Embed Size (px)
Citation preview

PARTNERSHIPS FOR STUDENT
MENTAL HEALTH:
THE STATE OF PLAYDr Ron Alcorn,
Consultant Psychiatrist and
Royal College of Psychiatrists representative for
student mental health
Student Mental Wellbeing: Policy, Practice and Future Directions
February 13th 2015

Background – the HE student group
• Increased access to and participation in HE
• Research shows higher levels of stress and symptoms in HE populations compared with matched controls
• Widespread perception of an increasing range and severity of problems amongst students in HE
• New influences on mental wellbeing; impacts of social networking (positive and negative), information from the internet (eg; self-diagnosis), drug and alcohol patterns/access
• HE mental health epidemiological and survey information is often dated and limited
• Rapidly changing context calls for new and more sophisticated partnerships


Background – HE Support Services
• Pressure of numbers
• Greater complexity (and risk)
• Rising expectations
• Reduced resources
• Moves to shorter interventions (similar to trends in services generally)
• Broader range of interventions (alongside face-to-face, 1:1 work); information / bibliotherapy / internet-based interventions / groups / call-lines / remote (“Skype”) sessions
• On-campus Mental Health Advisors / Coordinators / Mentors / peer-led or mutual-aid services
• Wide variety of joint arrangements with other providers (eg;NHS)

Ideal service for HE students (or what would optimised partnerships look like?)
• Prompt, accessible, flexible, effective
• Accounts for adjustment and developmental processes (resists
“over-medicalisation”)
• Young person centred but working towards adult integration
• Flexible around the academic year and academic priorities
• Allows for diagnostic, therapeutic and prognostic uncertainties

Ideal service for HE students
• Targeted interventions for vulnerable groups such as international
students , those with pre-existing problems and possibly those with
strong family histories of mental health or addiction problems
• Offers treatments that don’t have a negative impact on learning or
performance
• Offers continuity throughout the period of being a student
• Handles transitions from “home” adolescent settings and into adult,
“real world” settings


and services that address ….
• Crisis interventions
• Autism spectrum disorders (Aspergers syndrome)
• Eating disorders
• Adult ADHD
• Emerging personality difficulties (emotionally unstable / borderline patterns and self-harm)
• Emerging major mental illness (bipolar affective disorders and schizophrenia)
• Anxiety disorders that affect study (OCD/social phobia)
and….
• Co-occurrence with specific learning problems
and…
• Use sensitive, “early intervention” methodologies

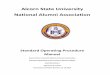
Services in the Local NHS
Services ‘at Home’
Services in the
Voluntary Sector/ Charitable Sector
Services in the
Local Authority/ Public Health
STUDENT IN HIGHER
EDUCATION

Partnerships with “home” services
• Adolescence into early adulthood is when many mental health problems first emerge, come in to “focus” and affect functioning
• Potential discontinuities for existing physical and mental health care in the move to HE
• Adult services may question existing diagnoses, have reduced access to effective treatments and medications and employ less assertive engagement models
• Transitions can be coupled with the student’s desire to “leave it all behind”, make a fresh start or exploit the “gaps”
• Transitions from other countries come with all the issues mentioned above along with stresses of acclimatisation/acculturation

Key priorities
• Timely flow of information / health records / liaison with key informants
• Information and preparation for the student and the family
• Introduction and orientation to the HE locality services (pre-entry “bridging”)
• Crisis and contingency plans
• Continuity across holidays / breaks
• Managing expectations


NHS - strategic context
• Health and Social Care Act 2012
• Clinical Commissioning Groups (CCGs) – led by GPs
• GP-leads for specific areas (mental health / young people), enhanced service arrangements for targeted conditions
• Creation of Public Health England (PHE)
• Allowing healthcare market competition / bidding and tendering for all services
• New combinations of agencies in new types of partnerships (many now non-NHS)
• New regulatory bodies (Monitor / CQC)

NHS – services context• Development of Primary Care for the local context / more creative responses
• Move to Primary Care Psychiatry (less emphasis on secondary care / improving access / reducing stigma)
• IAPT (Improving Access to Psychological Therapies) – stepped care models / other than face-to-face options
• Psychological Medicine / Liaison teams in acute hospitals (“RAID” models)
• Emphasis on recovery models / peer-led and mutual aid / service-user involvement / outcomes
• Retraction of some specialist functions/teams - absorbed back into the Community Mental Health Team (CMHT)
• Cuts to funding year on year
• Waiting lists / ever more stringent criteria / shorter packages of care

Local Authority - strategic context
• LAs now commission and administer Public Health functions
• Director of Public Health sits in the local authority
• Local responses to local needs
• Joint Strategic Needs Assessment (JSNA) – sets out priorities for funding and targets
• Health and Wellbeing Boards (multi-agency)
• Cuts to local authority and social care budgets
• Ring-fence taken off some budgets

Local Authority – services context
• Competitive bidding-tendering
• New combinations of agencies in new types of partnerships
• Services such as alcohol and drug / sexual health / smoking cessation / health campaigns have moved out of the NHS into the local authority
• These services vary in their knowledge of and preparedness for student health / mental health issues
• Opportunities exist for joint working / developing student-specific information / participation in Pubic Health-led campaigns (prevention, reducing stigma, health promotion)

3rd sector ,charities, student-led
organisations, independent sector • Expanding sector
• Innovative and responsive options and interventions
• Can be more flexible and responsive to student needs / feedback / co-production
• Ideally complementary but sometimes competitive
• Fears about short-term funding streams / impact of market economics on existing services / “following the money”
• In-house vs out-sourcing
• Specific local vs national focus


New Challenges / Opportunities
• Redefining CAMHS – increasing the age limit into the twenties (“adolescence is the puberty of the body, the twenties is the puberty of the mind”)
• Integrated Young People’s commissioning
• GP Choice agenda
• Portable / personal clinical records
• Personalised budgets / support for carers (Care Act 2014)
• New technologies
• Confidentiality-information sharing protocols / “network” protocols

New Challenges / Opportunities
• Time and trust to build collaborations, networks, joint protocols, pathways
• Mapping and keeping abreast of local services and mental health provision / avoiding duplications of service
• Fielding the frequent questions….“what to you expect us to do that you can’t?” / “don’t you have that in-house?” / “wouldn’t it be quicker if you saw them?”
• Jointly funded or shared posts / in-reach services
• New models (DBT / MBT – AMBIT) adapted for HE populations
• Regular network / liaison meetings / joint-training

New Challenges / Opportunities
• Developing new skills – lobbying, writing business cases
• Understanding other sectors’ priorities, language, funding
streams, funding timetables, opinion leaders
• Using research and grants to get new services and /or
improve the evidence base
• HE institutions sharing experience and practice models

Student Mental Wellbeing: Policy, Practice and Future Directions
February 13th 2015
• Reference
Royal College of Psychiatrists position paper
“Report on the Mental Health of Students in Higher
Education” – CR112 (2003), revised CR116 (2011)
and thanks to my colleagues at QMUL and in the London
Student Mental Health Psychiatry Network