Embed Size (px)
Citation preview
HYPERTENSION Regulation of Blood pressure
Mohammad Ilyas, M.D.
Assistant Clinical Professor
University of Florida / Health Sciences Center
Jacksonville, Florida USA 1

Outline
1. Definition, Regulation and Pathophysiology
2. Measurement of Blood Pressure, Staging of Hypertension and Ambulatory Blood Pressure Monitoring
3. Evaluation of Primary Versus Secondary
4. Sequel of Hypertension and Hypertension Emergencies
5. Management of Hypertension (Non-Pharmacology versus Drug Therapy)
6. The Relation Between Hypertension: Obesity, Drugs, Stress and Sleep Disorders.
7. Hypertension in Renal diseases and Pregnancies
8. Pediatric, Neonatal and Genetic Hypertension
2
Regulation of Blood Pressure
• There are two basic mechanisms for regulating blood pressure:
(1) Short-term mechanisms, which regulate blood vessel diameter, heart
rate and contractility
(2) Long-term mechanisms, which regulate blood volume
3

Regulation of Blood Pressure
• The body responds to variations in the effective circulating
volume in two steps:
(1) The change is sensed by the pressure receptors; (Sensors)
(2) These receptors then activate a series of effectors that restore
volume by varying vascular resistance, cardiac output, and
renal Na+ and water excretion.
4

Short-Term Regulation
• Rising blood pressure Stretching of arterial
walls Stimulation of baroreceptors in carotid,
sinus, aortic arch, and other large arteries of the
neck and thorax Increased impulses to the brain
from baroreceptors Increased parasympathetic
activity and decreased sympathetic activity
Reduction of heart rate and increase in arterial
diameter Lower blood pressure
5

Baroreceptors
• These are the stretch receptors present in the wall of blood vessel
(Carotid Sinus and Aortic Arch) and Heart (Atria at the junction
of SVC and Pulmonary vein).
• These receptors are located in the adventitia, consist of extensively
branched, knobby, coiled, intertwined ends of myelinated nerve fiber.
• In chronic Hypertension these receptors reset to maintain an elevated
blood pressure.
6

7

Baroreceptors
• Baroreceptors sense stretch and rate of stretch by generating
action potentials (voltage spikes)
• Located in highly distensible regions of the circulation to
maximise sensitivity
8
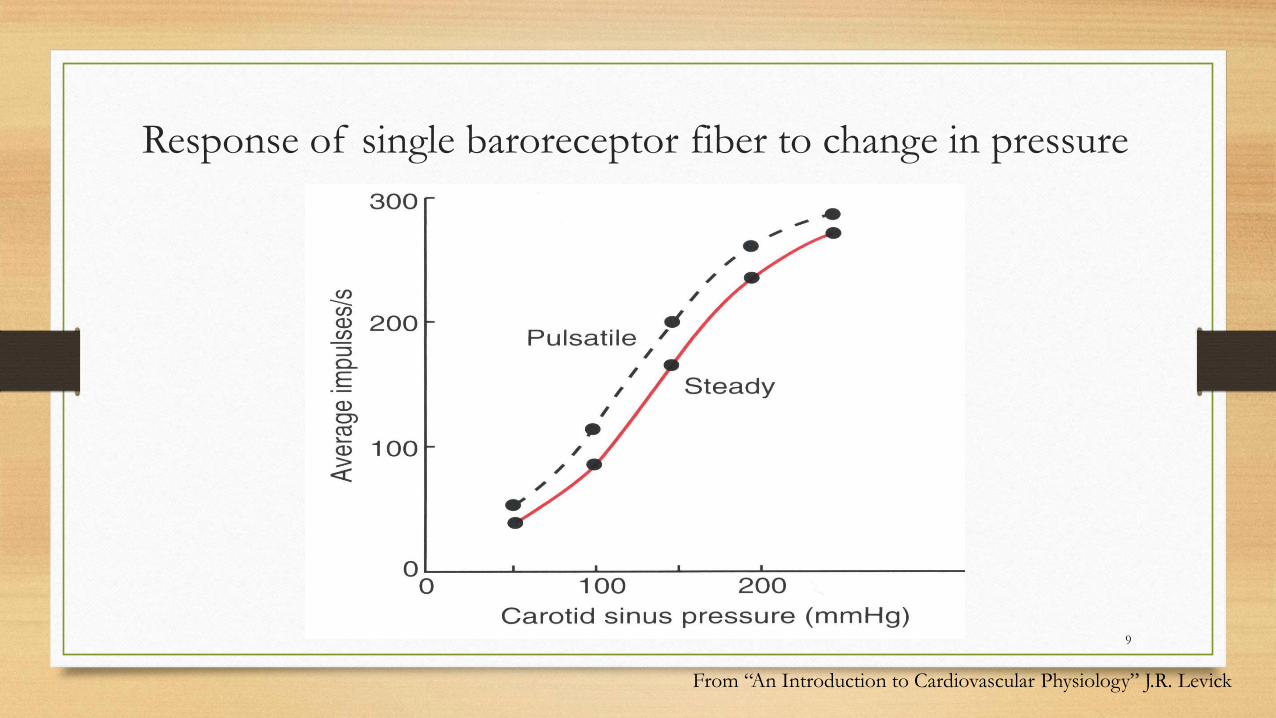
Response of single baroreceptor fiber to change in pressure
From “An Introduction to Cardiovascular Physiology” J.R. Levick
9

These receptors works more effectively in MAP between 80 – 160 mm of Hg.
Carotid sinus receptors are physiologically more important than Aortic arch receptors.
Atrial Baroreceptors are of 2 types:
Type-A- Active during systole.
Type-B- Active during diastole.
Atrial stretch receptors also respond to hypovolemia by increasing the secretion of AVP, Renin and Aldosterone.
10

Increased Parasympathetic Activity
Effect of Increased Parasympathetic and Decreased Sympathetic Activity on Heart and Blood Pressure:
1. Increased activity of vagus (parasympathetic) nerve
2. Decreased activity of sympathetic cardiac nerves
3. Reduction of heart rate
4. Lower cardiac output
5. Lower blood pressure
11

Decreased Sympathetic Activity
Effect of Decreased Sympathetic Activity on Arteries and Blood Pressure:
1. Decreased activity of vasomotor fibers (sympathetic nerve fibers)
2. Relaxation of vascular smooth muscle
3. Increased arterial diameter
4. Lower blood pressure
12

Short-term Regulation of
Rising Blood Pressure
1. Rising blood pressure
2. Stretching of baroreceptors
3. Increased impulses to the brain
4. Increased parasympathetic activity
5. Decreased sympathetic activity
6. Slowing of heart rate
7. Increased arterial pressure
8. Reduction of blood pressure
13

Short-term Regulation of
Falling Blood Pressure
Falling blood pressure Baroreceptors inhibited Decreased impulses to the brain Decreased parasympathetic activity and increased sympathetic activity
Three effects:
1. Heart: increased heart rate and increased contractility
2. Vessels: increased vasoconstriction
3. Adrenal gland: release of epinephrine and norepinephrine which enhance heart rate, contractility, and vasoconstriction
• Increased blood pressure
14
Sympathetic Activity on
Heart and Blood Pressure
Effect of Increased Sympathetic Activity on Heart and Blood Pressure:
1. Increased activity of sympathetic cardiac nerves
2. Decreased activity of vagus (parasympathetic) nerve
3. Increased heart rate and contractility
4. Higher cardiac output
5. Increased blood pressure
15

Vasomotor Fibers
Effect of Increased Sympathetic Activity on Arteries and Blood Pressure:
1. Increased activity of vasomotor fibers (sympathetic nerve fibers)
2. Constriction of vascular smooth muscle
3. Decreased arterial diameter
4. Increased blood pressure
16
Sympathetic Activity on
Adrenal Gland and Blood Pressure
Effect of Increased Sympathetic Activity on Adrenal Glands and Blood Pressure:
1. Increased sympathetic impulses to adrenal glands
2. Release of epinephrine and norepinephrine to bloodstream
3. Hormones increase heart rate, contractility and vasoconstriction.
Effect is slower-acting and more prolonged than nervous system control.
• Increased blood pressure
17

Chemoreceptors
• Very similar to baroreceptors, except that they respond to chemical changes.
• At low O2 or high CO2 or H+ (as occurs during low pressure because of
decreased blood flow), chemoreceptors are stimulated.
• Chemoreceptors excite the vasomotor center, which elevates the arterial
pressure.
18

CNS Ischemic Response
• If blood flow is decreased to the vasomotor center in the lower brainstem
and CO2 accumulates, the CNS ischemic response is initiated.
• Very strong sympathetic stimulator causing major vasoconstriction and
cardiac acceleration.
• Sometimes called the “last ditch stand”.
19

Auto-regulation of Blood Pressure
• It occur both at tissue level (local Regulation) and at systemic level (systemic Regulation)
LOCAL REGULATION:
• Capacity of tissue to regulate its own blood flow is called as Autoregulation.
• It is well developed in kidney and also seen in brain, liver, heart, intestine and skeletal muscle.
20

Auto-regulation of arterioles (in the absence of external stimuli)
Myogenic mechanism
( response to mechanical stimulus):
• Vessels Smooth Muscle (VSM) fiber contract
when it stretched and relaxes when pressure
in the vessel increases.
• Net effect: maintenance of near constant
blood flow for a particular metabolic level.
21

Metabolic mechanism
Accumulation of metabolites like Lactate, Phosphate, histamine, CO2, H+,
NO, K+ and adenosine (Specially in skeletal muscle)
Decrease in O2, and pH, causes vasodilatation in arteriole and increases
the blood flow to the tissue
Whereas increased O2, TXA2, Endothelin, substance-P, serotonin causes
vasoconstriction
22

Chemical Physiologic role Source Type
Nitric oxide (NO) Paracrine mediator Endothelium Local
Atrial natriuretic peptide
ANP
Reduce blood pressure Atrial myocardium, brain
Hormonal
Vasoactive intestinal peptide (VIP)
Digestive secretion, relax smooth muscle
Neurons Neural, hormonal
Histamine Increase blood flow Mast cells Local, systemic
Epinephrine (b2) Enhance local blood flow to skeletal muscle, heart, liver
Adrenal medulla Hormonal
Acetylcholine (muscarinic)
Erection of clitoris, penis Parasympathetic neurons
neural
Bradykinin Increase blood flow via nitric oxide
Multiple tissues Local
Adenosine Enhance blood flow to match metabolism
Hypoxic cells local
Vascular Smooth Muscle (VMS) relaxants
23

Vascular Smooth Muscle (VMS) Contraction
Chemical Physiologic role Source Type
Nor Epi (a ) Baroreceptor reflex Sympathetic neurons Neural
Endothelin Paracrine Vascular endothelium Local
Serotonin Platelet aggregation, smooth muscle contraction
Neurons, digestive tract, platelets
Local, neural
Substance P Pain, increased capillary permeability Neurons, digestive tract Local, neural
Vasopressin Increase blood pressure during hemorrhage
Posterior pituitary Hormonal
Angiotensin II Increase blood pressure Plasma hormone Hormonal
Prostacyclin Minimize blood loss from damaged vessels before coagulation
endothelium local
24

Neural Control
Systemic Regulation
Other than venules and capillaries all vascular system are innervated.
Both cholinergic and adrenergic nerve plexuses lies on adventia and extend branches to the surface of VSM, only the neurotransmitters reach the inner part of VSM by diffusion and exert there effect.
There is no tone in cholinergic system, but the vasoconstrictor fibers are tonically active so sympathectomy causes vasodilatation in most of vessels.
25
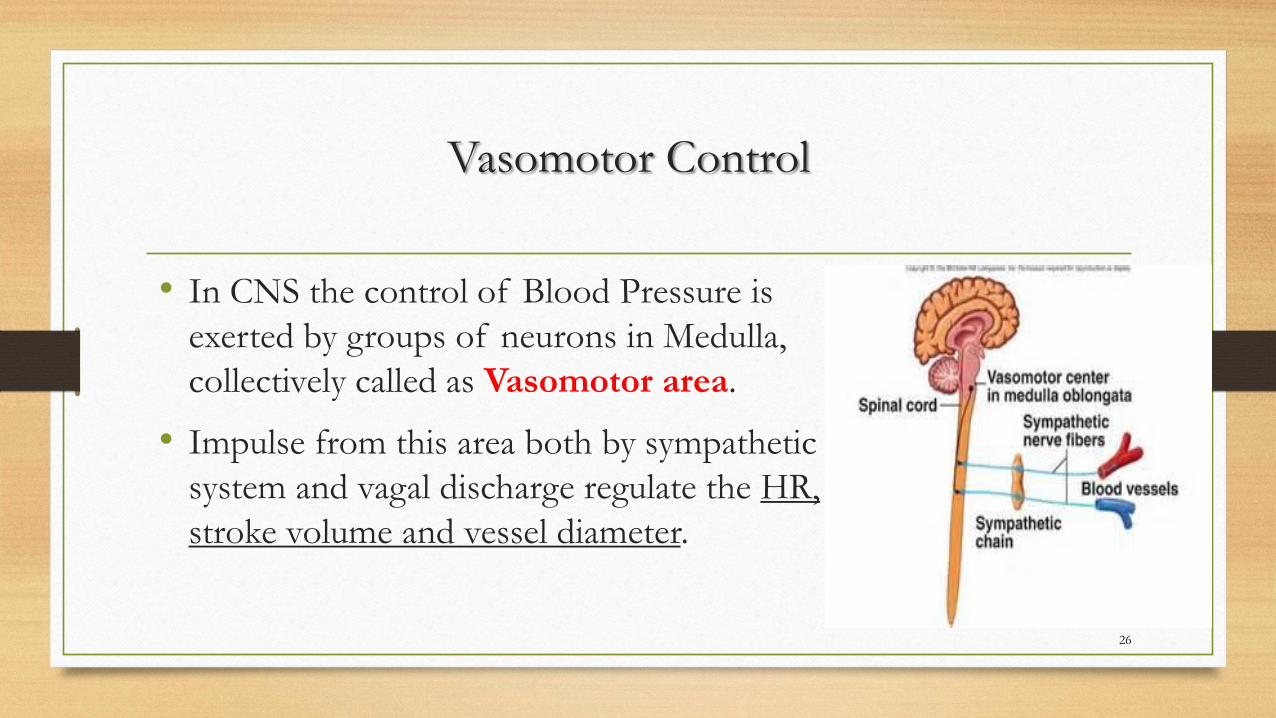
Vasomotor Control
• In CNS the control of Blood Pressure is
exerted by groups of neurons in Medulla,
collectively called as Vasomotor area.
• Impulse from this area both by sympathetic
system and vagal discharge regulate the HR,
stroke volume and vessel diameter.
26

Long-Term Regulation of BP
Long-term regulation of blood pressure is primarily accomplished by altering blood volume.
The loss of blood through hemorrhage, accident, or donating a pint of blood will lower blood pressure and trigger processes to restore blood volume and therefore blood pressure back to normal.
• Renin-Angiotensin System
• Anti-Diuretic Hormone
• Atrial Naturetic Peptide
27
28
Renin-Angiotensin System
• Renin – hormone that acts as an enzyme; released when arterial
pressure drops – i.e., when renal perfusion is inadequate
• Helps raise arterial pressure
• Can be life-saving system in circulatory shock

29

Factors affecting Renin secretion:
Stimulatory:
o Increased sympathetic activity via renal nerve.
o Increased circulating catecholamine.
o Prostaglandins.
Inhibitory:
o Increased Na+ and Cl- delivery to macula densa.
o Increased afferent arteriolar pressure.
o Angiotensin-II.
o Vasopressin
30

Vasoconstriction
NE
31

Arteries
Veins
Reduced renal
blood flow
Juxtaglomerular
apparatus
Renin
Angiotensinogen
Angiotensin I
Angiotensin II
Increased
pre-load
Increased
after-load
vasoconstriction
Increased aldosterone
secretion
Sodium retention
Fluid re-absorption
Increased
blood volume
Renin/angiotensin/aldosterone system (RAAS)
LV filling pressure)
(LV pressure
beginning of systole)
32

Aldosterone Mechanism
• Aldosterone promotes increased reabsorption
of sodium from the kidney tubules.
• Each distal convoluted tubule winds through the
kidney and eventually empties its contents into a
urine-collecting duct.
• The peritubular capillaries absorb solutes and
water from the tubule cells as these substances
are reclaimed from the filtrate.
33
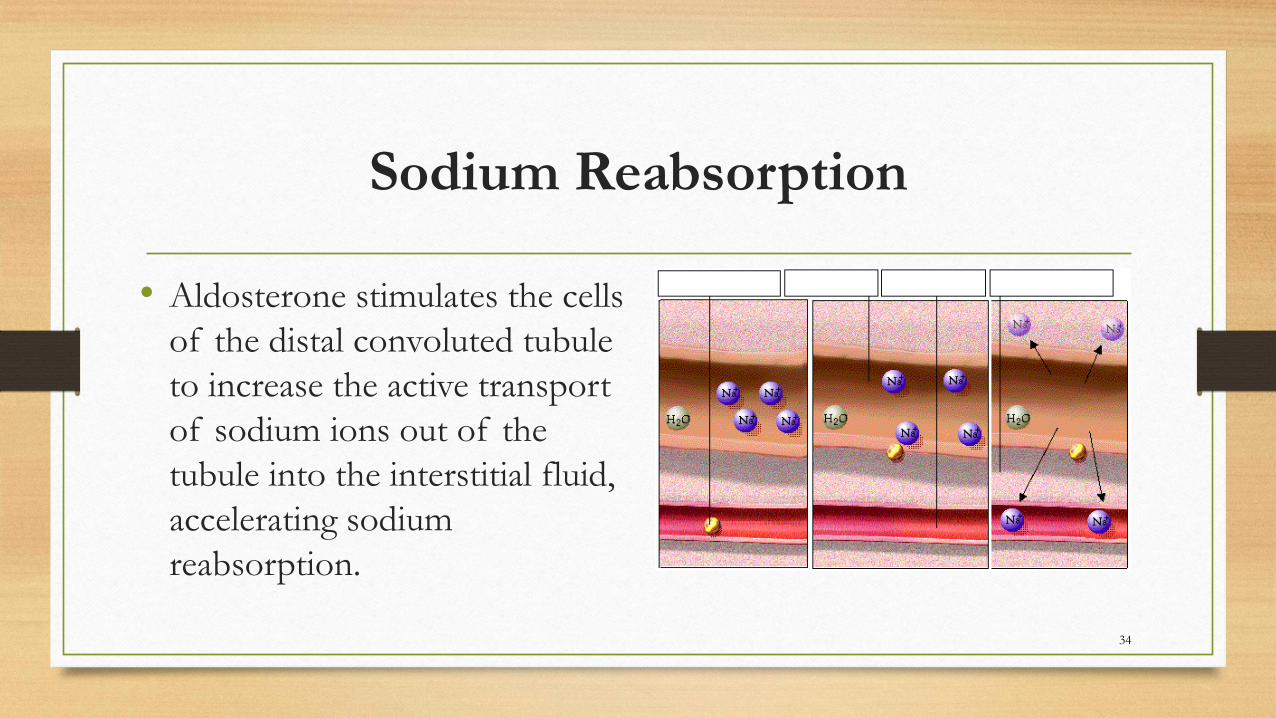
Sodium Reabsorption
• Aldosterone stimulates the cells
of the distal convoluted tubule
to increase the active transport
of sodium ions out of the
tubule into the interstitial fluid,
accelerating sodium
reabsorption.
34

Water Reabsorption
• As sodium moves into the bloodstream, water follows. The reabsorbed water
increases the blood volume and therefore the blood pressure.
35

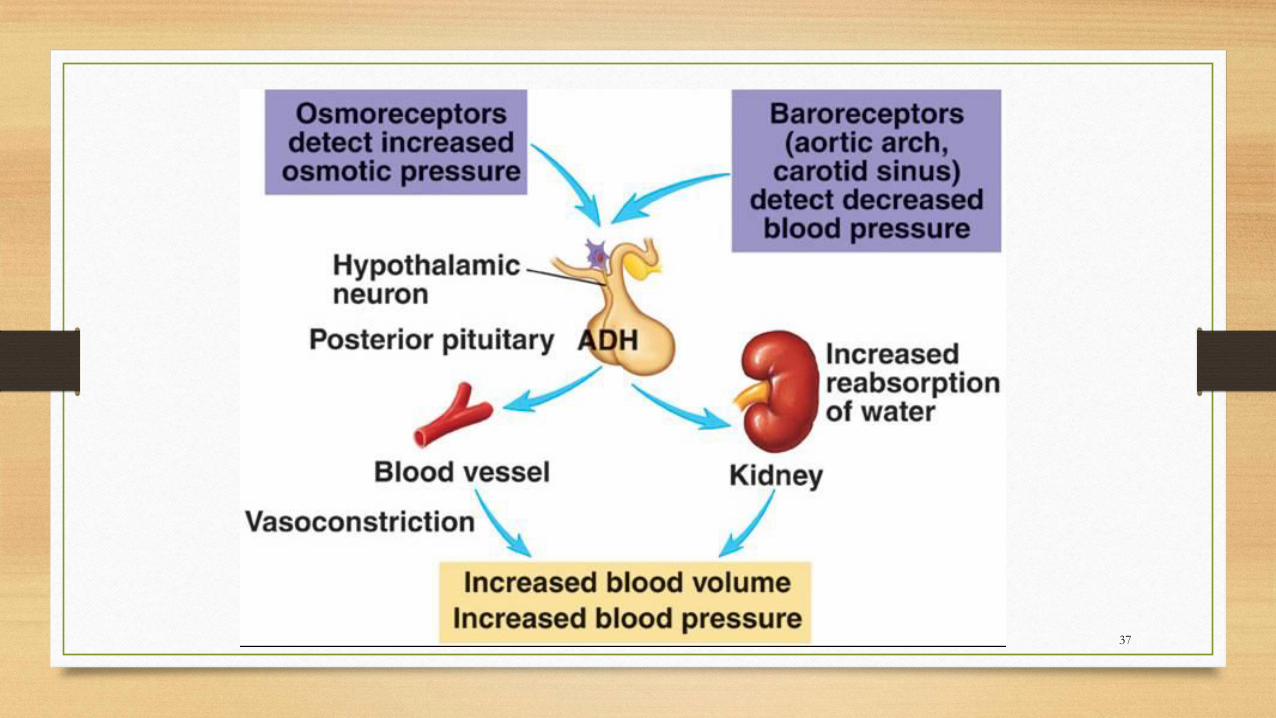
Vasopressin (ADH)
• Arginine vasopressin (AVP), antidiuretic hormone (ADH), Neuro-hypophysial hormone
• Its two primary functions are to retain water in the body and to constrict blood vessels.
• Vasopressin is a peptide hormone that increases water permeability of the kidney's collecting
duct and distal convoluted tubule by inducing translocation of aquaporin-CD water channels in
the kidney nephron collecting duct plasma membrane.
• It is derived from a pre-pro-hormone precursor that is synthesized in the hypothalamus and
stored in vesicles at the posterior pituitary. Most of it is stored in the posterior pituitary to be
released into the bloodstream.
• It has a very short half-life between 16-24 minutes.
36
37

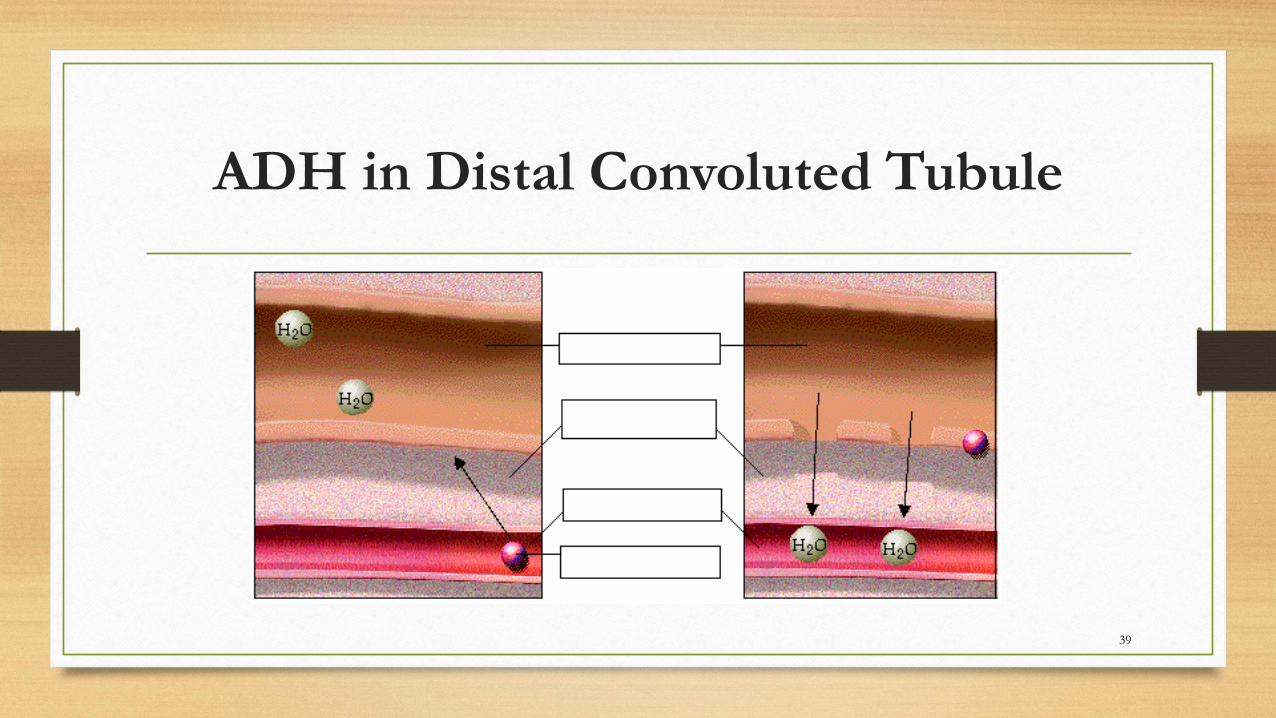
ADH in Distal Convoluted Tubule
• ADH promotes the reabsorption of water from the kidney by stimulating an
increase in the number of water channels in the distal convoluted tubules
and collecting tubules (ducts).
• These channels aid in the movement of water back into the capillaries,
decreasing the osmolarity of the blood volume and therefore blood pressure.
38
ADH in Distal Convoluted Tubule
39

A short-term effect of increased osmolarity
• A short-term effect of increased osmolarity is the excitation of
the thirst center in the hypothalamus.
• The thirst center stimulates the individual to drink more water and
thus rehydrate the blood and extracellular fluid, restoring blood
volume and therefore blood pressure.
40

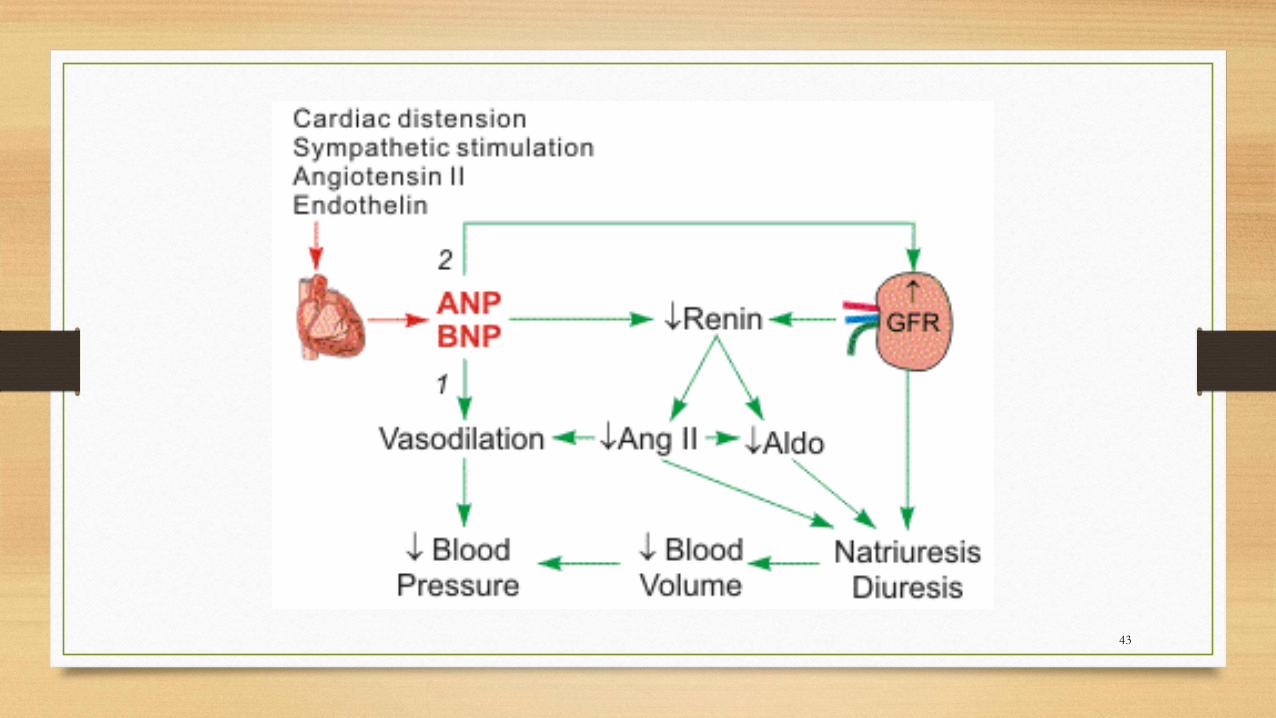
Atrial Natriuretic Peptide (ANP)
• ANP is a 28-amino acid peptide that is synthesized, stored, and released by
atrial myocytes in response to atrial distension, angiotensin II stimulation,
endothelin, and sympathetic stimulation (beta-adrenoceptor mediated).
• Elevated levels of ANP are found during hyper-volemic states, which occurs
in congestive heart failure.
• ANP is first synthesized and stored in cardiac myocytes as pre-pro-ANP,
which is then cleaved to pro-ANP and finally to ANP.
• ANP is the biologically active peptide 41
Atrial Natriuretic Peptide (ANP)
This hormone is stored and secreted by muscle of Atrium and to some extent ventricle and its secretion is stimulated by ECF volume and ingestion of Na+
Dilating afferent arteriole and relaxing mesangial cells
Inhibiting Na+ reabsorption in renal tubule
Relaxing the VSM of arteriole and venule
42
43
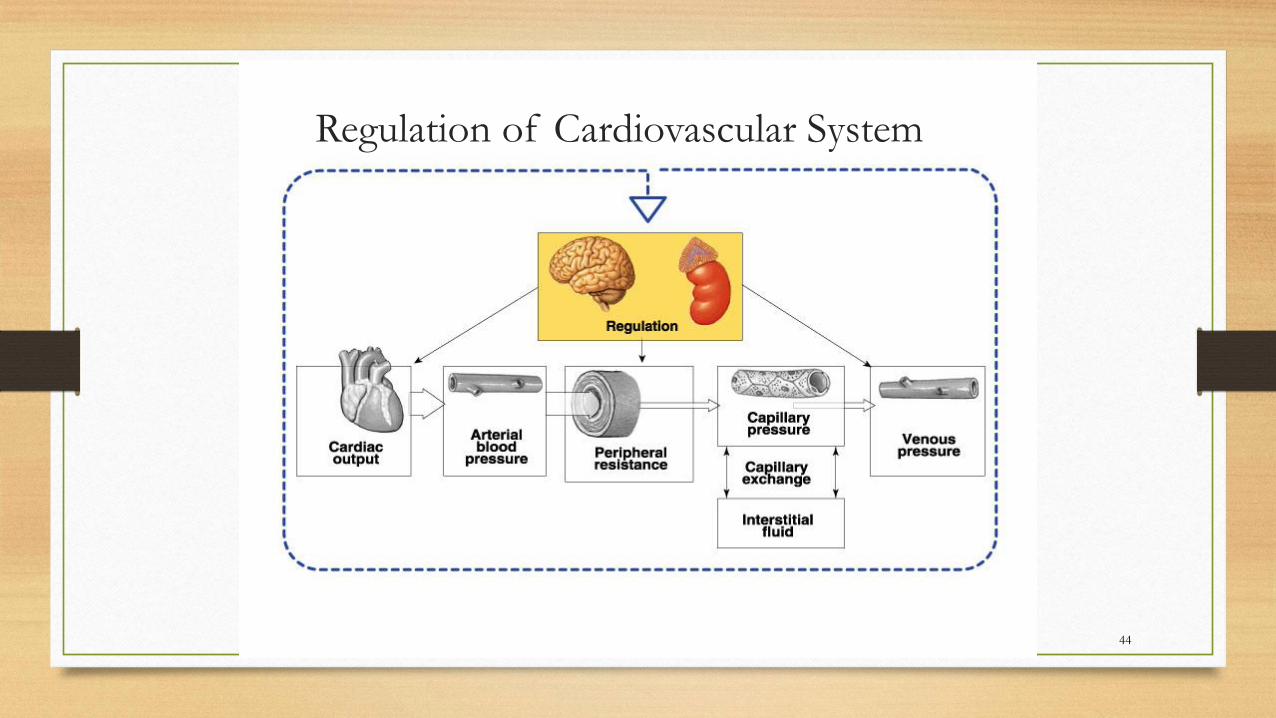
Regulation of Cardiovascular System
44
Summary
1. In the short-term, rising blood pressure stimulates increased parasympathetic activity, which leads to reduced heart rate, vasodilation and lower blood pressure.
2. Falling blood pressure stimulates increased sympathetic activity, which leads to increased heart rate, contractility, vasoconstriction, and blood pressure.
3. Long-term blood pressure regulation involves renal regulation of blood volume via the renin-angiotensin mechanism and aldosterone mechanism.
4. Increased blood osmolarity stimulates release of antidiuretic hormone (ADH), which promotes reabsorption of water, and excites the thirst center, resulting in increased blood volume and blood pressure.
45

Summary
46