Embed Size (px)
Citation preview

Minimally invasive
endodontics
Dr. Jagadeesh. K P.G 3rd year

Contents
• Definition
• Introduction
• Principles of access cavity preparation
• Minimally invasive access strategies
• A new model for endodontic access
• Endodontic working width
• PIPS
Definition
• The world congress of MID defines minimally
invasive dentistry as those techniques, which respect
health, function and esthetics of oral tissue by
preventing disease from occurring, or intercepting its
progress with minimal tissue loss (Nový and Fuller
2008)

Primary goals of endodontics ???
Tooth retention
Prevention/management of pulpal and periapical disease

PRESERVING STRUCTURAL INTEGRITY
Maintaining strength and stiffness that resists structural deformation becomes the recognized goal of all restorative procedures, especially in endodontics.


Endodontically treated teeth are more brittle and hence more vulnerable to fracture??
Only moisture loss of 9% after root treatment. The predominant reason that endodontically treated
teeth are more prone to fracture relates more than any other attribute to the structural loss of those root treated teeth requiring restoration.
Helfer A R, Melnick S, Schilder H. Determination of the moisture content of vital and pulp less teeth. Oral Surg Oral Med Oral Pathol 1972; 34: 661–670

Unfortunately, structural loss alone cannot answer every clinical question that relates to dentin failure.

• The relevance of fatigue as a main mechanism for
tooth fracture and the resistance of dental tissues
to both the initiation and propagation of cracks is
an important research area
• The resistance to propagation of fatigue cracks in
dentin decreases with increasing patient age and
the incremental rate of crack extension is up to
100 times greater in seniors.

Why endodontically treated teeth fail?
• When endodontically treated teeth fail under function,
that outcome is determined primarily by 2 aetiologies.
Those causes stated most simply are:
1) the degree of stress experienced by the tooth under load
2) the inherent biomechanical properties of the remaining
structure responsible for resisting fracture.

PRINCIPLES IN ACCESS PREPARATION
Do no harm.
Assessment of restorability.
SLA???
External root surface as guide
• Patterns in orifice location, size, colour, shape: 9
LAWS.
(Krasner P, Rankow HJ. Anatomy of the pulp chamber
floor; JOE 2004,30:5)


MINIMALLY INVASIVE ACCESS STRATEGIES
• Important factors that will affect the ultimate
outcome of treatment
• Operator needs,
• Restoration needs,
• Tooth needs.

• Traditional endodontic access has been
endodontic centric, primarily focused on operator
needs, and has been decoupled from the
restorative needs and tooth needs.
• Balance needs to be restored to these 3 needs,
which are almost always in conflict when
performing complete cusp-tip to root-tip
treatment.

SETTING THE STAGE FOR CONTEMPORARY
MOLAR ENDODONTIC ACCESS


• Directed dentin and enamel conservation is the
best and only proven method to buttress the
endodontically treated molar.
• No man-made material or technique can
compensate for tooth structure lost in key areas of
the PCD.
• The primary purpose of the redesigned access is
to avoid the fracturing potential of the
endodontically treated molar

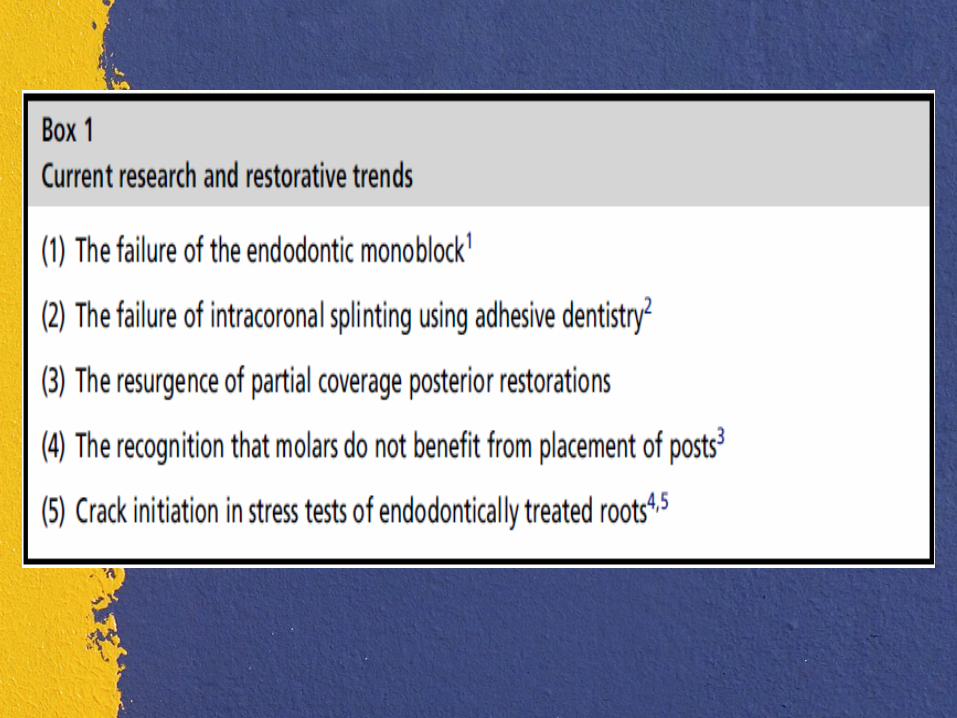
A NEW MODEL FOR ENDODONTIC ACCESS
1. Implant success rates2.Operating microscopes and micro-
endodontics3. Biomimetic dentistry4. Minimally invasive dentistry5. Esthetic demands of patients.
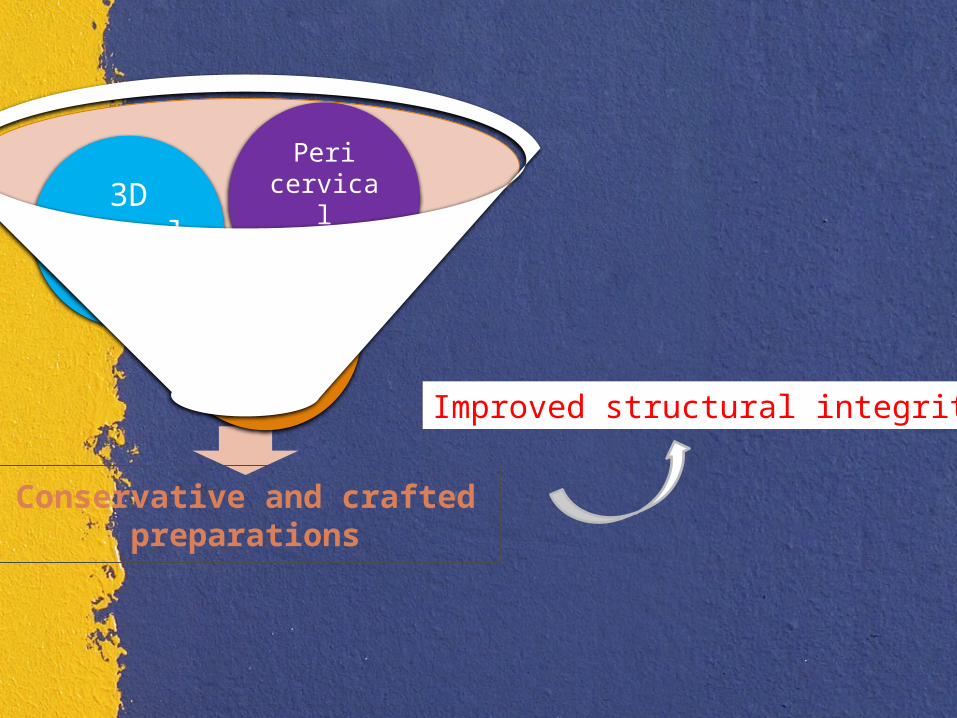
Conservative and crafted preparations
Sofitt
3D Ferrule
Peri cervical dentin
Improved structural integrity

Three-Dimensional Ferrule
• It has historically been described as axial wall
dentin covered by the axial wall of the crown
(or bridge abutment restoration). The research
varies on the actual minimal vertical amount
required, but the range of absolute minimums
is from 1.5 to 2.5 mm

3 components of three dimensional ferrule
Net taper
thickness
Vertical component

Thickness of ferrule
• The absolute minimum thickness is 1 mm; however, 2
mm is obviously a safer number. Girth becomes more
important closer to the finish lines of the preparation.
• The thickness of the remaining dentin (the wall thickness)
between the external surface of the tooth at the finish line
and the endodontic access is more important apically.
• axially deep finish lines on root structure can be
extremely damaging to 3DF.

Total Occlusal Convergence (TOC) or net taper
3 mm ferrule needed
4 mm ferrule needed
Deep chamfer marginal zones common with today’s porcelain
crowns
Needed how much ferrule???
• Light axiomarginal reduction coupled with
apically placed finish lines and a nonzero-
degree emergence profile of the restoration can
provide high 3DF. The concept of 3DF
incorporates an interplay between these factors
that, in sum, indicate the true ferrule quality.

Pericervical dentin (PCD)
Defined as the dentin near the alveolar crest.
• Critical zone roughly 4 mm coronal to the crestal bone -4
mm apical to crestal bone. crucial -transferring load from
the occlusal table to the root,
• PCD is irreplaceable.
No man-made material or technique can compensate for
tooth structure lost in key areas of the PCD.
Clark D, Khademi J. Modern molar endodontic access and directed dentin conservation. Dent Clin North Am 2010

LOOK, GROOM, AND FOLLOW: SHAPING VERSUS MACHINING

Why are round burs so destructive?


Why is complete deroofing so dangerous?
• attempts at removing the soffit that are far
more damaging to the surrounding PCD.
• The primary reason to maintain the soffit is to
avoid the collateral damage that usually occurs,
namely the gouging of the lateral walls.
• This 360 soffit or roof-wall interface can also
be compared with the metal ring that stabilizes
a wooden barrel.
Banking/Soffit (360)(Stepped access)
Small border amount of the chamber roof near the point where it curves 90° and becomes the wall LEFT BEHIND
Tiny “lip” or “cornice” 0.5 mm- 3.0 mm (strength and anatomy). strength continuous ring of dentin (BRAZING EFFECT).

Dotted line shows the typical cut made to remove the entire pulp horn. Area between the lines should be maintained and is referred to as the soffit

Bend and flex at the cervical area - most common area of occurrence for fracture failures in endodontically treated teeth
Robust coronal dentin -maintained good distance away from the tooth’s centroid,(cervical) - tooth is stiffened, resists bending, and should resist fracturing.
Clark D, Khademi J, Herbranson E. Fracture resistant endodontic and restorative preparations. Dent Today 2013.


Preservation of the roof-wall interface (or soffit). the small shapes, and preservation of key dentin.

Redesigned Access• The new vision-based mental model is Look, Groom,
and Follow.
• The new instruments are all round-ended tapers
• The rounded ends are to increase the radii of the gouges
and nicks that can act as stress concentration points.
• The flat sides help create smoother, flatter walls and
minimize the gouges and dings that inevitably occur even
with the most careful technique
• Small, cone-shaped, low-speed bur (such as the EG2 [SS
White ])

CK burs or EndoGuide burs

Blind Tunneling



The enamel is cut back at 45 with the Cala Lilly shape. This modified preparation will now allow engagement of nearly theentire occlusal surface.

The Three Strikes Rule
(1) Excessive axial reduction (consistent with PFM or all-
porcelain restorations)
(2) Gouged endodontic access
(3) Large and arbitrarily round endodontic shape.
Undesirable access shapes
• The inverse funnel
• Blind tunneling
• Blind funneling

SHAPING THE ROOT CANAL SPACE
• Complex root canal anatomy should be considered one of
the most significant challenges in creating root canal
shapes that will support good obturation outcomes and
leave sufficient remaining strength in the root.
• After biomechanical instrumentation, the completed root
canal shapes need to withstand the internal compressive
forces of obturation; provide sufficient resistance form to
contain softened and compressible filling materials and
retain enough strength for mastication.

• Jou et al. coined the term ‘working width’ to alert
clinicians to the critical need to understand the horizontal
dimension of apical size and its clinical implication in
cleaning the apical terminus.
• Larger apical sizes -some literature credibility- bacterial
reduction
• “maintaining smaller sizes when possible (>20 ≤ 40)
desirable-preservation of radicular dentin methods of
canal cleaning and disinfection not at cost of losing
retained, sound tooth structure”
• James L Gutmann on MIE JCD 2013 (Guest editorial)

#30,#40 better than #20 - LARGER TAPER may compensate smaller sizes
Baumgartner et al; JOE 2004
• Root canal preparation instruments sometimes associated
with this strategy such as V‑Taper (SS White, Lakewood,
NJ, USA) and Endo-EZE AET (Ultradent, South Jordan
UT, USA) have not been shown to actually perform in a
superior way to traditional rotary instrumentation in the
laboratory
• Current Descriptions Of Horizontal Dimensions Of Root Canal
• Round(circular): Max IWW=Min IWW• Oval: Max IWW > Min IWW (2 times more)• Long oval: 2 or more times larger (upto 4)• Flattened(ribbon): 4 or more
Circumferential filing better for oval, long oval & ribbon shaped canals
Jou Y.et al; DCNA 2004



Traditional TechnologyStainless-Steel Hand Files
• Inexpensive, has a track record, usually safe, but…
• Time consuming
• Inflexible - difficulty negotiating curved canals
• Extrude debris periapically
• Pack debris into recesses
• Sequential irrigation
Issues with Rotary NiTi Files
• Peer-reviewed research has shown, so far, the following
consequences:
• Unpredictable File separation – even with advanced
metallurgy and reciprocation
• Excessive removal of dentin – especially with high-taper
systems
• Periapical debris extrusion – especially with reciprocation
• Packing of debris into recesses

• Efficiency of NaOCl is reduced when used with single-
file systems, due to shorter working time and non-
sequential work
• Formation of dentinal Micro-cracks, especially with
single-file systems

Cone beam CT presenting oval cross-sections of canals




• Achieve minimally-
invasive
• 3D root canal shaping,
cleaning
• and simultaneous Irrigation.

Abrasive surface

Compression

Gradual expansion by the SAF

1. Vertical vibration – 0.4 mm amplitude at 5,000 rpm
2. Slow low-torque rotation – at ~80 rpm
3. Clutch mechanism to avoid rotation while engaged with canal walls
4. Continuous irrigation


Hero Shaper ProTaper (complete fracture)
SAF

Dentinal micro-Crack Formation during Root Canal Preparations by Different NiTi Rotary Instruments and the Self-Adjusting File
Yoldas et al, J Endod 2012; 38:232-235


C-Shaped canals - Danger zone
Green - before preparation Red - after preparation
Solomonov et al, J Endod 2012; 38:209-214
SAF ProTaper

PIPS

conclusion

REFERENCES• Clark D, Khademi J. Modern molar endodontic access
and directed dentin conservation. Dent Clin North Am
2010
• Clark D, Khademi J, Herbranson E. Fracture resistant
endodontic and restorative preparations. Dent Today
2013
• Clark D, Khademi J, Herbranson E. The new science
of strong endo teeth. Dent Today 2013.
• Yi-Tai Jou et al Endodontic Working Width: current
concepts and techniques

• Helfer A R, Melnick S, Schilder H. Determination of the
moisture content of vital and pulp less teeth. Oral Surg Oral
Med Oral Pathol 1972; 34: 661–670
• Sedgley C M, Messer H H. Are endodontically treated teeth
more brittle? J Endod 1992; 18: 332–335.
• Krasner P, Rankow HJ. Anatomy of the pulp chamber floor;
JOE 2004,30:5
• Reeh E S, Messer H H, Douglas W H. Reduction in tooth
stiffness as a result of endodontic and restorative procedures.
J Endod 1989; 15: 512–516.

• Minimally invasive endodontics: challenging prevailing
paradigms A. H. Gluskin, C. I. Peters and O. A. Peters
• Pathways of pulp 10th ed. stephen cohen

Thank u