Embed Size (px)
Citation preview

Chapter 7
Neurocognitive disorders

Chapter outline
• Introduction• The classification of Neurocognitive
disorders• History of Neurocognitive disorders• Delirium• Neurocognitive Disorders (Dementia)• Amnestic disorders (ICD-10)• Assessment of neurocognitive disorders• Contextual and cross-cultural perspectives

Introduction• Cognition refers to tasks that include:
• memory • language• orientation • judgment• problem-solving • planning • ability to have interpersonal relationships • praxis (perform actions)
• Cognitive disorder is when regular trouble in these areas disrupts daily functioning.
• Causes of cognitive disorders include head injury, medical conditions, substance abuse, and aging.

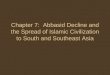
Temporal Lobe
Occipital lobe
Frontal Lobe Parietal lobe
Motor cortex Sensory Cortex

Thalamus
Amygdala
Hippocampus
Pons
Hypothalamus
MedullaCerebellum
Spinal cord

Introduction, cont.

Classification of Neurocognitive disorders
• Three groups: • Delirium, • Major or Minor Neurocognitive Disorders
(Dementia) • Amnestic disorders.
• Within Major or Minor Neurocognitive Disorders: e.g. Alzheimer’s disease, Vascular dementia, Multi-infarct dementia, Frontotemporal, Creutzfeldt-Jacob disease (mad cow disease), Huntington’s disease, Parkinson’s disease, Human Immunodeficiency Virus (HIV) disease, etc.

History of Neurocognitive disorders
• No longer referred to as organic because name implies that non-organic disorders or functional mental disorders (e.g. depression) have no biological basis.
• ICD-10 still uses the term ‘organic’.

DeliriumClinical picture• Temporary state of mental confusion, with
fluctuating consciousness.• Occurs suddenly and is reversible.• Abnormal mental state, not a disease, often
accompanied by anxiety, disorientation and incoherent speech.
• Main feature - impairment in consciousness.• Consciousness ranges from fully alert to comatose.

Delirium, cont.Epidemiology• General population:
• 18-55 yrs: 0.4%• 55 yrs +: 1.1%
• Medical inpatients:• 10%-13% (increasing in the elderly)
• Delirium incidence for new admissions: 3%-29%• Occurrence rate per admission: 11%-42%

Delirium, cont.Aetiology

Delirium, cont.Classified according to aetiology• Delirium due to general medical condition• Delirium due to misuse/abuse of substances -
Intoxication Delirium/Substance Withdrawal Delirium
• Delirium due to several causes - Delirium Due to Multiple Aetiologies
• When aetiology is unknown - diagnosed as Delirium Not Otherwise Specified

Delirium, cont.Treatment and management• If associated with underlying physical cause:
• recovery can be expected • provided physical cause treated correctly
• Recovery can occur in a few hours to days.• Co-occurring dementia and old age contribute to
longer recovery time.• Better recovery if:
• underlying aetiology addressed• premorbid functioning good• no previous diagnosis of delirium

Delirium, cont.• Most individuals make full recovery.• Delirium may progress to stupor, coma, seizures, or
death, especially if underlying aetiology not addressed.
• Environmental interventions:• limit environmental factors that exacerbate
delirium • give cognitive and emotional support to re-
orient and reassure patients• Doctors may also prescribe drugs to control
agitation.

Major or Minor Neurocognitive Disorders (NCD)
• The DSM-IV-TR referred to these disorders as Dementia, and ICD-10 still uses this description.
• Although the DSM-5 now refers to these disorders as Neurocognitive Disorders (NCD), the term dementia is still retained to certain extent (APA, 2013).
• The APA (2013) states that the term dementia is a customary description of degenerative disorders for older adults, however, the term neurocognitive disorders is more inclusive as it includes neurocognitive disorders that affect younger people as well (APA, 2013).
• The APA (2013) views these disorders as unique when compared to the other DSM-5 categories as the underlying pathology and aetiology can be easily determined.
• The primary diagnosis would be Major or Mild NCD, followed by an aetiological subtypes (e.g. Alzheimer’s disease, Parkinson’s disease, HIV infection, etc.)

Major or Minor Neurocognitive Disorders
To understand the clinical picture of these disorders, it is necessary to note which neurocognitive domains are affected. The DSM-5 describes these as follows (APA, 2013):• Complex attention: Sustained, divided and selective attention as
well as processing speed.• Executive functioning: Planning, decision making, working
memory error detection and correction, inhibition and mental flexibility.
• Learning and memory: All memory registers (e.g. short-term, semantic, autobiographical) and implicit learning.
• Language: Expressive and receptive language.• Perceptual-motor: This includes visual perception, visuo-
constructional abilities, perceptual-motor, praxis and gnosis.• Social cognition: Recognition of emotions and theory of mind.

NCDClinical picture• Gradual loss of mental abilities resulting in an
inability to complete simple, everyday activities.• May also lose ability to solve problems, control
emotions and undergo personality change.• Other symptoms: Hallucinations, agitation, and
memory loss.• Dementia can be caused by various diseases.• Common in the elderly - not to be confused with
normal decline in cognitive functioning occurring with age.
• Memory impairment a core symptom.• Person unable to learn new things and forgets
things.

NCD, cont.• Deterioration of language function: Aphasia and
echolalia.• Deterioration of ability to recognise familiar objects
and people.• Problems with executive functioning associated
with the frontal lobe.• Spatially disorientated; poor judgement and insight.• May not be aware of memory loss and cognitive
deterioration and may do irrational things.• Demonstrate inappropriate behaviour or become
violent towards others.• Depression and suicide common.• Physical injuries resulting from motor disturbances.

NCD, cont.Epidemiology, cont. • Prevalence of dementia in Africa lower than rest
of the world.• Possible reasons for lower rates include:
• differential survival rates• relatives hiding symptoms due to stigma• reluctance to seek medical assistance• poor access to medical care• feeling old person come to end of useful life• defective case finding techniques
• Incomplete statistics of prevalence in developing societies, but estimate is 6.8%.
• Prevalence of different causes of dementia varies across cultural groups.

NCD, cont.Aetiology• Dementias are sub-categorised according to
presumed aetiology, and include:• Dementia of the Alzheimer’s Type• Vascular Dementia• Dementia Due to Other General Medical
Conditions• Substance-Induced Persisting Dementia• Dementia Due to Multiple Aetiologies• Dementia Not Otherwise Specified

NCD, cont.Alzheimer’s Type• Most common - 50% of all cases.• Major risk factors are:
• family history• genetic factors• head injury
• Onset of Alzheimer’s is subtle - initial memory impairment and gradual deterioration of cognitive abilities.
• Pathology is associated with parietal and temporal regions of the brain.

NCD, cont.Vascular • Cerebrovascular disease is second most common
cause of dementia.• Injury or brain disease infarctions (death/damage of
vessels) due to obstruction in blood supply lesions and changes to brain structures.
• Abrupt onset and fluctuating course. • Risk factors: Hypertension, diabetes, advanced age,
stroke, alcoholism, cardiovascular risk factors (smoking, obesity).
• Disorder more common in men.• Compared to Alzheimer’s Type, more likely to have
depression, affective changes, disturbance of gait, and confusion.

NCD, cont.
Parkinson’s disease• Disorder which affects muscle movement,
resulting from loss of dopamine-producing brain cells.

NCD, cont.
Huntington’s disease• Genetically influenced degeneration of brain cells. • Chance of inheritance is 50-50, with inheritance predicting certain onset. • Dementia associated with the disease characterised by more motor than language abnormalities. Figure 7.2: MRI image – demonstrates
bilateral atrophy of the head of the caudate nuclei and compensatory ventricular dilatation of the frontal horns bilaterally suggestive of Huntington’s disease

NCD, cont.Picks Disease
Frontotemporal• Shrinking of the frontal and temporal regions. • Most common in men with first-degree relatives.• Leads to prominent personality and behavioural changes.
Figure 7.3: CT scan of Pick’s disease

NCD, cont.
Lewy body disease• Round deposits in the cerebral cortex which
contain damaged nerve cells. • Similar to Alzheimer’s but more rapid.

NCD, cont.
Creutzfeldt-Jakob disease• More commonly known as ‘mad cow disease’.• Rare disease affecting muscle control, personality
and memory.• As the illness worsens blindness, involuntary
movements, weakness and, eventually, coma.
✪ See slide show at:http://reference.medscape.com/features/slideshow/
cjd#

NCD, cont.
Human Immunodeficiency Virus (HIV) disease• Characterised by:
• forgetfulness• slowness• poor concentration• difficulties with problem solving• apathy• social withdrawal
Figure 7.5: HIV particles adhering to a CD4 lymphocyte

NCD, cont.
Head trauma• Extremely high prevalence in South Africa due to
high incidence of motor vehicle accidents and violence (see Table 7.5).
• Head injury-related dementia is characterised by emotional lability, dysarthria (speech impairment) and impulsivity.

NCD, cont.

NCD, cont.
Substance-Induced Persisting NCD resulting from:
• abuse of drugs or medication• toxic exposure

NCD, cont.Treatment and management of NCD• Condition is often not reversible.• But, important to know the underlying cause
in order to try to reverse or arrest the process.• Preventative measures, especially in vascular
dementia, can be implemented.• Those suffering from changes in cognitive function
can benefit from supportive and educational psychotherapy.

Amnestic disorders (ICD-10)Clinical picture• Memory impairment in the absence of other
cognitive impairments.• Characterised by:
• inability to learn new information (anterograde amnesia) or
• inability to recall knowledge stored from before onset of disorder (retrograde amnesia)
• Short-term and recent memory are affected. • Onset can be sudden or gradual.

Amnestic disorders, cont.Classified according to aetiology • Amnestic Disorder Due to a General Medical
Condition • Substance-Induced Persisting Amnestic Disorder• Amnestic Disorder Not Otherwise Specified
Epidemiology• No adequate studies on incidence and
prevalence of amnestic disorders.• Probably quite high in SA due to high incidence
of motor vehicle accidents and violence.

Amnestic disorders, cont.
Aetiology• Main brain areas implicated in amnestic disorders:
• temporal lobes• midline nuclei of the thalamus• Hippocampus• mamillary bodies• amygdala (left more implicated than right).
• Frontal lobe symptoms include confabulation and apathy.

Amnestic disorders, cont.Aetiology, cont.• Possible causes of amnestic disorders:
• systemic conditions (such as thiamine or Vitamin B1 deficiency) (e.g. Korsakoff’s syndrome)
• hypoglycaemia (low blood sugar)• brain-related conditions like hypoxia (low oxygen)• seizures and epilepsies • surgical procedures to the brain/head injury • infections (e.g. herpes simplex encephalitis) • tumours • cerebro-vascular diseases • substance-related conditions (e.g. alcohol,
neurotoxins, sedatives, and over-the-counter-drugs)• multiple sclerosis

Amnestic disorders, cont.Treatment and management • Primary approach = treat underlying cause:
• If underlying cause is primary, systemic or cerebral, can use thiamine, antiretroviral medication, or aspirin.
• Despite variety of pharmaco-therapeutic trials, no drug treatments have proved effective in amnestic disorders.
• Rehabilitation for mild cases of amnesia involves memory techniques and tools.
• Emotional and social support for difficulties in occupational and social functioning.
• Many people gradually recover; psychotherapy, counselling help individual adjust to illness and recovery.

Assessment of Neurocognitive disorders
• Review of clinical notes • Interview• Observation • Screening tests:
• Mini Mental Status Examination (MMSE) to evaluate cognitive function
• Glasgow Coma Scale (GCS) to quantify the level of consciousness
• Clock Drawing Test (CDT) to assess cognitive functioning in psychiatric and neurological settings
• Dementia scales include:• HIV Dementia Scale (HDS)• Deterioration Cognitive Observee (DECO)• Clinical Dementia Scale (CDS)

Assessment of Neurocognitive disorders, cont.
• Scales are filled out by a health practitioner or caregiver.
• Both the HDS and DECO scales correlate positively with the MMSE.
• More sophisticated neuropsychological tests may be administered after screening.
• Other assessments include:• X-rays• MRI (Magnetic Resonance Imaging)• fMRI (Functional Magnetic Resonance Imaging)• PET (Positron Emission Tomography)

Contextual & cross-cultural perspectives
• Individual or group beliefs influence health behaviour.
• Beliefs also influence how health-care facilities are used.
• Important to be aware of cultural and language differences - can influence diagnosis of cognitive disorders.
• In SA, evaluation and understanding influenced by:• past inequalities in education• lack of facilities and resources

Contextual & cross-cultural perspectives, cont.
• Some cognitive symptoms accounted for by different indigenous world views:• Ukuthwasa = calling to be a traditional healer
(role = to help in caring/healing process of the whole person)
• Ukufa kwabantu = ‘illnesses of the people’; not recognised by the patient as an illness/disease but as disturbance caused by breaking a taboo or displeasing an ancestor or due to a spell that has been cast on the patient:• Indiki, ufufunyane or izizwe (spirit possession) • Umnyama (pollution or contamination) • Ubuthakathi (bewitchment or sorcery)• Ukuphonsa (curses or spells) • Umkhondo; umeqo; idliso (some form of poisoning)

Contextual & cross-cultural perspectives, cont.
• All cultures and religions have traditional explanations for abnormal behaviour.
• Western society relies on technological medicine; 80%-90% from developing societies rely on traditional healing.
• Being unaware of patient’s cultural background misdiagnoses and distress for the patient.
• Most neuropsychological and psychological assessments developed in Western context may be invalid when used in developing countries.
• Also, individuals from other cultures may not be familiar with general knowledge used in tests.

Conclusion• Prevalence of cognitive disorders increasing due
to greater longevity (better health, improved diet and living conditions, etc.).
• Three categories: Delirium; dementia; amnestic disorders.
• For each, aetiology influences onset, course, treatment, and outcome of disorder.
• Diagnosis is complex and difficult because of:• symptom overlap with medical conditions• beliefs• cultural and contextual factors