Embed Size (px)
Citation preview
ALLEN YEOH, MDSingapore
• Associate Professor, National University Singapore
• Dr. Yeoh’s interests are in the field of treatment and biology of childhood malignancies. Others include: Micro array studies and minimal residual disease detection in childhood acute leukaemias. Associate Professor Allen Yeoh is the Principal Investigator of the multi-centre Malaysia-Singapore ALL and AML studies. The Ma-Spore ALL 2003 study successfully used minimal residual disease stratification to tailor the intensity of therapy with an excellent ~80% 6-year EFS. Allen’s interest is in translational clinical research in acute leukaemia in children. He holds multiple awards including the American Society of Hematology Merit Award 2001, Asian Innovation Award 2003, Singapore Clinician Scientist Awards 2005, 2008 and 2013.
Personalised Therapy in Paediatric ALL
Allen YeohViva-Goh A/Prof in Paediatric Oncology
Yong Loo Lin School of MedicineNational University of Singapore
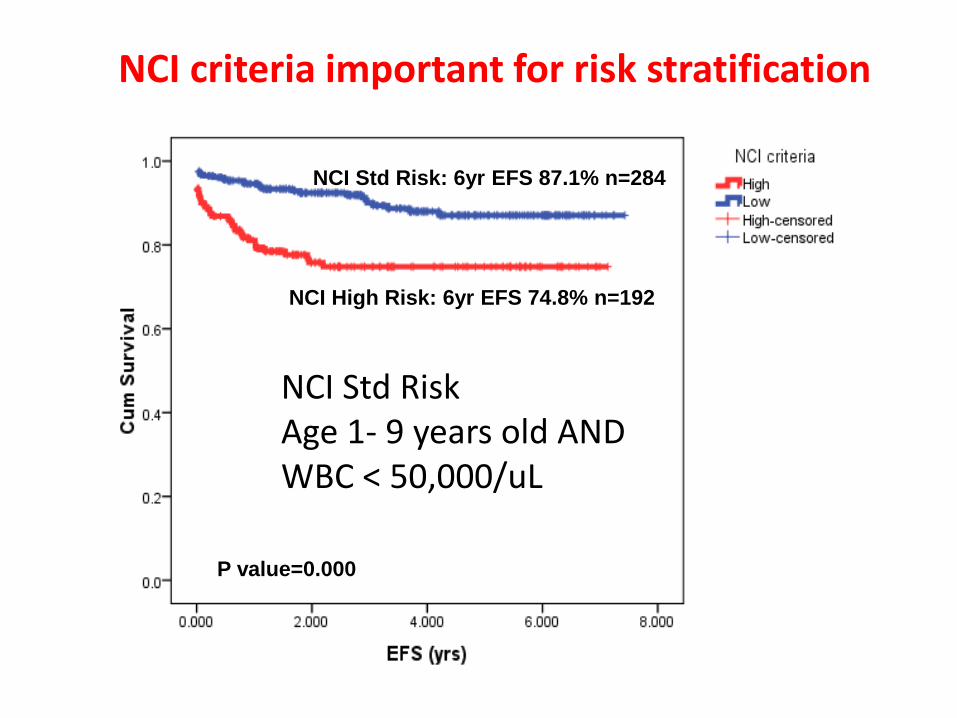
NCI criteria important for risk stratification
NCI Std Risk: 6yr EFS 87.1% n=284
NCI High Risk: 6yr EFS 74.8% n=192
P value=0.000
NCI Std Risk Age 1- 9 years old ANDWBC < 50,000/uL
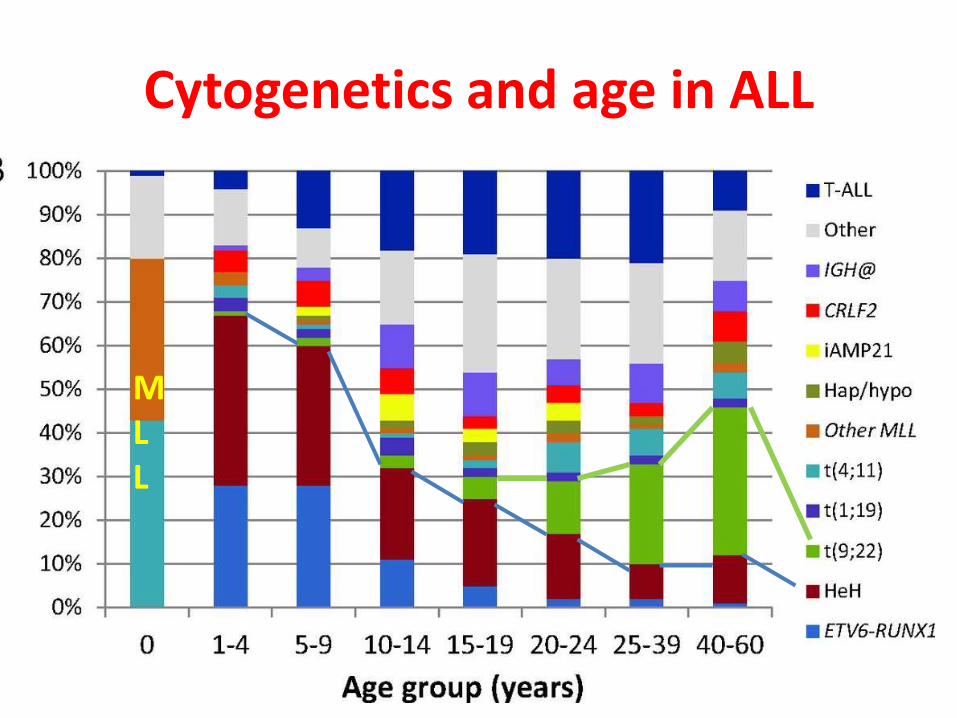
Cytogenetics and age in ALL
MLL
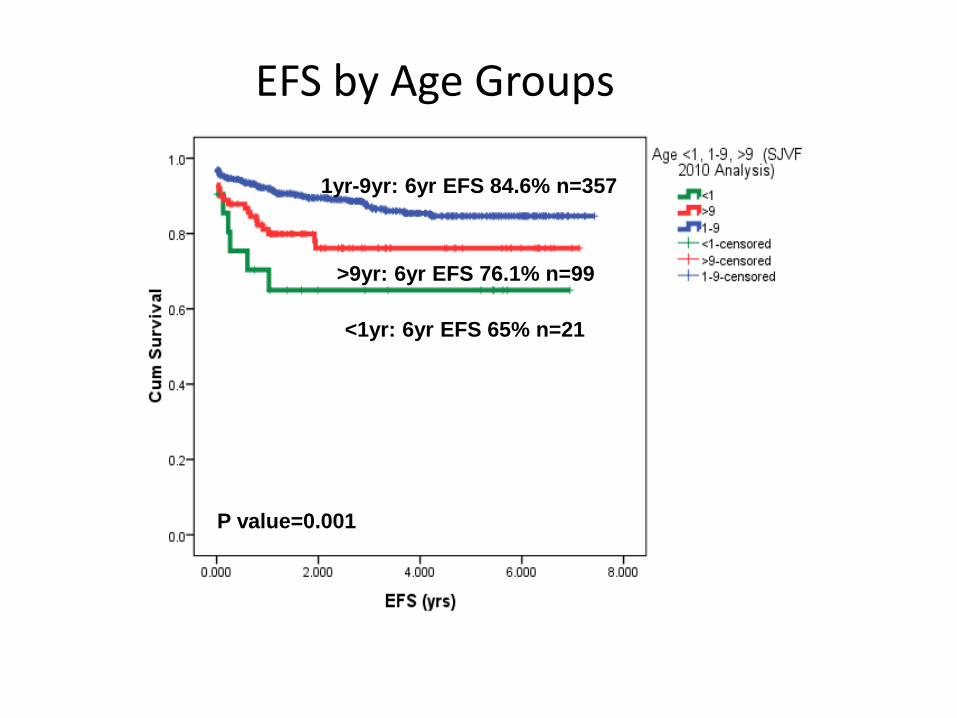
EFS by Age Groups
P value=0.001
1yr-9yr: 6yr EFS 84.6% n=357
>9yr: 6yr EFS 76.1% n=99
<1yr: 6yr EFS 65% n=21
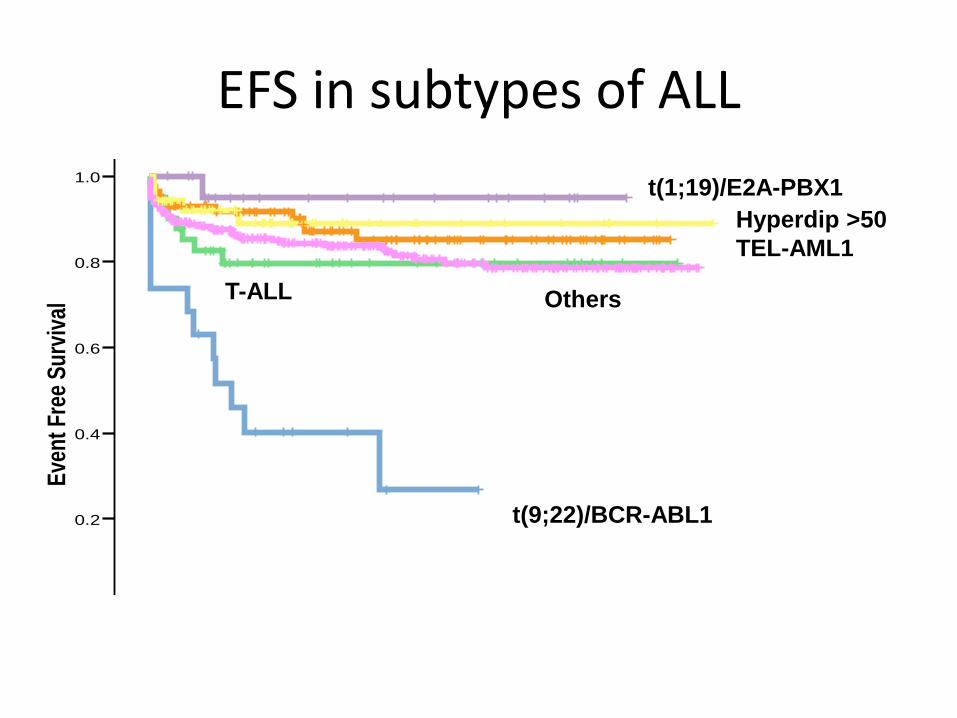
EFS in subtypes of ALL
Years from diagnosis
876543210
Eve
nt
Fre
e S
urv
ival
1.0
0.8
0.6
0.4
0.2
0.0
Pre-B ALL without BCR-ABL/t(9;22)-censored
ALL with hyperdiploid karyotype >50-censored
ALL with E2A-PBX1/t(1;19)-censored
ALL with TEL-AML1/t(12;21)-censored
T-ALL-censored
Pre-B ALL with BCR-ABL/t(9;22)-censored
Pre-B ALL without BCR-ABL/t(9;22)
ALL with hyperdiploid karyotype >50
ALL with E2A-PBX1/t(1;19)
ALL with TEL-AML1/t(12;21)
T-ALL
Pre-B ALL with BCR-ABL/t(9;22)
ALL Subtypes
Survival Functions
t(9;22)/BCR-ABL1
t(1;19)/E2A-PBX1
Hyperdip >50
TEL-AML1
OthersT-ALL
• Newly diagnosed NCI Standard Risk B-ALL• Age 1-9.99 years • Initial WBC <50,000/μL
• FISH - +4/+10 or ETV6-RUNX1• Rapid early response – Day 8/15 and• Day 33 MRD
• 5313 eligible pts enrolled 2005-2010
COG AALL0331 Eligibility
Maloney, ASH 2013

AALL0331: EFS and OS
5 yr EFS 89% (0.6%)5 yr OS 96% (0.4%)
Maloney, ASH 2013

Triple trisomies OR
TEL-AML1 , &
Day 15 (or 8) marrow
M1, &
Day 29 MRD < 0.1%,
No CNS 2/3, or
testicular disease
*No triple trisomies OR
TEL-AML1, &
Day 15 (or 8) marrow
M1, &
Day 29 MRD < 0.1%
*Unless CNS 2 at dx
CNS 3
OR
Day 15 marrow M2/3,
OR
Day 29 MRD ≥ 0.1% -
1%
MLL w/RER
Steroid pretreatment
Age 1.0-9.99 years
WBC < 50,000/ul
B precursor ALL only
AALL0331: Post-Induction Treatment
Assignment
Standard Risk-HighStandard Risk-
Average
Randomized study
Standard risk-
Low
Randomized study
3 drug induction-Dex, PEG, VCR
Maloney, ASH 2013
MRD cutoff ≥ 0.1%
used to define poor
response; now use ≥
0.01%

AALL0331: CCR for Risk Groups
0 2 4 6 8
0.0
0.2
0.4
0.6
0.8
1.0
Years
CC
R p
robabili
ty
2 SR Low n 1857
3 SR Average n 1500
4 SR High n 636
AALL0331
CCR by stratum
5-Year CCR ratesSR-Low 95.2% (SE 0.6%)SR-Av 88.8% (SE 1.1%)SR-High 85.7% (SE 1.8%)
Mattano and Maloney,
NCI SR + (+4/10/17) or ETV6-RUNX1AALL 0331 – Low risk
• And no CNS or testicular leukemia, and
• rapid marrow response (<5% blasts d15 and end-IND (MRD) <0.1%).
Intensification of Rx did not improve outcome:
• Intensification by 4 additional PEG-Asp (2500U/m2) every 3 wks during consolidation/interim
5y CCR 96.0% (0.8) vs 94.4% (1.0) (p=0.1)
5y OS 98.3% (0.6) vs 99.3% (0.4) (p=0.05)
• Intensification by IV Capizzi MTX
3y EFS IV MTX 99.0% (0.4) vs 97.0% (0.5), p=0.16
Mattano LA, et al. ASH 2014. Abstr 793
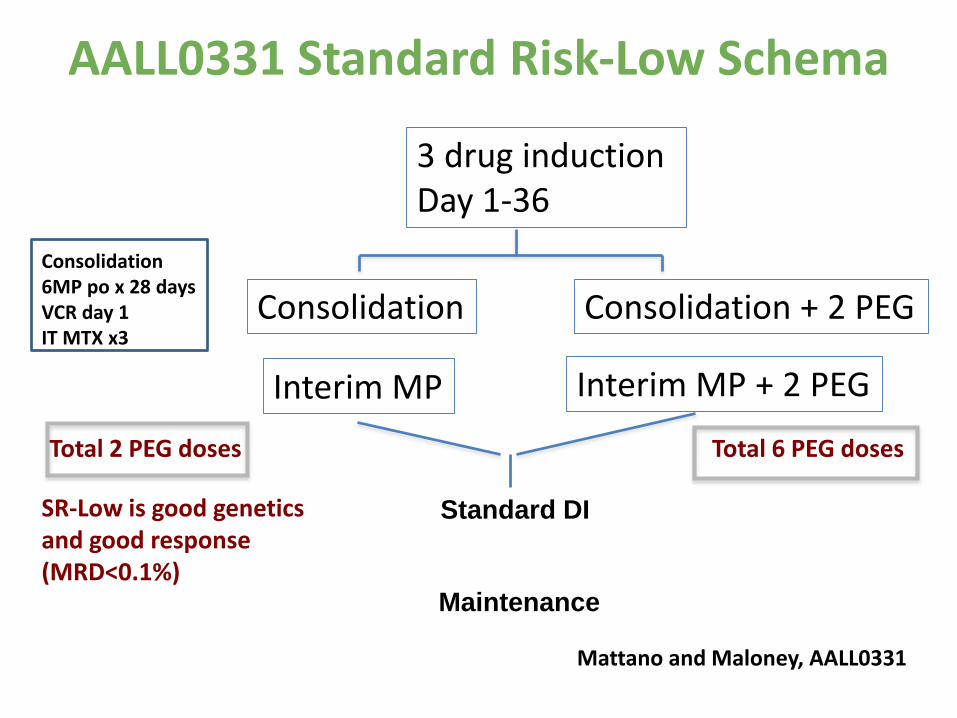
AALL0331 Standard Risk-Low Schema
Standard DI
Maintenance
Total 2 PEG doses Total 6 PEG doses
Mattano and Maloney, AALL0331
Consolidation6MP po x 28 daysVCR day 1IT MTX x3
SR-Low is good genetics and good response (MRD<0.1%)
3 drug induction Day 1-36
Consolidation
Interim MP
Consolidation + 2 PEG
Interim MP + 2 PEG

0 2 4 6 8
0.0
0.2
0.4
0.6
0.8
1.0
Years
CC
R p
rob
ab
ility
LRAsp LRAsp IV arms n 928
LRS LRS IV arms n 929
AALL0331 SR-Low Group
CCR by PEG regimen
One sided P value 0.1341
AALL0331 SR-Low: No Benefit with Intensified Pegasparaginase
5-Year CCR ratesStd 94.4% (SE 1.0%)Std + int PEG 96.0% (SE 0.8%)
Mattano et al. ASH 2014 Abstr 793
14
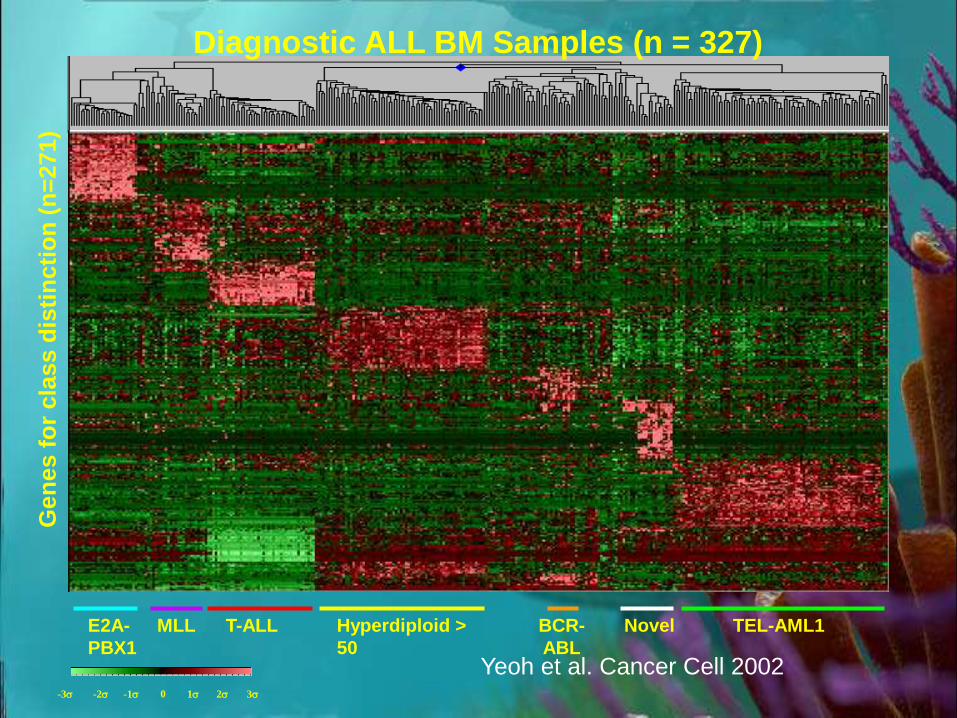
Diagnostic ALL BM Samples (n = 327)
3-3 -2 -1 0 1 2
Gen
es f
or
cla
ss d
isti
ncti
on
(n
=271)
TEL-AML1BCR-
ABL
Hyperdiploid >
50
E2A-
PBX1
MLL T-ALL Novel
Yeoh et al. Cancer Cell 2002

Prediction Accuracy Using Support Vector Machines
SubgroupsTraining Set
Apparent Accuracy
Test Set
True Accuracy Sensitivity Specificity
T-ALL
E2A-PBX1
TEL-AML1
BCR-ABL
MLL rearrangement
Hyperdiploid > 50
100%
100%
98%
96%
100%
93%
100%
100%
99%
97%
100%
96%
100%
100%
100%
83%
100%
100%
100%
100%
98%
98%
100%
93%
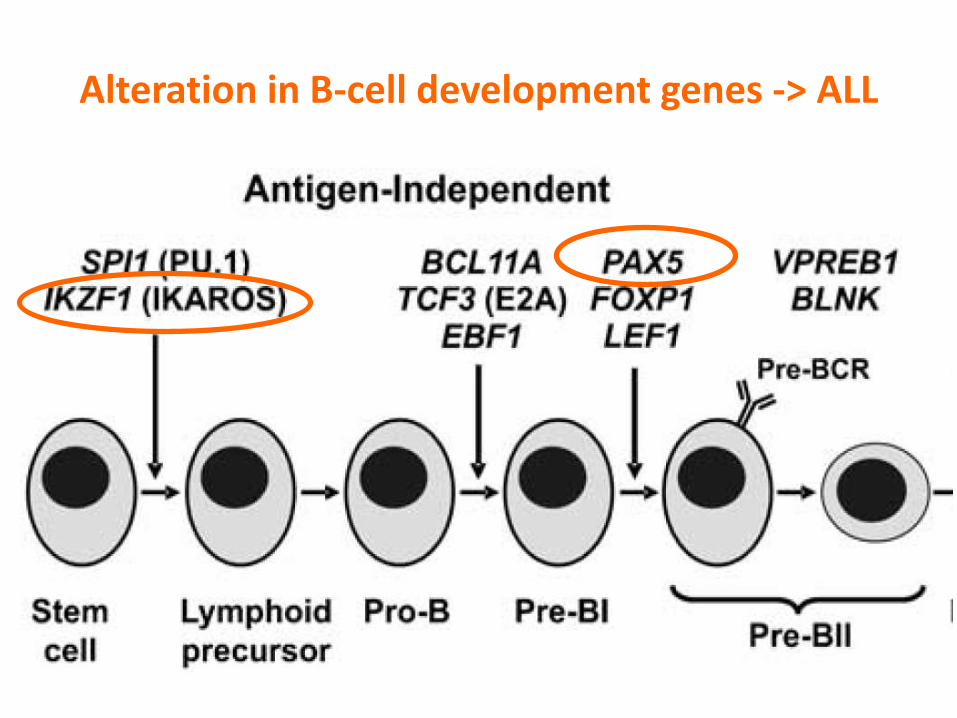
Alteration in B-cell development genes -> ALL

Ikaros del BCR-ABL1 –ve poorer outcome
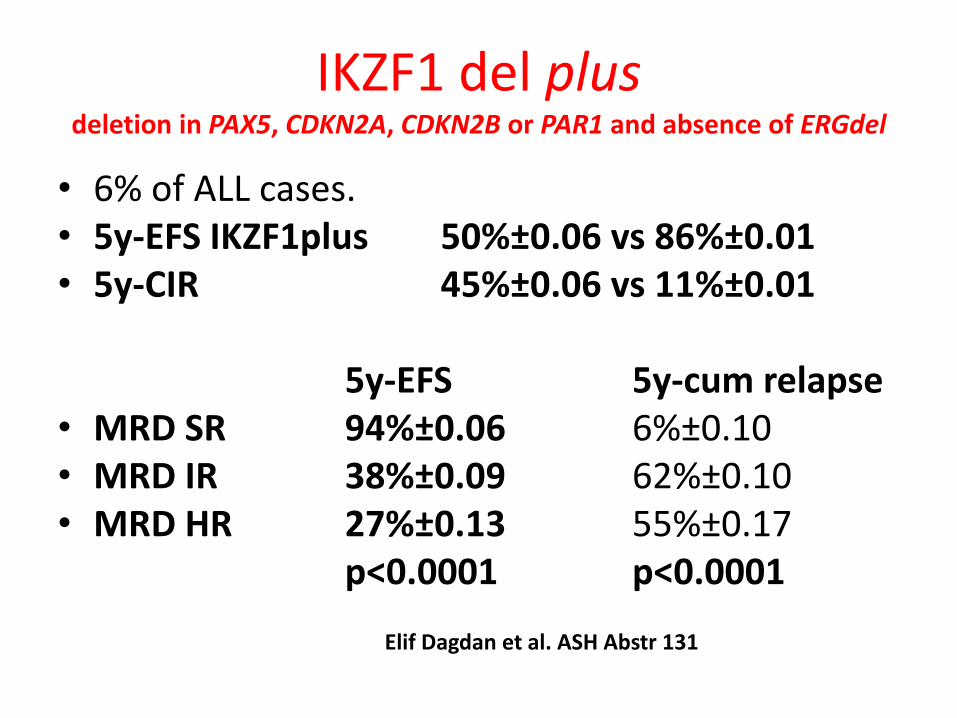
IKZF1 del plus deletion in PAX5, CDKN2A, CDKN2B or PAR1 and absence of ERGdel
• 6% of ALL cases. • 5y-EFS IKZF1plus 50%±0.06 vs 86%±0.01 • 5y-CIR 45%±0.06 vs 11%±0.01
5y-EFS 5y-cum relapse• MRD SR 94%±0.06 6%±0.10 • MRD IR 38%±0.09 62%±0.10 • MRD HR 27%±0.13 55%±0.17
p<0.0001 p<0.0001
Elif Dagdan et al. ASH Abstr 131
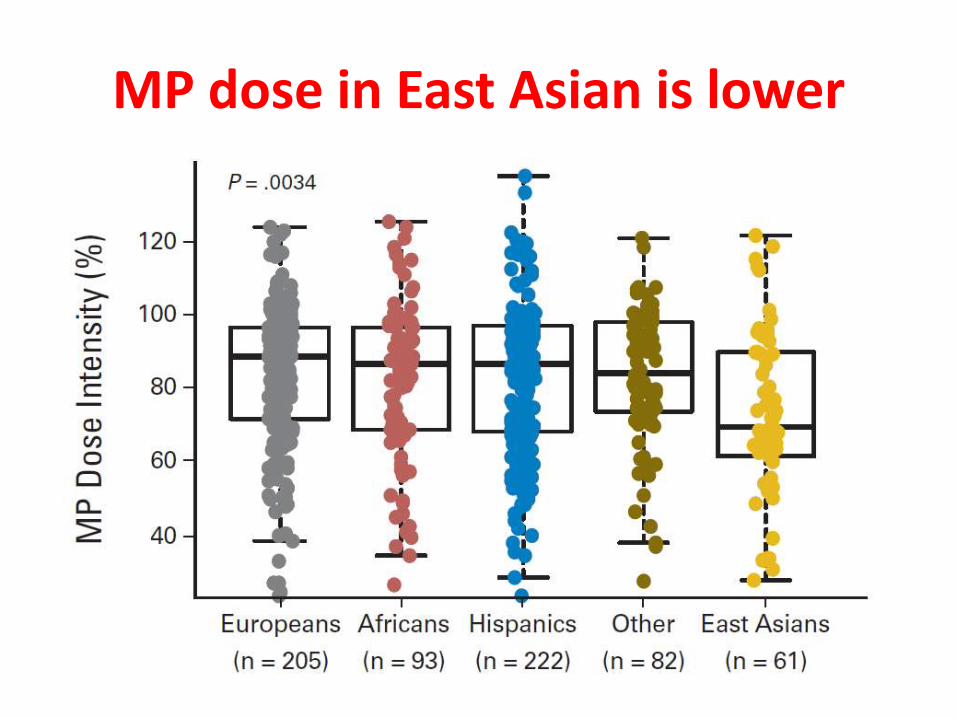
MP dose in East Asian is lower
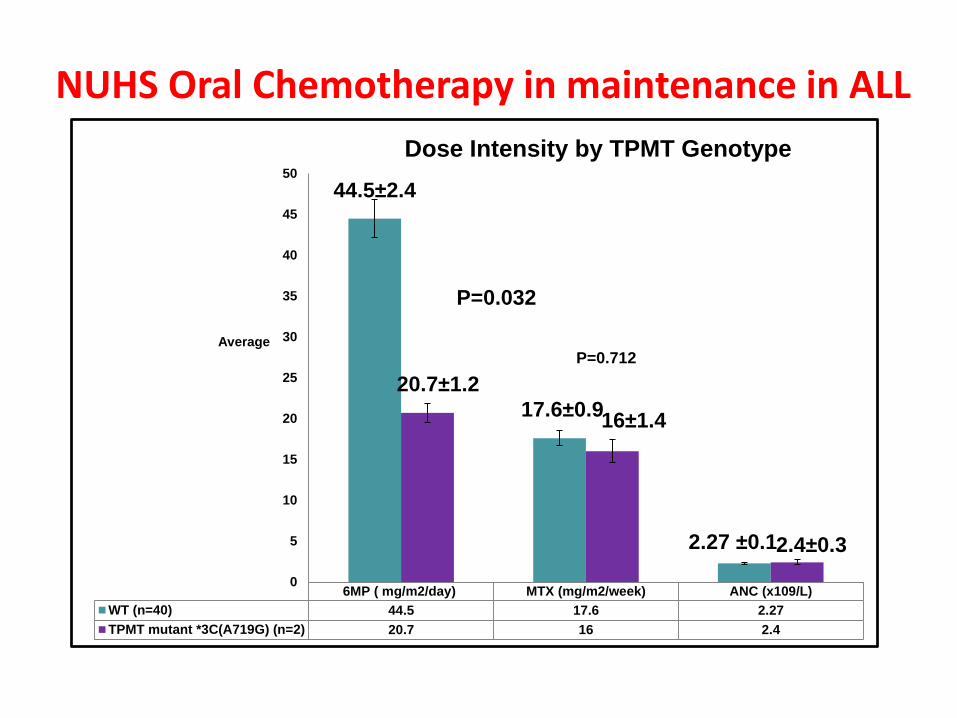
6MP ( mg/m2/day) MTX (mg/m2/week) ANC (x109/L)
WT (n=40) 44.5 17.6 2.27
TPMT mutant *3C(A719G) (n=2) 20.7 16 2.4
44.5±2.4
17.6±0.9
2.27 ±0.1
20.7±1.2
16±1.4
2.4±0.3
0
5
10
15
20
25
30
35
40
45
50
Average
Dose Intensity by TPMT Genotype
NUHS Oral Chemotherapy in maintenance in ALL
P=0.032
P=0.712

TPMT mutation in 3.1% Ma-Spore ALL 2003 study
Ethnic
TPMT Chinese Indian Malay Others Total
Wild Type
247
(95.4%)
44
(93.6%)
202
(93.5%)
34
(100%)
527
(94.8%)
*3C (A719G)
8
(3.1%)
2
(4.3%)
6
(2.8%)
0
(0%)
16
(2.9%)
*6 (A539T)
1
(0.4%)
0
(0%)
0
(0%)
0
(0%)
1
(0.2%)
NA
3
(1.1%)
1
(2.1%)
8
(3.7%)
0
0%)
12
(2.1%)
Total 259 47 216 34 556
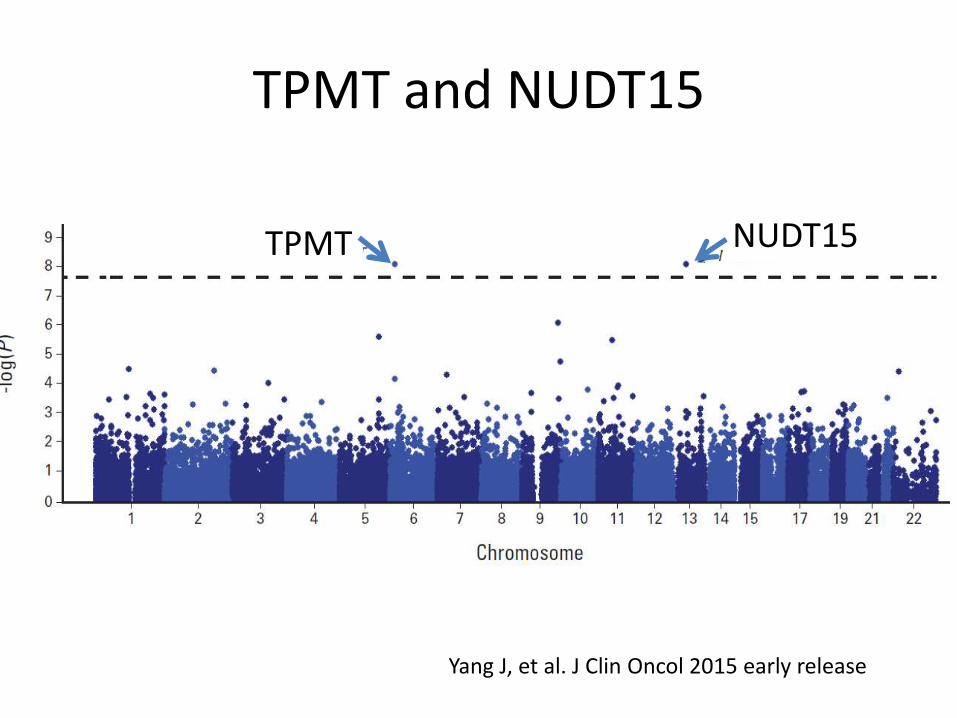
TPMT and NUDT15
NUDT15TPMT
Yang J, et al. J Clin Oncol 2015 early release

TPMT *3C/*3A
Yang J, et al. J Clin Oncol 2015 early release
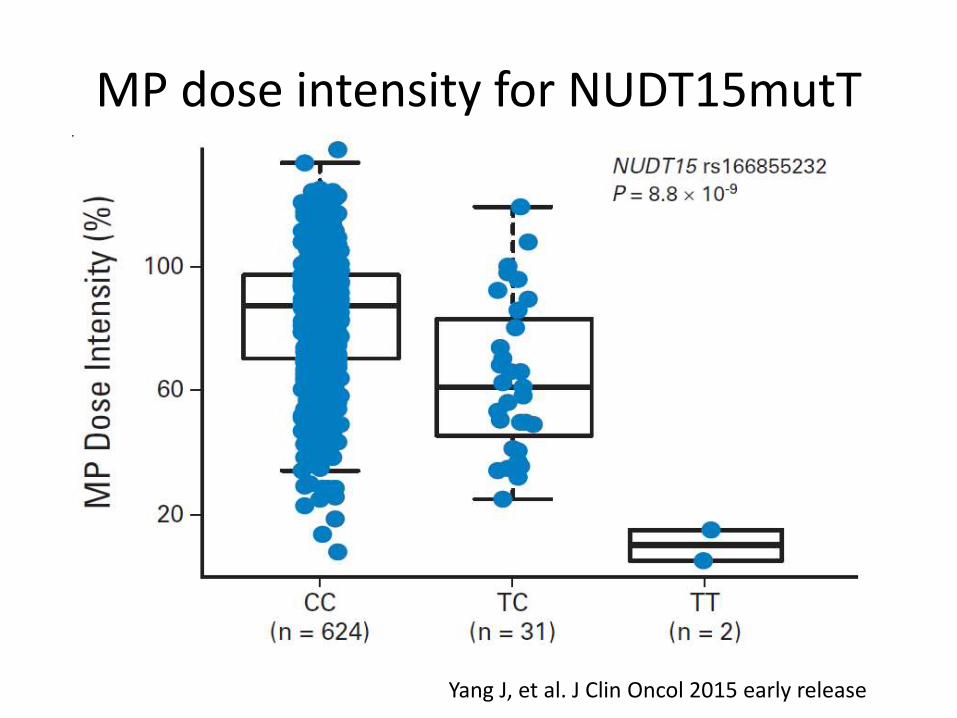
MP dose intensity for NUDT15mutT
Yang J, et al. J Clin Oncol 2015 early release
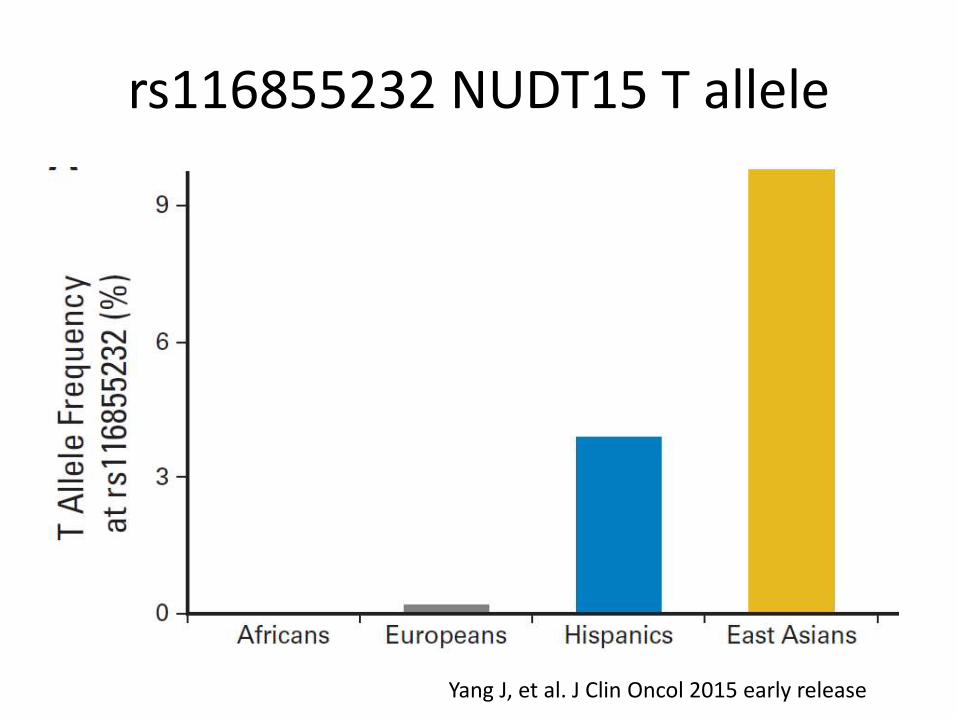
rs116855232 NUDT15 T allele
Yang J, et al. J Clin Oncol 2015 early release
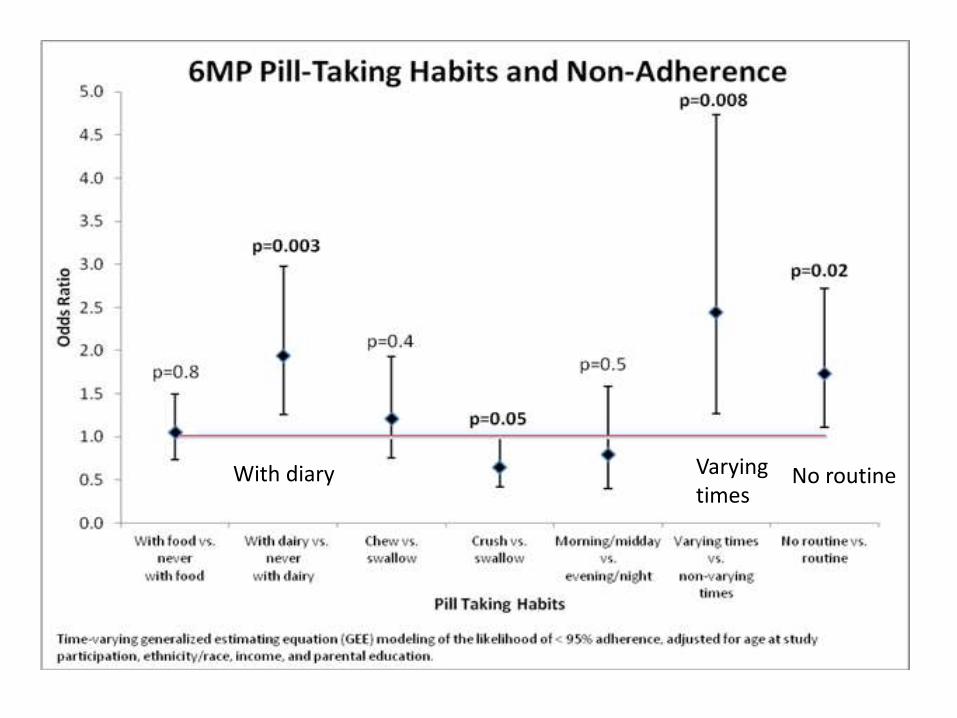
Varying times
No routineWith diary

0%
10%
20%
30%
0 1 2 3
Cu
mu
lati
ve in
cid
en
ce o
f re
lap
se
Years since study exit
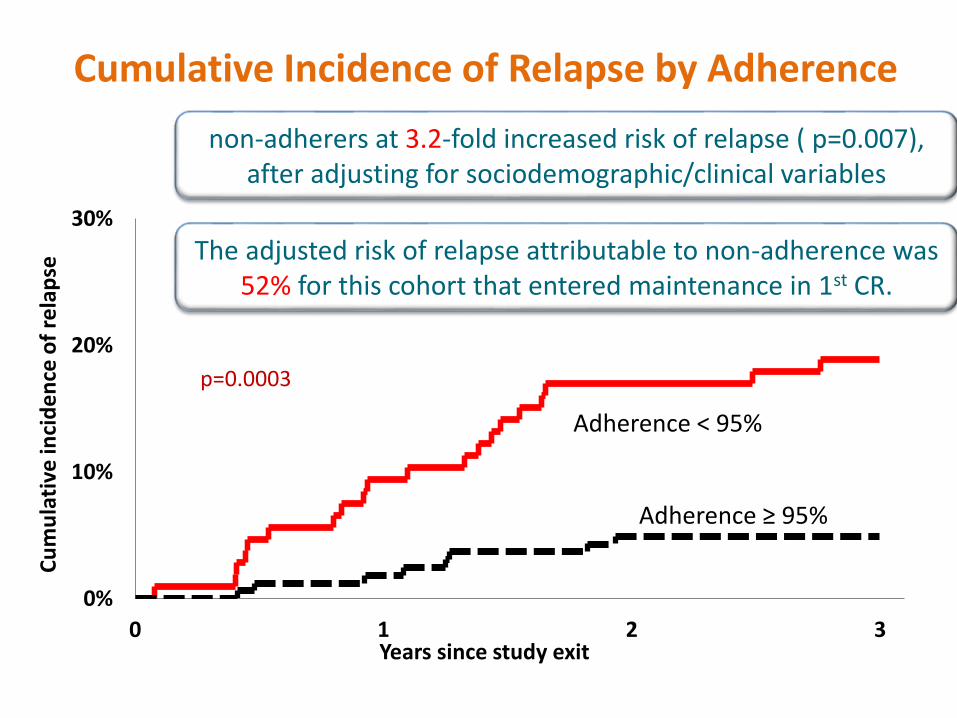
Cumulative Incidence of Relapse by Adherence
Adherence ≥ 95%
Adherence < 95%
p=0.0003
non-adherers at 3.2-fold increased risk of relapse ( p=0.007), after adjusting for sociodemographic/clinical variables
The adjusted risk of relapse attributable to non-adherence was 52% for this cohort that entered maintenance in 1st CR.
00.00
Years since study exit
Cu
mu
lati
ve in
cid
ence
of
rela
pse
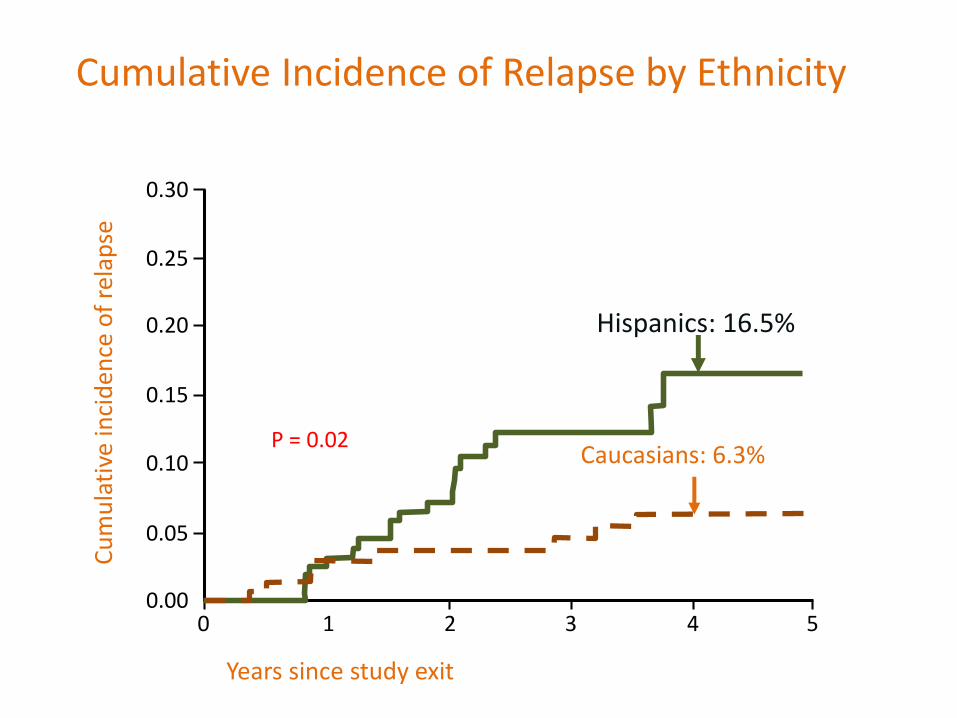
P = 0.020.10
0.20
0.30
1 2 3 4 5
0.25
0.15
0.05
Cumulative Incidence of Relapse by Ethnicity
Hispanics: 16.5%
Caucasians: 6.3%
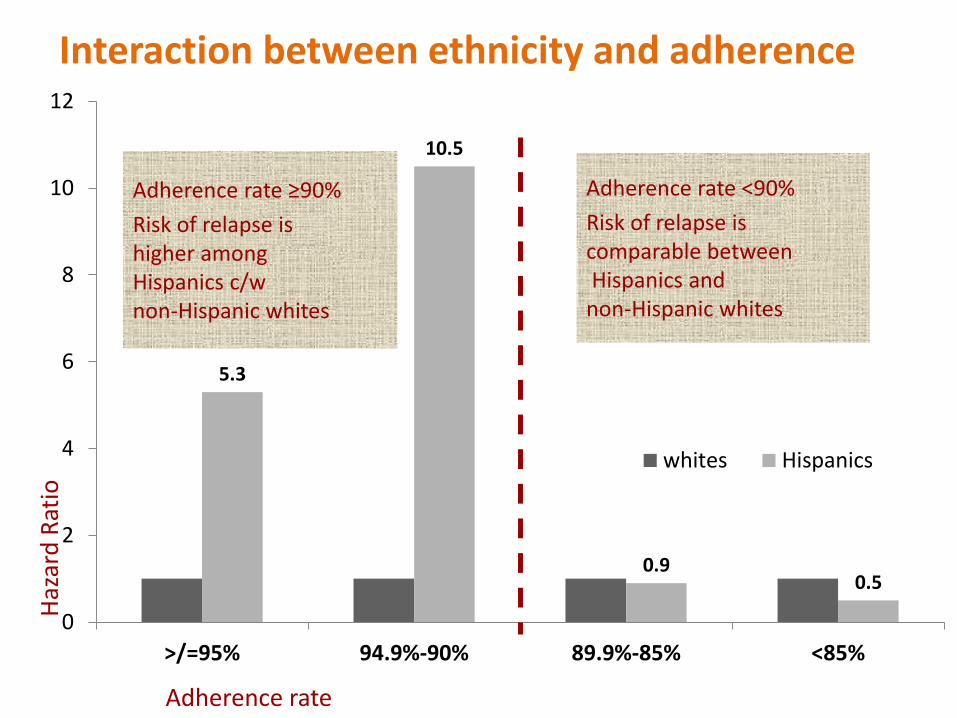
Interaction between ethnicity and adherence
5.3
10.5
0.90.5
0
2
4
6
8
10
12
>/=95% 94.9%-90% 89.9%-85% <85%
whites Hispanics
Haz
ard
Rat
io
Adherence rate
Adherence rate ≥90%
Risk of relapse ishigher among Hispanics c/w non-Hispanic whites
Adherence rate <90%
Risk of relapse is comparable betweenHispanics and
non-Hispanic whites
MP compliance important
• Schedule >95% important.
• Regular routine dosis better – better complianc.
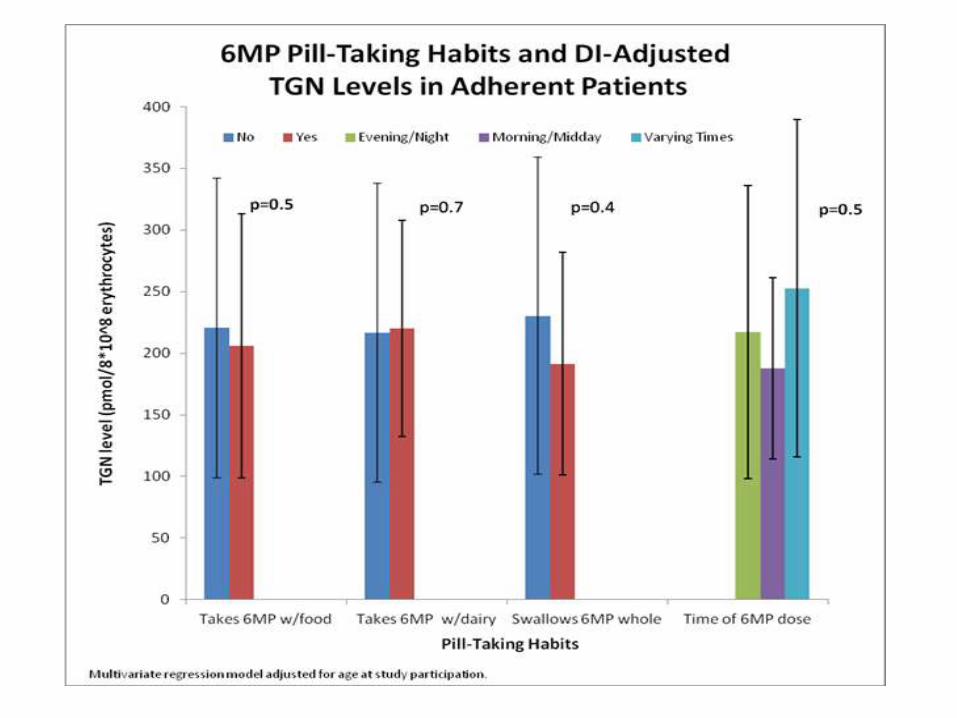
• With food or dairy or at night not critical for high dose MP 75 mg/m2 per day. Not sure if lower doses matters.
• Not need to be too strict – regular more impt
COG AALL0433 Intermediate risk relapse
• early isolated CNS/testicular relapse (<18 m), or late BM/combined relapse (≥36 m) of B-ALL
• N = 271 eligible patients
• 0.1% end-induction MRD predict outcome
• late BM relapse MRD- after induction 3-yr EFS of 80.4 ± 4.7% - no need SCT
• SCT for – Late BM relapse and MRD +ve
– Early isolated extramedulary relapse -
Lew G, et al. ASH 2014. Abstr 684
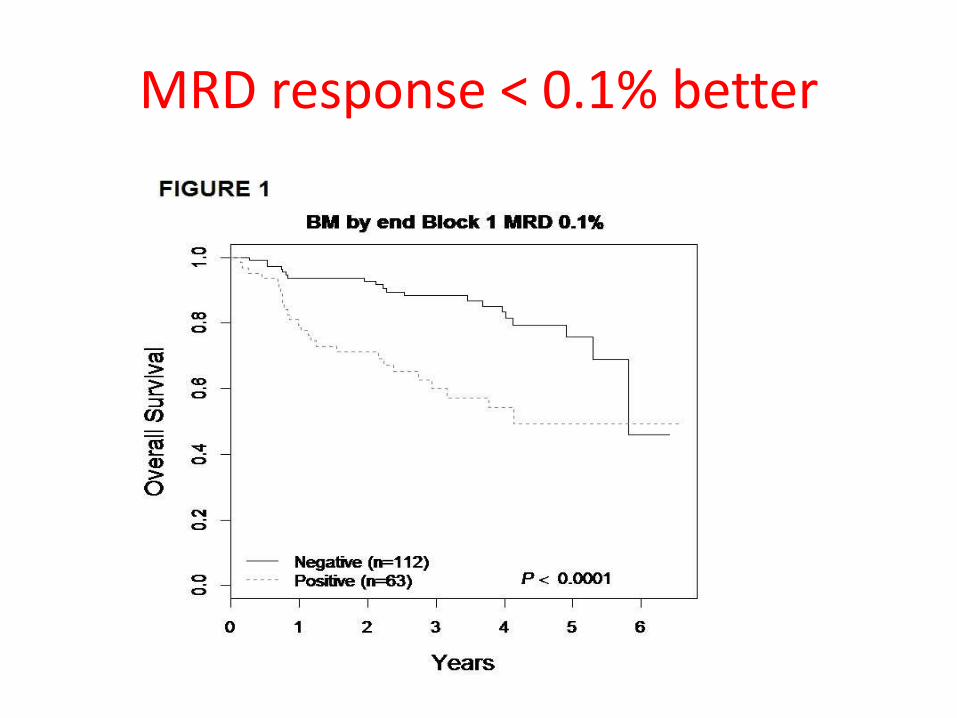
MRD response < 0.1% better
Early bilateral isolated testicular relapse poor outcome – BFM ALL-REZ• ALL-REZ trials (1983-2013) = 1603 boys
• Testicular = 302 (18.8% of boys). Isolated testicular 8.4%.
• No difference in timing compared to combined relapse.
• Rx Affected testes 24Gy, other side 15-18Gy. Reinduction and full Rx.
• 5y EFS Isolated testicular 0.70±0.04 better outcome than combined relapse (0.54±0.04, p=0.005)
• Multivariate poorer outcome: – Time to relapse,
– Bilateral testicular relapse
– Combine BM and testicular relapse
• Subsequent relapse mainly in BM.
Christiane Chen-Santel, et al. ASH 2014. Abstr 68
NECTAR T2008-002Nelarabine-Etoposide-Cycloph in T-acute lymphoblastic relapse
• NEL 650 mg/m2,
• CPM 440 mg/m2 and
• ETOP 100 mg/m2, each given daily for 5 days
No IT 7 days prior or 21 days after NEC
19 patients with relapsed/refractory T-ALL/LL
T-ALL 44% response
T-LL 25% response
James Whitlock et al. ASH 2014. Abstr 795
BLAST – Blinatumumab ALL Single arm, Phase II study.
• N= 116 ALL patients with MRD positive > 10-3
• Blinatumomab 15 µg/m²/day was given by continuous IV infusion for 4 weeks
• complete MRD response (negative MRD ≥ 10-4
after 1 cycle)
• 59% grade ≥ 3 SAE and 27% grade ≥4 SAEs– pyrexia (15%), tremor (7%), aphasia (5%),
encephalopathy (5%), atypical pneumonia
• Most respond by 1 cycle.
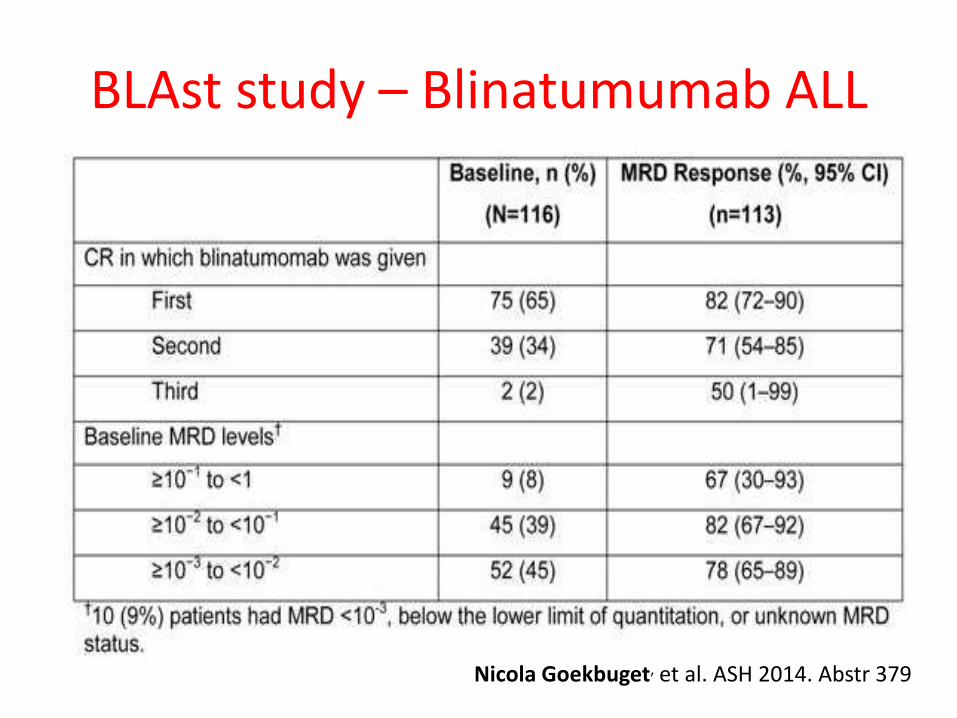
BLAst study – Blinatumumab ALL
Nicola Goekbuget, et al. ASH 2014. Abstr 379

Pediatric ChemoRx vs BMT in adult Ph-ve ALL
DFCI vs CIBMTR
Matthew D. Seftel, et al. ASH 2014. Abstr 319

Adults T- Lymphoblastic LymphomaGraall-Lysa LL03
• 131 T-LL patients
• 5y EFS 61% and 5y-OS 66%.
• IPI-score had no prognostic value,
• Raised LDH (71% pts)
– lower EFS (HR = 2.8 [1.3 – 6.1]) and
– OS (HR = 3.5 [1.4 – 9.1])
• AlloSCT did not improve outcome
Stephane Lepretre et al. ASH 2014. Abstr 371

Personalised MedicineCurrent
Morphology + cytochemistryFlow cytometry
B vs TCytogeneticsHyperdiploid > 50Hypodiploid < 44
OFTBCR-ABL1MLL-AF4E2A-PBX1ETV6-RUNX1
Future
Real-time PCRMRD
Multiparametric flow Flow MRD
PharmacogenomicsTPMT, NUDT15
Microarray GEPNext generation sequencing
RNA seqExome profilingWhole genome seq
Thank you





























