Embed Size (px)
Citation preview

Role of Adjunct devices in PCI
Dr Mahadeva Swamy BSR Cardiology, JIPMER

Adjunct devices in PCI Plaque modification
Cutting Balloon (CBA)
Laser (ELCA)
Atherectomy (DCA, PTRA)
Thrombectomy
EPD
Plaque modification Atheroablative devices during PCI → facilitate
procedural success and reduce restenosis
Plaque modification is valuable tool for treatment of complex lesions
Vessel pretreatment → larger MLD and lower TLR rate

Lesion pretreatment & plaque modification Regular balloon & stent do not adequately
address problems of plaque shift and resistant lesions
Lesion pretreatment is to facilitate procedural success and reduces restenosis
Mechanism:Minimizes plaque shifting
Decreases recoilOptimal stent expansion


Cutting balloon angioplasty (CBA) Cutting balloon – controlled longitudinal
incisions (atherotomy)
Improve luminal enlargement at lower pressure inflation
Improved acute results with less barotrauma → long term clinical benefit

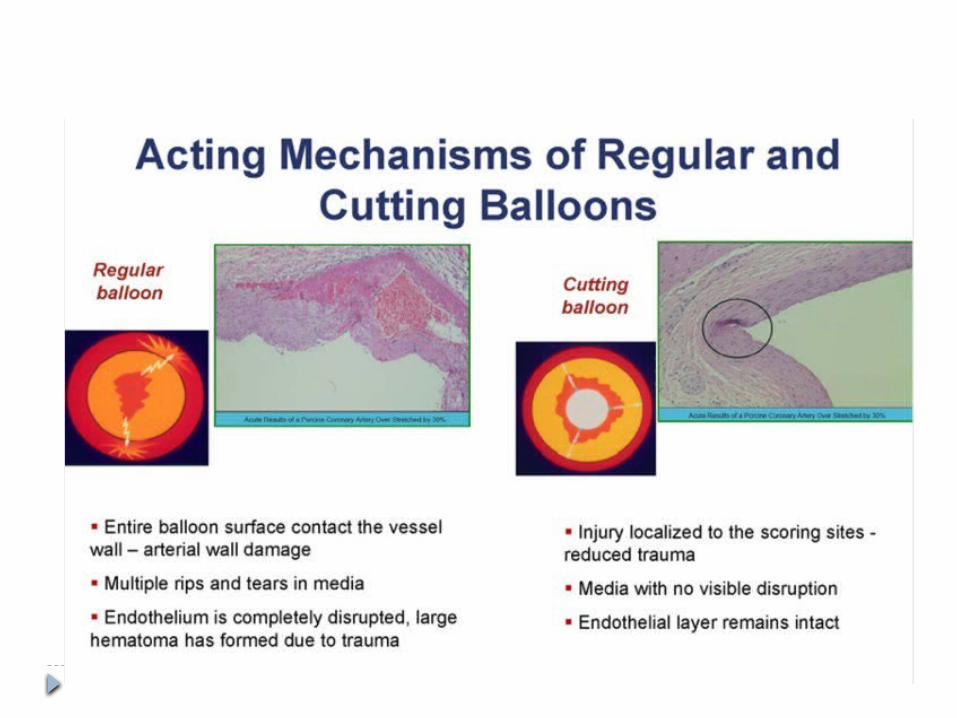
Mechanism of action of CBA Controlled microincisions in atheroma at lower
pressure – reduced barotrauma
Better luminal enlargement at lower pressures
In calcified lesions, CBA achieves larger lumen gain
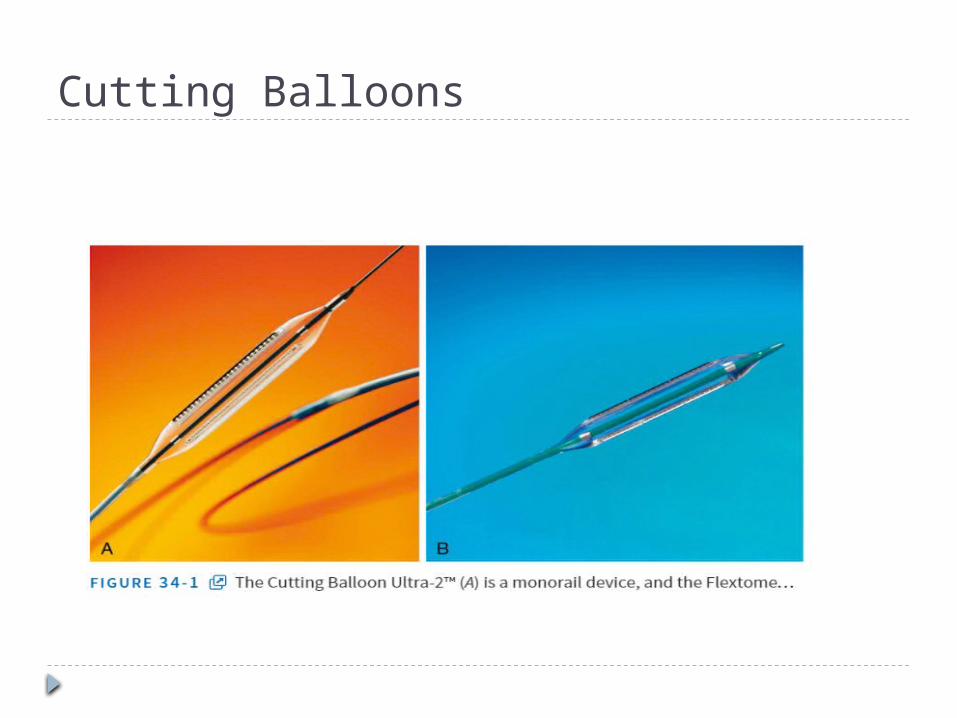
Cutting Balloons
Equipment Cutting balloons – 6, 10 & 15 mm
Atherotomes (3-4)are mounted longitudinally along the balloon surface
Atherotomes Balloon diameter3 2 & 3.25 mm 4 3.5 & 4 mm

Technique Less compliant and trackability
Tortuous proximal anatomy – CBA may not be feasible
Risk of blade fracture or retention – minimized by slowly inflation and deflation
Complications: Slightly higher risk of coronary perforation (0.8 %
vs 0.0 %)
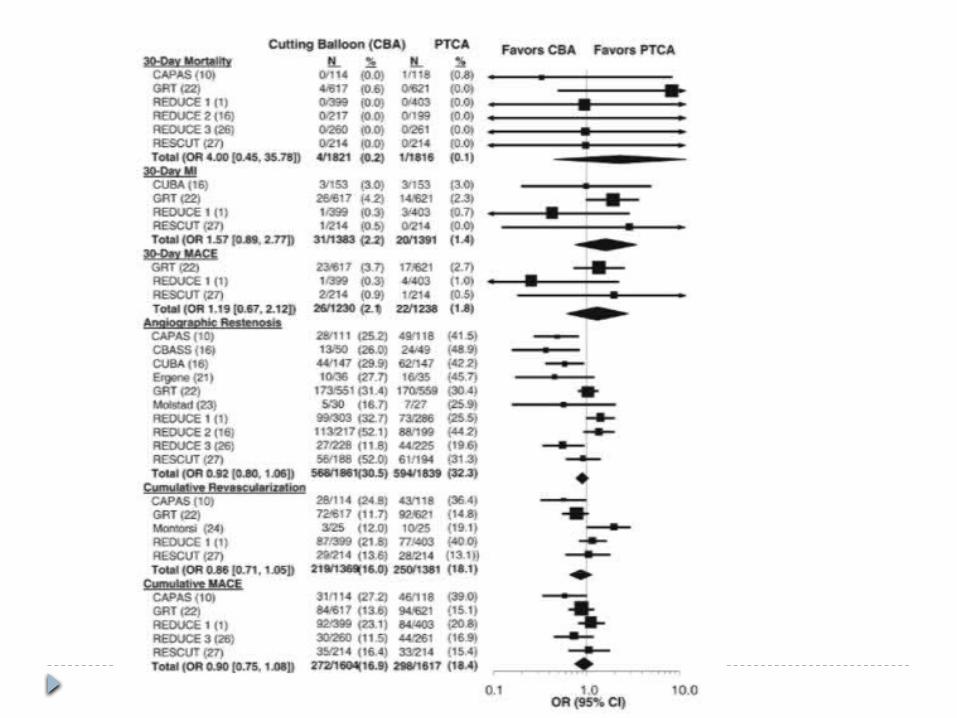

Conclusion: Cutting/scoring balloon In RCT, cutting balloon alone has not shown to
improve outcomes compared to balloon angioplasty
CBA – Plaque modification in complex procedures
Bifurcation lesions Ostial lesions Mild to moderately calcified lesions Instent restenosis
Lesion selection Bifurcation lesion – plaque shift and high
restenosis CBA lower restenosis (40 % vs 67%)
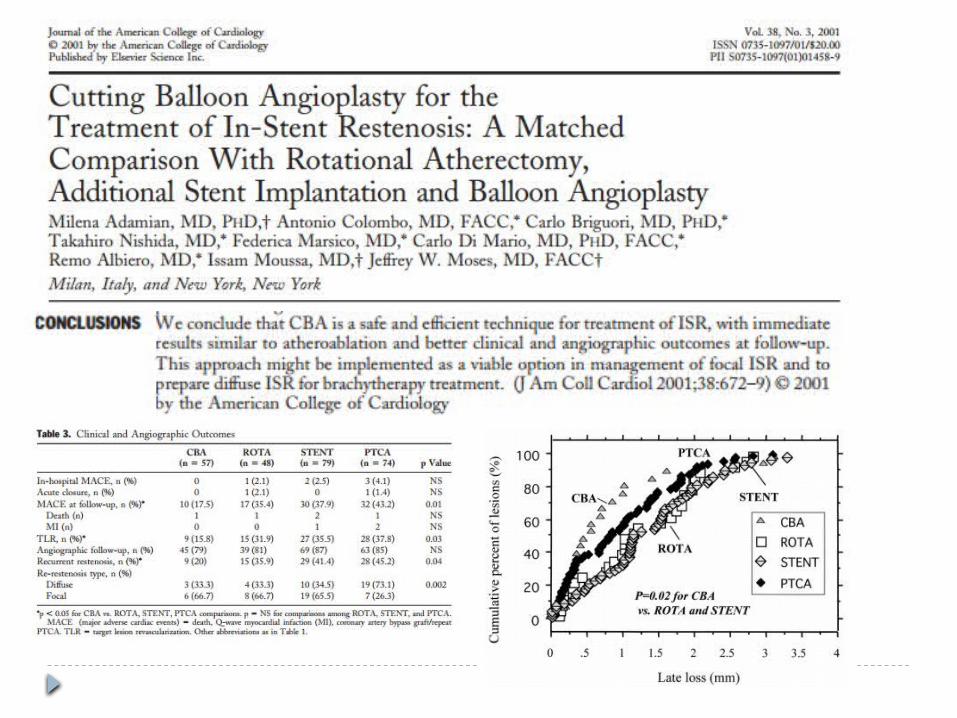
Instent restenosis (REDUCE 3 trial ) Reduced balloon slippage Plaque extension through the stent struts
Ostial lesions

CBA recommendations Class IIb
Cutting balloon angioplasty might be considered to avoid slippage-induced coronary artery trauma during PCI for in-stent restenosis or ostial lesions in side branches. (LOE: C)
Class III:Cutting balloon angioplasty should not be performed routinely during PCI. (LOE: A)
2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention

Angiosculpt Scoring balloon catheter – semicompliant
balloon with nitinol spiral cage
Low crossing profile (2.7F)
More flexible alternative to cutting balloon

Laser angioplasty ELCA – precise plaque removal
Infrequently used (high cost, lack of benefit over PCI alone)
Adjunctive method for debulking
Excimer laserExcimer laser in UV wavelength is well absorbed by both atheromatous plaques and thrombi
Laser : Thrombolysis Inhibit platelet aggregation May ablate atherosclerotic plaque
Tissue ablation mechanisms: Vaporization of tissue (Photothermal effect) Ejection of debris (Photoacoustic effect) Direct breakdown of molecules (Photochemical
dissociation)
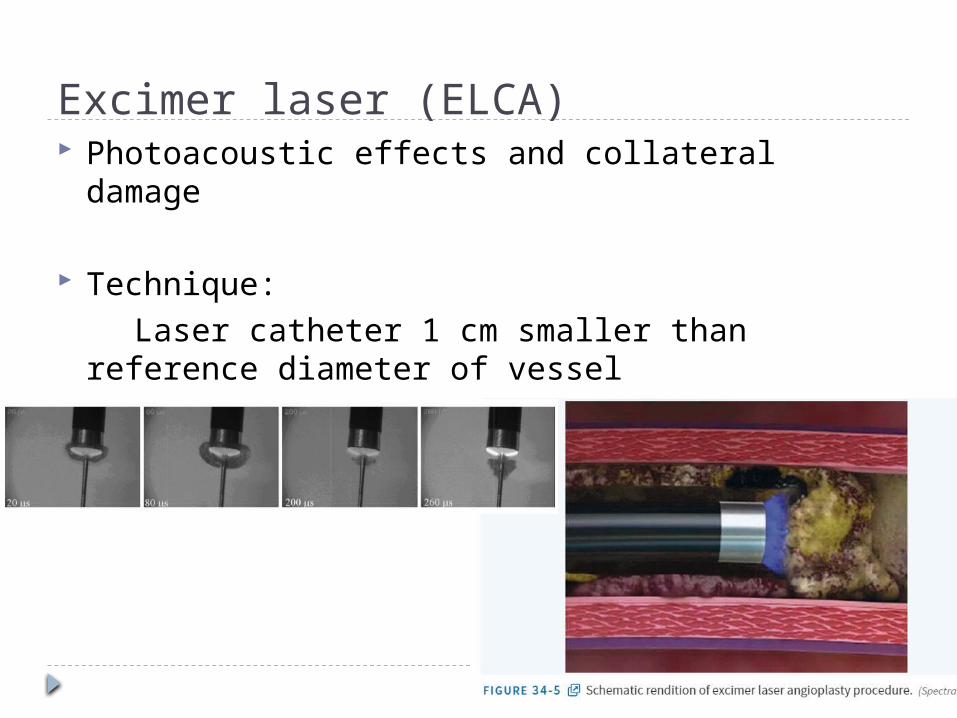
Excimer laser (ELCA) Photoacoustic effects and collateral damage
Technique: Laser catheter 1 cm smaller than reference
diameter of vessel Saline flush Slow catheter advancement at 0.2 mm/s → maximal
ablation
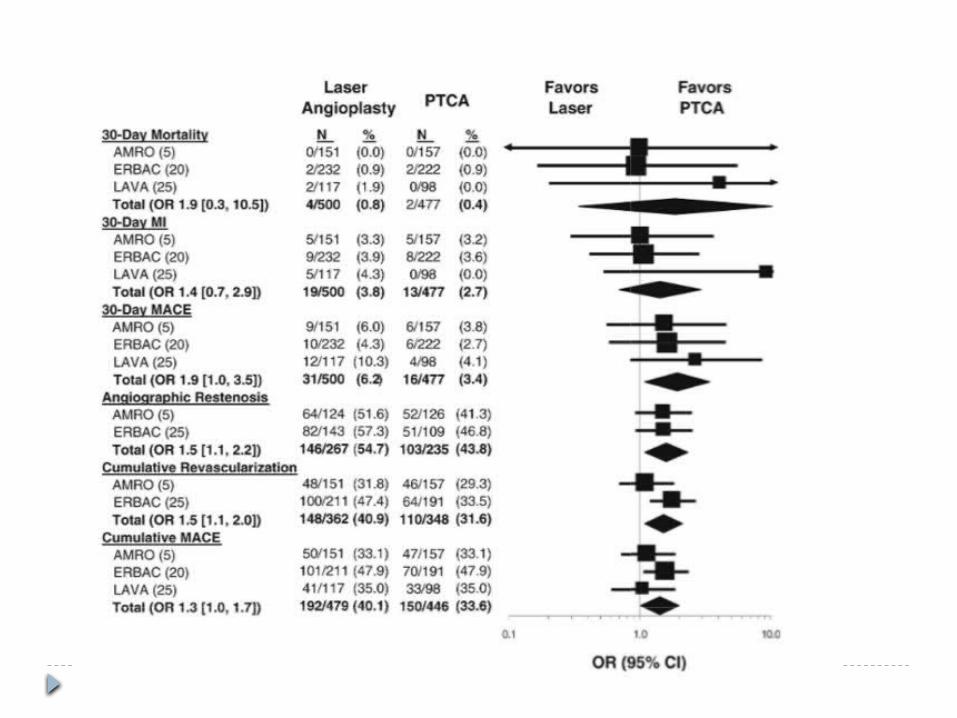

ECLA: Lesion selection Long lesions
Moderately calcified lesions
Total occlusions (AMRO trial – successful recanalization in 60 % of uncrossable total occlusions with conventional guidewires)
Undilatable lesions ( ECLA has similar success rate as PTRA)
No benefit in ISR
ECLA recommendations Class IIb . Laser angioplasty might be considered for
fibrotic or moderately calcified lesions that cannot be crossed or dilated with conventional balloon angioplasty.(LOE: C)
Class III. Laser angioplasty should not be used routinely during PCI. (LOE: A)
2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention

Directional coronary atherectomy (DCA) First FDA approved non balloon PCI device (1990)
SilverHawk – novel plaque excision system
DCA failed to acheive better clinical outcome compared to PTCA in randomized trials
Periprocedural MI Difficulty in achieving optimal debulking
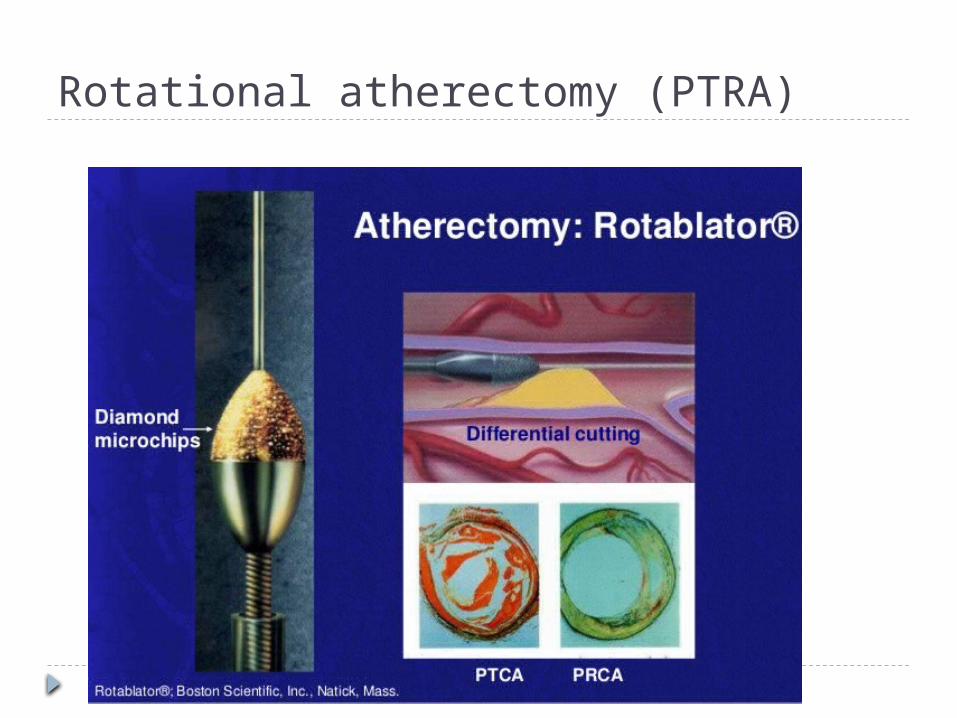
Rotational atherectomy (PTRA)

Mechanism of PTRA Differential cutting
Cuts more rigid, inelastic material
Orthogonal friction displacement Reduces friction between vessel wall and entering device
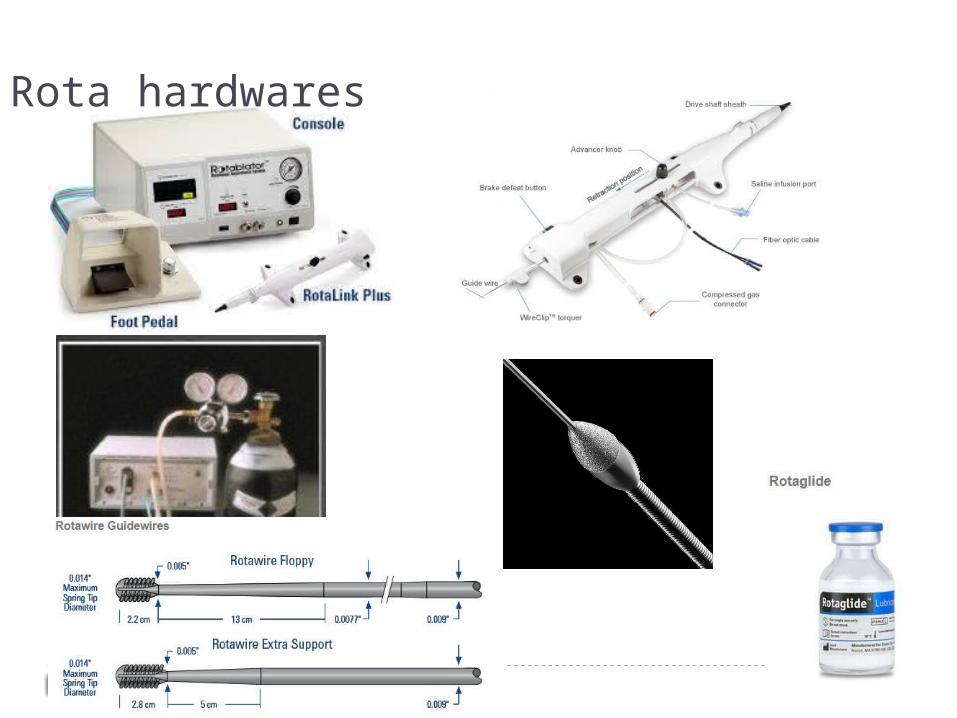
Rota hardwares
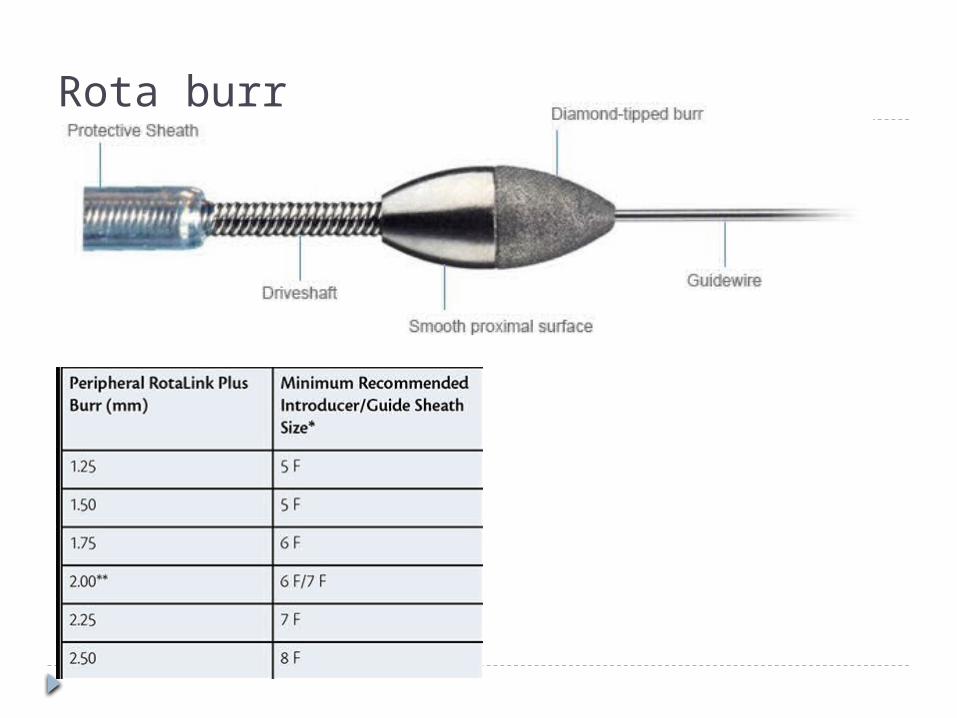
Rota burr
Burr /artery ratio: 0.7 Rotational speed up to 2,00,000 rpm
Lower rpm 1,40,000 a/w less heat generation and platelet activation
Runs should be limited to 20 seconds
Decelerations of >5000 should be avoided
Contraindications to Rotablation Dissection Angulated lesions (> 60-90⁰) Thrombus containing lesion Saphenous venous grafts Acute MI

Indications for PTRA Calcified lesions Undilatable lesions Bifurcation lesion Ostial lesion

Complications Slow flow, no reflow Non QWMI Coronary perforation Dissection Bradycardia & AV
block Vasospasm
Rotablator system failure
Burr entrapment (Kokesi effect)
Burr detachment Burr stalling Rota guide wire
fracture

PTRA recommendations Class IIa
Rotational atherectomy is reasonable for fibrotic or heavily calcified lesions that might not be crossed by a balloon catheter or adequately dilated before stent implantation. (LOE: C)
Class III: Rotational atherectomy should not be performed routinely for de novo lesions or in-stent restenosis. (LOE: A)
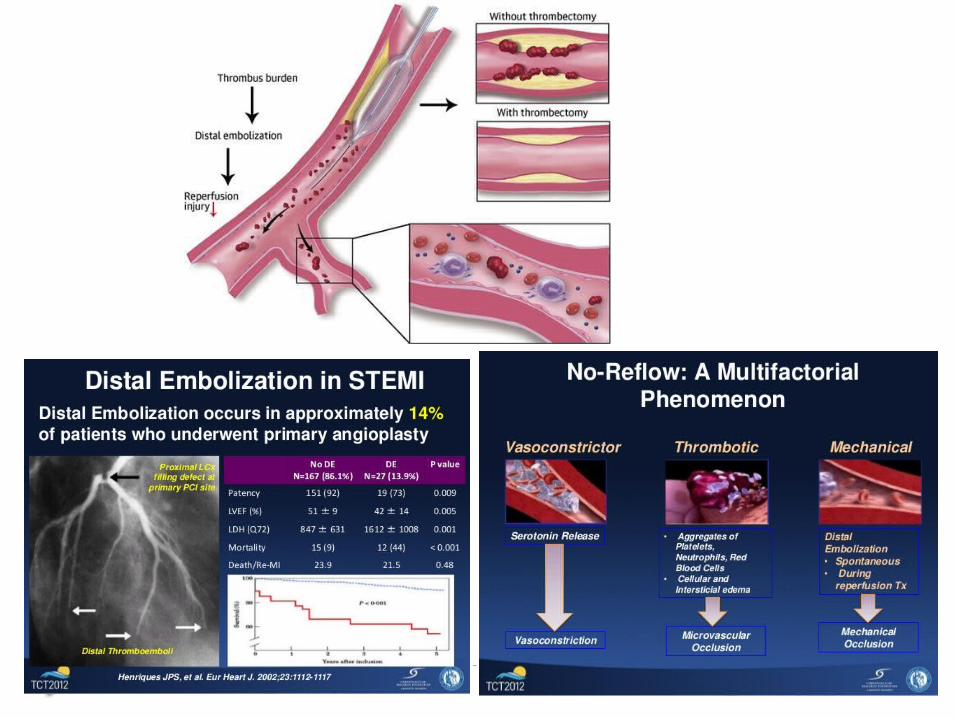

Mechanical thrombectomy PCI in acute MI @ distal emboli, no reflow & abrupt
closure
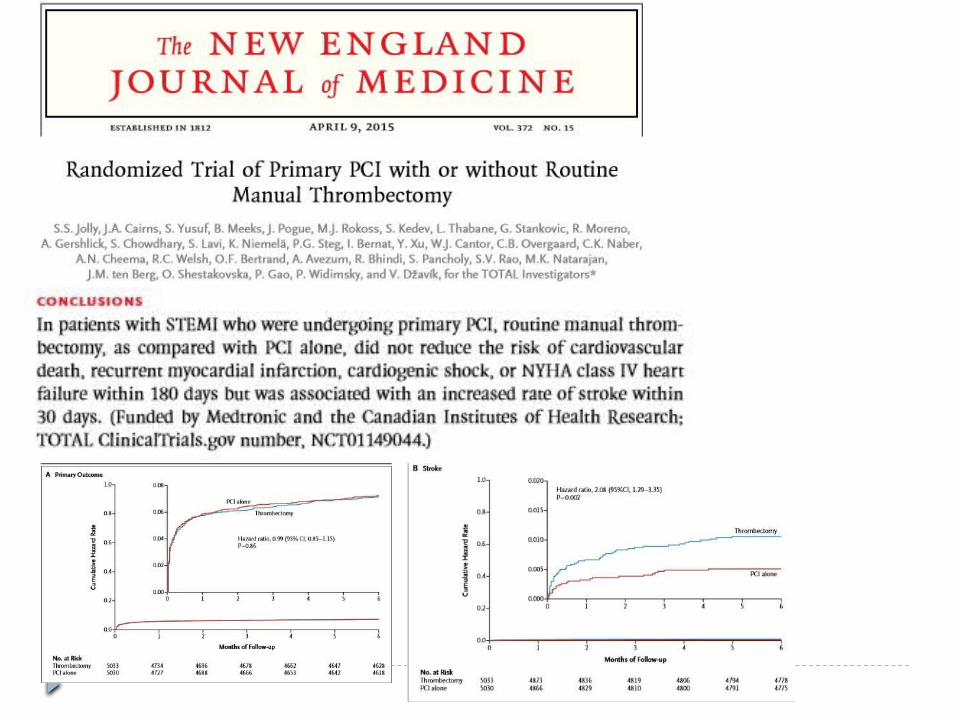
Thrombectomy in primary PCI was a/w improved myocardial perfusion (TIMI III flow, MBG 3, & ST resolution)
No difference in overall 30 day mortality
Increased risk of stroke
Survival benefit with manual aspiration catheters and worse outcome with mechanical devices

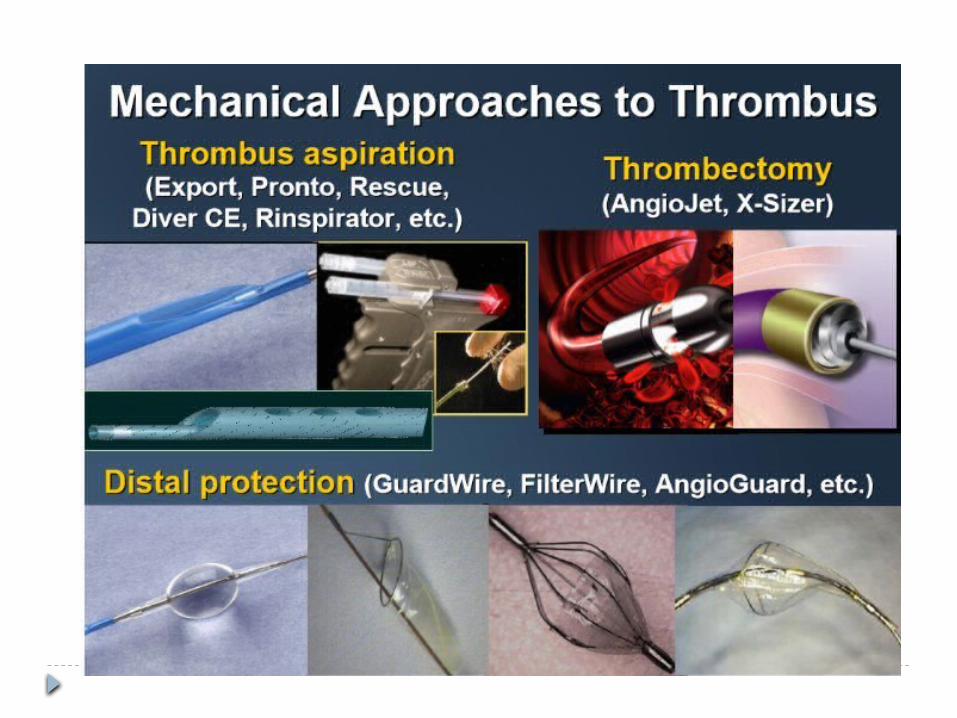
Simple vs ‘Complex’
X-Sizer AngioJet ThromCat
Pronto Export Diver

Manual thrombus aspiration Reduction of thrombotic burden Prevents of thrombus embolization Preservation of microvascular integrity Reduction of infarct size Improved myocardial tissue perfusion Improved LV function recovery and modelling


Limitations: Difficult delivery along tortuous vessels Reduced ability to aspirate at distal segment Dissection/perforation Distal embolization Insufficient thrombus removal

Power sourced thrombectomy devices Angiojet rheolytic thrombectomy Excimer laser X-Sizer
Higher extraction yield in large thrombus burden
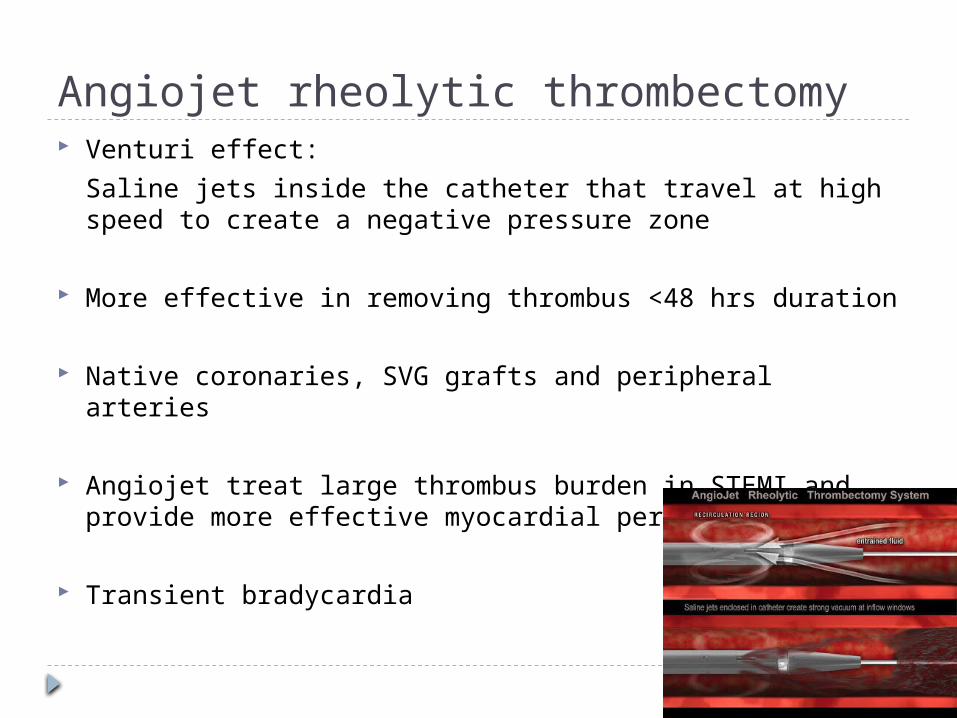
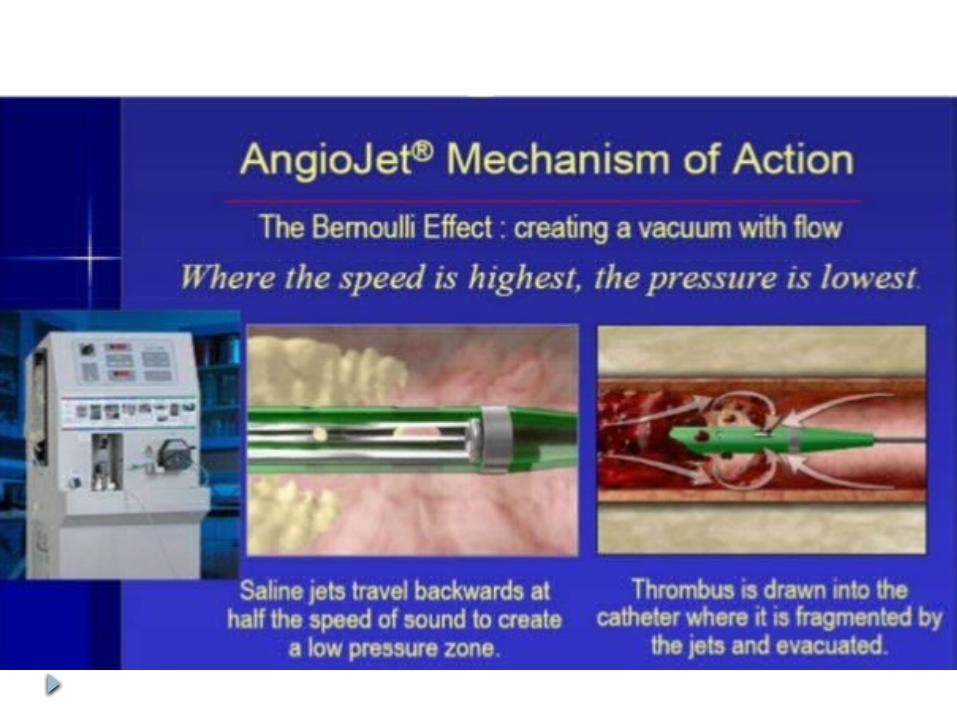
Angiojet rheolytic thrombectomy Venturi effect:
Saline jets inside the catheter that travel at high speed to create a negative pressure zone
More effective in removing thrombus <48 hrs duration
Native coronaries, SVG grafts and peripheral arteries
Angiojet treat large thrombus burden in STEMI and provide more effective myocardial perfusion
Transient bradycardia


Recommendations
Aspiration thrombectomy is reasonable for patients undergoing primary PCI. (Level of Evidence: B)
Coronary ultrasound thrombolysis (Acolysis) Acolysis probe deliver low frequency sound –
lyse /liquify the thrombus
Therapeutic ultrasound frequency - 19 to 50 kHz
Higher power & low frequencies →higher amplitude of probe motion (20-110 micro m) → tissue disruption, cavitation and heating
Acolysis system in SVG PCI in ACS (RCT) Lower success and higher 30 day MACE

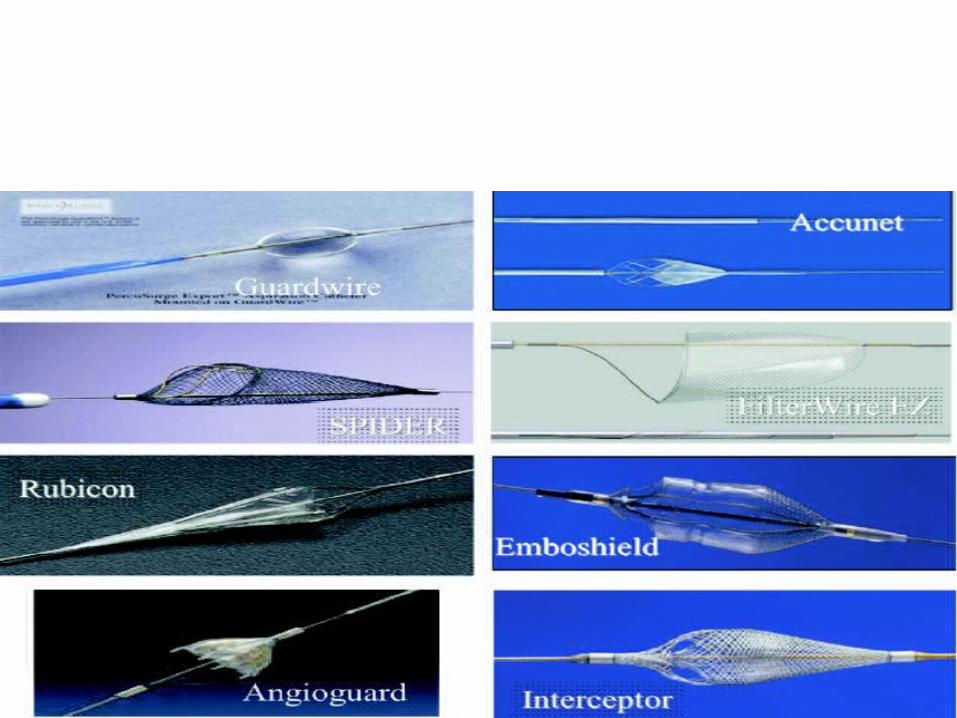
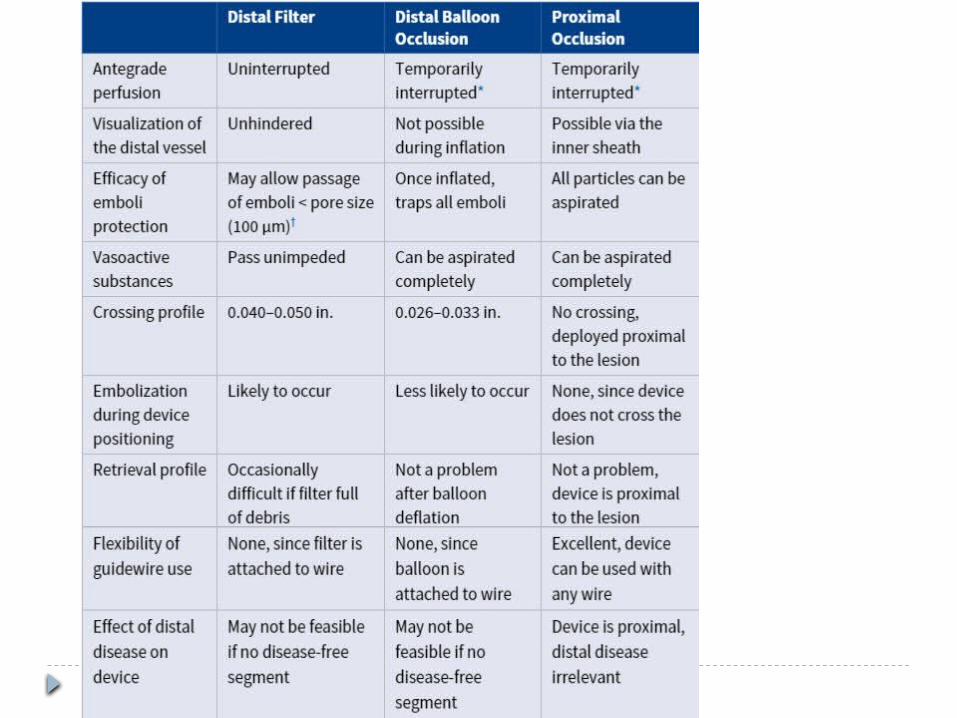
Embolic protection devices PCI of SVG grafts and thrombus lesions → distal
microembolization & spasm → no reflow and periprocedural MI
EPD’s minimize ischemic injury and no-reflow by trapping fragmented plaque & thrombus

EPD devices Primary PCI Disappointing
No benefit of routine EPD use in primary PCI (RCT- EMERALD, PROMISE, DEDICATION,
PROXIS)
Lack of benefit of EPD in acute MI Delay in reperfusion Increased embolization during delivery Embolization in to side branches

Class I Embolic protection devices (EPDs) should be used during saphenous vein graft (SVG) PCI when technically feasible. (Level of Evidence: B)


THANK YOU















![Type Interface PCI ID Vendor Description - Trend Micro PCI Ethernet... · PCI Ethernet 1022:7462 Advanced Micro Devices Inc. [AMD] AMD-8111 Ethernet PCI Ethernet 1259: ... Type Interface](https://img.dokumen.tips/doc/110x75/5ae414087f8b9a90138e713b/type-interface-pci-id-vendor-description-trend-micro-pci-ethernetpci-ethernet.jpg)


![UltraScale Devices Gen3 Integrated Block for PCI Express v4...° Compliant with the PCI Express Base Specification, rev. 3.0 [Ref 2] ° Compatible with conventional PCI software model](https://img.dokumen.tips/doc/110x75/5f5c1523f8bd7a42c663cbd7/ultrascale-devices-gen3-integrated-block-for-pci-express-v4-compliant-with.jpg)










