Embed Size (px)
DESCRIPTION
lec 2 immunology
Citation preview


II. Acquired (specific or adaptive)
immunity
•The adaptive immune system is
composed of highly specialized,
systemic cells & processes that
eliminate or prevent pathogenic
challenges.

• The adaptive immune response has
the ability to recognize and
remember specific pathogens (to
generate immunity), and to mount
stronger attacks each time the
pathogen is encountered.
•It is adaptive immunity because the
body's immune system prepares
itself for future challenges.

Antigen or Immunogens
•Antigen is a foreign substance of
high molecular weight that
induces a specific immunological
response in the form of antibody
mediated immunity (AMI), or
cell-mediated immunity (CMI) or
both.
Ag: antibody generator.

Molecules differ in their
effectiveness in stimulating Ab
production as proteins &
polysaccharides are generally
good antigens, whereas lipids &
DNA are rarely antigenic.

Epitope: is a part of antigen
recognized by the immune system
(antibody).
Any given antigen may have several
epitopes.
Each epitope is recognized by a
different antibody.


Ags are large molecules ( high M.W).
Hapten: partial antigen, specific non
protein substance which does not itself
elicit antibody formation but elicit the
immune response when coupled with
carrier protein.
As Penicillin: has low M. W. & by itself
is not an antigen, in body changed by
enzyme result in molecule that can
combine with large protein carrier to
form antigenic hapten carrier complex.

Origin of Antigens
1. Exogenous Antigens: Ags that
have entered the body from the
outside by inhalation, ingestion,
or injection.

2. Endogenous Antigens:
Ags generated within the cell, as a
result of normal cell metabolism,
or because of viral or intracellular
bacterial infection.

3. AutoAntigens:
Is usually a normal protein that is
recognized by the immune system
of patients suffering from a
specific autoimmune disease.
These antigens under normal
conditions, not be the target of the
immune system.

Types of antigen
A.Heterologous antigen:
is an Ag derived from one species
and is capable of stimulating an
immune response in another
species.

B. Homologous Antigen:
is an Ag in an individual of one
species which is capable of
eliciting an immune response in
genetically different individual of
the same species e.g. RBCs &
tissue Antigens.

C. Heterophile Antigens(common
to more than one species):
Antigens share the antigenic
determinants & the Antibody
formed to any of them could react
with the other (cross reaction).
Cross reactivity: reaction between
antibody & antigen that differ
from the immunogen.

a. Human heart valve tissue &
certain Antigen found in
Steptococcus pyogenes.

b. Forssman Antigen: glycopeptide
heterophile protein found in
certain animals as dog, horse, cat,
sheep (RBCs), pneumococci
which valuable in determining
infection with mononucleosis;
antibody formed in human react
with Forssman antigen on sheep
RBCs & make hemolysis of the
blood.

Antibody structure



Antibody structure
Monomer: A flexible Y-shaped
molecule with four protein chains:
2 identical light chains (L)
polypeptide chain of about 200
amino acids.
2 identical heavy chains (H)
polypeptide chain of about 450
amino acids.

These two chains are held
together by disulfide bonds.
Ab molecules combined with
large Ag molecules form different
angles around this flexible area,
& the arms of the Y rotate to
bring the variable regions of the
molecule into contact with the
Ag.

Constant Regions: Stem of
monomer & lower parts of Y arms.
The constant regions for all
molecules of the same antibody
class have the same amino acid
sequence & determines the
mechanism used to destroy antigen.
Fc region: Stem of monomer only
important because they can bind to
complement or cells.

Variable Regions: Two sections at
the end of Y’s arms. Contain the
antigen binding sites (Fab).
Identical on the same antibody,
but vary from one antibody to
another.

Ab Binding Sites
Typically, an Ab molecule has two
identical binding sites, one at the end
of each arm of the Y.
Ag-Ab relationships like lock & Key.
•In order for an Ag-Ab reaction to
be triggered, there must be a close
physical & chemical complementary
fit between the two.

1.Van der Waal's forces:
attract all molecules through their
electron clouds.
2.Hydrogen bonding:
electromagnetic interaction between
polar molecules in which hydrogen
is bound to a highly electronegative
atom as (N) or (O), strong than van
der waal’s

3. Electrostatic: attraction between
Ab & Ag molecules due to
electrically charged particles.
4. Hydrophobic regions: attracted in
an aqueous environment; this is
probably the strongest force
between them.
Affinity: the measure of binding
strength of antigen antibody
interaction.


Immunoglobulin isotype Heavy chain
IgG g
IgA a
IgD d
IgE e
Immunoglobulin Classes
IgM m

I. IgM
Structure: Pentamer
Percentage serum antibodies: 5-10%
Location: Blood, lymph, B cell surface.
Half-life in serum: 5 days
Complement Fixation: Yes
Placental Transfer: No
Known Functions: First antibodies
produced during an infection.

II. IgA (2 subclasses, IgA1-2)
Structure: Dimer
Percentage serum antibodies: 10-15%
Location: Secretions (tears, saliva, intestine,
milk), blood & lymph.
Vibrio cholerae, Streptococcus mutans, and
Neisseria gonorrhoeae will not bind to cell
surfaces in the presence of secretory IgA.
Some pathogenic bacteria produce an
enzyme splits the secretory IgA (IgA
protease).

Half-life in serum: 6 days
Complement Fixation: No
Placental Transfer: No
Known Functions: Localized protection of
mucosal surfaces.

III. IgG (4 subclasses, IgG1-4)
Structure: Monomer, has 2 epitope-
binding sites.
Percentage serum antibodies: 80%
Location: Blood, lymph, intestine
Half-life in serum: 23 days
Complement Fixation: Yes
Placental Transfer: Yes
Known Functions: Enhances
phagocytosis, neutralizes toxins &
viruses, protects fetus & newborn.

IV. IgE
Structure: Monomer
Percentage serum antibodies: 0.002%
Location: Bound to mast cells and
basophils
Half-life in serum: 2 days
Complement Fixation: No
Placental Transfer: No
Known Functions: Allergic reactions.
Possibly lysis of worms.

V. IgD
Structure: Monomer
Percentage serum antibodies: 0.2%
Location: B-cell surface, blood, and lymph
Half-life in serum: 3 days
Complement Fixation: No
Placental Transfer: No
Known Functions: initiate immune
response.


Consequences of Antigen-
Antibody Binding

1. Agglutination: Antibodies cause antigens (microbes) to clump together.

2. Opsonization: Antigen (microbe) is covered with antibodies that enhances
its ingestion & lysis by phagocytic cells.

3. Neutralization: IgG inactivates pathogen
by binding to their surface & neutralize
toxins by blocking their active sites.

4.Antibody-dependent cell-mediated
cytotoxicity: Used to destroy large
organisms (e.g.: worms). Target
organism is coated with antibodies &
bombarded with chemicals from
nonspecific immune cells.

5. Complement Activation: Both IgG & IgM
trigger complement system which results in cell
lysis.

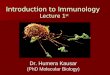
Pattern of Antibody Levels During
Infection
Primary Response:
–After initial exposure to antigen, no
antibodies are found in serum for
several days.
–A gradual increase in antibody, first
IgM is observed.
–Gradual decline of antibodies follows.

Secondary Response:
Subsequent exposure to the same
antigen displays a faster & more
intense antibody response.
A secondary response usually involves
a change in Ab class, often from IgM to
IgG.
This is known as class switching and is
mediated by IL-4 produced by the Th
cell that activates the memory B-cell.

Antibody Response After Exposure to Antigen
IgM
IgG
Class switch

Three important feature of the
immunological response
1. Specificity. An Ab or reactive T-cell will
react specifically with Ag that induced its
formation; it will not react with other
Ags.
2. Memory. Once the immunological response
has reacted to produce a specific type of
Ab or reactive T-cell, it is capable of
producing more of the Ab or activated T-
cells rapidly & in larger amounts.

3. Tolerance. An animal generally does not
undergo an immunological response to its
own (potentially-antigenic) components.
The animal is said to be tolerant to self-
Ags.
This ensures that under normal conditions,
an immune response to "self" Ags (called
an autoimmune response) does not occur.
Autoimmune responses are potentially
harmful to the host.

Types of T-cell
1. Helper T (Th) Cells:
Helper T cells are named for their
ability to help other cells in the
immune system achieve
maximum efficiency.

2. Cytotoxic T (Tc) Cells:
•Cytotoxic T cells kill cells that
have been infected with viruses,
and some tumor cells.
•The cytotoxic T cell secretes a
protein called perforin, which
makes a hole in the cell
membrane, causing the cell to lyse
and die.

3. Regulatory T (Treg) Cells or
suppressor T-cell:
Shutting down the immune response
after they have successfully eliminated
invading organisms.
Maintain the tolerance to the self
antigen.
Modulation of Treg can treat
autoimmune disease, cancer &
facilitate organ transplantation.

Possible mechanisms of this action
1. Inhibit conversion of B-cells to plasma
cells & suppress the activity of some
of the T cells.
2. Absorption of essential cytokines thus
preventing the division of other
lymphocytes.
3.Release of non- specific
immunosuppressive molecules.

4. Delayed Hypersensitivity T (TD)
Cells:
Participate in cell-mediated
reactions but do not interact with
B-cells.
TD cells are responsible for
recruiting & activating
phagocytes.

TS and TC cells recognize Ag
fragments associated with MHC
class I molecules.
TH and TD cells recognize Ag
associated with MHC class II
molecules.

Cytokines
1. IL-1 & IL-2:
Macrophages secrete a potent
cytokine known as IL-1, which
acts on several different cell types.
IL1 binding by IL-1 receptors
(IL-1R) on the Th cell acts as an
activation signal & causes Th cell
to divide, producing clonal copies.

IL-1 is a key component of the immune
response because Th cells are one of its
main targets.
During this activation stage, the
stimulated Th cells begin to make IL-2,
which in turn stimulates other Th & Tc
precursors to form active Tc cells.

IL-2 secreted by Th cells acts with
other cytokines such as IL-4 to
stimulate Ag-activated B-cells to
proliferate & produce antibody
forming plasma cells.
The end result is stimulation of several
cells through the actions of IL-1 & IL-
2, resulting in both humoral & cell-
mediated immune responses.

2. interferon (IFN-α and IFN-ɤ)
Named interferon because it interfere with
viral replication.
Produced by leukocytes & inhibits viral
replication in virtually any cell in the body.
3.Tumor necrosis factors (TNF-α & TNF-β)
Capable of destroying a variety of tumors
provided that TNF-producing cells have
access to the tumor.

The complement system
It is a biochemical cascade which
helps clear pathogens from an
organism.
It is part of the larger immune
system that is not adaptable and
does not change over the course of
an individual's lifetime; as such it
belongs to the innate immune
system.

Over 25 proteins & protein fragments make
up the complement system.
These proteins are synthesized mainly in
the liver, and they account for about 5% of
the globulin fraction of blood serum.
Circulate in the blood as inactive
components.
•When stimulated by one of several
triggers, proteases in the system cleave
specific proteins to release cytokines &
initiate an amplifying cascade of further
cleavages.

The end result of this activation
cascade is massive amplification of the
response & activation of the cell-killing
membrane attack complex.
Membrane attack complex: typically
formed on the surface of pathogenic
bacterial cell as a result of complement
system & forms transmembrane
channels which disrupt the
phospholipid bilayer of the target cell
lead to cell lysis.

Membrane attack complex or Lytic complex


Three biochemical pathways activate
the complement system:
1. The classical complement
pathway.
2. The alternative complement
pathway.
3. Mannose-binding lectin pathway.

1- Classical pathway (adaptive immunity)
Activation of the C1-complex (C1q, C1r,
and C1s), which occurs when C1q binds to
IgM or IgG complexed with Ags.
C1 bind & split C4 & then C2 produce C2a
& C4b.
C2a & C4b bind to C3 convertase which
promote clevage of C3 into C3a & C3b.
C3a & C3b bind to C2a & C4b to make C5
which enhance phagocytosis.

2- Alternative pathway (innate
immunity)
The alternative pathway is triggered
by C3 hydrolysis directly on the
surface of a pathogen.
It does not rely on a pathogen-binding
protein like the other pathways.
C5a and C3a are known to trigger
mast cell degranulation.

3- Lectin pathway (Mannose-binding
lectin or MBL) (innate immunity)
The lectin pathway is homologous to
the classical pathway, but with the
opsonin, mannose-binding lectin
(MBL) & ficolins, instead of C1q.
This pathway is activated by binding
mannose-binding lectin to mannose
residues on the pathogen surface,
which activates the MBL-associated
serine proteases.

MASP-1 & MASP-2 very similar to C1r &
C1s respectively), which can split C4 & then
C2 produce C2a & C4b.
C2a & C4b bind to C3 convertase which
promote cleavage of C3 into C3a & C3b.
C3a & C3b bind to C2a & C4b to make C5
which enhance phagocytosis.
Ficolins (homologous to MBL): group of
oligomeric lectin with subunits of
fibrinogen like, collagen like molecules &
lectin.

Complement System

The Biological Effects of Complement
1.Opsonization: The C3b molecules are
opsonins which are any molecules
enhance phagocytosis such as antibody
or complement spilit .

2. Inflammation: The C5a and C3a
fragments are important inflammatory
activators inducing vascular
permeability & activation of
phagocytes.
3. Lysis: C5b binds & recruits C6 & C7
to the target surface
4.Immune complex clearance:
Complement has a very important role
in solubilizing & causing removal from
the circulation of immune complexes.

Immunization
Immunization: is the process by
which an individual's immune system
becomes fortified against an agent
(known as the immunogen).
Immunization can be done through
vaccination. Vaccines against M.O.s
that cause diseases can prepare the
body's immune system, thus helping
to fight or prevent an infection.

Types of Immunization
1. Naturally Acquired Immunity: Obtainedin the course of daily life.
A. Naturally Acquired Active Immunity:
– Antigens or pathogens enter bodynaturally.
– Body generates an immune response toantigens.
– Immunity may be lifelong.

B. Naturally Acquired PassiveImmunity:
– Antibodies pass from mother to fetusvia placenta or breast feeding.
– No immune response to antigens.
– Immunity is usually short-lived (weeksto months).
– Protection until child’s immune systemdevelops.

2. Artificially Acquired Immunity(vaccination):
Obtained by receiving a vaccine or immuneserum.
A. Artificially Acquired Active Immunity:
– Antigens are introduced in vaccines(immunization).
– Body generates an immune response toantigens.
– Immunity can be lifelong (oral poliovaccine).

B. Artificially Acquired PassiveImmunity:
– Preformed antibodies are introducedinto body by injection.
– Immunity is short lived (half life threeweeks).
– Host immune system does not respondto antigens.

Who should not be vaccinated?
Women who are pregnant (or plan a
pregnancy in the near future).
People with weakened immune systems
should not get live virus vaccines.
People who have had a major allergic
reaction to a specific vaccine or one of its
components should avoid revaccination
with that vaccine.

How are vaccines made?
•Vaccines are made in several
different ways.
1. Inactivate (killed vaccine, 3 doses):
grown in culture then killed using
method such as formaldehyde.
Viral: polio.
Bacterial: diphtheria, pertusis,
tetanus vaccines (DPT).

2. Attenuated (weakened live vaccine,
one dose):
Bacterial: BCG against T.B.
Viral: measles vaccine.
Immunity from a live virus vaccine is
generally lifelong. However, these
“live virus” vaccines should not be
given to people who are
immunocompromised, such as some
people with cancer or AIDS.

Immune tolerance
Specific non reactivity of the immune
system to a particular antigen.
1.Innate tolerance
Innate tolerance is the body's tolerance
for its own Ags & proteins. When
natural tolerance fails, or when the
body does not properly recognize itself,
an autoimmune disorder results.

2. Acquired tolerance
Acquired or induced tolerance is the
immune system's tolerance for
external Ags.
Such as medication used to avoid
transplant rejection.

Immunodeficiency
In medicine, immunodeficiency (or
immune deficiency) is a state in which
the immune system's ability to fight
infectious disease is compromised or
entirely absent.
A person who has an
immunodeficiency of any kind is said
to be immunocompromised.

Primary immune deficiency diseases:
The World Health Organization
(WHO) recognizes over 100
primary immune deficiency
diseases. The most common types of
primary immune deficiency
diseases:

1. X-Linked Agammaglobulinemia
(XLA)
Congenital.
Low or absent IgG due to failure of B-
lymphocyte precursors to mature into
B-lymphocytes & plasma cells. Since
they lack the cells responsible for
producing antibodies.
The gene responsible for maturation
found in X-chromosome, so the disease
mainly found in boys.

2. Common Variable Immunodeficiency
(CVID)
Normal B cell but with low levels of
antibody production.
It is a relatively common form of
immunodeficiency, hence, the word
“common.” The degree and type of
deficiency of serum immunoglobulins, and
the clinical course, varies from patient to
patient, hence, the word “variable.”

3. The X-Linked Hyper IgM Syndrome
Patients with the disease have an
inability to switch their Ab production
from IgM to IgG, IgA, and IgE.
As a result, patients have decreased
levels of IgG & IgA & normal or
elevated levels of IgM.
The most common form is inherited as
an X-chromosome & affects only boys.

4. Selective IgA Deficiency
Individuals with Selective IgA
Deficiency lack IgA, but usually have
normal amounts of the other types of
immunoglobulins.
Most affected people have no illness as
a result.
Others may develop a variety of
significant clinical problems & increase
risk of respiratory, GIT & urogential
disorders.

5. IgG Subclass Deficiency
The IgG class of immunoglobulins is itself
composed of four different subtypes of
IgG molecules called the IgG subclasses.
Patients who lack, or have very low
levels of, one or two IgG subclasses, but
whose other Ig levels are normal, are said
to have a selective IgG subclass
deficiency.
Defects occur in heavy chain genes in the
regulation of isotypes.

6. Severe Combined Immunodeficiency
(SCID)
Severe Combined Immunodeficiency is an
uncommon primary immunodeficiency in
which there is combined absence of T-
lymphocyte and B-lymphocyte function.
This condition is most serious of the
primary immunodeficiencies.
bone marrow transplantation, exist that
can cure the disorder and the future holds
the promise of gene

7. The Wiskott Aldrich Syndrome
Primary immunodeficiency disease
involving both T- and B-lymphocytes.
Platelets are also affected lead to
thrombocytopenia.

8. The DiGeorge Syndrome
Developmental defect in the thymus
gland & T-lymphocyte production
may be impaired, resulting in
recurrent infections.

9. Ataxia-Telangiectasia (neurologic
abnormalities)
Variable immunodeficiency involving
both cellular (T-lymphocyte) &
humoral (B-lymphocytes) immune
responses.
Destroy parts of the motor control area
of the brain leading to an unbalance
(ataxia), dilated blood vessels
(telangiectasia) of the eyes & skin.

10. Chediak-Higashi Syndrome
Hereditary fatal disease results from
the slow fusion of the lysozymes to
the phagosomes & hence ingested
bacteria are not destroyed.

Acquired immunodeficiency
Immune deficiency as a result of
particular external processes or
diseases"secondary“
immunodeficiency.
Common causes:
anti-rheumatic
Immunosuppressive drugs

Many specific diseases:
1. cancer with bone marrow &
blood cells.
2. acquired immunodeficiency
syndrome (AIDS), caused by the
human immunodeficiency virus
(HIV).

Hypersensitivity

Nearly 40 years ago Gell and
Coombs proposed a classification
scheme which defined 4 types of
hypersensitivity reactions.
The first 3 are mediated by Ab, the
fourth by T cells.

I.Type I Hypersensitivity (anaphylactic
reaction)
Immediate hyper sensitivity reaction to
exogenous antigen mediated by IgE.
Such as:
Hay fever (allergic rhinitis; allergic
condition affect mucous membrane of the
upper repiratory tract & eyes,
characterized by nasal discharge,
sneezing, itching, watery eyes caused by
abnormal sensitivity to airborne pollen.),

Eczema: pruritic dermatitis characterized
by erythema, edema, serous exudate in
the epidermis.
Asthma: chronic inflammatory disease of
the airways, inflammation cause the air
way to spasm & swell so the airway
narrow.
Urticaria: a vascular reaction of the the
skin marked by apprance of elevated red
batches with severe itching.

The high affinity IgE receptors are found
on mast cells & basophils. Each cell has a
high density of these receptors (40-
250,000 per cell) so that a wide spectrum
of Ag specificities is represented.
Such cross-linking leads to rapid
degranulation (60-300 secs) of the mast
cells & the release of primary
inflammatory mediators stored in the
granules.

These mediators cause all the normal
consequences of an acute inflammatory
reaction, increased vascular permeability,
granulocyte chemotaxis.
Mast cell activation via IgE also leads to
the production of two other types of
mediators. These secondary mediators,
unlike the stored granule contents, must
be synthesized de novo & comprise
arachadonic acid metabolites (essential
fatty acid) (prostaglandins &
leukotrienes).


Allergens
Ags that trigger allergic reactions &
provoke IgE-mediated responses.
Typical allergen sources include
pollens, food, insect venoms, fungal
spores and the feces of the HDM
(Human dust mite).

There are two types of allergic
reaction according to mode of entry
of the allergen:
1. Local (atopic) allergy
Occurs after inhalation or ingestion
of the allergen & causes a localized
reaction such as asthma, hay fever.

2. Systemic anaphylaxis
The consequences of a generalized
reaction are potentially fatal.
Ingestion of nuts or seafood, insect
bites (venom), & drug injection may all
cause life-threatening reactions in
highly sensitized individuals.

Death in such cases is due to systemic
release of vasoactive mediators
leading to general vasodilation &
smooth muscle contraction resulting
in sudden loss of blood pressure,
massive edema & severe bronchiole
constriction (systemic anaphylaxis).

Diagnostic tests for immediate
hypersensitivity
Include skin (prick & intradermal) tests
measurement of total IgE & specific IgE
antibodies against the suspected
allergens.
Total IgE & specific IgE measured by a
(ELISA).
Drop of allergy-producing substance on
the skin & making breaks by lightly
pricking the surface.


Symptomatic treatment
Antihistamines: block histamine
receptors.
Chromoglycate (mast cell stabilizer):
prevent the release of histamine.
Corticosteroids: used mainly for local
anaphylxis.

Thank You











![immunology-lecture-cellular-immunity [Λειτουργία συμβατότητας]](https://img.dokumen.tips/doc/110x75/616a270f11a7b741a34f5f44/immunology-lecture-cellular-immunity-.jpg)