Embed Size (px)
Citation preview

+
How To Approach MTC
Sara Al-Ghanem

+Objectives
Introduction
Pathology
Classification & clinical pic.
Approach to MTC
2

+ History ( from the patient )
33 y\o female pt ,G7P4+2
Medically free
No s\p
No hx of allergy
She was will till 1 year ago , when she started to suffer from neck pain in the
RT side .
While she was eating her daughter accidently noted that she has a neck
swelling on rt side .
The swelling increased in size with time
There was no skin changes or discharge coming from it
No other swelling in the body
3

+
She has symptoms suggesting hypothyroidism in the form of :
cold intolerance, wt gain & malaise
also she is having compressive symptoms , like dysphagia
,hoarseness
No hx of aspiration or respiratory distress
No hx of neck radiation in childhood
FHx: her aunt has a thyroid problem ? She did know the dx &
no surgery was done for her
4

+Hospital course
Initially she was dx with lymphadenitis in PHC & received a
course of Ab . But she did not improve.
U\S was arranged & upon the finding , they FNA was requested
FNA showed hashimoto thyroididtis
after that she was referred to GS , & they did excisional LN
biopsy for her .
Finally we received the pt in ENT clinic as a case of met
medullary Ca in RT cervical LN
5

+ENT Plan
The patient was admitted in the hospital on Tuesday under care
of Dr.Al-Saab for further evaluation & multidisciplinary
assessment with other teams before surgery
6

+On EX
By inspection of the neck:
1- there is goiter more prominent in RT side
2- scar in RT side of neck measuring about 3 cm ( in level II)
By palpation :
There swelling is located in center of the neck
moving with deglutition
More prominent in RT side ( 3*2.5 cm ) , left side ( 2*2)
Firm, not fixed to underlying skin
With no substernal extension
Bil cerviacl lymphadenopathy ( level II)
7

+Labs
Calcitonin
Calcium
Metanephrine ?
8

+Imaging
CT of chest & neck ?
It was done yesterday but we are waiting the report
9

+Surgery Plan ?
That what I am looking for
10

+Introduction
Medullary thyroid cancer (MTC) is a neuroendocrine tumor of the parafollicular
or C cells of the thyroid gland
11
+Gross pathology
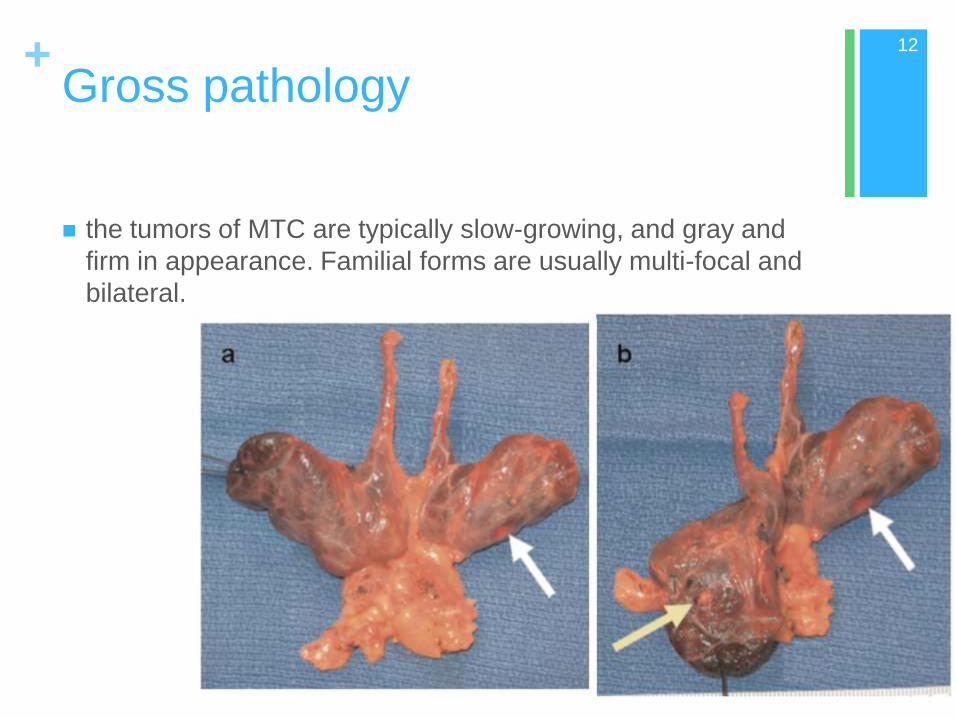
the tumors of MTC are typically slow-growing, and gray and
firm in appearance. Familial forms are usually multi-focal and
bilateral.
12

+Microscopic features ( histology )
Histologically, MTC is characterized by uniform polygonal cells with central nuclei and finely granular eosinophilic cytoplasm.
The finding of stromal amyloid is a distinguishing feature of MTC, but is present in only one-third of cases.
C-cell hyperplasia is a precursor to malignant transformation, and is most commonly seen in familial MTC
The presence of amyloid is a diagnostic finding, but immunohistochemistry for calcitonin is more commonly used as a diagnostic tumor marker.
These tumors also stain positively for CEA and calcitonin gene–related peptide.
13

+PATTERNS OF METASTASES
14

+
MTC frequently metastasizes to regional lymph nodes, and
these metastases are often apparent at the time of diagnosis.
The frequency has been reported to be over 50% in patients
who present with palpable, established primary tumors. Spread
is most frequent to the central compartment (Level VI), followed
by the ipsilateral jugular chain of nodes (Levels II through V)
and the contralateral cervical nodes.
Spread is also seen to the upper and anterior mediastinum
Hematogenous spread may occur to the lungs, liver, bones,
brain, and soft tissues .
15

+
Medullary thyroid carcinoma
(MTC) comprises 5– 10% of all
thyroid cancers.
16

+MTC is a sporadic malignancy in the
majority of cases (75%), with the
remainder comprising three familial
syndromes: MEN 2A, MEN 2B, and
familial non-MEN MTC (FMTC).
MEN 2A, the most common syndrome
(up to 80% of hereditary cases)
17

+Sporadic MTC
Sporadic MTC accounts for about 80 %
The typical age of presentation is in the fifth or sixth decade .
there may be a slight female preponderance
The most common presentation of sporadic MTC is that of a
solitary thyroid nodule
In most patients, the disease has already metastasized at the
time of diagnosis.
50%of patients have clinically detectable CLN involvement
15% have symptoms of upper aerodigestive tract compression.
5% have distant metastatic
18

+Sporadic MTC
19
Systemic symptoms may occur due to hormonal secretion
by the tumor.
Tumor secretion of calcitonin, calcitonin-gene related
peptide, or other substances can cause :
diarrhea
or facial flushing in patients with advanced disease.
In addition, occasional tumors secrete corticotropin (ACTH),
causing ectopic Cushing's syndrome.

+Inherited MTC
MEN2 is subclassified into three distinct syndromes, each
of which is transmitted in an autosomal dominant fashion
and is associated with MTC:
MEN2A
MEN2B
and familial medullary thyroid cancer (FMTC).
These syndromes result from different mutations in the
RET proto-oncogene.
20

+
MEN2A
the most common syndrome (up to 80% of hereditary cases).
M = multi-focal, bilateral MTC 100% penetrance
P = pheochromocytoma 42% penetrance
H = hyperpar- athyroidism 10 – 30% penetrance
Less commonly, this syndrome includes a skin condition,
lichen planus amyloidosis, and/or Hirschsprung disease.
2 MPH or 2 Miles Per Hour
21

+MEN 2B
MTC (also with 100% penetrance),
Marfanoid habitus.
Mucosal neuromas,ganglioneuromatosis of the gastrointestinal tract, and
megacolon. ( variable presence )
Pheochromocytoma (40% penetrance)
MMMP (Think: 3M Plastics)
22

+
23

+
FMTC is characterized by development
of MTC alone .
24

+the clinical presentation and
manifestations of MEN2-associated
MTC are similar to those of sporadic
MTC.
The most common presentation is that
of a solitary thyroid nodule or cervical
lymphadenopathy.
25

+Hx & PE
FNA biopsy
aided by immunocyto- chemical staining
for calcitonin.
genetic testing for
a hereditary syndrome.
Serum calcitonin and CEA
Radiologic evaluation
Testing for coexisting
tumors
STAGING
26
+
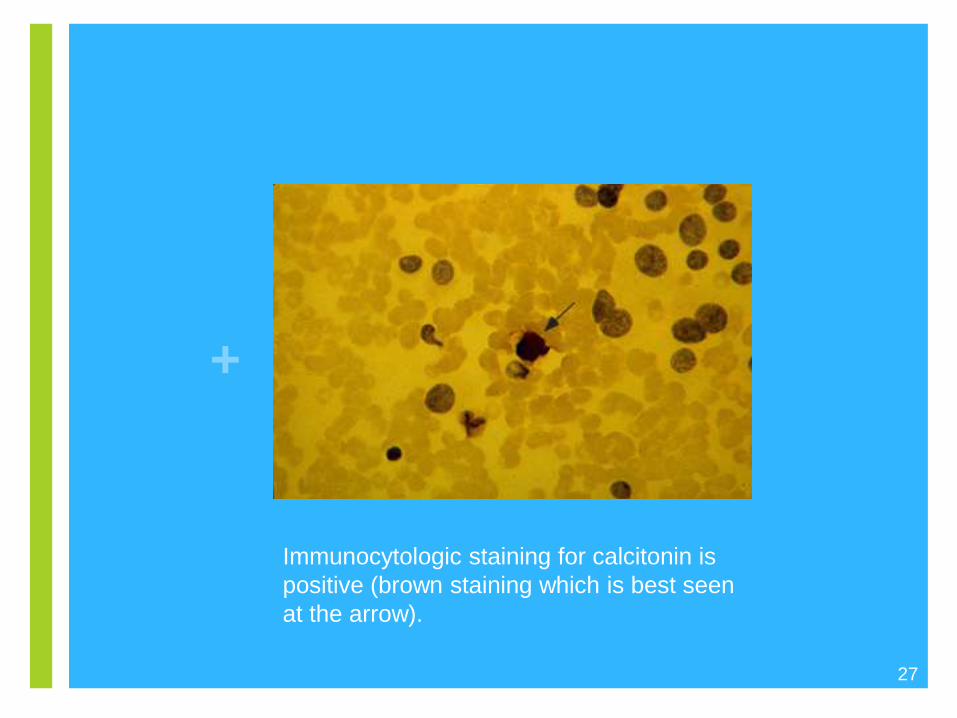
Immunocytologic staining for calcitonin is
positive (brown staining which is best seen
at the arrow).
27
+
28
ultrasonography of the neck is indicated to look for cervical lymph node
involvement.
For patients with local lymph node metastases on ultrasound or with
preoperative serum basal calcitonin >400 pg/mL :
indicating high risk of local or distant metastatic disease
additional imaging is required to assess for metastatic disease:
chest CT, neck CT, three-phase contrast-enhanced liver CT or contrast-
enhanced liver MRI
Radiologic evaluation

+genetic testing for a hereditary syndrome
29
All patients presenting with clinically evident MTC should have
genetic testing to evaluate for a hereditary syndrome.
Approximately 6–10% of patients who present with MTC with no
family history will be found to have a germline RET mutation.
In patients at-risk for familial MTC, the availability and accuracy of
genetic screening for RET mutations has replaced yearly screening
calcitonin measurement as the primary diagnostic tool
because identification of a mutation allows diagnosis and treatment prior
to the C-cell proliferation (either through hyperplasia or cancer) necessary
to elevate calcitonin levels

+genetic testing for a hereditary syndrome
In patients at-risk for MEN 2B, genetic testing should be done
immediately after birth, because MTC is usually already established
by that time and early thyroidectomy is necessary to increase
chance for cure.
In patients at-risk for FMTC or MEN 2A, genetic screening may be
done in early childhood (before age 5 or 6), to allow planning for
preventative thyroidectomy.
30

+
31
Stage I —
MTCs that are less than 2 cm in diameter
without evidence of disease outside of the thyroid
gland
Stage II —
Any tumor between 2 and 4 cm
without evidence of extrathyroidal disease
Stage III —
Any tumor greater than 4 cm,
or level VI nodal metastases
or microscopic extrathyroidal invasion regardless of
tumor size
Stage IV —
Any distant metastases,
or lymph node involvement outside of level VI,
or gross soft tissue extension

+SURGICAL STRATEGY FOR MTC
the operative procedure recommended is a total thyroidectomy with a
central compartment lymphadenectomy
and parathyroid auto- transplantation,
and ipsilateral functional neck dissection (Levels II – V)
Bilateral neck dissections may be considered.
Radioactive iodine, external beam radiation therapy (EBRT), and
conventional chemotherapy have not been effective.
32

+
Points to Remember 33

+
34
A characteristic feature of this tumor is the production of calcitonin.
Most cases are sporadic
Medullary thyroid cancer (MTC) is a neuroendocrine tumor of the
parafollicular or C cells of the thyroid gland
For patients diagnosed with MTC on the basis of cytologic evaluation of a
thyroid nodule, evaluation should include measurement of serum
calcitonin, carcinoembryonic antigen , U\S of the neck, genetic testing for
germline RET mutations, and biochemical evaluation for coexisting
tumors, especially pheochromocytoma
Genetic analysis, along with imaging and calcitonin testing aid in
optimizing surgical resection in these cases.

+References
Current approaches to medullary thyroid
carcinoma, sporadic and familial.
35

+
36


![Thyroid Cancer and Thyroid Nodules.ppt [Read-Only] · Thyroid CaThyroid Ca 20012001. Newer Exceptions Unfortunately recent Studies have shown exceptions: *** *** In one study of papillary](https://img.dokumen.tips/doc/110x75/5d4794b388c9931b4f8b7654/thyroid-cancer-and-thyroid-read-only-thyroid-cathyroid-ca-20012001-newer.jpg)