Embed Size (px)
Citation preview
VIGNAN INSTITUTE OF PHARMACEUTICAL TECHNOLOGY
Pharm-dPharmacotherapeuticsCase presentation on epigastric herniaM.SAI NAVYA15AC1T0015

Epigastric Hernia
• It occurs in the middle of the body between the breast bone & the belly button or naval.

Epigastric hernia
Causes• Lesser strength of connective tissue of
stomach(due to heavy lifting,etc.)• Obesity• Pregnancy• Accumulation of fluid in the stomach cavity.• Sometimes persistent coughing can cause
epigastric hernia.
Signs & Symptoms
Abdominal bulge
Pain Nausea

Pathophysiology

Complication• A lot of complications may pop up if the epigastric hernia is not
treated properly or on time. There may be loops of bowel when the weakness in the muscle wall enlarges. Due to this a blockage may cause which will result in vomiting and stomach ache.
• Strangulation is one serious complication observed in epigastric hernia.

Diagnosis• Physical examination: Epigastric hernia is often small or barely visible.• To take an internal look at the abdominal
wall between the breast bone & naval: 1) USG 2) CT Scan
TreatmentPharmacological• Antibiotics : Cefoxitin Gentamicin Ampicillin• Antianxiety Agents : These agents are indicated for
patients who may experience significant anxiety before a surgery – Lorazepam
Midazolam• NSAIDs : Diclofenac Ibuprofen Naproxen

Non pharmacological : • Surgery – Epigastric hernia repair Procedure: Anesthesia is given (general) Surgery begins with an incision on either side of the hernia A laproscope is inserted into one incision, the other incision
is used for additional surgical instruments The surgeon then isolates the portion of the abdominal lining
that is pushing through the muscle. This tissue is called hernia sac. The surgeon returns the
hernia sac to its proper position , then begins to repair the muscle defect.
If the defect in the muscle is small , it may be sutured closed. For large defects , a mesh graft will be used to cover the
hole. Once the mesh is in place or the muscle has been sewn , the
laproscope is removed & the incision can be closed It is closed with sutures .
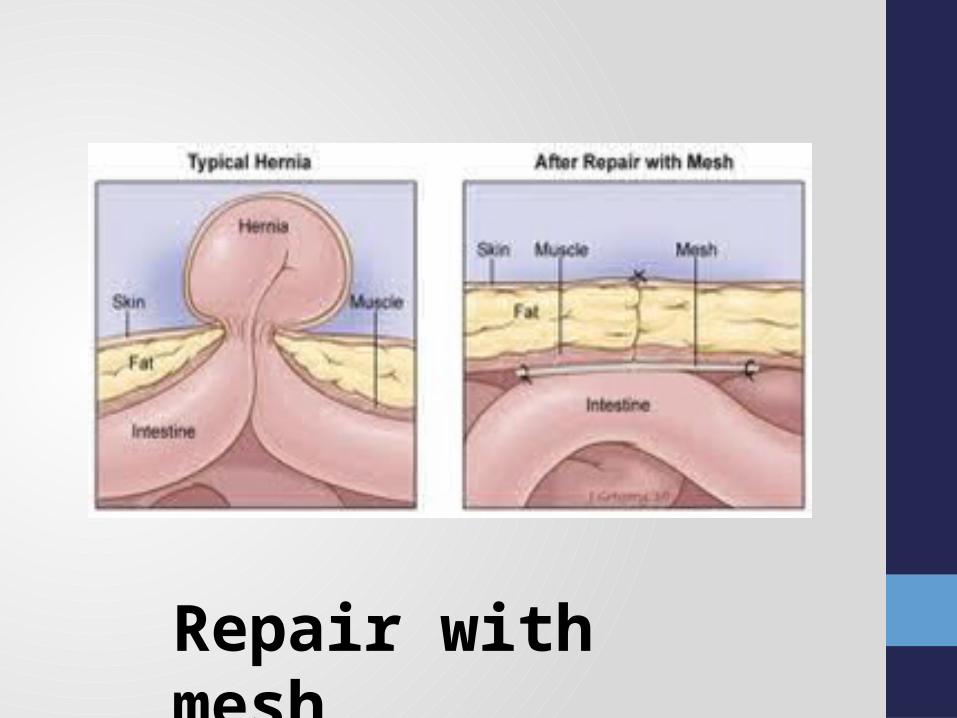
Repair with mesh

Soap note on epigastric pain

SUBJECTIVE FINDINGS• A male patient of age 66 years admitted in the
hospital with the complaints of pain & swelling over epigastric region since 15 years.• He has H/O hypertension since 2 years.• His past medication history include intake of
analgesics , but the medications are not available. • He consumes caffeine.• He has neither surgical nor family history.• He has no drug allergies.

OBJECTIVE FINDINGSPhysical examination• All the vitals were tested for 6 days.• His temperature was high on 1st & 6th day.• His blood pressure was abnormal (high).• His was pulse rate was high.• His respiratory rate was high.
Objective findings• Hemoglobin was decreased.• Lymphocytes were increased slightly.• Monocytes were decreased slightly.• ESR was increased
Specialized diagnostic tests• USG: 7.8cm defect noted in the parietal layer of anterior abdominal wall in
epigastric region with herniation of bowel & omentum Impression: epigastric hernia.

ASSESSMENT• Based on patient’s complaints (pain
&swelling over epigastric region)& USG(epigastric hernia), the patient is confirmed with epigastric hernia.• Chronic use of NSAIDs (analgesics) lead
to ulcers.
PLAN Non pharmacological:Surgery – lap hernia repair prolene mash

PHARMACOLOGICALDrug Composition Dose Route Frequency DaysTab CYRA-D Domperidone
Rabeprazole1 tab P/O OD 5
Tab Telmisartan
Telmisartan 40mg P/O OD 5
Inj NOSOCEF Ceftriaxone 1gm P/O BD 2
Inj TRAMADOL
Tramadol 1 amp IV BD 2
Inj PANTOP Pantoprazole 40mg IV OD 2
Tab DOLO Paracetamol 650mg P/O SOS -
Inj FEBRINIL Paracetamol 1amp IV SOS -
Inj VOVERAN Diclofenac 1 amp IM SOS -
10RL Ringer lactate solution
1 pint IV SOS -
Pre operation
Post operation
SOS Medication

Drug / Composition
Indication Contraindication Monitoring parameters
ADRs
CYRA –D / Domperidone, Rabeprazole
Acidity Concomitant use with rilpivirine & alazanavir
Monitor Mg levels prior to initiation
Diarrhoea, headache, pruritus, dizziness
TELMIKIND/ Telmisartan
HTN Severe hepatic impairment
Monitor BP , serum creatinine levels , electrolytes
Dizziness, fatigue , headache , sinusitis
NOSOCEF / Ceftriaxone
Susceptible Bacterial infection
Hypersensitivity to ceftriaxone or other cephalosporin
Perform CBC at regular intervals during prolonged treatment. Observe for signs &symptoms of anaphylaxis
Diarrhoea, nausea, vomiting.
TRAMADOL / Tramadol
Post operative pain
Suicidal patients , acute intoxification of hypnotics
Monitor pain relief , resp. rate , BP , pulse rate , abuse
Resp. depression, seizure , dizziness , headache.

Drug / Composition
Indication Contraindication Monitoring parameters
ADRs
PANTOP / Pantoprazole
Ulcers Concomitant use with rilpivirine , atazanavir
Monitor Mg levels prior to initiation
Diarrhoea, headache, pruritus, dizziness
DOLO/ Paracetamol
Pain reliever/ fever reducer
Not to be used if allergic to acetaminophen or paracetamol
Monitor serum paracetamol levels when acute over dosage is expected
Nausea, loss of appetite
FEBRINIL/ Paracetamol
Pain reliever/ fever reducer
Not to be used if allergic acetaminophen or paracetamol
Monitor serum paracetamol levels when acute over dosage is expected
Nausea , loss of appetite
VOVERAN / Diclofenac
Post operative pain
Hypersensitivity , asthma , urticaria
Periodically monitor serum transaminase values , CBC , BP
Edema , CHF, HTN, Tachycardia, nausea , diarrhoea
RINGERS LACTATE SOLUTION
Replacement of fluid & electrolytes
- Monitor fluid balance , electrolytes , acid base balance
Allergic reactions

DRUG INTERACTIONS• They are no major or moderate drug interactions.
MINOR INTERACTION: Ceftriaxone × Diclofenac
FOOD DRUG INTERACTIONS:
Interaction Mechanism Management Tramadol × Alcohol
Result in additive CNS depression
Avoid taking alcohol
Telmisartan × food
Moderate to high dietary intake of K+, especially salt substitutes may increase the risk of hyperkalemia
Avoid eating potassium containing salt substitutes
PHARMACIST INTERVENTIONDOSE ADJUSTMENT : No dose adjustment is requiredPATIENT COUNSELLING : • Do not drive or operate machinery.• Avoid drinking alcohol , soft drinks & grape fruit juice.• Do not crush or chew the tablets.• Take PANTOP immediately before a meal.AFTER DISCHARGE:• Rest for few days. • Have a pillow handy to over abdomen for support.• Do not lift heavy objects.

MY TREATMENTPRE SURGERY
Drug Dose Frequency RoutePANTOPRAZOLE 40 mg OD P/O
TELMISARTAN 40 mg OD P/O
POST SURGERYDrug Dose Frequency Route
AMPICILLIN 500 mg BD P/O
PARACETAMOL 650 mg SOS P/O
RL 1 Pint SOS IV
PANTOPRAZOLE 40mg OD P/O

REFERENCES• http://www.webmd.com/digestive-disorders/tc/common-types-
of-hernias-epigastric-hernia• https://www.verywell.com/epigastric-hernia-diagnosis-
treatment-and-surgery-3157222• https://www.epainassist.com/abdominal-pain/what-is-
epigastric-hernia• http://emedicine.medscape.com/article/189563-medication#6• https://image.slidesharecdn.com• http://californiahernia.com/wp-content/uploads/2015/09/
hernia-illustration.jpg• http://www.mims.com/india






























