Embed Size (px)
Citation preview

Principles of “Targeted Therapy”

• Thanks to recent acquisitions in the field of molecular biology it has been possible to identify new biological targets expressed by tumor cells
• Using drugs directed against these targets it is possible to hit, in a “targeted way” these cells
• One of the most studied target is the Epidermal Growth Factor Receptor (EGFR)
TARGETED-THERAPY

• Signal transduction inhibitors
• Proteasomes inhibitors (Multiple Myeloma)
• Cox-2 inhibitors (Colon Poliposis)
• Vaccines, immunotherapy and gene therapy
TARGETED THERAPY IN CANCER

Nat Rev Cancer. 2009 Jan;9(1):28-39.
Targeting cancer with small molecule kinase inhibitors.
Zhang J, Yang PL, Gray NS.
Deregulation of kinase activity has emerged as a major mechanism by which cancer cells evade normal physiological constraints on growth and survival. To date, 11 kinase inhibitors have received US Food and Drug Administration approval as cancer treatments, and there are considerable efforts to develop selective small molecule inhibitors for a host of other kinases that are implicated in cancer and other diseases. Herein we discuss the current challenges in the field, such as designing selective inhibitors and developing strategies to overcome resistance mutations. This Review provides a broad overview of some of the approaches currently used to discover and characterize new kinase inhibitors.
FURTHER READING

MetastasisProliferation
Cell-cycle progression
pY
pYK K
pY
M
G1S
G2
Growth factor
SIGNAL TRANSDUCTION INHIBITORS

• EGFR Inhibitors– Gefitinib (Iressa)– Erlotinib (Tarceva)
• EGFR Monoclonal antibodies– Cetuximab (Erbitux)
• VEGF Monoclonal antibodies– Bevacizumab (Avastin)
TARGETED THERAPIES

EGF VEGFBevacizumab
GefitinibErlonitib
AZD(TK inhibitor)
Cetuximab

myc cyclin D1
Jun Fos
RRRR
RR
K
KK
Gene transcriptionGene transcription
RR
K
EGFR SIGNALING

myc cyclin D1
Jun Fos
RRRR
KRR
K
RR
K
MAPKMAPK
MEKMEK
RASRAS RAFRAF
SOSSOS
GRB2GRB2PI3-KPI3-K
AKTAKT
Proliferation
Inhibition of apoptosis
KPPPP
PPPP
PPPP
MetastasisAngiogenesis
GEFITINIB
Gene transcriptionGene transcription
EGFR SIGNALING

Iressa received accelerated FDA approval in May 2003 as a 3rd line therapy in NSCLC
based on the IDEAL-2 study.
GEFITINIB (IRESSA®)

0
10
20
30
40
5060
70
80
90
100
Pazienti
Perce
ntuale
di ri
spos
ta
Totale
Donne conadenocarcinomanon fumatrici
0
10
20
30
40
50
60
70
80
90
100
Pazienti
Perce
ntuale
di ri
spos
ta
Uomini
Donne
Adenocarcinoma
Non fumatori
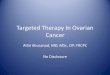
IRESSA®: results in different subgroups of patients with NSLC

pre-treatment post-treatment
RESULTS (I)

pre-treatment post-treatment
RESULTS (II)

• The efficacy of GEFITINIB is limited to a subset of patients (nonsmoker women affected by adenocarcinoma)
• The overall response rate is 7%• In nonsmoker women with adenocarcinoma the response
rate reaches 50%• Gefitinib toxicity is lower with respect to that observed
with conventional chemotherapy
CONCLUSIONS

myc cyclin D1
Jun Fos
RRRR
KRR
K
RR
K
MAPKMAPK
MEKMEK
RASRAS RAFRAF
SOSSOS
GRB2GRB2PI3-KPI3-K
AKTAKT
Proliferation
Inhibition of apoptosis
KPPPP
PPPP
PPPP
MetastasisAngiogenesis
ERLOTINIB
Gene transcriptionGene transcription
EGFR SIGNALING

Tarceva
(n=488)
Placebo
(n=243)
Resp. Rate 8.9% <1%
Median survival
6.7 mo 4.7 mo
PFS* 2.2 mo 1.8 mo
Shepherd FA et al. NEJM 2005
Most common AE: rash, diarrhea
*sopravvivenza libera da progressione
ERLOTINIB (TARCEVA®) IN NSLC
Tarceva received FDA approval in 2004 as a 2nd or 3rd line therapy in NSCLC based on Shepherd’s trial.
* Progression Free Survaival

• TALENT trial - Cisplatin/gemcitabine + (tarceva or placebo) - Phase III– 1172 pts., previously untreated
Tarceva Placebo
Med. survival (days)
301 309
TTP* (days) 167 179
Gatzemeier U. ASCO 2004 Abstract
*intervallo per ripresa di progressione tumorale
* Time To Progression
ERLOTINIB (TARCEVA®) IN NSLC

Group RR (%) p
Women v men 19 v 3 0.001
Japanese v
non-Japanese27.5 v 10.4 0.0023
Adenocarcinoma v others
13 v 4 0.046
BAC* v adeno 38 v 14 <0.001
Never smoker v current/former
36 v 8 <0.001
Fukuoka JCO 2003;21:2237-46. Kris JAMA 2003;290:2149-58. Miller JCO 2004;22:1103-09.* Bronchioloalveolar carcinoma
PREDICTORS OF RESPONSE TO TK INHIBITORS IN NSCLC


Pao et al. JCO 2005; 23:2556-2568.

Some patients have significant initial clinical response to TK Inhibitors, but then develop progressive disease– Secondary mutation found (4/7 pts.)
• Substitution of methionine for threonine at position 790
• Get steric hindrance of TK Inhibitor binding
Pao et al. 2005; PLoS Med 2:1-11.Kobayashi et al. 2005; NEJM 352:786-92.
ACQUIRED RESISTANCE TO TK INHIBITORS

OTHER MUTATIONS
Pao et al. JCO 2005; 23:2556-2568.
Mutation

• Mutations in K-ras– Occur in 15-30% of lung adenocarcinomas– High incidence in heavy smokers
• Predict a poor response to TK inhibitors
• EGFR and K-ras mutations are mutually exclusive
Ahrendt SA et al. Cancer 2001; 92:1525-30.Kosaka T et al. Cancer Res 2004; 64: 8919-23.Eberhard DA et al. JCO 2005;23:5900-09.
MUTATIONS IN K-ras

• Many centers have started testing for the most common mutations in EGFR
• Problem: • What to do if negative for mutations?
– Some pts. with responses to Gefitinib/Erlotinib have no detectable EGFR mutation
MUTATIONAL PROFILING

ANTI EGFR MONOCLONAL ANTIBODIES
Pao et al. JCO 2005; 23:2556-2568.
mAb (CETUXIMAB)

RR (%)
(CI)
Median survival
(mo.)
Median TTP* (mo.)
Cisplatin/Vinor.20
(7.6-32.4)7.0 4.2
Cisplatin/Vinor.
+Erbitux
32
(17.5-46.0)8.3 4.7
Rosell 2004 ASCO Abstract
CETUXIMAB WITH CHEMO: RESULTS
RR: response rateTTP: time to progression

Survivalin circulationIntravasation
Invasion
initiationof growth
Sustainedgrowth
Primarytumour
Clinicallyevident metastasis
Adapted from Chambers A, Matrisian L. J Natl Cancer Inst 1997;89:1260–70
ANGIOGENESIS:MULTIPLE STEPS IN CANCER BIOLOGY

Sustained Growth requires blood vessels
Primarytumor
Metastasis
VEGF
EGF
Multiple steps in cancer biology Heading towards Personalized Care

ANGIOGENESIS

ANGIOGENESIS IN TUMORS

Endostatin is a natural antiangiogenic protein that inhibits the growth of blood vessels
Vaccines targeting tumor angiogenesis—a novel strategy for cancer immunotherapy Y. Okaji et al, 2006
ANGIOGENESIS INHIBITION

Nature Reviews Drug Discovery 4, 448-449 (2005)
Anti-angiogenesi (II)Anti-angiogenesi (II)
Bevacizumab (Avastin, Genetech): Vascular Endothelial Growth factor (VEGF) inhibitor.Phase III Trial in NSCLC:- Survival of 12.5 months in Avastatina/CHT arm vs. 10.5 months in conventional CHT arm - 2 years survival: 22% vs. 17%- Adverse events: 5% major bleedings, 1% mortality

Avastin + ChemoAvastin + Chemo
Carbo/Taxol
(n=32)
Carbo/Taxol + Avastin
(n=35)
Median survival
(mo.)14.9 17.7 (NS)
RR (%) 18.8 31.5
TTP* (mo.) 4.2 7.4Johnson et al., JCO 2004.Johnson et al., JCO 2004.(19/32 pts. crossed over)
Avastin in combination with Tarceva appears to have a synergistic effect*intervallo per ripresa di progressione tumorale

Animal Model to study angiogenesis

Growth Factor Reduced BD Matrigel Matrix
Storage -30°C
Melting +4°C
Solidification +37°C
Matrigel is an extracellular matrix produced by murine sarcoma Engelbreth-Holm-Swarm (EHS), consisting predominantly of laminin (60%), collagen IV (30%),heparan sulphate (5%), proteoglycans (3 %) and entactin (1%).

• Matrigel subcutaneous injection (the matrix can be mixed with different molecules to be studied).
• After the injection, thanks to body temperature, the matrix solidifies and leads to the formation of “plugs”. With appropriate stimuli the angiogenic process starts and develops into the plugs.
Model for in vivo study of angiogenesis using Matrigel Matrix

MATRIGEL PLUGS

Reperimento dei plugs dopo 7 giorni dall’inoculo
sezione addominale lungo la linea mediana
isolamento masserelle dai tessuti
conservazione del materiale in apposite biocassette
Allestimento sezioni istologiche fissazione in formalina
inclusione in paraffina
taglio con microtomo
allestimento vetrino
colorazione

RESULTS EVALUATION

NEGATIVE CONTROLS
MATRIGEL MATRIGEL + Gas 6