Embed Size (px)
Citation preview

Gombalandi Ruben WML5th course vnmu
RUBEN GOMBALANDI 5Th course WML

OPPORTURNISTIC INFECTIONS IN HIV ,MANAGEMENT ,PREVENTION

There are more people who are alive today, than have ever
died!!

78 million are infected with a virus called HIV.

STRUCTURE
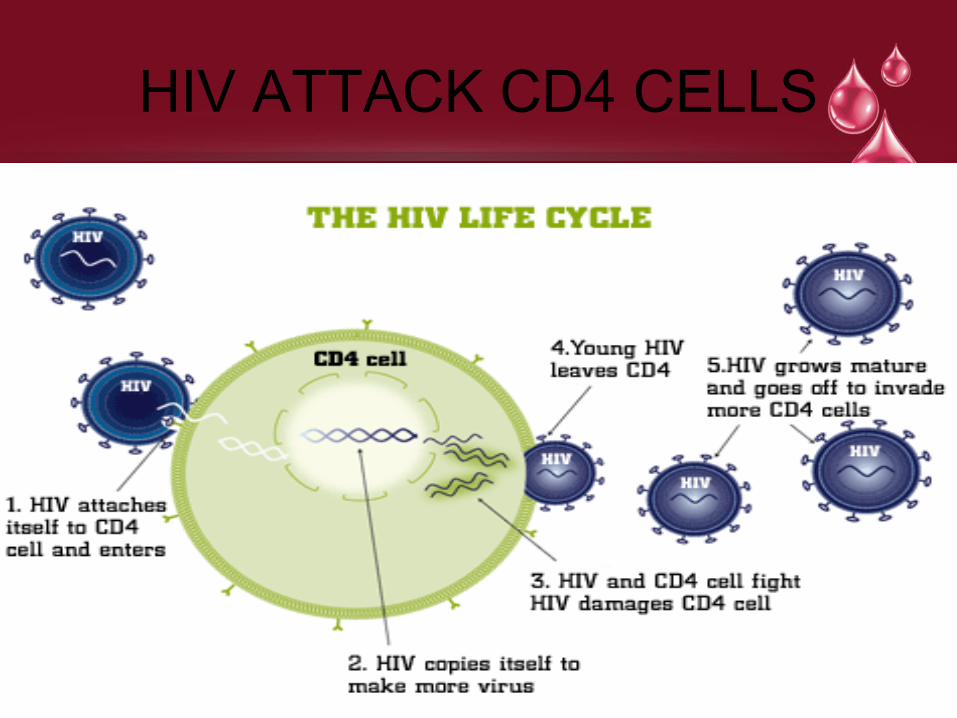
HIV ATTACK CD4 CELLS


What is an opporturnistic infection ?
• Infection by a microorganism that normall does not cause disease but becomes pathogenic when the body’s immune system is impaired and unable to fight off infection.
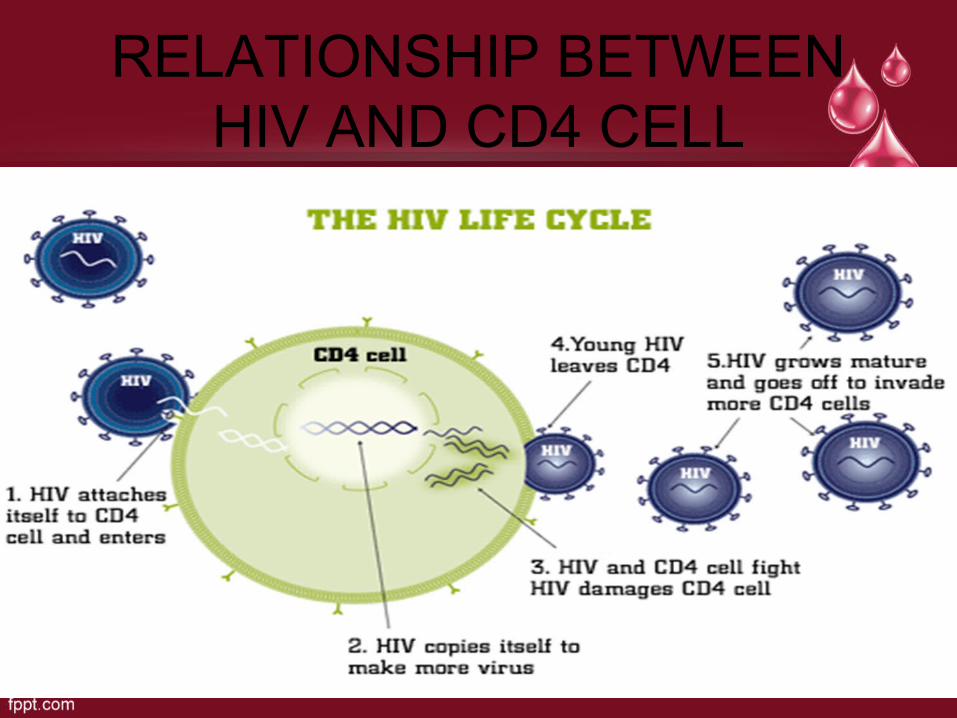
RELATIONSHIP BETWEEN HIV AND CD4 CELL

CD4
• Is a type WBC
• Normal : 500 -1500 CD4 cells/mm3
• Cd counts are important because it guides us on the management of HIV,and also help us to know how urgent it is for us to start treatment and the prophylaxis we need to start .
• Determines OI Risk.

MAJOR OI’S TO KNOW
• Tuberculosis
• Pneumocystis jiroveci pneumonia (pjp)
• Mycobacterium Avium complex
• Enteric bacterias : salmonella, shigella, campylobacter , Listeria , cryptosporidium
• Cryptococus
• Histoplasma
• Coccidiodomycosis

Viruses, (OI)
• Cytomegalovirus
• Herpes simplex virus 1 ad 2
• Human herpes simplex virus 8( kaposi sarcoma)
• Human papiloma virus
• Varicella zoster virus


OI’S AND HIV
• OI’S can be the first presetation in an HIV Patient .
• OI can also be associated with immune reconstitution inflammatory sydrome (IRIS)
• During treatment we can have drug-drug interaction between drugs for treating OI and drugs for treating HIV (HAART)
• Which is a big cause of morbidity and and mortality ,but they are preventable .
•

IRIS
Is an inflammatory disease that occurs in response to a specific opporturnistic pathoen within weeks or months after starting ART.Mostly caused by enhanced and dsyregulated immune response to antigens.

presentation
• Patients present as exacerbation of partially or recently treated OI
• OR
• They present with inflammatory response to previously undiagnosed OI

RISK FACTORS
• Greater risk when starting ART at high viral load .and low cd4 cell - <50
• Can difficult to identify,because no lab test that can help to make diagosis .
• Severity varies from mild to life threatening

Management
• Treate the OI
• Continue ART
• USE anti-inflammatory drugs.
OI PROPHYLAXIS

PROPHYLAXIS

Drugs used FOR PRIMARY PROPHYLAXIS
• pjp,:Tmp/smx ,1 DS Qday or 1ss po Q day
• Toxoplasmosis :TMP/SMX ,1DS Qday
• Diseminated MAC COMPLEX: Azithromycin 1200 mg po Qweek

SECONDARRY PROPHYLAXIS
• PJP :TMP/SMX
• TOXOPLASMOSIS :PYRIMETHAMINE 25-50Mg PO Qday + sulfadiazine 2000-4000mg PO Qday + leucovorin 10-25 mg PO Q Day
• MAC : CLARITHROMYCIN 500 Mg PO BID + ETHAMBUTOL 15 Mg/kg.PO QDay

OI’S EXPOSURE
• Sexual
• Iv drug abuse
• Enviroment
• Other individuals
• Animals
• Travel

SEXUAL EXPOSURE
• Hepatitis,A,B,C
• Human papillomavirus
• Cytomegalovirus
• Herpes simplex virus
• Syphilis ,chlamdia,gonorrhea
• Eteric organism

PREVENTION
USE IT PROPERLY

IV DRUG USE
• HEP C
• Bacterial infection (stap aureus,) : cellulitis ,bacteremia ,endocarditis,osteomyelitis
• Drug contaminant : black tar heroin.
• Increase risky behaviour

PREVENTION
• Treatment programs
• Immunize against HEP A and HEP B.
• Discuss ways to aviod sharing needles and other equipment
• Prosper cleaning of equipment

ENVIROMENTAL EXPOSURE
• Toxoplasma gondii
• Cryptosporidium
• Coccidiodes
• Histoplassma capsulatum
• Cryptococcus neoformans
• Aspergillus

HOW DO WE GET EXPOSURE
• Daily living: candida,MAC,Cryptococcus
• Geography : histoplasma,cocidioides
• Work related : Aspergillus ,histoplasma
• Hobbies : toxoplasma, cryptococcus ,

PREVENTION
• Wash hands
• Protective gears
• To minimize risk of histoplasma, people with CD4 count <150 cells should aviod,:
• Cleaning, remoldeling,or demolishing old buildings
• Cave exploration
• Contact with bird or bat dropping

OTHER INDIVIDUALS
• Activities and employment
• Health care facilities ,correctional institutions
• Child care providers,CMV,Cryptococcus ,HEP A.

PREVENTION
• Test for latent TB: PPD>5mm, rule out active disease
• Significant exposure to TB,should be treated for latent TB infection regardless of PPD result,(isoniazid for 9 months)

ANIMAL EXPOSURE
• Toxoplasma
• Cryptosporidium
• Salmonella
• Campylobacter
• Bartonella
• Brucella
• Cryptococcus
• M .avium and marinum

EXPOSURE
• OCCUPATION: Vets,pet stores,farms e.t.c
• AVIOD : Bite,scratch,by these animal ,

VACINES IN HIV
• Vacines have better efficacy when CD4 count is >200
• If vacines are give when CD4 Count are less 200,consider repeating when CD4 counts is >200-300
• Live vacines required special consideration because of chances of developing active infection






























