentin.
Teeth varies from gray to brownish violet to
yellowish brown color.
Crown fractures easily because of abnormal DEJ.
Pulp chambers and root canals may be partially
or completely obliterated.
Radiographically, the teeth exhibit thin, short
roots.

DENTIN DYSPLASIARare disturbance of dentin formation.
Normal enamel but atypical dentin with
abnormal pulp morphology.
It is subdivided into two types:
TYPE 1 RADICULAR
TYPE 2CORONAL
TYPE 1 (RADICULAR)
Normal color & shape in both dentition.
Exfoliate with little or no trauma.
Short or abnormal roots.
Pulp chambers & canals are usually
obliterated.
20 % of teeth with type I disease have
apical radiolucencies.


TYPE 2 (CORONAL)
Primary dentition appears as in D.I., but
permanent dentition is normal.
Obliteration of the pulp chamber in
deciduous dentition.
Abnormally large pulp chamber in
permanent dentition.
Roots are normal in shape & proportion


ODONTODYSPLASIA
• Hypoplastic & hypocalcified dentin & enamel •central incisors > lateral incisors >canines
(maxillary)•Delayed eruption.
•Ghostlike appearance in image.•Marked reduction in amount of dentin.
•Thin enamel , less dense as usual.



![Anomaly Detection: Principles, Benchmarking, Explanation ...web.engr.oregonstate.edu/~tgd/...anomaly-detection... · Towards a Theory of Anomaly Detection [Siddiqui, et al.; UAI 2016]](https://img.dokumen.tips/doc/110x75/5fd8992320a65f059c333c6d/anomaly-detection-principles-benchmarking-explanation-webengr-tgdanomaly-detection.jpg)







![Deep Anomaly Detection - AiFrenzAI Friends]Deep Anomaly... · Deep Anomaly Detection Kang, Min-Guk Mingukkang1994@gmail.com Jan. 16, 2019 1/47](https://img.dokumen.tips/doc/110x75/5fb2a9a0b51b275c5a47b39a/deep-anomaly-detection-aifrenz-ai-friendsdeep-anomaly-deep-anomaly-detection.jpg)