Embed Size (px)
Citation preview
End Tidal CO2 (EtCO2) Monitoring:
Using EtCO2 Monitoring in the Home-Setting For Patients With Neuromuscular Disease
DO
C1
11
84
17

Agenda
• What are the benefits of CO2 monitoring?
• The basics of CO2 monitoring
• What capnograms can tell• Clinical Application in ALS & Other
Neuromuscular Diseases• Summary• FAQ’s

Nonin hand-held side-stream sampling technology ~$1100.00
Smith’s Medical BCI Capnocheck II hand-held side-stream technology~ $1700.00 - $1900.00

Oridian and Nellcor portable hand-held devices – side-stream sampling technology

BREAS VIVO 50 mainstream device~ $2500.00


DataScope Transcutaneous monitor $4495.00 refurbished
Transcutaneous CO2 Monitoring
The Accuracy of Transcutaneous PCO2 in Subjects With Severe Brain Injury: A Comparison With End-Tidal PCO2
Sebastien Rosier, Yoann Launey, Jean-Paul Bleichner, Bruno Laviolle, Alice Jouve, Yannick Malledant, Philippe Seguin
BACKGROUND: In patients suffering from brain injury, end-tidal PCO2(PETCO2) monitoring is controversial, but transcutaneous PCO2 (PtcCO2), which is noninvasive and utilizes immediate display, may be an alternative method. We hypothesized that PtcCO2 would be more accurate than PETCO2 for monitoring PaCO2 in patients with severe brain injury.METHODS: A prospective observational study included consecutive mechanically ventilated adult subjects who had acute brain injury and an arterial catheter in place. When an arterial blood gas analysis was required, the PETCO2 and PtcCO2 values were simultaneously recorded. The agreement between the PETCO2, PtcCO2, and PaCO2 measurements (reference) was determined using the Bland-Altman method. The number of outliers defined by the formula ([PETCO2 or PtcCO2] − PaCO2) > ± 4 mm Hg indicated the proportion of measurements that were considered clinically unacceptable.RESULTS: A total of 25 subjects were included in the study, and 85 simultaneous measurements of PaCO2, PtcCO2, and PETCO2 were obtained. The bias and precision between PaCO2 and PtcCO2 were −0.75 and 6.23 mm Hg, respectively. The limits of agreement ranged from −12.97 to 11.47 mm Hg. The bias and precision between PaCO2 and PETCO2 were 0.68 and 5.82 mm Hg, respectively. The limits of agreement ranged from −10.72 to 12.08 mm Hg. There were 34 (40%) outliers for the PtcCO2 sensor and 34 (40%) outliers for the PETCO2 sensor (P > .99).CONCLUSIONS: The accuracy of PtcCO2 was not superior to that of PEtCO2 for assessing PCO2 levels and should not be used to monitor these levels in subjects with severe brain injury.

Mainstream or Sidestream Capnography?TECHNICAL CONSIDERATIONSMichael B. Jaffe, PhDRespironics Novametrix, Inc., Wallingford CT
• Infrared measurement of carbon dioxide monitoring (capnography) dates back to the 1940’s
• A capnometer, by definition is either diverting (i.e., sidestream) or non-diverting (i.e., mainstream). • A diverting capnometer transports a portion of a patient’s
respired gases from the sampling site, through a sampling tube, to the sensor
• a non-diverting capnometer does not transport gas away from the sampling site
• one can view the difference between mainstream (non-diverting) capnography and sidestream (diverting) capnography as clinically measuring carbon dioxide at the sample site versus measuring carbon dioxide in the monitor distant from the sample site.

Mainstream or Sidestream Capnography?TECHNICAL CONSIDERATIONSMichael B. Jaffe, PhDRespironics Novametrix, Inc., Wallingford CT
The measurement of the partial pressure of a gas significantlydistant from the sampling site raises a number of “laws ofphysics” issues including:
(1) water removal (2) different conditions at the sampling site and sample cell in
terms of temperature and humidity (3) mixing of the sample gas as it is drawn through the cell, (4) variable pressure drop across the tubing and the possible misrepresentation of the partial pressure values
due to the above and other effects (5) dynamic distortions to the waveform.
While some of these effects can be compensated for or corrected by othermeasurements or by the assumption of nominal values, other effects cannot.
Mainstream or Sidestream Capnography?TECHNICAL CONSIDERATIONSMichael B. Jaffe, PhDRespironics Novametrix, Inc., Wallingford CT
• With mainstream devices, the sensor consisting of the sample cell and infrared bench is placed at the airway. This location results in a “crisp” graphical representation of the time varying CO2 value (capnogram) that reflects in real-time the partial pressure of carbon dioxide within the airway.
• A detailed study of adverse events found that capnography was critical for the detection of general anesthesia incidents. The study also reported failures of capnography to detect problems when it should have and it was noted that about a third of these failures were due to problems with sidestream gas sampling and a third due to the improper setting of alarms.
Why EtCO2 Monitoring?
ISO Standard 10651-2, Part 2, “Home care ventilators for ventilator-dependent patients,” states that either EtCO2 monitoring or exhaled tidal volume or minute volume monitoring is required.
EtCO2 monitoring may be a better clinical indicator of patient ventilation than the exhaled tidal volume or minute volume measurement because it measures alveolar ventilation
Capnography in Critical Care MedicineEugene Y. Cheng, Harvey Woehlck, Anthony J. Mazzeo Journal of Intensive Care Medicine 01/1997; 12(1):18-32. DOI: 10.1177/088506669701200103
ABSTRACT
Capnography is a noninvasive method of monitoring exhaled CO2 and is used in many situations as a reflection of arterial CO2 concentration. Expired CO2 can be accurately measured using infrared spectrometry, mass spectrometry, and Raman scattering. Colorimetric CO2 detectors are useful as a qualitive indicator of the presence of CO2. Trending end-tidal CO2 and analysis of the capnographic wave form can provide information on changes in a patient's cardiopulmonary status or malfunction of equipment used to support a patient's cardiovascular or pulmonary systems. The accuracy of end-tidal CO2 measurements as a reflection of arterial CO2 tension in critically ill patients with respiratory or cardiovascular problems is limited.

Capnography in Critical Care MedicineEugene Y. Cheng, Harvey Woehlck, Anthony J. Mazzeo Journal of Intensive Care Medicine 01/1997; 12(1):18-32. DOI: 10.1177/088506669701200103
Changes in deadspace, respiratory rate and depth, positive end-expiratory pressure, aveolar circulation, and cardiac output can significantly impact end-tidal CO2 values more than arterial CO2 concentrations. With marked changes in end-tidal CO2 that are of concern, arterial blood gas analysis should be obtained to determine if the end-tidal CO2 measurement is representative of a change in arterial CO2 concentrations. Despite the limitations of end-tidal CO2 as a reflection of arterial CO2, it is still useful as a noninvasive monitor to alert clinicians of potential changes in a patient's cardiopulmonary condition.

EtCO2 and COPD
Comparison of the End-Tidal and Arterial PCO2 Gradient During Exercise in Normal Subjects and in Patients With Severe COPD Zhi Liu; Francisco Vargas; David Stansbury; Scott A. Sasse; Richard W. Light
Conclusion: • during exercise, the P(ET-a) CO2 gradient in
normal subjects and in patients with COPD increases significantly,
• the P(ET-a) CO2 gradient is more closely correlated with the VD/VT than any other physiologic variable, and
• changes in the PETCO2 during exercise are not correlated closely with changes in the PaCO2.

Correlation of End Tidal Carbon Dioxide and Arterial Carbon Dioxide in Premature Infants2005 Study by John Emberger BS RRT, Robert Locke DO, Michael Western AS RRT, Departments of Respiratory Care and Neonatology, Christiana Care Health System, Newark, DE
Respiratory Care Journal 2005 Open Forum Abstracts
Conclusions:
• EtCO2 correlated very closely to PaCO2
• EtCO2 monitoring may be an accurate non-invasive method of trending PaCO2 in this population
• EtCO2 monitoring may be a safe, non-invasive method for reducing the number of blood gas measurements as well as providing real-time PaCO2 information to the clinician in mechanically ventilated premature infants
END-TIDAL CARBON DIOXIDE MONITORING IN PATIENT CONTROLLED ANALGESIAA 2007 Open Forum Abstract published in the Respiratory Care Journal by T. McCarter,Z.Shaik, K. Scarfo, T. LauraConclusions:
• Relying on pulse oximetry alone is potentially dangerous as it reflects oxygenation status of the patient rather than effective ventilation
• The risk of respiratory depression in the setting of PCA warrants a technology that can measure the RR, EtCO2 concentration and depict it in a wave form
• Direct monitoring of respiratory rate and exhaled CO2 concentration with capnography is more effective in the detection of respiratory depression than the monitoring of oxygenation alone
• While pulse oximetry monitors oxygenation, capnography monitors respiratory rate and effectiveness of ventilation
• Changes in pulse oximetry may lag behind changes in respiratory rates
• The patients saved might have otherwise suffered negative respiratory events and/or depression requiring additional interventions and services were they not monitored by this technology.
End-Tidal and Arterial Carbon Dioxide MeasurementsCorrelate Across All Levels of Physiologic Dead SpaceStudy done by S David McSwain MD, Donna S Hamel RRT FAARC, P Brian Smith MD, Michael A Gentile RRT FAARC, Saumini Srinivasan MD, Jon N Meliones MD, and Ira M Cheifetz MD FAARC
Respiratory Care Journal, March 1, 2010 vol 55 no. 3 288-293
Conclusion:
• We found moderate to strong positive linear correlation coefficients between EtCO2 and PaCO2 for all 4 VD/Vt ranges although the strength of the correlations decreased slightly as VD/Vt increased

Capnography for Assessing Nocturnal Hypoventilation and Predicting Compliance with Subsequent Noninvasive Ventilation in Patients with ALS
Sung-Min Kim, Kyung Seok Park, Hyunwoo Nam, Suk-Won Ahn, Suhyun Kim
• Patients with amyotrophic lateral sclerosis (ALS) suffer from hypoventilation, which can easily worsen during sleep. This study evaluated the efficacy of capnography monitoring in patients with ALS for assessing nocturnal hypoventilation and predicting good compliance with subsequent noninvasive ventilation (NIV) treatment.
• Nocturnal monitoring and brief wake screening by capnography/pulse oximetry, functional scores, and other respiratory signs were assessed in 26 patients with ALS. Twenty-one of these patients were treated with NIV and had their treatment compliance evaluated.
• Capnography is an efficient tool for assessing nocturnal hypoventilation and predicting good compliance with subsequent NIV treatment of ALS patients, and may prove useful as an adjunctive tool for assessing the need for NIV treatment in these patients.

Respiratory Management of ALS Lee Guion 2010, p.124-125
“Elevated EtCO2 occurs with hypercapnia in spontaneously breathing patients. Daytime hypercapnia as an indicator of hypoventilation in ALS has yet to be studied, but it has the potential for detecting early respiratory insufficiency. EtCO2 correlates well with PaCO2 in the absence of lung or cardiovascular disease (Morely, et.al., 1993)”

• CO2 monitoring improves quality of life for patients with respiratory muscular disorders
• NIV of patients with muscular disorders (e.g. DMD) which cause pulmonary complications and increased risk of sleep-disordered breathing may improve quality of life and reduce a high morbidity and early mortality.
• The ATS states in Consensus statement on respiratory care of the patient with DMD that an annual PSG with continuous non-invasive gas monitoring is ideal.
• PSG is time-consuming and costly, but useful information may also be obtained by night SpO2 and EtCO2 monitoring if PSG is not available.
Indications and outcomes of non-invasive ventilatory support in restrictive and obstructive disorders. Winck JC, Simons AK in: Ambrosino N, Goldstein RS. Ventilatory support for chronic respiratory failure. New York: Informa Healthcare USA, Inc, 2008; 225, 17: 211-30.
Respiratory monitoring in neuromuscular disease — capnographyas an additional toolSylvia Kotterba, Tanja Patzold, Jean-Pierre Malin, Maritta Orth, Kurt Rasche
AbstractDaytime complaints like fatigue, sleepiness and cognitive dysfunction in neuromuscular disease can be due to nocturnal hypercapnia and hypoxemia. Daytime respiratory diagnostics does not reflect sleep disordered breathing. Nocturnal pulse oxymetry and capnography were performed in 11 patients (15–75 years old) with different slowly progressive neuromuscular diseases. Only four patients complained of dyspnea. Pulmonary function was abnormal in three patients. Blood gas samples showed a hypoxemia in three patients. Pulse oxymetry results were pathological in six patients. Nine patients presented abnormal capnographies. According to these results either nocturnal oxygen application was initiated or ventilatory parameters were modified. Daytime symptoms and muscular strength improved markedly.
Capnography and pulse oxymetry should be performed during the course of neuromuscular disease to detect respiratory insufficiency. Capnography seems to be a more sensitive indicator for respiratory impairment especially when artificial ventilation has been initiated. © 2001 Elsevier Science B.V.

What are the benefits of CO2 monitoring?
• Capnography directly measures the ventilatory performance of the lungs, hyper/hypoventilation or rebreathing is quickly detected
• CO2 monitoring provides continuous measurements, registering any fluctuations over a longer period (e.g. nocturnal fluctuations)
• CO2 monitoring contributes to improved decision making and quicker treatment adjustments
• CO2 monitoring can now be done easily at home, e.g. to verify the treatment during the first days after discharge to the home
• Gives a rapid and reliable method to detect life-threatening conditions such as malposition of tracheal tubes, ventilatory failure and defective breathing circuits
• Main stream CO2 monitoring is a well proven1, easy to use, robust and cost-effective method
Increasing insight in the quality of ventilation!
1. Jaffe, MB, Anesth Analg 2008;107:890 – 904.

The basics of CO2 monitoring
Normal Physiological values :
During cellular metabolism O2 and food are converted into energy and consumed by the tissue. The by-product of metabolism is Carbon Dioxide
CO2 is transported by the venous blood and carried back to the lungs
Exhaled air is the “final common path” for a complex system of CO2 production, cardiovascular transport, lung perfusion, and respiratory ventilation.
Lung diseases causing incomplete alveolar emptying or ventilation/ perfusion mismatch will impact the CO2 elimination
(Mechanical) Ventilation will move the ambient air into the alveoli of the lungs and eliminate the CO2 out of the lungs with the exhaled gasflow.
Source: PhaseIn sales guide
Metabolism
Cardiac function
Lung function
Ventilation
CO2
Arterial End Tidal
35 – 45mmHg 30 – 43mmHg
4.7 – 6.0kPa 4.0 – 5.7kPa
4.6 – 5.9% 4.0 – 5.6%
CO2
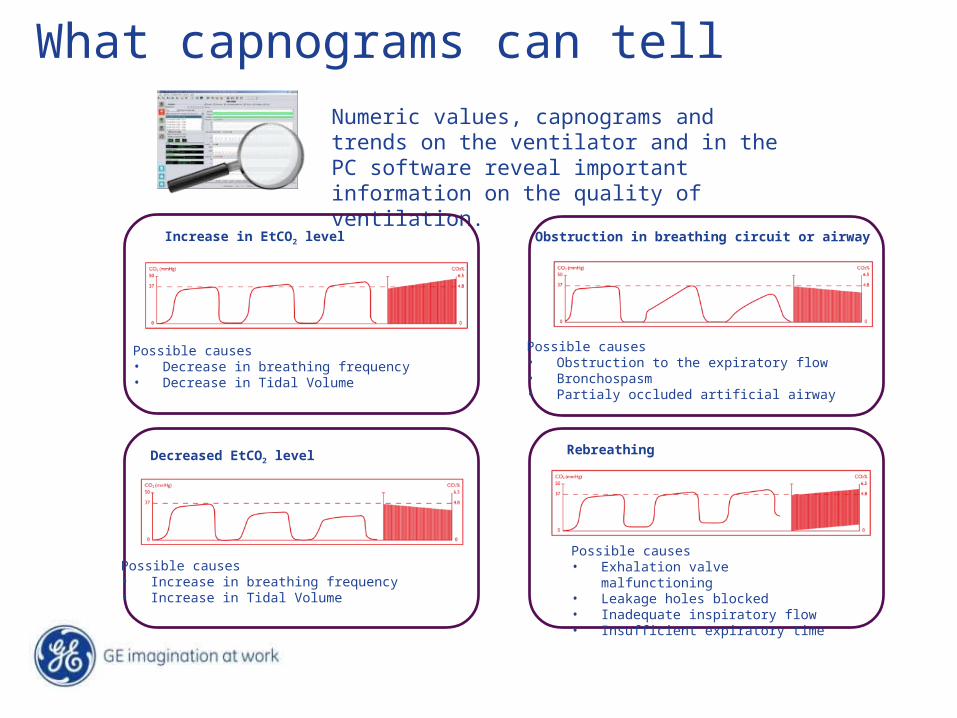
What capnograms can tell
Possible causes• Decrease in breathing frequency • Decrease in Tidal Volume
Increase in EtCO2 level
Numeric values, capnograms and trends on the ventilator and in the PC software reveal important information on the quality of ventilation.
An decrease in EtCO2 level
Possible causes• Increase in breathing frequency • Increase in Tidal Volume
Possible causes• Obstruction to the expiratory flow• Bronchospasm• Partialy occluded artificial airway
Obstruction in breathing circuit or airway
Rebreathing
Possible causes• Exhalation valve malfunctioning • Leakage holes blocked• Inadequate inspiratory flow • Insufficient expiratory time
Decreased EtCO2 level
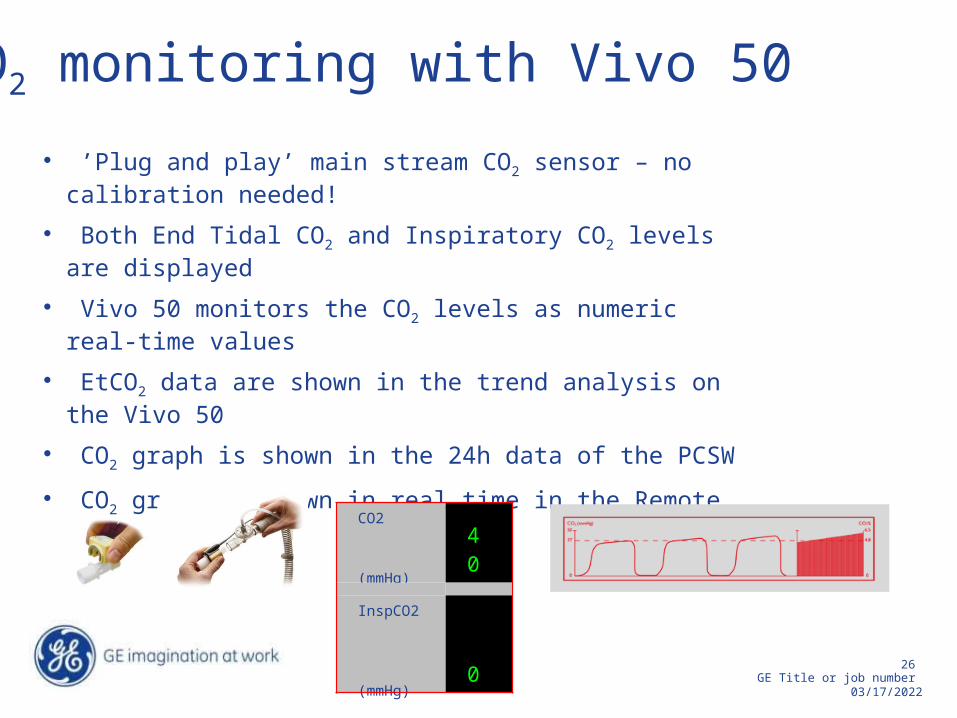
• ’Plug and play’ main stream CO2 sensor – no calibration needed!
• Both End Tidal CO2 and Inspiratory CO2 levels are displayed
• Vivo 50 monitors the CO2 levels as numeric real-time values
• EtCO2 data are shown in the trend analysis on the Vivo 50
• CO2 graph is shown in the 24h data of the PCSW
• CO2 graph is shown in real time in the Remote Monitoring PCSW
CO2 (mmHg)
40
InspCO2 (mmHg) 0
CO2 monitoring with Vivo 50

One-Two Punch in Monitoring
Physiological measurements are usually a much better indicator of the patient’s condition than measuring exhaled volumes
EtCO2 monitoring combined with SpO2 monitoring may give a much better indicator of alveolar ventilation and perfusion than monitoring the exhaled tidal or minute volume alone and may alert the clinician to an impending problem quicker

AARC Clinical Practice GuidelineCapnography/Capnometry during Mechanical Ventilation—2003 Revision & Update 4.0 INDICATIONS:
On the basis of available evidence, capnography should not be mandated for all patients receiving mechanical ventilatory support, but it may be indicated for:
4.1 Evaluation of the exhaled CO2, especially end-tidal CO2, which is the maximum partial pressure of CO2 exhaled during a tidal breath (just prior to the beginning of inspiration) and is designated PetCO2
4 . 2 Monitoring severity of pulmonary disease and evaluating response to therapy, especially therapy intended to improve the ratio of dead space to tidal volume (VD/VT) and the matching of ventilation to perfusion (V/Q) and , possibly, to increase coronary blood flow

AARC Clinical Practice Guideline (cont)4.4 Continued monitoring of the integrity of the ventilatory circuit, including the artificial airway
4 . 5 Evaluation of the efficiency of mechanical ventilatory support by determination of the difference between the arterial partial pressure for CO2 (PaCO2) and the PetCO2
4 . 6 Monitoring adequacy of pulmonary, systemic, and coronary blood flow
4.8 Graphic evaluation of the ventilator-patient interface; evaluation of the shape of the capnogram may be useful in detecting rebreathing of CO2, obstructive pulmonary disease, waning neuromuscular blockade (‘curare cleft’), cardiogenic oscillations, esophageal intubation, cardiac arrest, and contamination of the monitor or sampling line with secretions or mucus
4 . 9 Measurement of the volume of CO2 elimination to assess metabolic rate and/or alveolar ventilation

AARC Clinical Practice Guideline (cont)CO2 MV 7.0 LIMITATIONS OF PROCEDURE OR DEVICE:
Capnography, when performed using a device calibrated and operated as recommended by the manufacturer, has few limitations.
It is important to note that although the capnograph provides valuable information about the efficiency of ventilation (as well as pulmonary, systemic, and coronary perfusion), it is not a replacement or substitute for assessing the PaCO2.
The difference between PetCO2 and PaCO2 increases as dead
space volume increases.
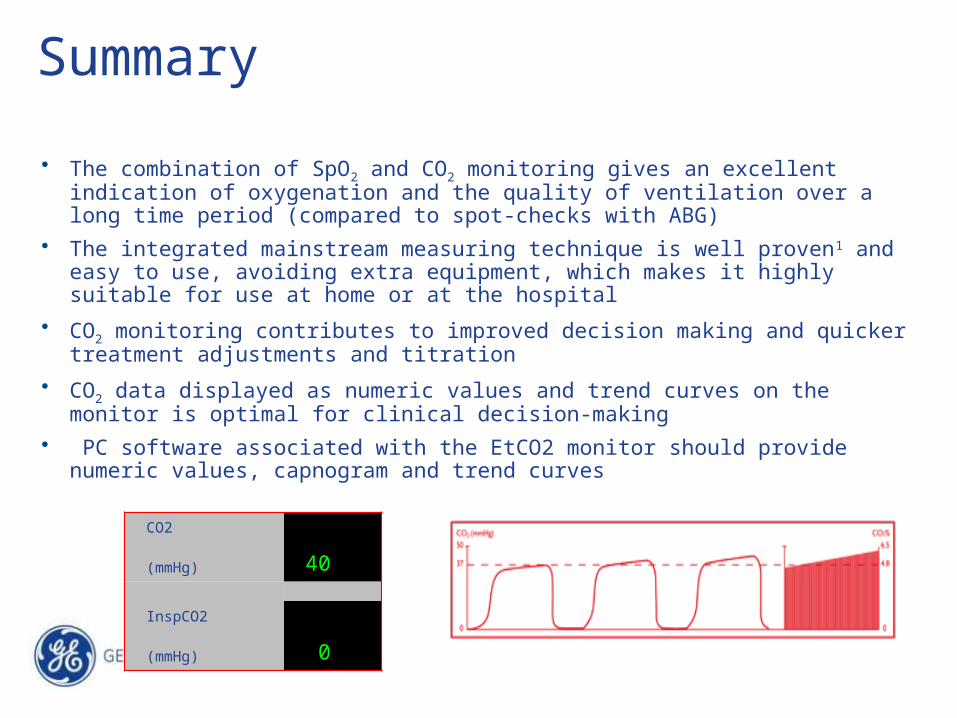
Summary
• The combination of SpO2 and CO2 monitoring gives an excellent indication of oxygenation and the quality of ventilation over a long time period (compared to spot-checks with ABG)
• The integrated mainstream measuring technique is well proven1 and easy to use, avoiding extra equipment, which makes it highly suitable for use at home or at the hospital
• CO2 monitoring contributes to improved decision making and quicker treatment adjustments and titration
• CO2 data displayed as numeric values and trend curves on the monitor is optimal for clinical decision-making
• PC software associated with the EtCO2 monitor should provide numeric values, capnogram and trend curves
CO2 (mmHg) 40
InspCO2 (mmHg) 0

Q&AQuestion Answer
What is the best location for sampling or measuring the end-tidal carbon dioxide concentration in an intubated patient?
Regardless of the type of sampling technique, place the airway adapter or sampling port as close as possible to the patient’s airway.
What is the clinical significance for advocating monitoring of the end-tidal carbon dioxide levels?
The ideal end-tidal carbon dioxide monitor provides both numeric and graphic waveform displays. The display on the monitor represents the highest concentration of carbon dioxide reached at the end of exhalation and is assumed to represent alveolar gas, which under normal ventilation-perfusion matching in the lungs closely parallels arterial levels of carbon dioxide. Thus, the end-tidal carbon dioxide tension (EtCO2) is thought to be a non-invasive estimate of the patient’s alveolar ventilation status by its close correlation with arterial carbon dioxide tension (PaCO2) under normal conditions.
Can capnographic waveform displays provide clinically useful information independent of the numerical end-tidal carbon dioxide reading?
It is important to recognize that clinicians should never accept any EtCO2 value without first determining the quality of the capnogram or end-tidal carbon dioxide waveform. In those situations where the EtCO2 numerical value is of questionable benefit, inspection of the waveform tracings alone has the potential to provide the clinician with useful information.
Why use EtCO2 monitoring when ABG is avaliable?
EtCO2 monitoring is a complement to ABG providing continous monitoring and quick response. ABG sample collection & analysis is not practical for homecare.

Q&AQuestion Answer
Why did Breas choose end-tidal CO2 in stead of transcutaneous CO2 for the Vivo 50?
Since the Vivo 50 is a ventilator designed for use in the home environment, we choose a robust, simple and cost effective method. The EtCO2 sensor is light, easy to install and does not need calibration.
Can EtCO2 be used with any type of patient?
EtCO2 is most suitable for the follow up of patients suffering from restrictive diseases or with a decreased respiratory drive. The correlation between arterial CO2 levels is less for patients suffering from airway diseases such as COPD and in these cases other methods of measuring CO2 might be considered.
How do major leaks or episodes of asynchronisation affect EtCO2 measurements?
Accurate EtCO2 measurements depend on proper ventilation. In case a major leak or a period of asynchronization occurs, ventilator settings and mask fitting must be checked to restore proper ventilation. The Vivo 50 will alarm in these situations to warn the user about the ongoing events. Once proper ventilation is restored, EtCO2 measurements will turn back to normal.
Does the sensor used with Vivo 50 need calibration?
The sensor does not need calibration and can be directly connected to the Vivo 50. This facilitates use both in the hospital and in the home environment?
What is the benefit of measuring EtCO2 at home?
With EtCO2 measurements and capnograms, the physician can obtain a good view on the quality of ventilation. This will contribute to quick decision making if ventilator settings need to be changed. The easy to use sensor enables CO2 measurements without disturbance of the patient, which makes this method highly suitable for use in the home environment.
Q&AQuestion Answer
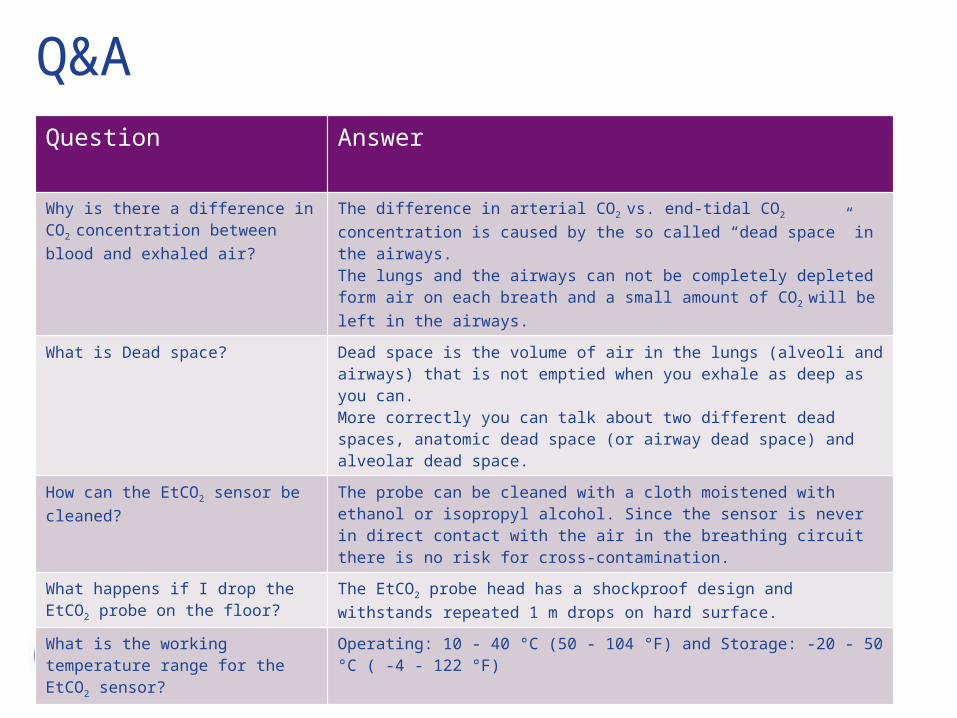
Why is there a difference in CO2
concentration between blood and exhaled air?
The difference in arterial CO2 vs. end-tidal CO2 concentration is caused by the so called “dead space” in the airways.The lungs and the airways can not be completely depleted form air on each breath and a small amount of CO2 will be left in the airways.
What is Dead space? Dead space is the volume of air in the lungs (alveoli and airways) that is not emptied when you exhale as deep as you can.More correctly you can talk about two different dead spaces, anatomic dead space (or airway dead space) and alveolar dead space.
How can the EtCO2 sensor be cleaned?
The probe can be cleaned with a cloth moistened with ethanol or isopropyl alcohol. Since the sensor is never in direct contact with the air in the breathing circuit there is no risk for cross-contamination.
What happens if I drop the EtCO2 probe on the floor?
The EtCO2 probe head has a shockproof design and withstands repeated 1 m drops on hard surface.
What is the working temperature range for the EtCO2 sensor?
Operating: 10 - 40 °C (50 - 104 °F) and Storage: -20 - 50 °C ( -4 - 122 °F)
Q&A
Question Answer
At which altitude can the EtCO2 sensor probe be used?
The EtCO2 sensor probe can be used up to 3012 meters above sea level.
What happens if the EtCO2 sensor sensor is exposed to water or moist?
The EtCO2 sensor probe is not waterproof but is classified as drip, leak and spill proof.
How often should the EtCO2 sensor Airway Adapters be changed.
The EtCO2 sensor Airway Adapter is a single patient use product and is usually changed as a part of the regular routine.
What is the warm-up time for EtCO2 sensor ?
Warm-up time is 5 sec and full specifications will be reached within 60 sec.
How often does the EtCO2 sensor require gas calibration?
Room air calibration is automatically performed when changing airway adapter (<5 sec). A zero reference calibration has to be performed at regular intervals (about every half year) or if an offset in gas readings is discovered when measuring gases.

Questions?





























