Embed Size (px)
Citation preview
Approach to child with abnormal movement
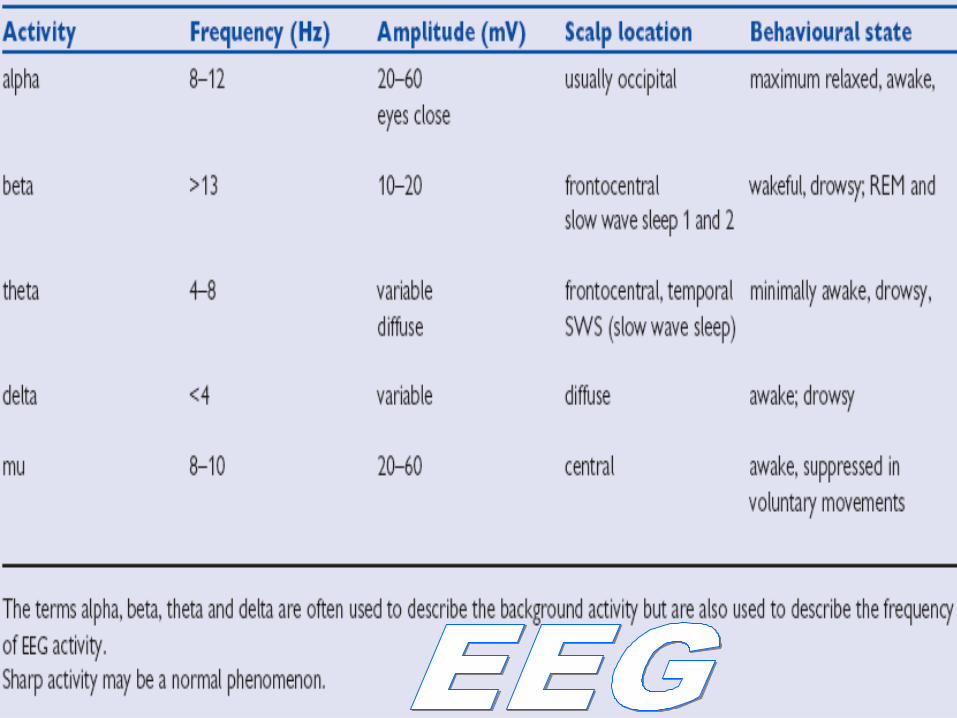
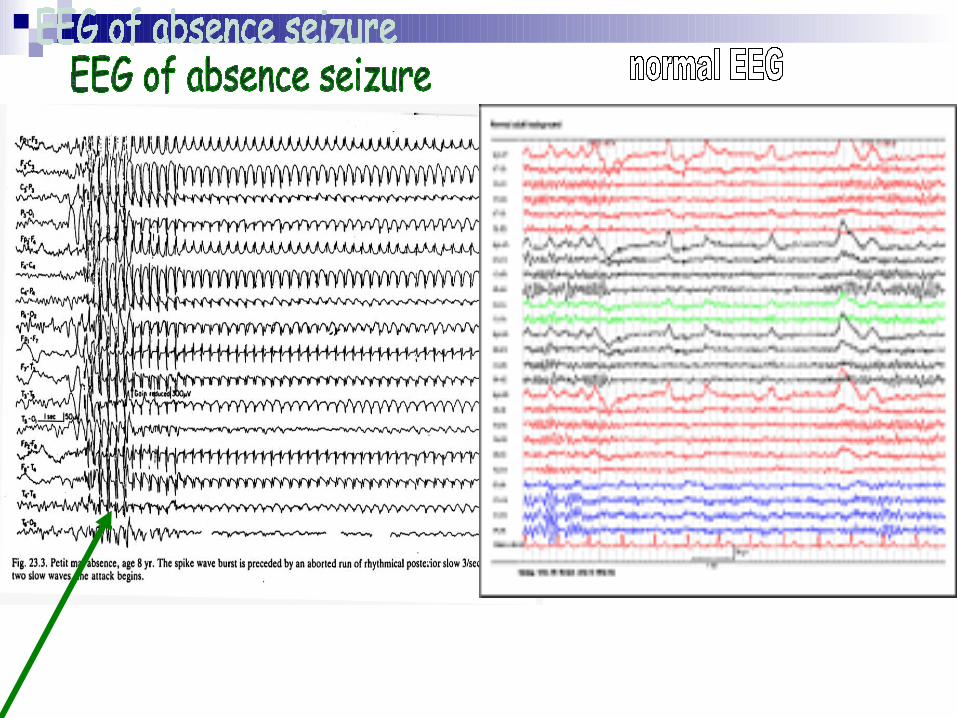
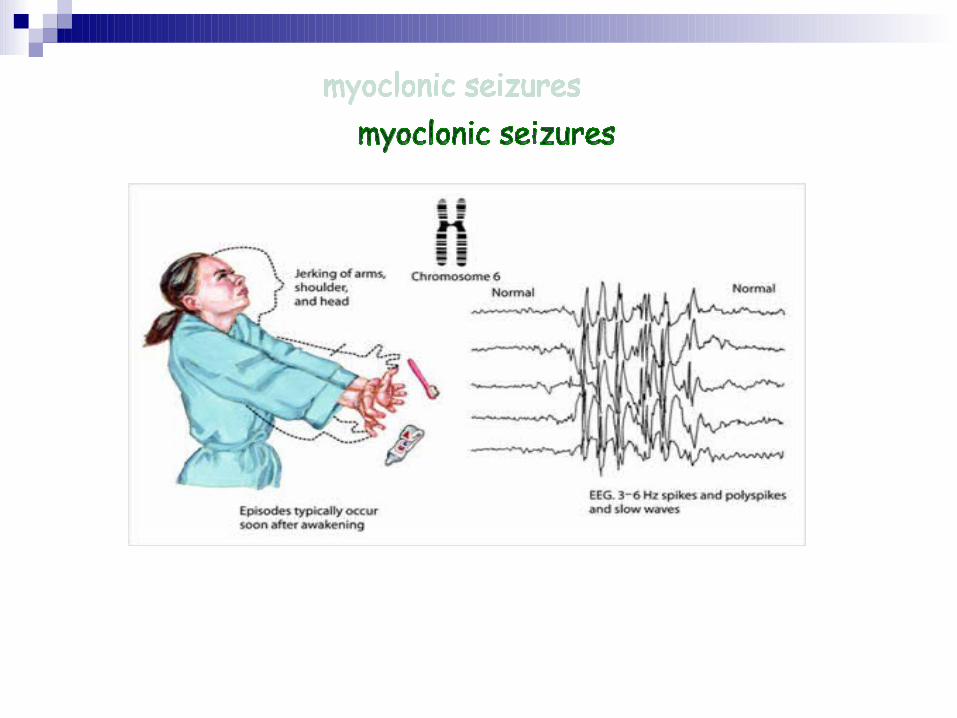
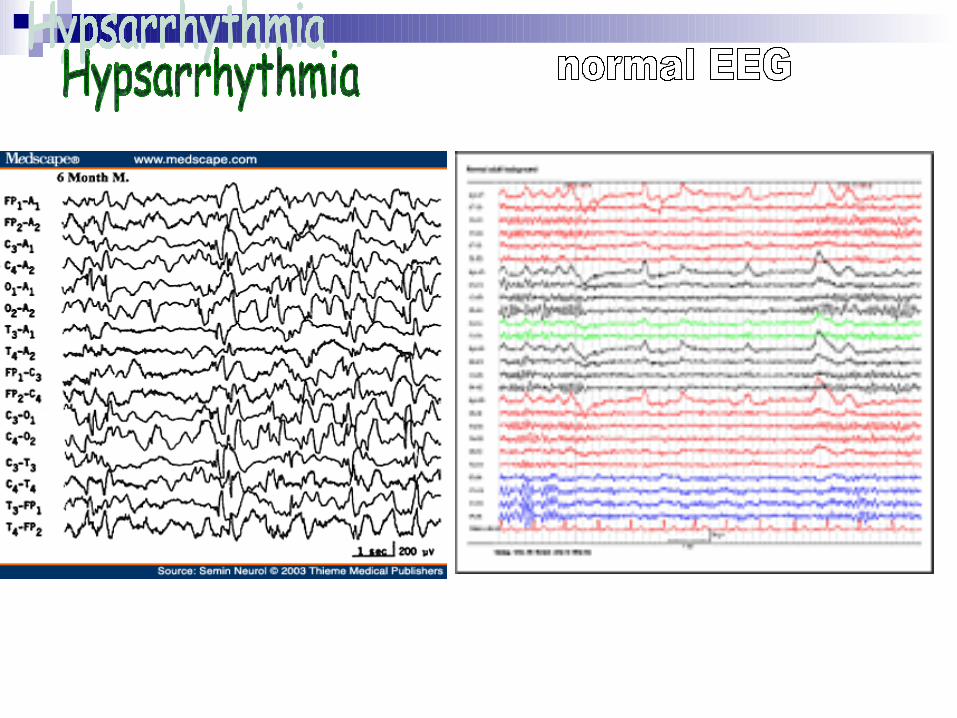
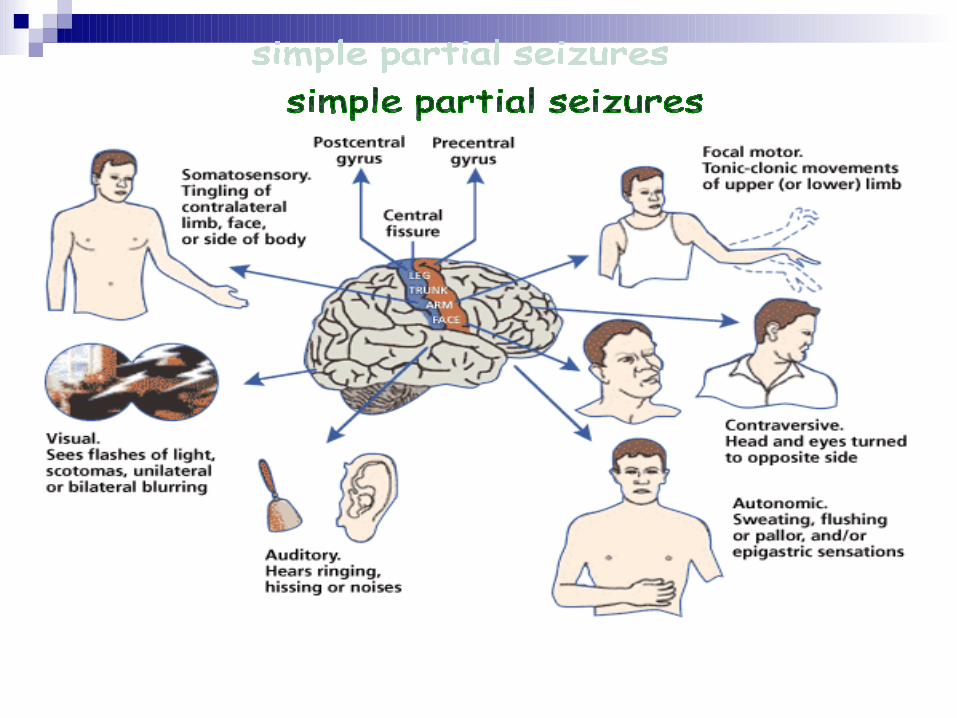
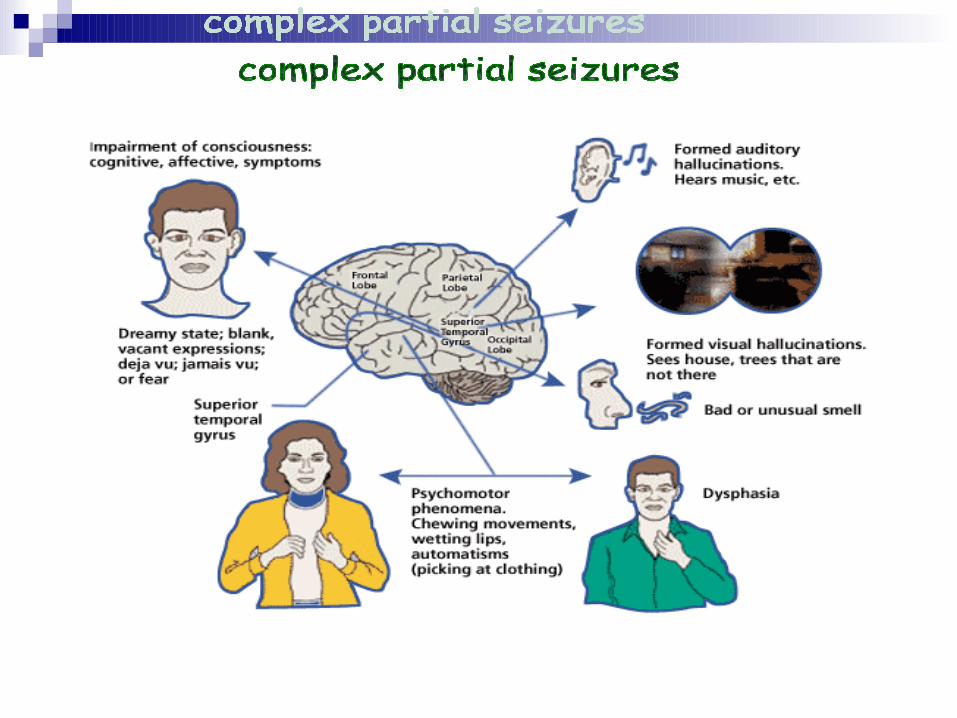
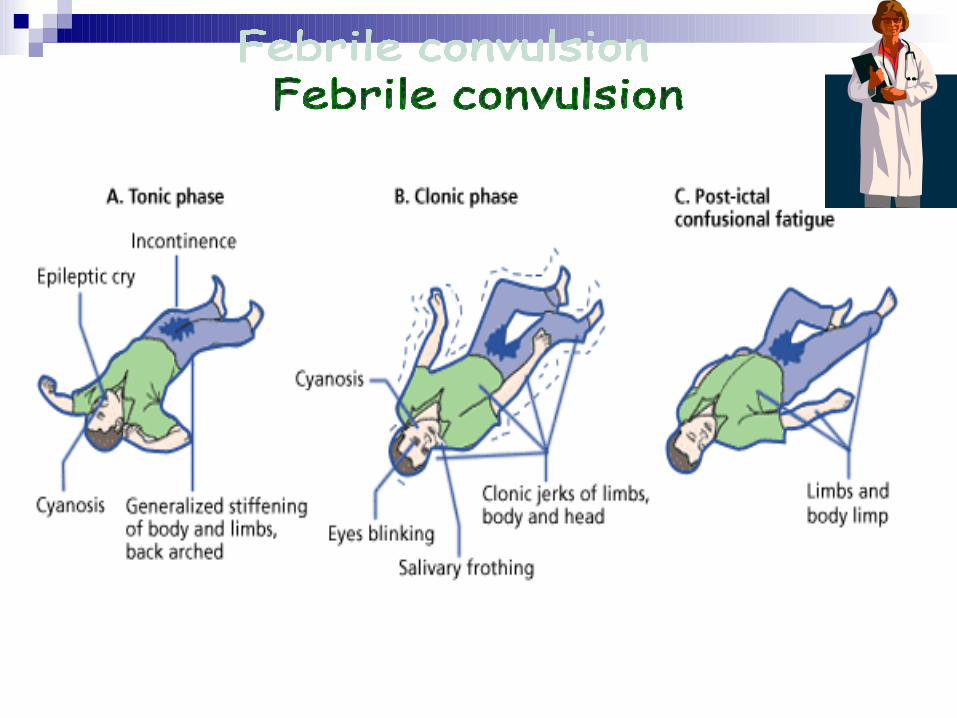
Quick review of the types of convulsion

PERSONAL H/Oage
* infantile spasm 3m-8m,rare after 2 years,* absence seizures 5-10 years ,rare before 2 years,
* febrile convulsions 6m-6years. sex
)absence seizures more in girls(. Address to know the distance.
HISTORY

Pseudosiezures:
””

H/O present illness Ictal , Preictal , Postictal .
Analysis of abnormal movement Describe this movement, How does it begin, Is it focal or generalized, How much it last, Is it the first time or not, Is it associated with :
loss of consciousness ,up rolling of eye ,cyanosis, secretions from mouth, head tilting, twitching of face , arching of spine, tongue bite, passage of urine or stool during the attack.
the pre-attack state of child ,is it perceded by :
fever & how much it was if measured by mother
)think of CNS infection or febrile convulsion “if within suggested age”(
Physical or emotional stress like excessive crying BHA
or anger SA .
Loud noisy sounds or strong flashes of light
Sleepy or just awake from sleep
possible Drugs (TCA, sympathomimitics, amphetamine(
or toxin ingestion .
Recent vaccinations
Trauma : describe trauma & assess its severity

the post-attack state of the child1-Was the attack followed by :
- Deep sleep- Coma
- Weakness or paralysis of limbs & how much each of those persist
2-how was the attack finished : spontaneously or with medications?

Systemic review
In systemic review try to roll out:*-Infection of CNS or any other system
*-hi ICP :vomiting, (headache & blurred vision in older children(.
*-Dehydration & electrolyte imbalance:
Suggested by h/o severe diarrhea or vomitting.
Birth H/O “ M u s t b e t a k e n i n de t a i l”
ANH: chronic illness (DM , HTN, PE ( , any bleeding: suggest Ischemic-hypoxic ecephalopathy.
Exposure to radiation or ingestion of teratogenic drugs ( as a cause of congenital cerebral malformations (
Natal H/O : prolonged or precipitate labour ,abnormal presentation, cord around the neck; (as cause of
birth asphyxia(.
Maturity (premature more risk of IVH , post mature risk of MAS(.
Post natal H/O
-Birth weight (LBW IVH( , cried immediately or not.
-Discharged on the same day or stayed in NN ICU .
-Any postnatal admission , h/o jaundice ( assess whether it was significant or not , e.g. when
appeared, disappeared, how treated?...(

Immunization h/o : if the attack preceded by vaccination.
Developmental h/o:
How old is child now & what can he do?
Was the child well & then regress in development (think of neurodegenerative disorders(
Presence of any neurological abnormality exclude febrile convulsions.

Past H/O:
*Ask whether this is the first attack or not, if not :
Describe the previous attacks , how treated ,and what was the diagnosis?
*Any previous admissions to hospital
*Any significant illness :
-Cerebral palsy: risky to develop seizures
-Renal failure: presented with seizures due to hypocalcaemia, hyponatremia
-DM : complicated by hypoglycemia

Family H/O
1-Of similar attacks, what was diagnosis (febrile convulsion usually have positive family H/O(
2-Of epilepsy
3-of consanguinity ( may suggest inherited metabolic disorders (
1-General examination*Level of consciousness (GCS(
*Vital signs & search for any obvious focus of infection. *Bulged AF in infant , papilledema in older children may
suggest ICP.*In older children ,check signs of meningeal irritation.
*Examine skin for stigmata of neuro-cutaneous disorders( café aulait spots, hypopigmented areas ,hemangioma(
2-Complete neurological examination to make sure of normal CNS.
3-Developmental assessment
EXAMIANTION

* CBC
* Blood glucose
* Septic work-up:
(Blood culture,urine culture, LP, CXR, throat swab(.
* Serum electrolytes( Na ,Mg ,Ca (
* Toxicology screen ( if drug overdose suspected( or metabolic screen
* CT,MRI : if h\o trauma or suspect rise ICP.
* EEG may play a role.
INVESTIGATION
Initial treatment:
A-Maintain airway patent , Put child in semi -prone position with head down to help drainage of secretions.B-Adequate breathing : O2 mask
C-Circulation : iv drip , normal saline & dextrose
D-Drugs : diazepam ,phenytoin ,phenobarbitone
Treatment of the cause accordingly.
Treatment

11 فاطمة فخري طاهر months old, female Libyan patient, lives in Benghazi blood group is A+ve , and the , )الليثي)history is taken from her mother.
She’s admitted on Friday 23th of may 2008 , at 5 pm,
Complaining of high fever and abnormal movement for 2 days before the admission.
Fever was high grade, measuring up to 40°C ,
starting from 2 weeks back as a symptom of gastroenteritis.
She had supportive and symptomatic treatment, but fever didn’t relieve completely.
Not associated with sweating , skin rash, chills or rigors.
No h/o any ill person of the family.
Panadol and cold sponging was used to decrease the temperature. With no increasing factors.

Regarding the abnormal movement: The 1st attack was on Friday before dawn at
2:30 am. Which persist for 15 minutes.
The mouth was cyanosed, and jerky movement of upper and lower limbs with loss of consciousness.
Post ictally, Fatima was sleepy and fatigue.
No thing abnormal by examination.
Investigation done:
CBC:
Hb 9.9 gm/dl
RBC 3800*10³
WBC 12.8*10³
MCV 86 fl
MCH 26 fl
Blood glucose 77 Blood urea 17 S. creatinine 0.5 Na 135 Ca 1.14
Lumber puncture: ( normal result )
CSF glucose 67 mg
CSF protein 19 mg
No RBCs or WBCs.
X-ray hand is done. And Fatima was putted on convulsion chart.
Next 2 days :
No other attacks had been happened.
Mother is advised to notice any rising in temperature of her daughter.
And discharged!!!!!.


4 أحمد أشرف مسعود years old Libyan patient, lives in Benghazi. History is taken from his mother.
Admitted to the hospital on Thursday, 12nd of June 2008 because of an abnormal limb movements 2 days before the admission.
No thing abnormal on examination, Also no thing abnormal by investigation .

So what’s the plan