Embed Size (px)
Citation preview
5 PULMONARY INFECTIONS
DAVID SUTTON
DAVID SUTTON PICTURES
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
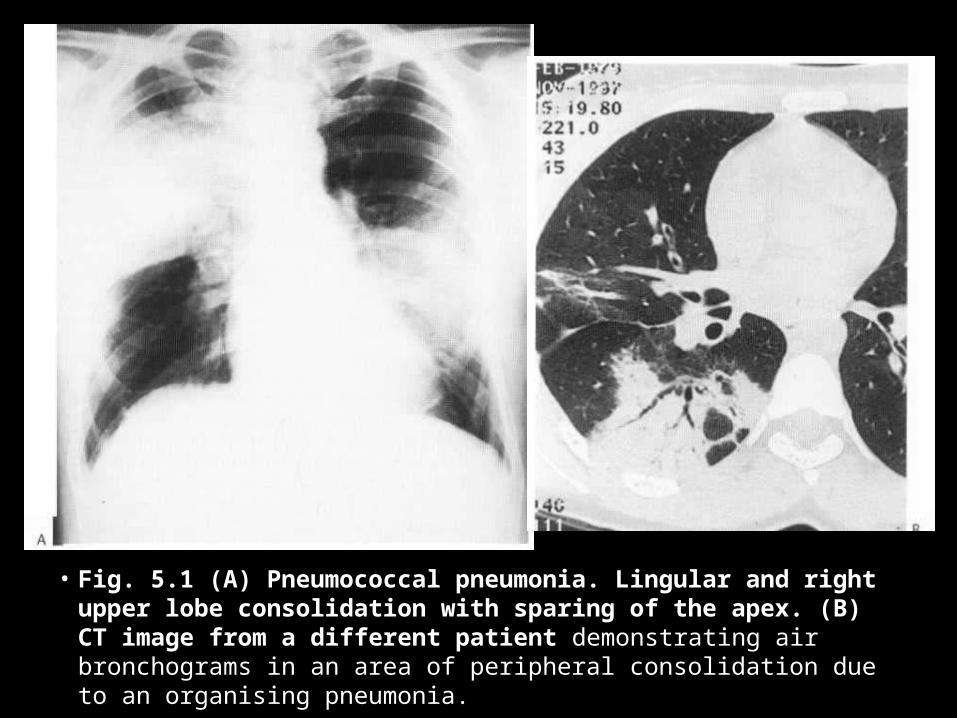
• Fig. 5.1 (A) Pneumococcal pneumonia. Lingular and right upper lobe consolidation with sparing of the apex. (B) CT image from a different patient demonstrating air bronchograms in an area of peripheral consolidation due to an organising pneumonia.
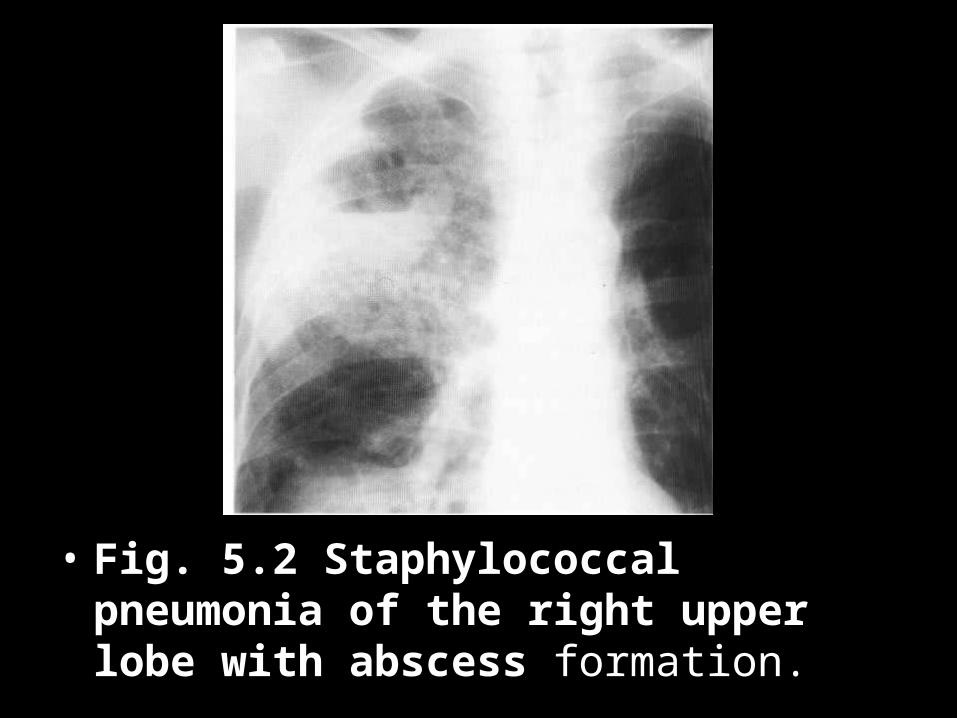
• Fig. 5.2 Staphylococcal pneumonia of the right upper lobe with abscess formation.
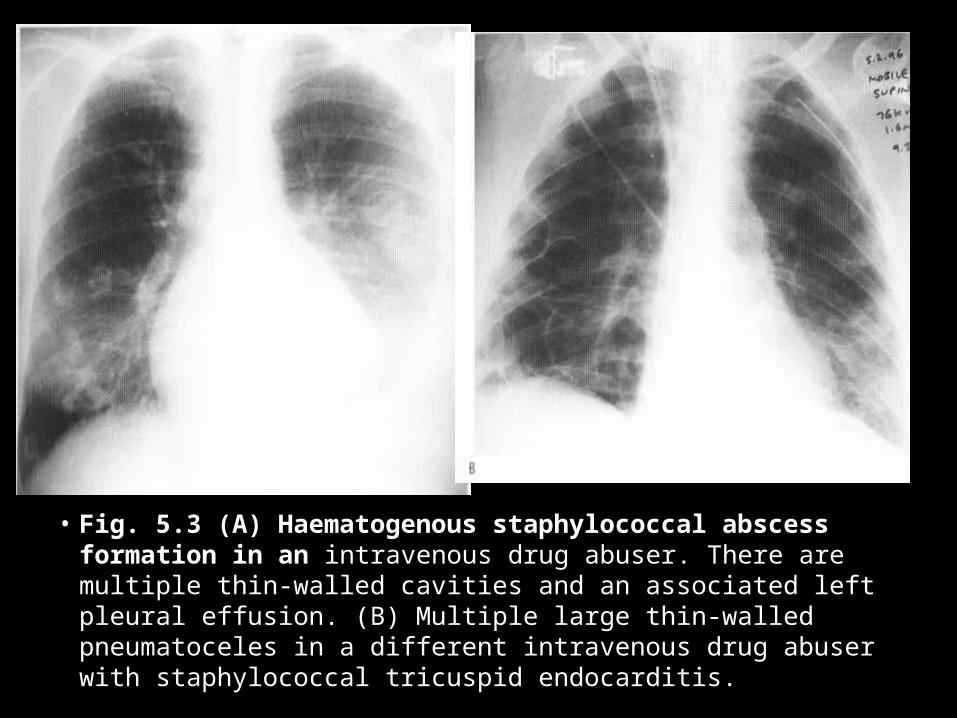
• Fig. 5.3 (A) Haematogenous staphylococcal abscess formation in an intravenous drug abuser. There are multiple thin-walled cavities and an associated left pleural effusion. (B) Multiple large thin-walled pneumatoceles in a different intravenous drug abuser with staphylococcal tricuspid endocarditis.
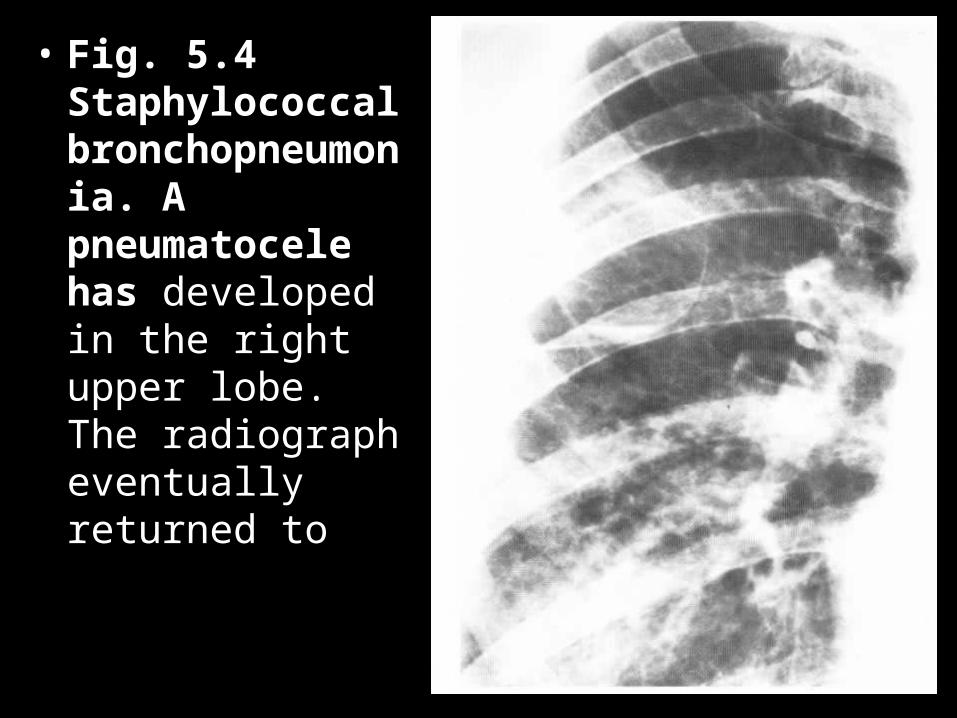
• Fig. 5.4 Staphylococcal bronchopneumonia. A pneumatocele has developed in the right upper lobe. The radiograph eventually returned to
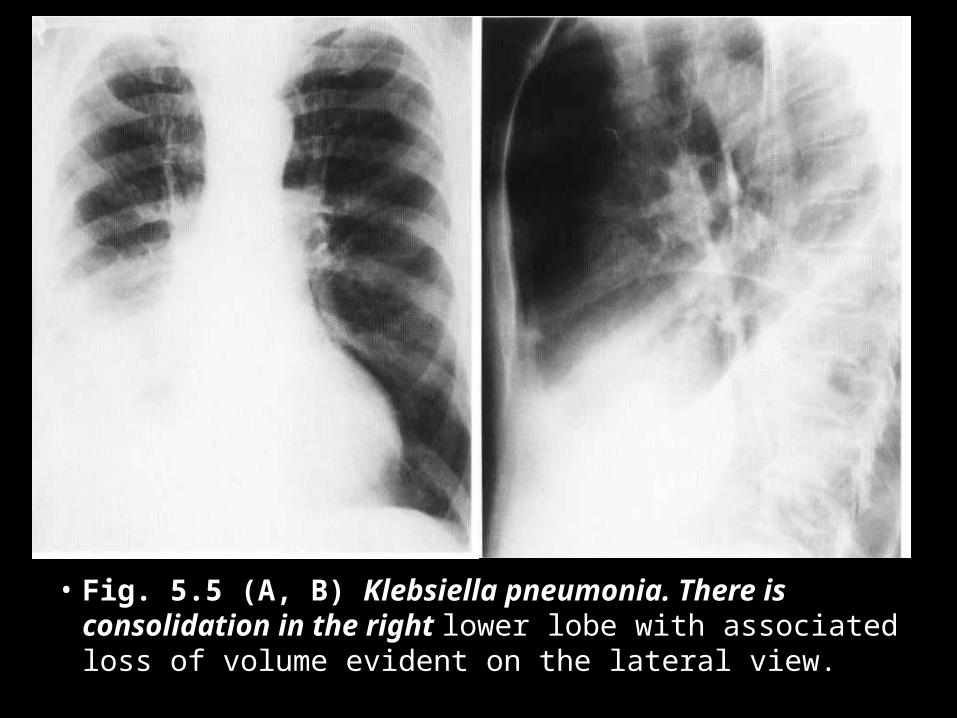
• Fig. 5.5 (A, B) Klebsiella pneumonia. There is consolidation in the right lower lobe with associated loss of volume evident on the lateral view.
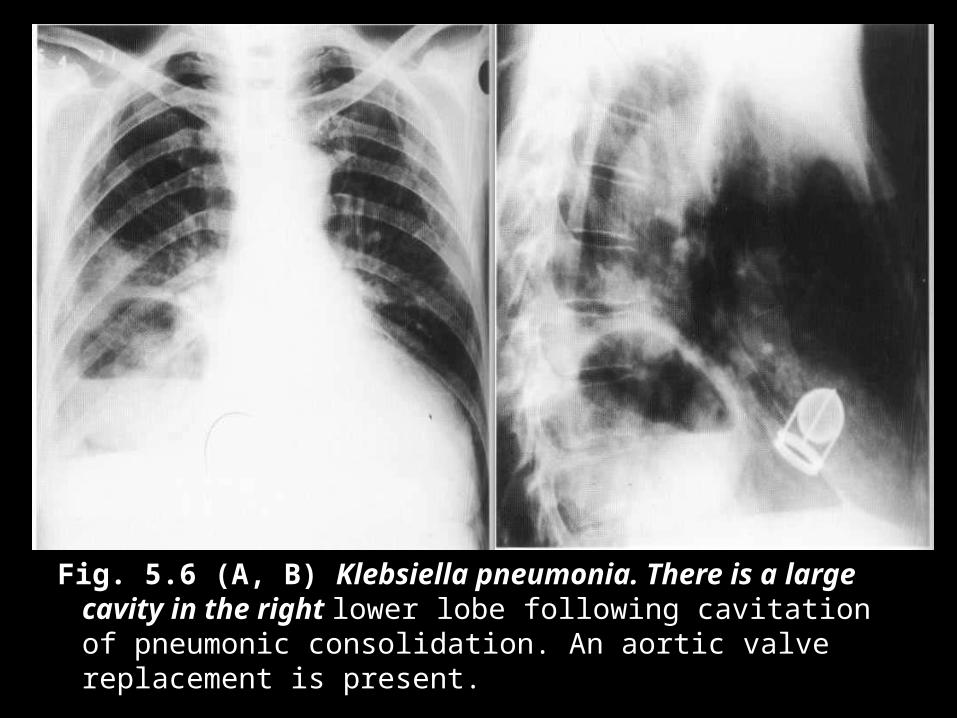
Fig. 5.6 (A, B) Klebsiella pneumonia. There is a large cavity in the right lower lobe following cavitation of pneumonic consolidation. An aortic valve replacement is present.

• Fig. 5.7 Klebsiella septicaemia. There is diffuse patchy alveolar shadowing
• with air bronchograms.
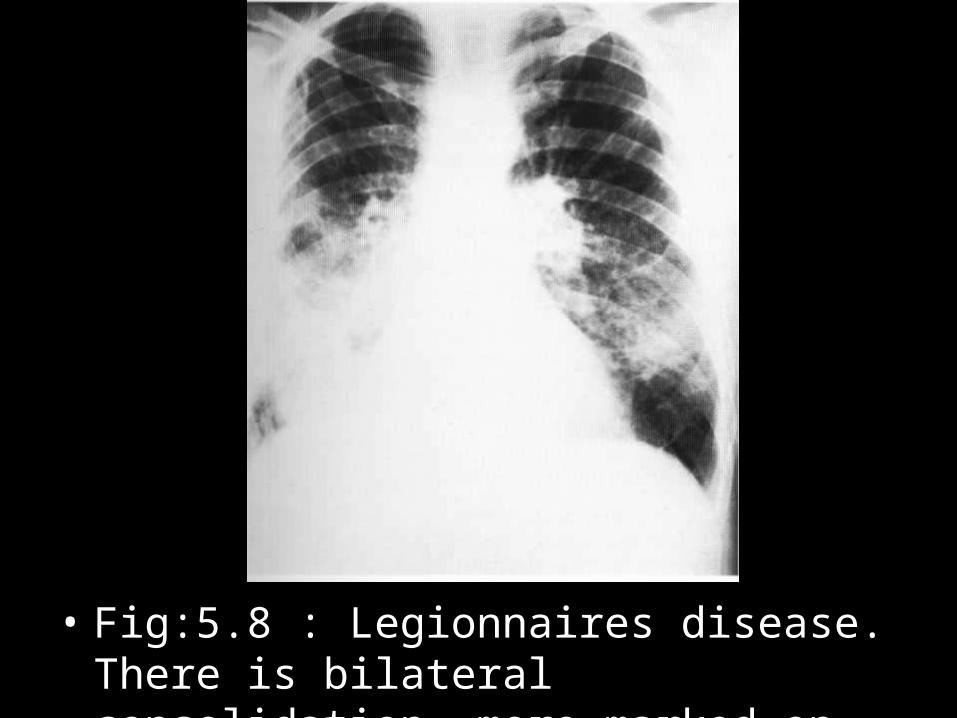
• Fig:5.8 : Legionnaires disease. There is bilateral consolidation, more marked on right.
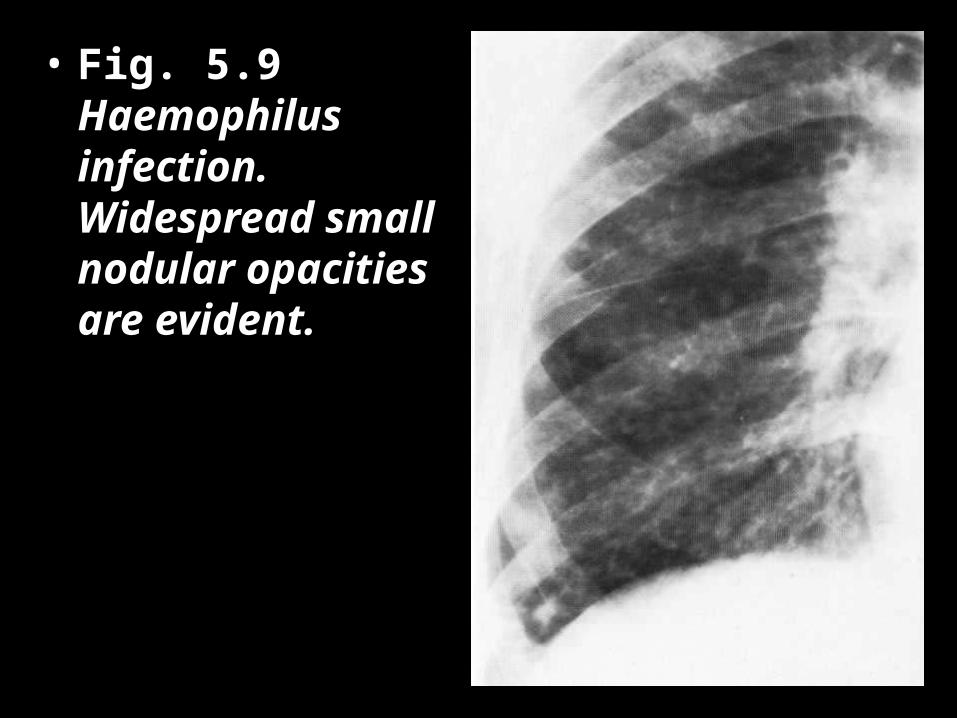
• Fig. 5.9 Haemophilus infection. Widespread small nodular opacities are evident.
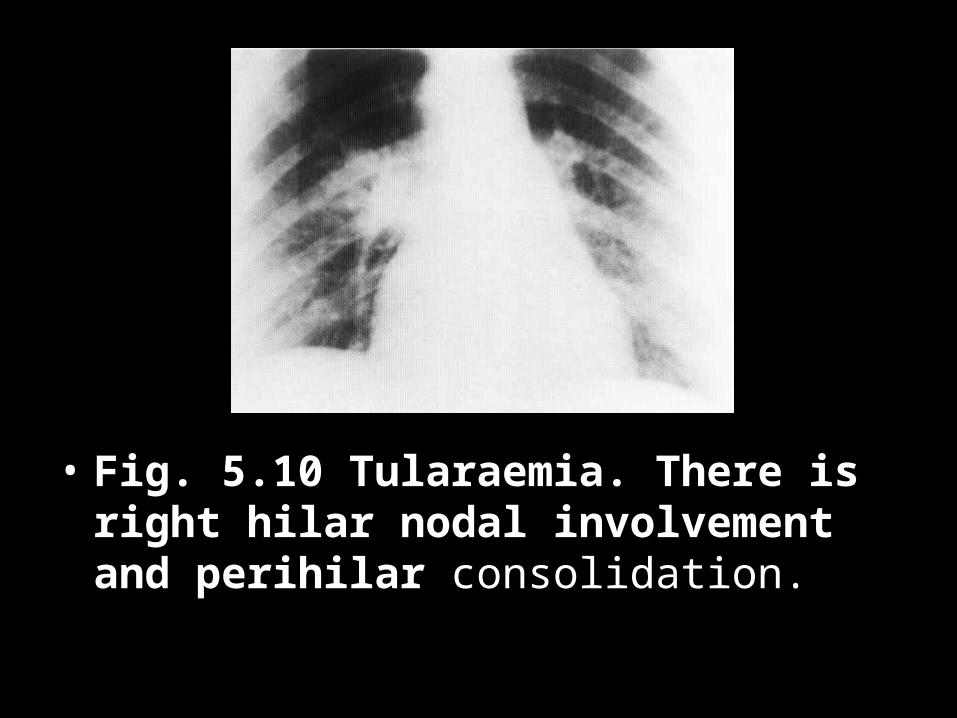
• Fig. 5.10 Tularaemia. There is right hilar nodal involvement and perihilar consolidation.
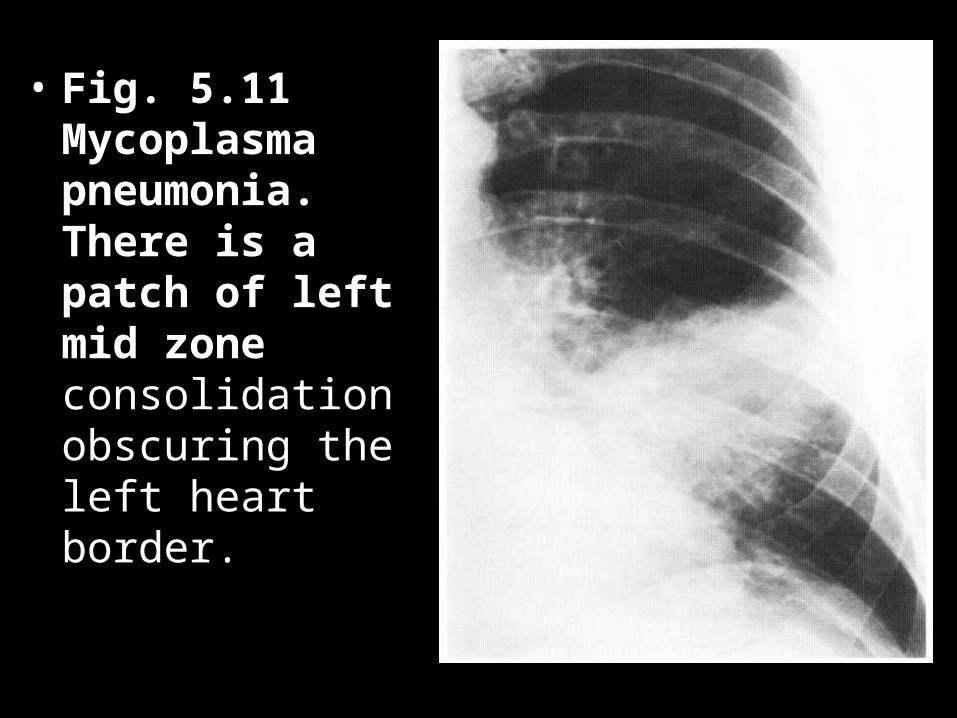
• Fig. 5.11 Mycoplasma pneumonia. There is a patch of left mid zone consolidation obscuring the left heart border.
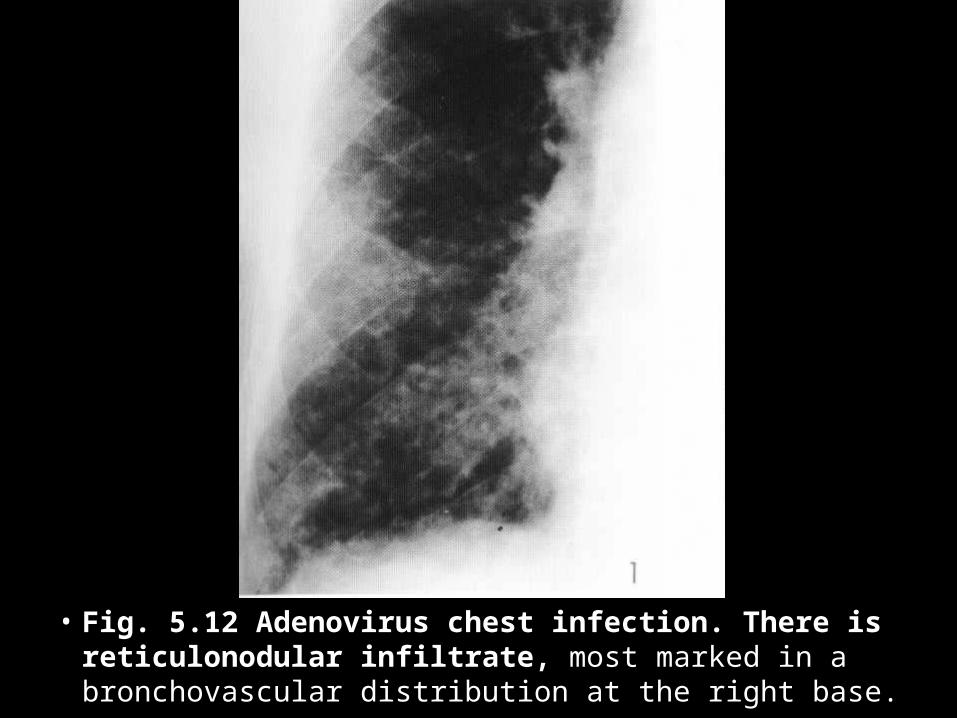
• Fig. 5.12 Adenovirus chest infection. There is reticulonodular infiltrate, most marked in a bronchovascular distribution at the right base.
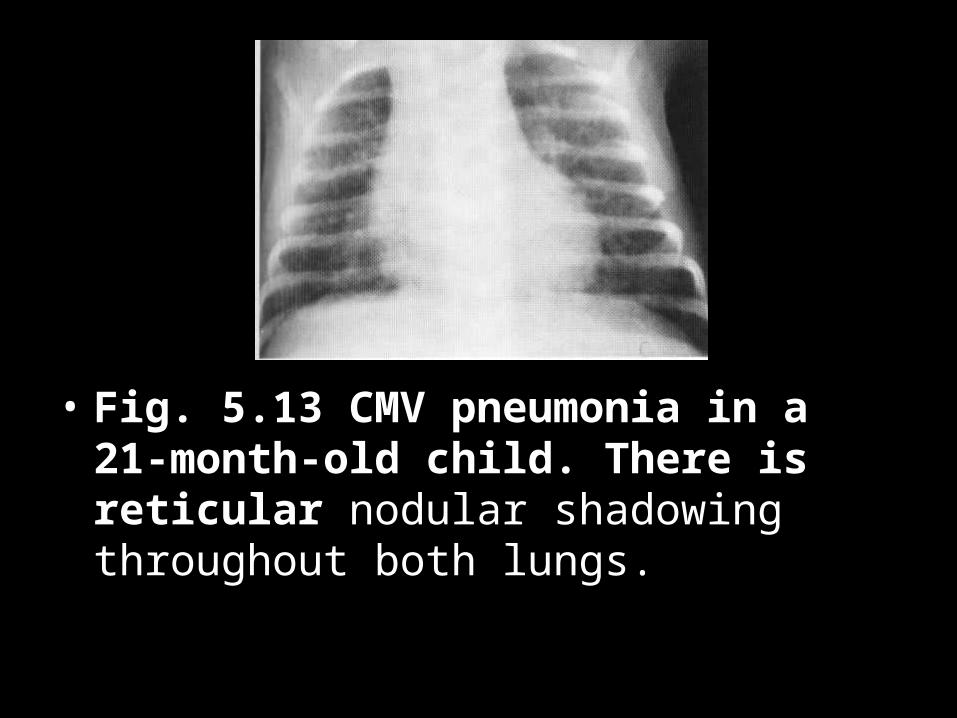
• Fig. 5.13 CMV pneumonia in a 21-month-old child. There is reticular nodular shadowing throughout both lungs.
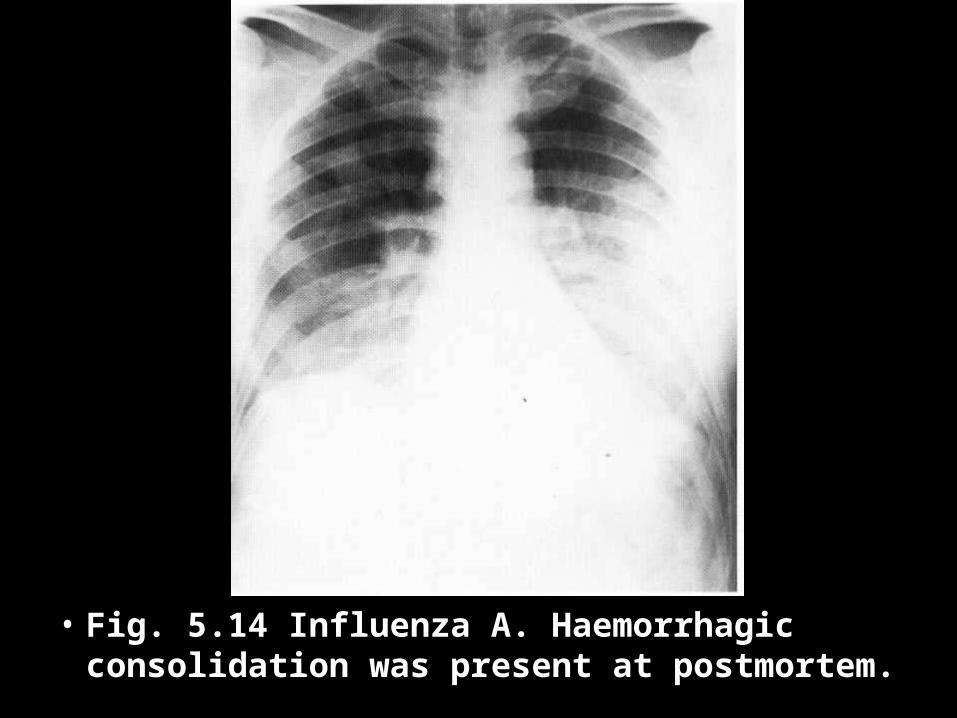
• Fig. 5.14 Influenza A. Haemorrhagic consolidation was present at postmortem.
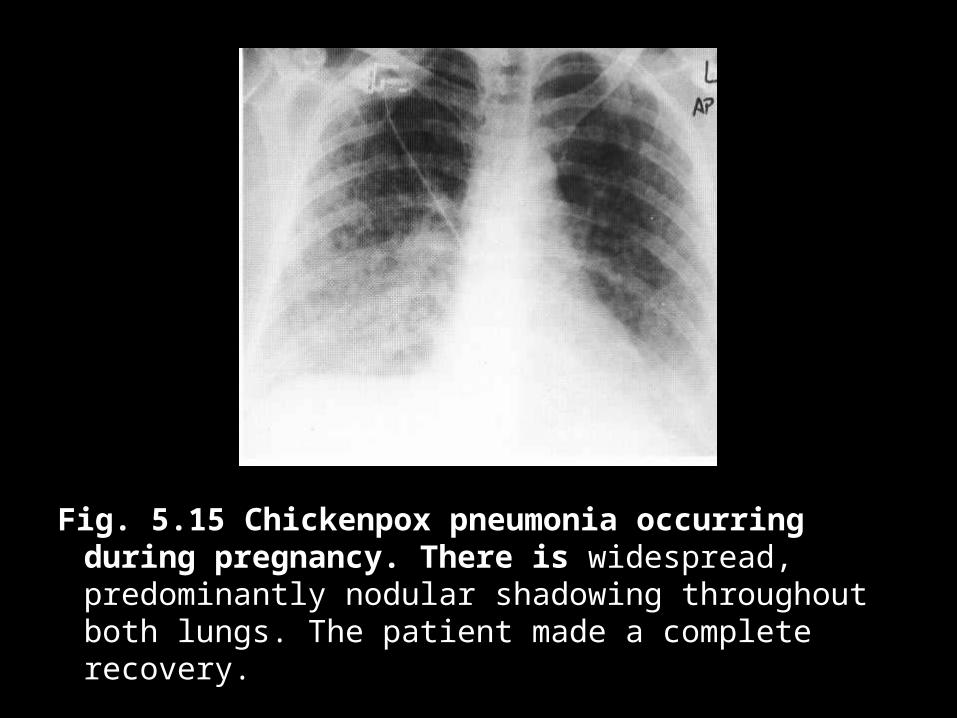
Fig. 5.15 Chickenpox pneumonia occurring during pregnancy. There is widespread, predominantly nodular shadowing throughout both lungs. The patient made a complete recovery.
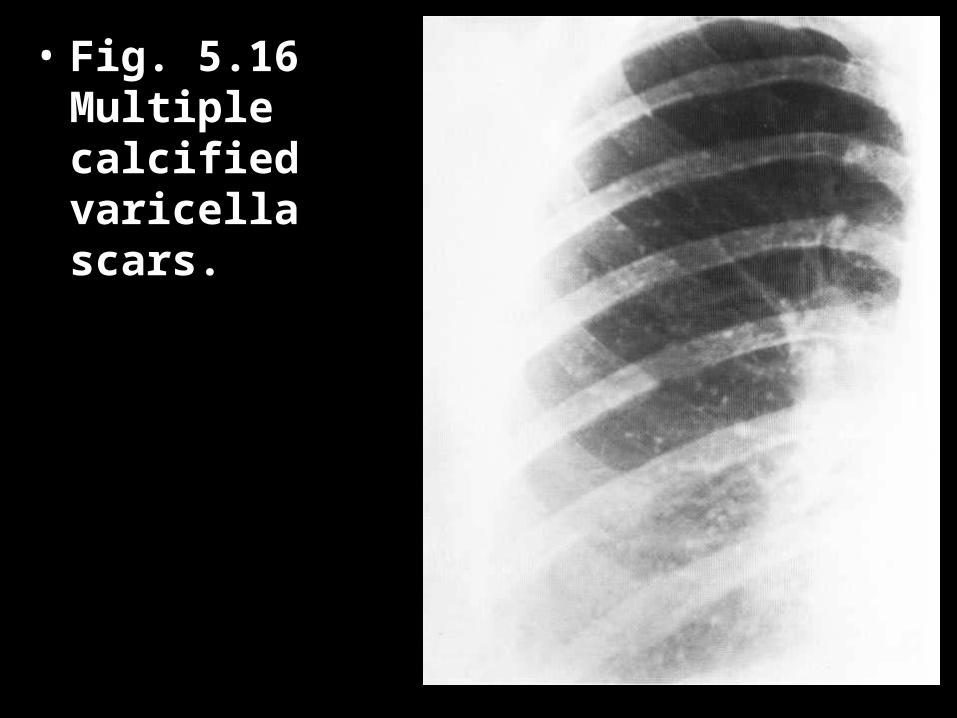
• Fig. 5.16 Multiple calcified varicella scars.
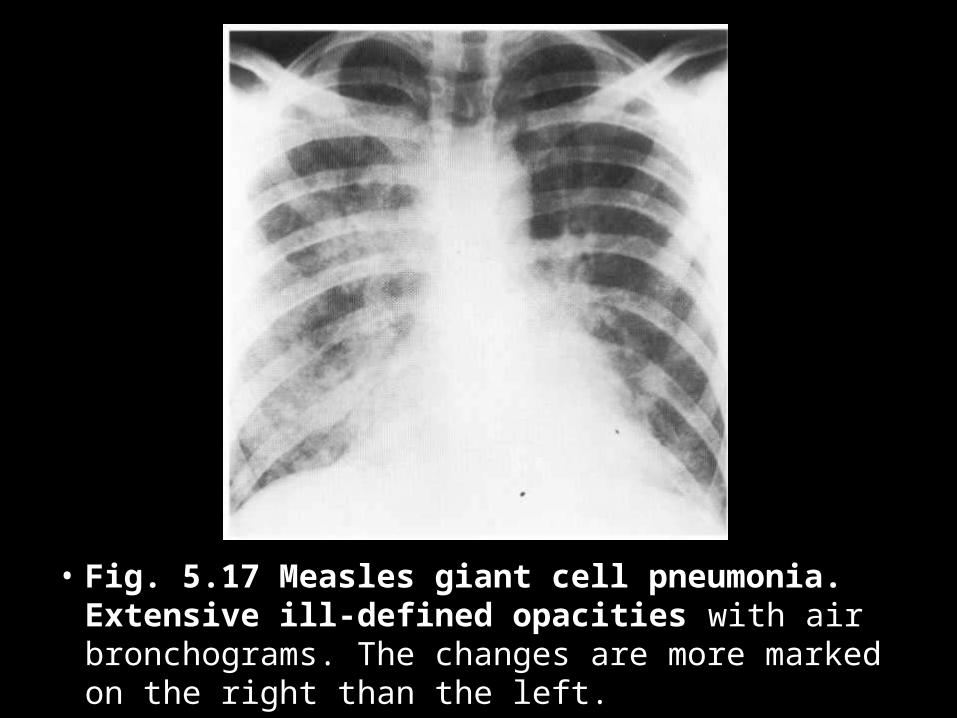
• Fig. 5.17 Measles giant cell pneumonia. Extensive ill-defined opacities with air bronchograms. The changes are more marked on the right than the left.
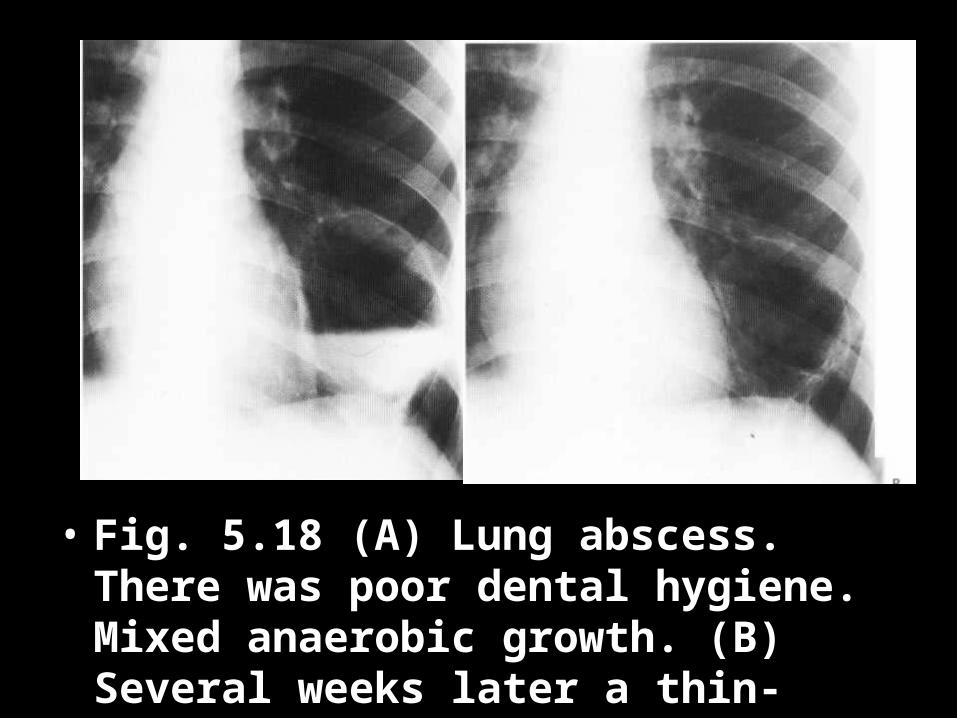
• Fig. 5.18 (A) Lung abscess. There was poor dental hygiene. Mixed anaerobic growth. (B) Several weeks later a thin-walled pneumatocele remains.
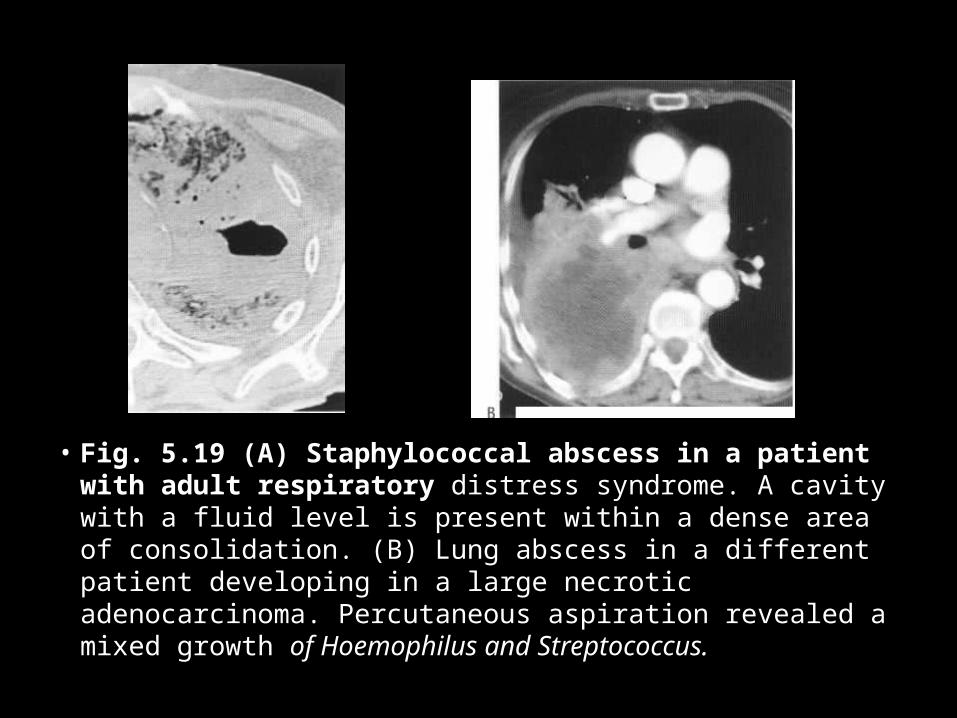
• Fig. 5.19 (A) Staphylococcal abscess in a patient with adult respiratory distress syndrome. A cavity with a fluid level is present within a dense area of consolidation. (B) Lung abscess in a different patient developing in a large necrotic adenocarcinoma. Percutaneous aspiration revealed a mixed growth of Hoemophilus and Streptococcus.
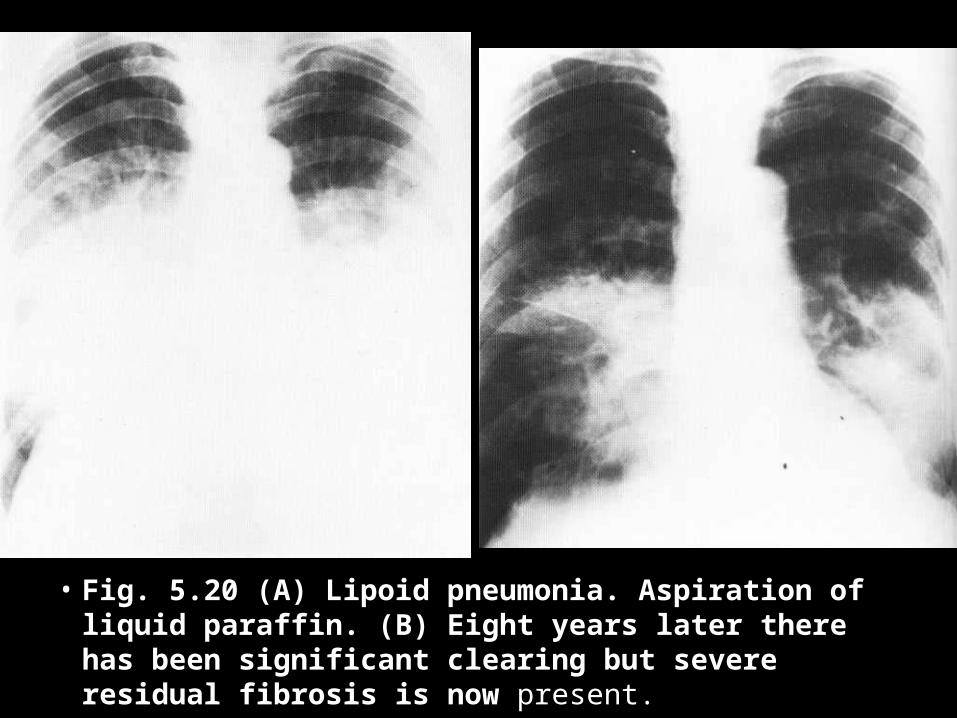
• Fig. 5.20 (A) Lipoid pneumonia. Aspiration of liquid paraffin. (B) Eight years later there has been significant clearing but severe residual fibrosis is now present.
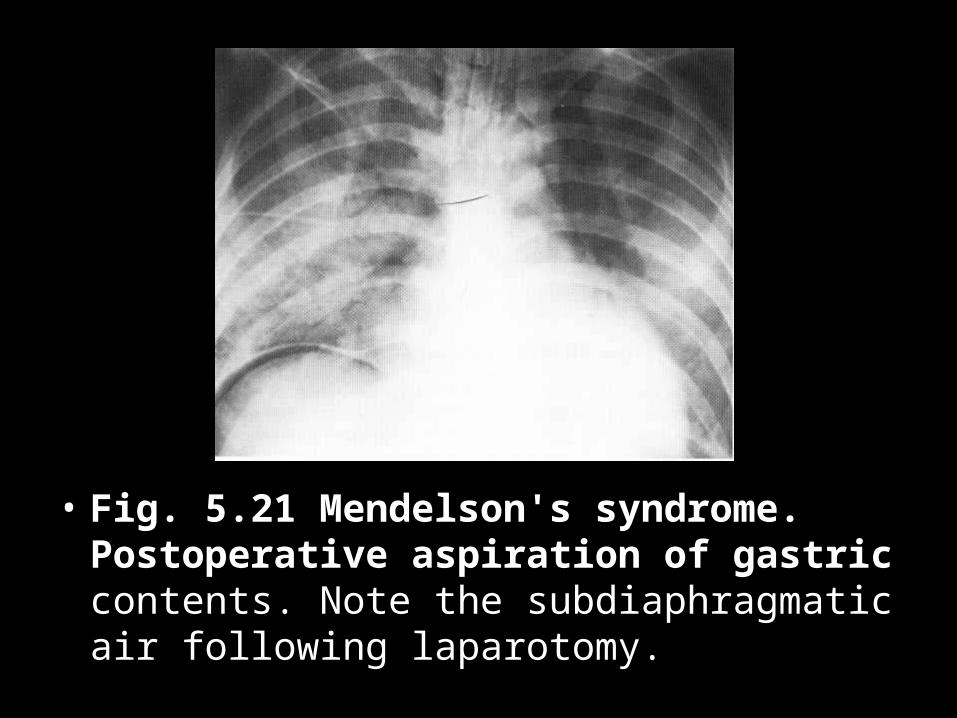
• Fig. 5.21 Mendelson's syndrome. Postoperative aspiration of gastric contents. Note the subdiaphragmatic air following laparotomy.
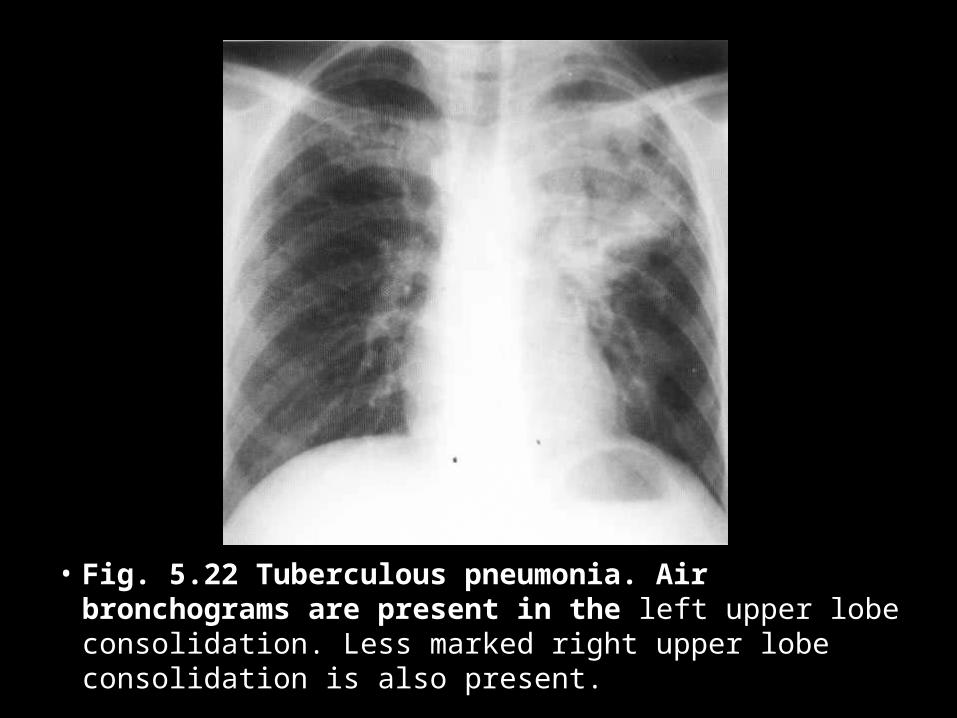
• Fig. 5.22 Tuberculous pneumonia. Air bronchograms are present in the left upper lobe consolidation. Less marked right upper lobe consolidation is also present.
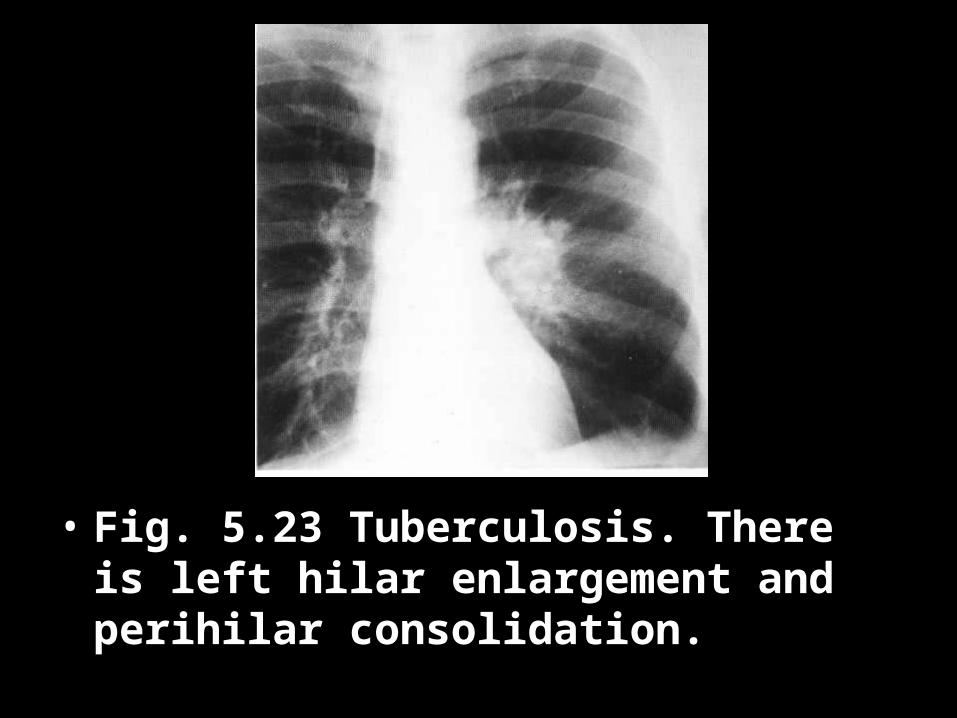
• Fig. 5.23 Tuberculosis. There is left hilar enlargement and perihilar consolidation.
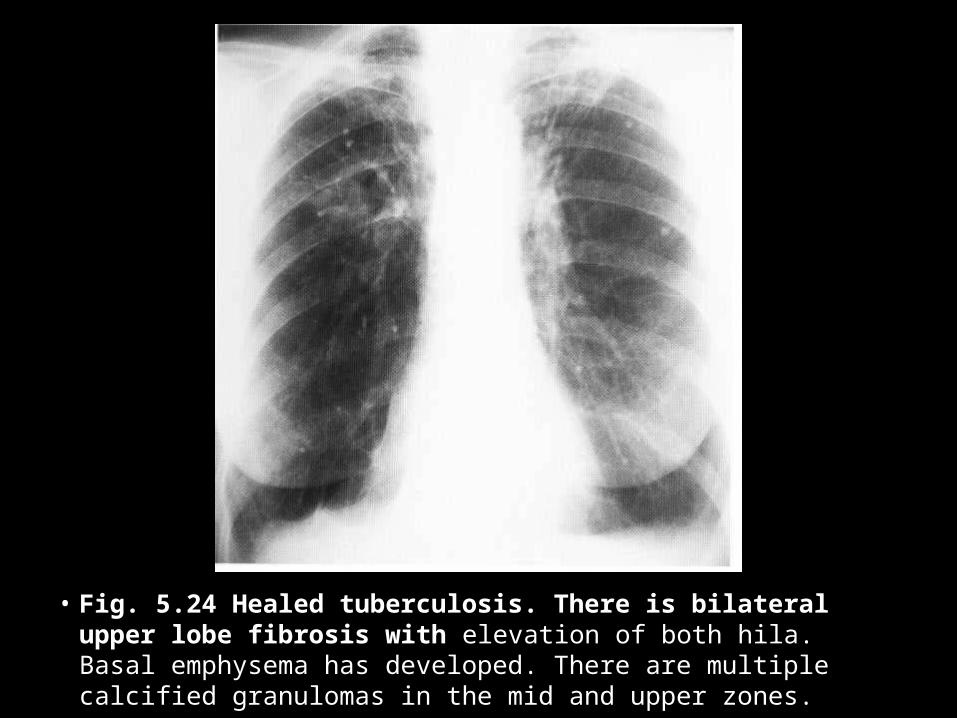
• Fig. 5.24 Healed tuberculosis. There is bilateral upper lobe fibrosis with elevation of both hila. Basal emphysema has developed. There are multiple calcified granulomas in the mid and upper zones.
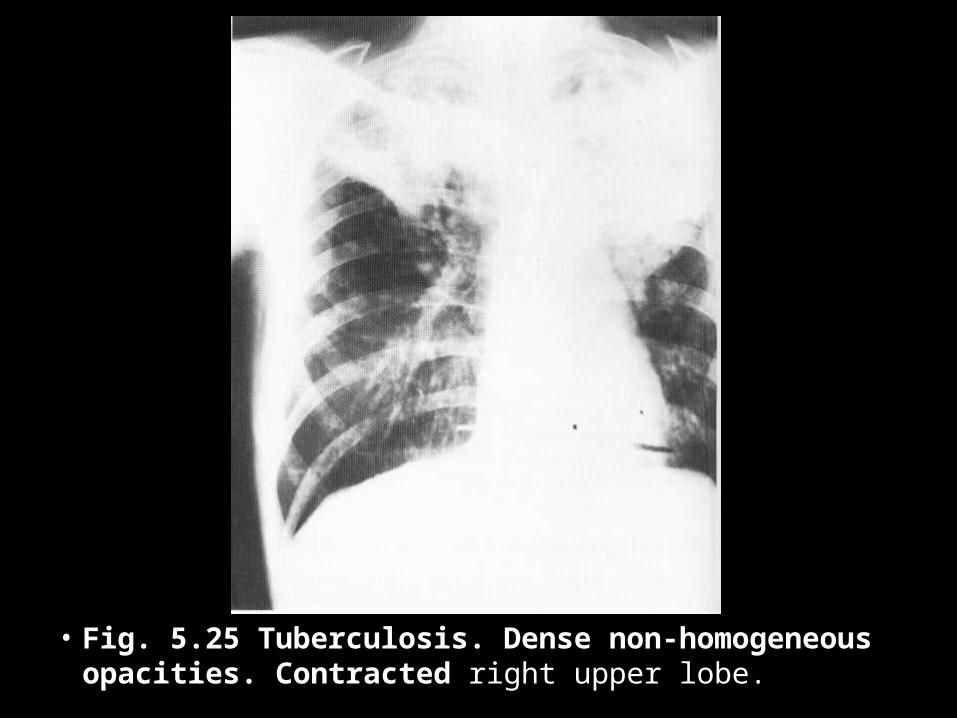
• Fig. 5.25 Tuberculosis. Dense non-homogeneous opacities. Contracted right upper lobe.
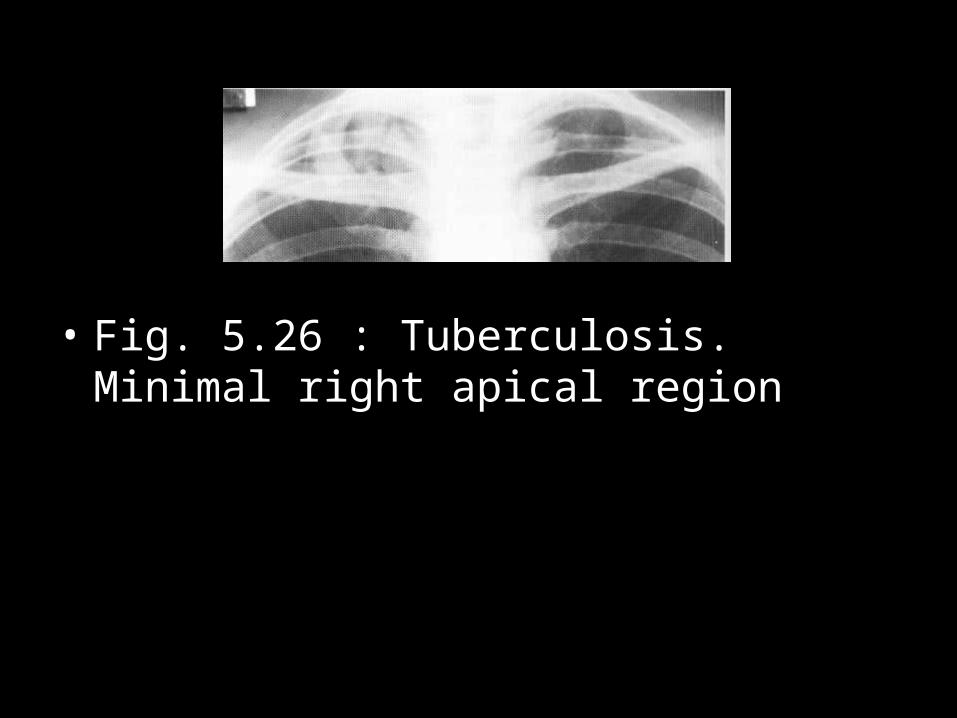
• Fig. 5.26 : Tuberculosis. Minimal right apical region
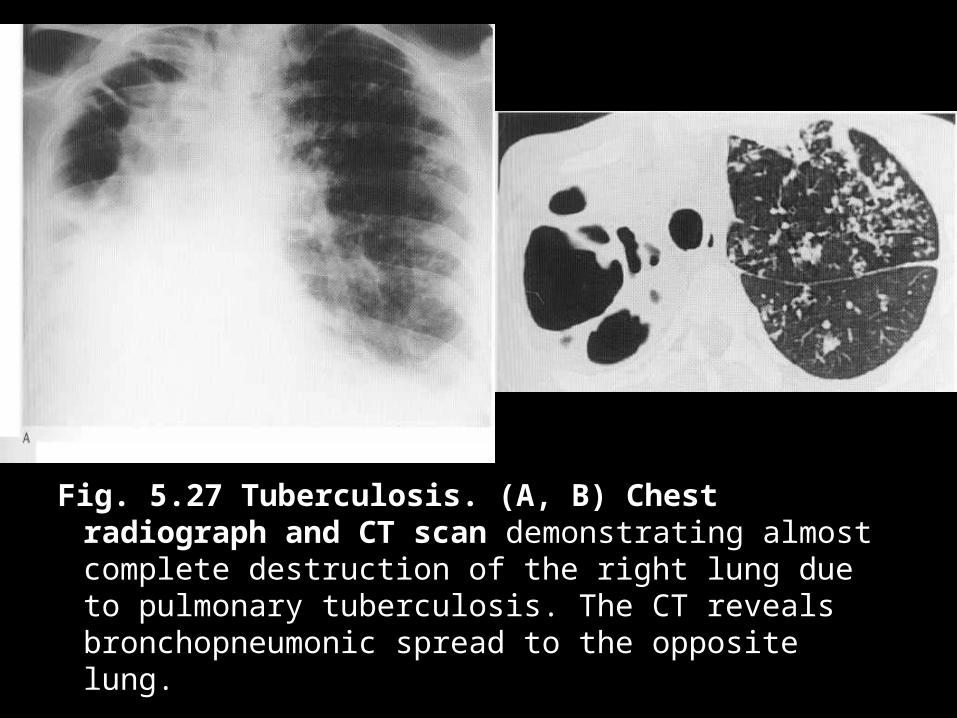
Fig. 5.27 Tuberculosis. (A, B) Chest radiograph and CT scan demonstrating almost complete destruction of the right lung due to pulmonary tuberculosis. The CT reveals bronchopneumonic spread to the opposite lung.
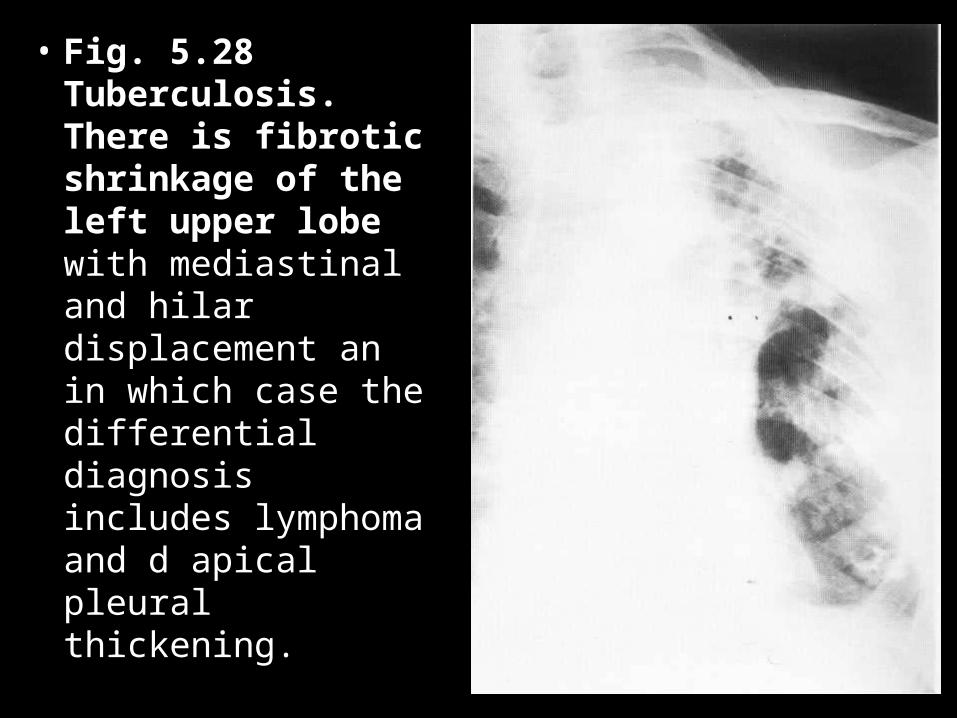
• Fig. 5.28 Tuberculosis. There is fibrotic shrinkage of the left upper lobe with mediastinal and hilar displacement an in which case the differential diagnosis includes lymphoma and d apical pleural thickening.
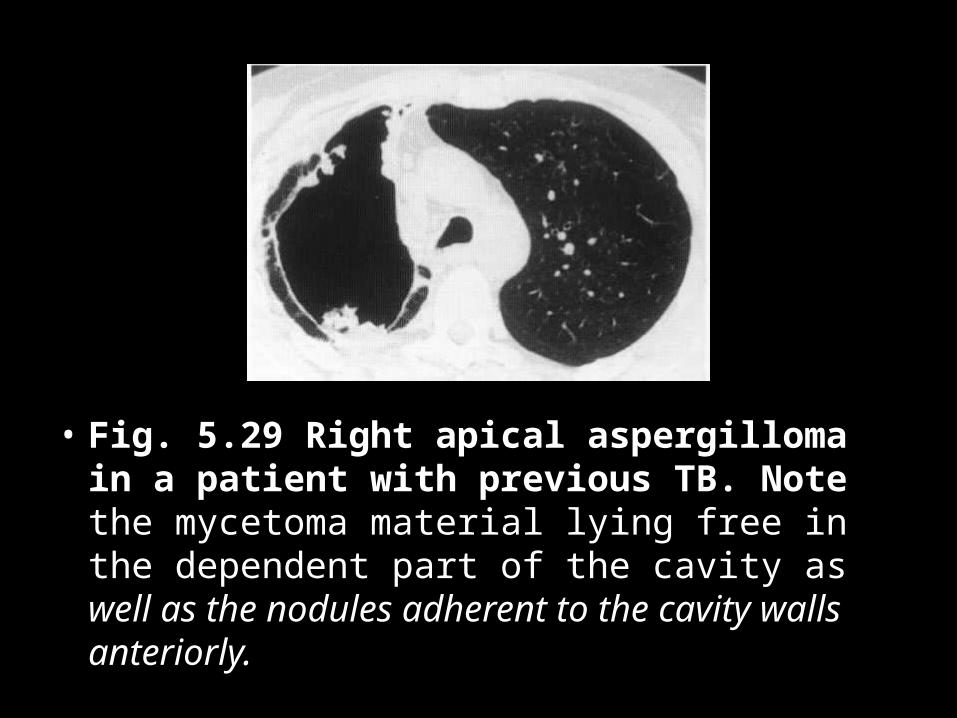
• Fig. 5.29 Right apical aspergilloma in a patient with previous TB. Note the mycetoma material lying free in the dependent part of the cavity as well as the nodules adherent to the cavity walls anteriorly.
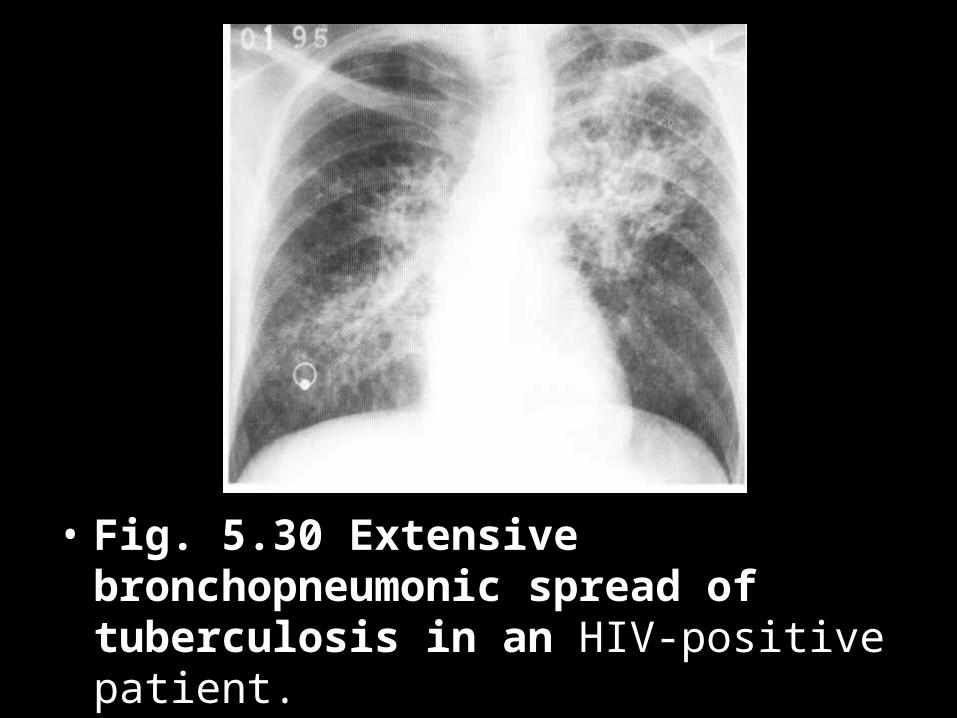
• Fig. 5.30 Extensive bronchopneumonic spread of tuberculosis in an HIV-positive patient.
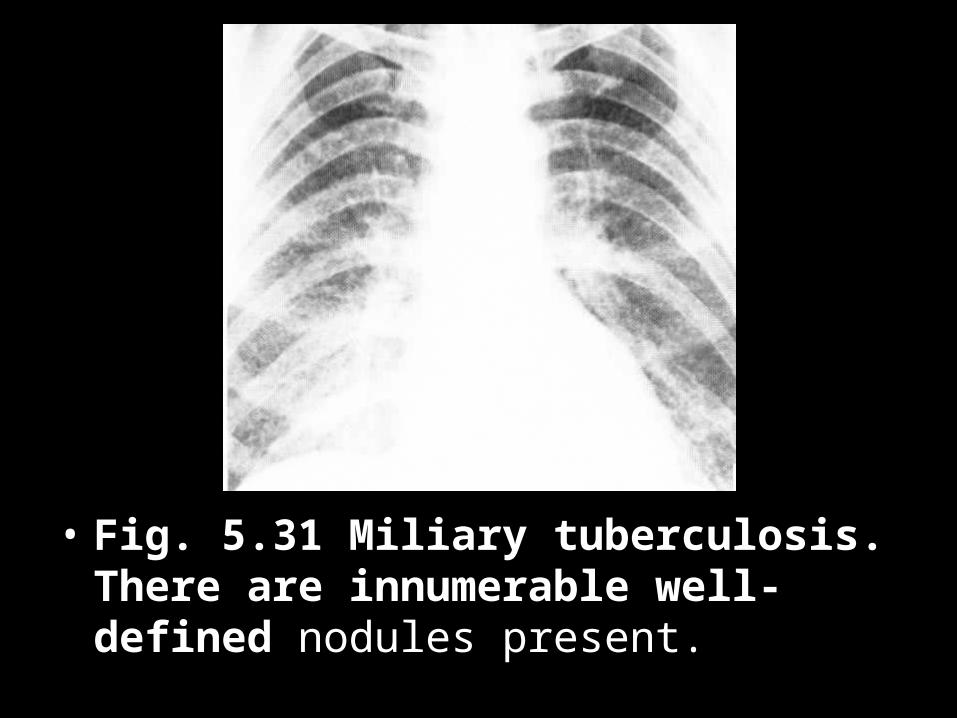
• Fig. 5.31 Miliary tuberculosis. There are innumerable well-defined nodules present.
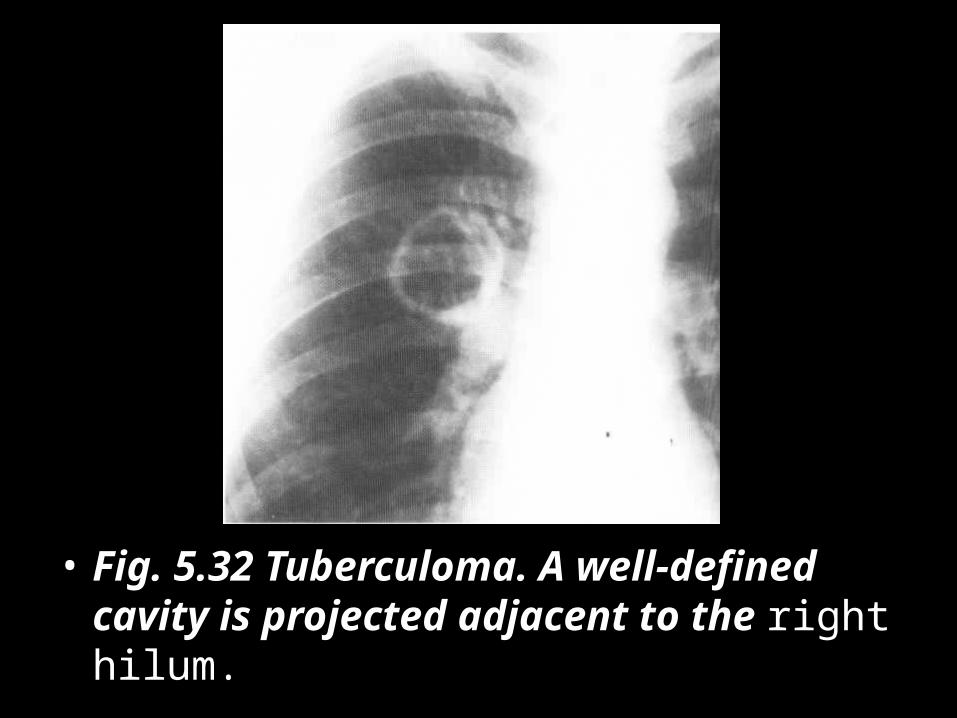
• Fig. 5.32 Tuberculoma. A well-defined cavity is projected adjacent to the right hilum.
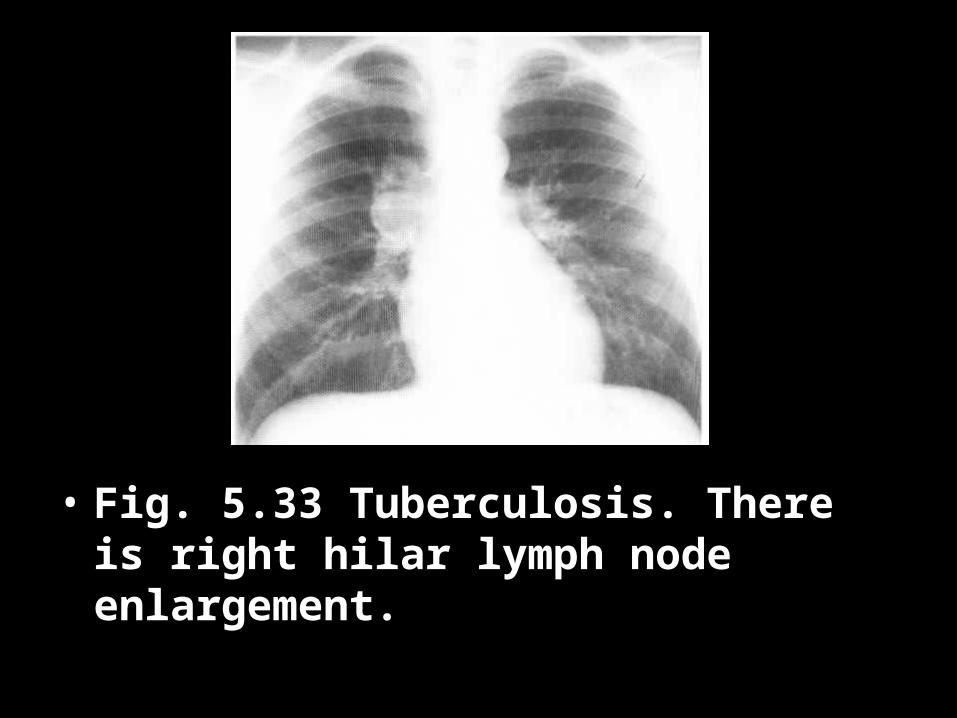
• Fig. 5.33 Tuberculosis. There is right hilar lymph node enlargement.
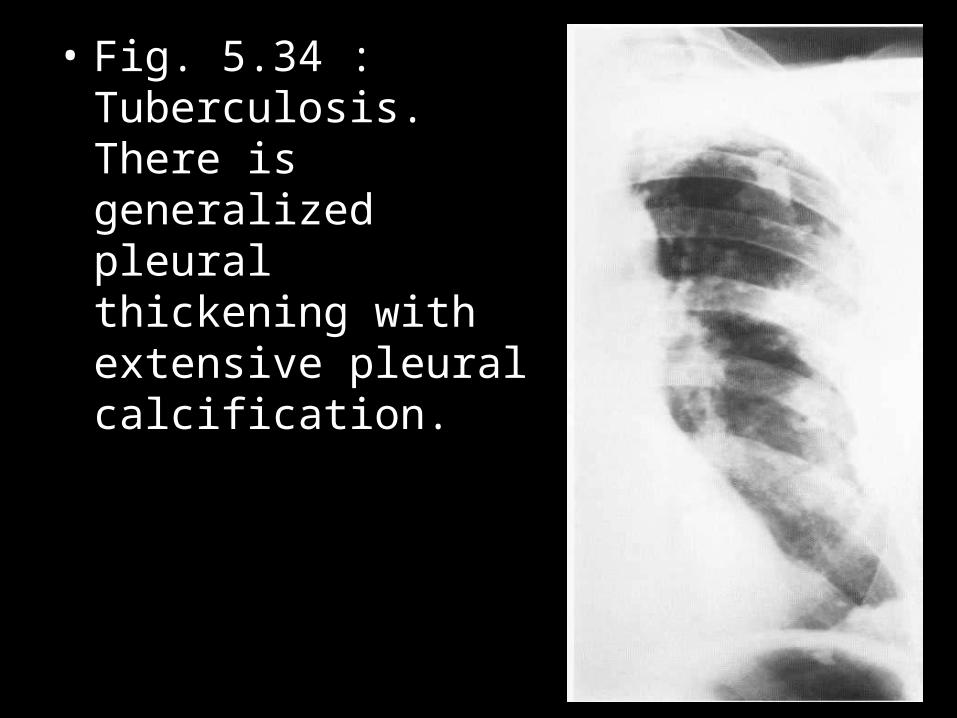
• Fig. 5.34 : Tuberculosis. There is generalized pleural thickening with extensive pleural calcification.
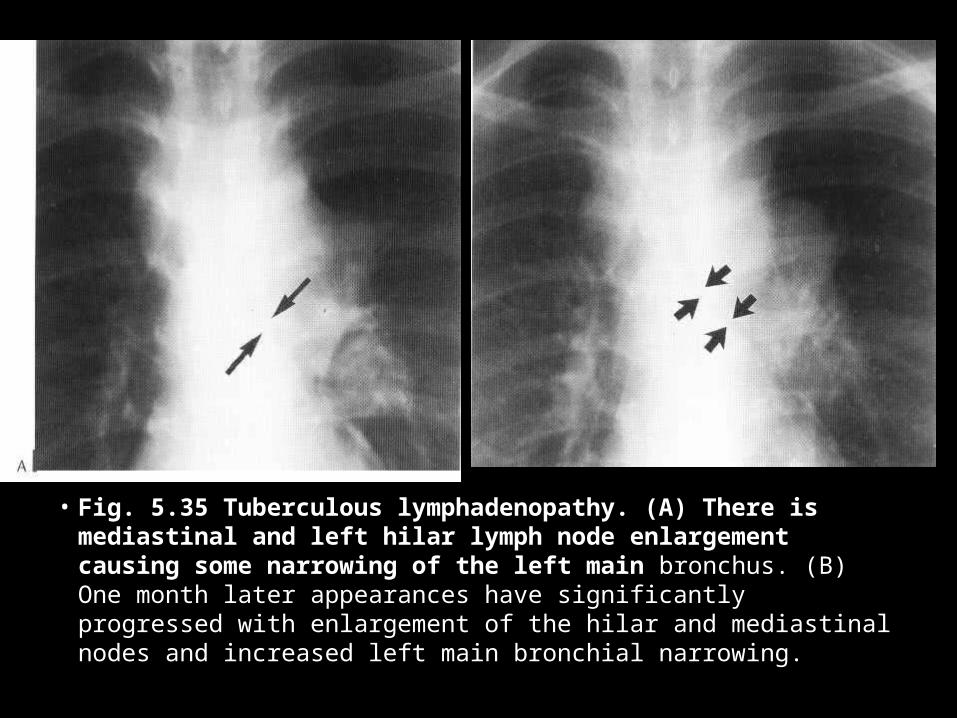
• Fig. 5.35 Tuberculous lymphadenopathy. (A) There is mediastinal and left hilar lymph node enlargement causing some narrowing of the left main bronchus. (B) One month later appearances have significantly progressed with enlargement of the hilar and mediastinal nodes and increased left main bronchial narrowing.
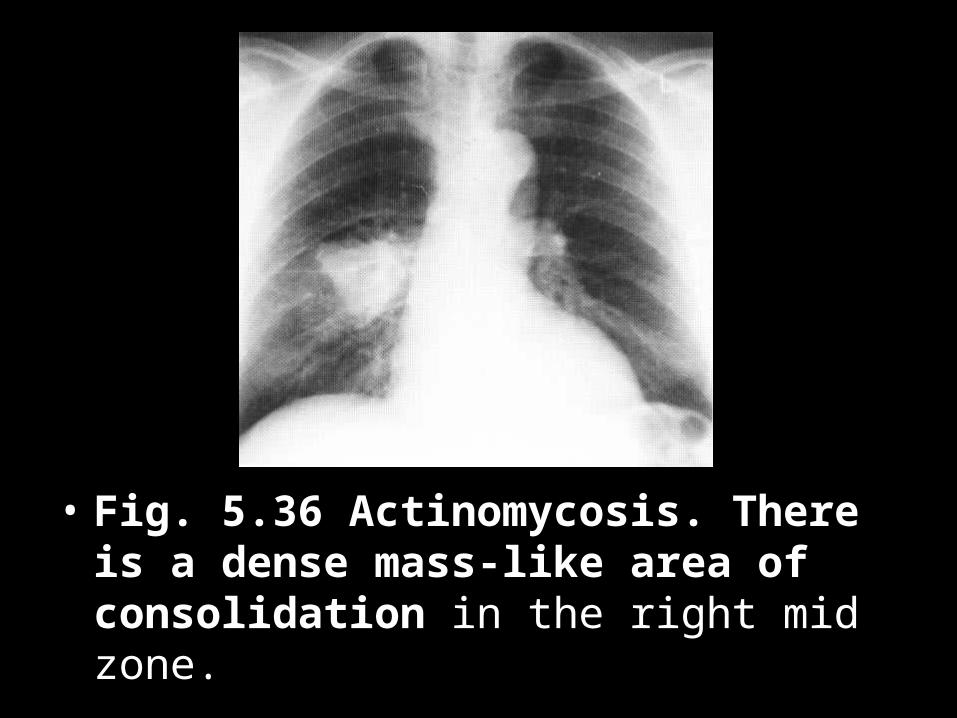
• Fig. 5.36 Actinomycosis. There is a dense mass-like area of consolidation in the right mid zone.
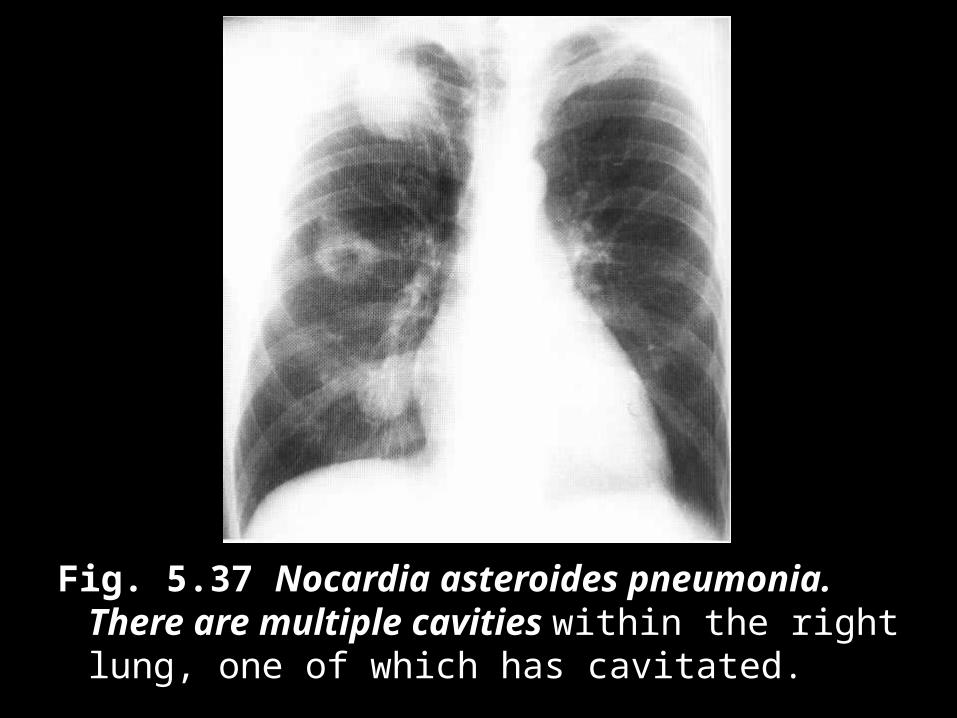
Fig. 5.37 Nocardia asteroides pneumonia. There are multiple cavities within the right lung, one of which has cavitated.
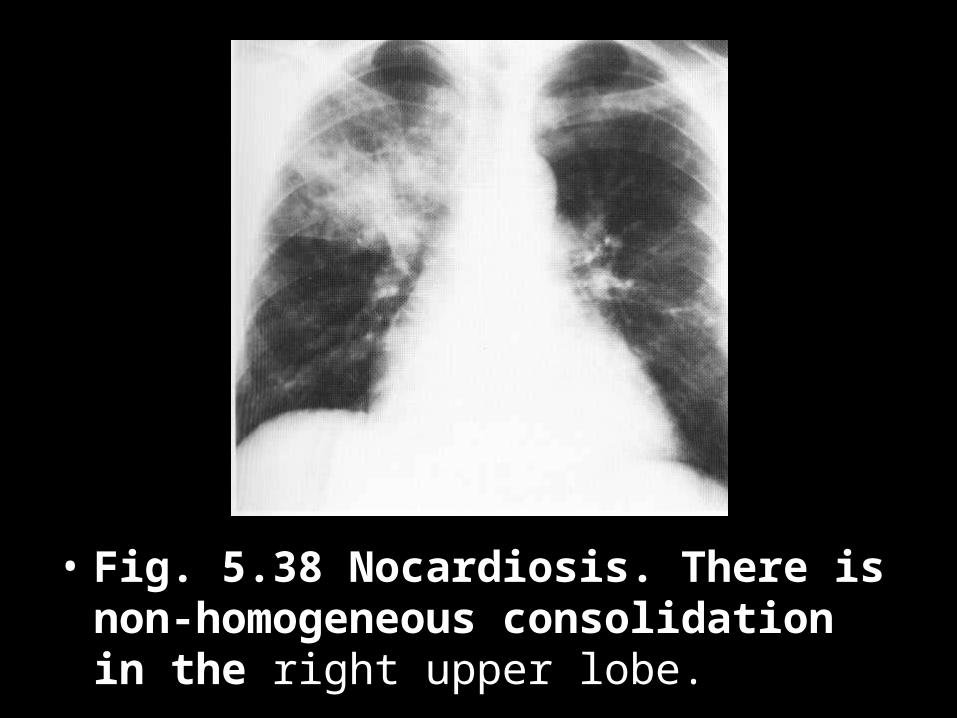
• Fig. 5.38 Nocardiosis. There is non-homogeneous consolidation in the right upper lobe.
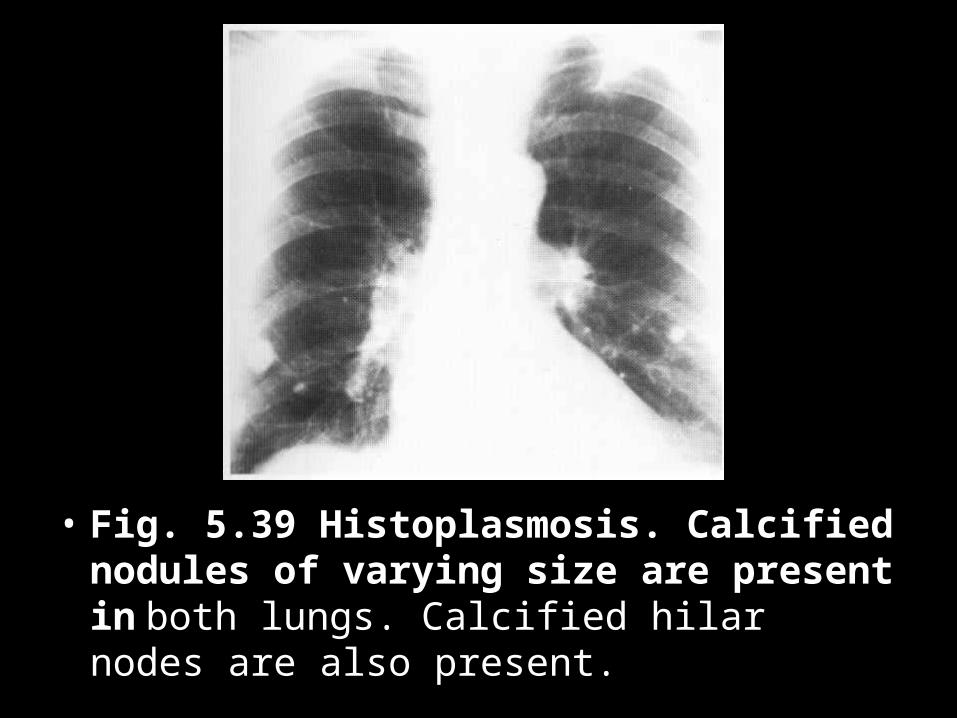
• Fig. 5.39 Histoplasmosis. Calcified nodules of varying size are present in both lungs. Calcified hilar nodes are also present.
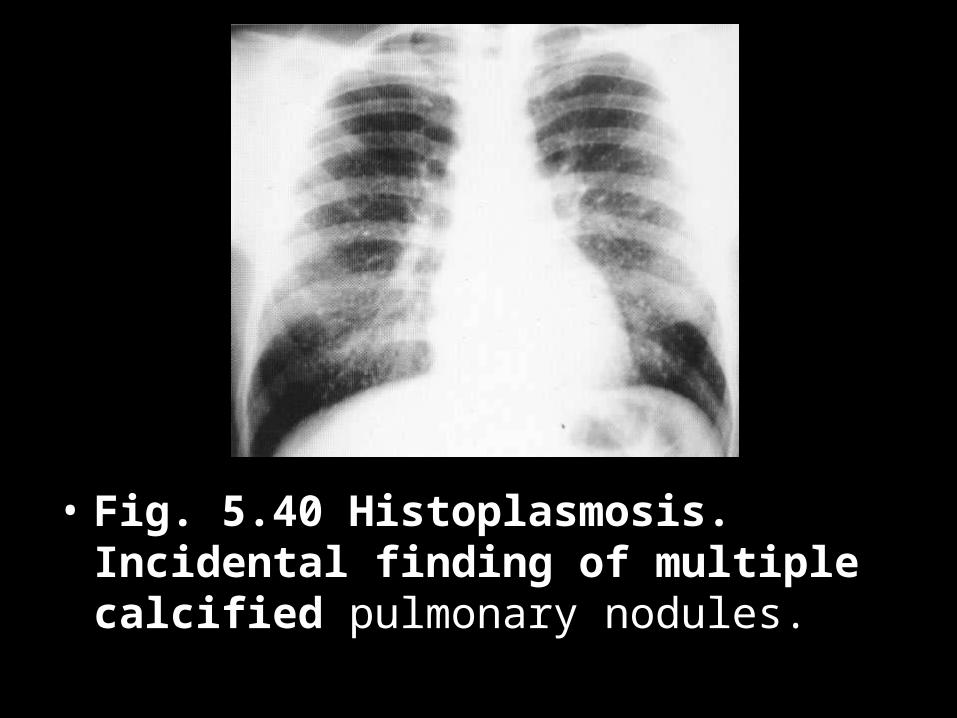
• Fig. 5.40 Histoplasmosis. Incidental finding of multiple calcified pulmonary nodules.
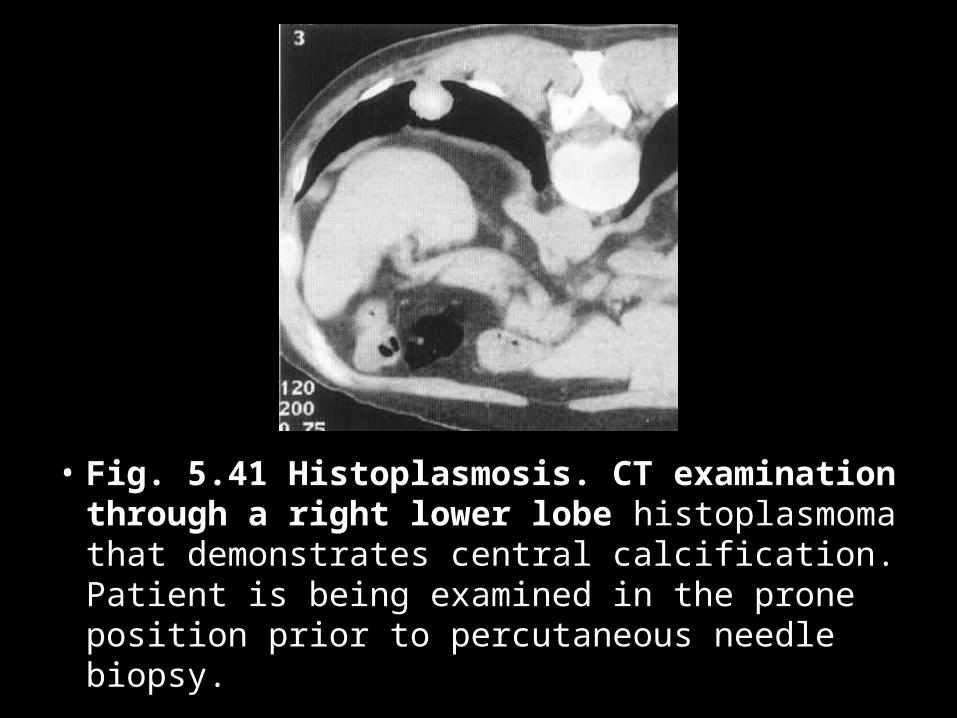
• Fig. 5.41 Histoplasmosis. CT examination through a right lower lobe histoplasmoma that demonstrates central calcification. Patient is being examined in the prone position prior to percutaneous needle biopsy.
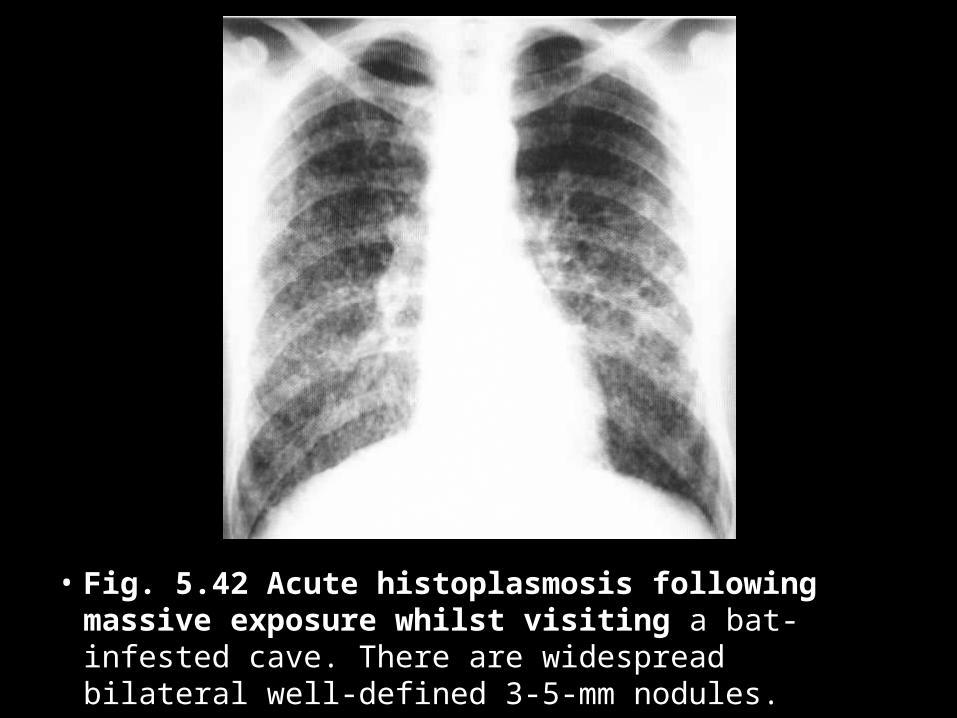
• Fig. 5.42 Acute histoplasmosis following massive exposure whilst visiting a bat-infested cave. There are widespread bilateral well-defined 3-5-mm nodules.
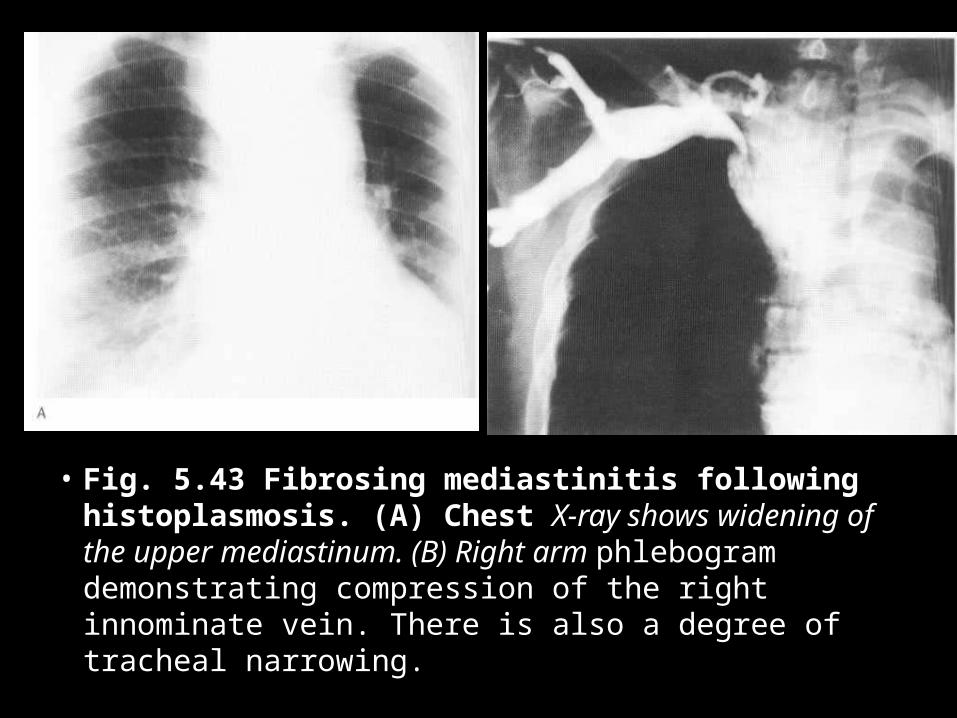
• Fig. 5.43 Fibrosing mediastinitis following histoplasmosis. (A) Chest X-ray shows widening of the upper mediastinum. (B) Right arm phlebogram demonstrating compression of the right innominate vein. There is also a degree of tracheal narrowing.
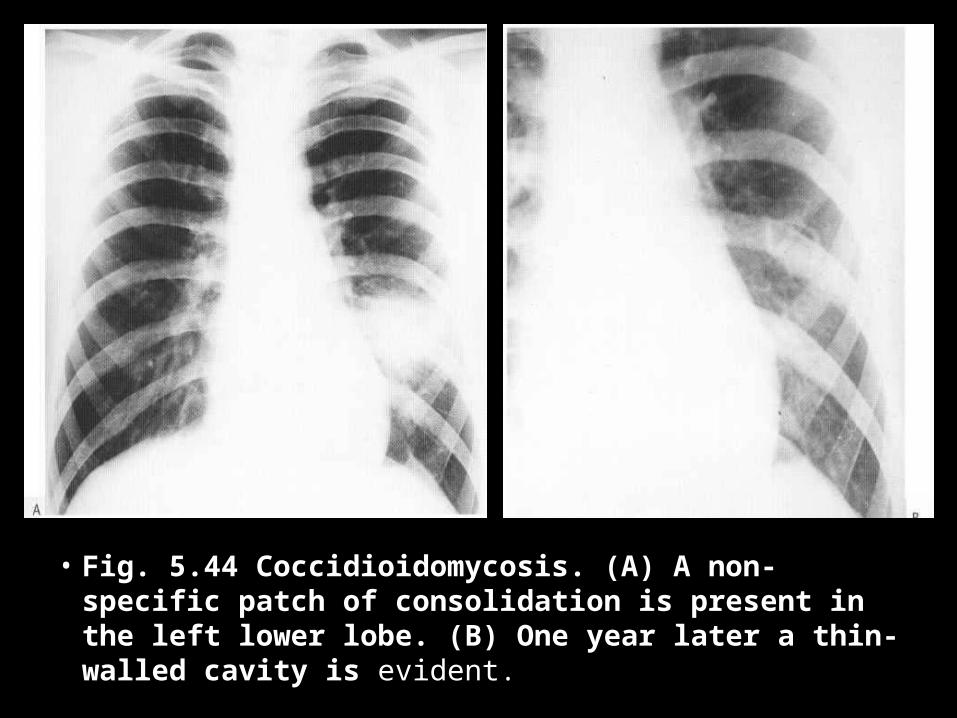
• Fig. 5.44 Coccidioidomycosis. (A) A non-specific patch of consolidation is present in the left lower lobe. (B) One year later a thin-walled cavity is evident.
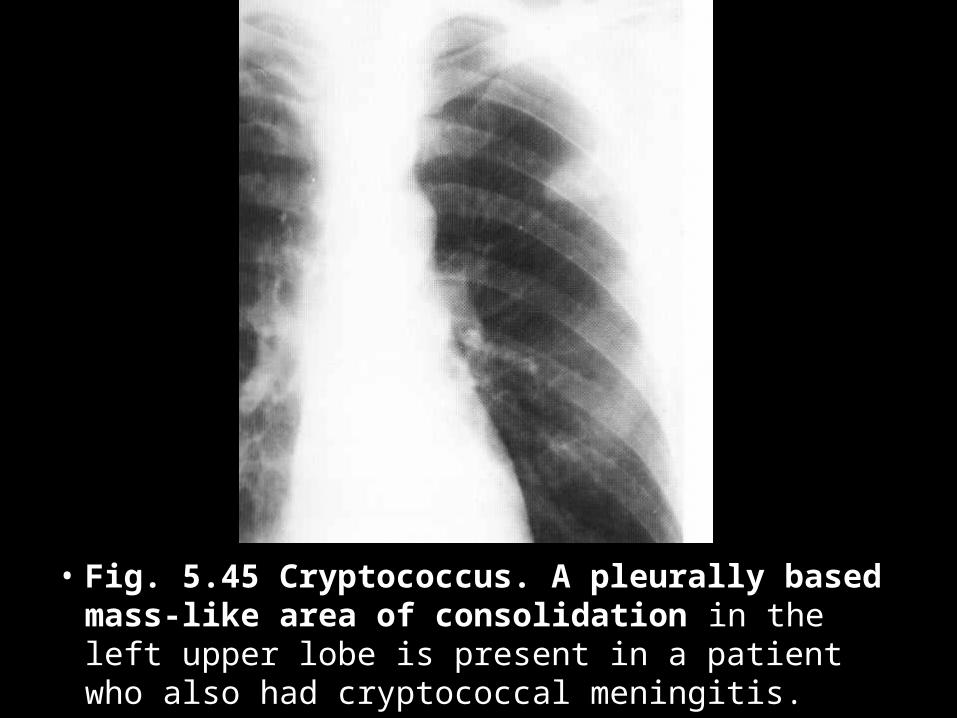
• Fig. 5.45 Cryptococcus. A pleurally based mass-like area of consolidation in the left upper lobe is present in a patient who also had cryptococcal meningitis.
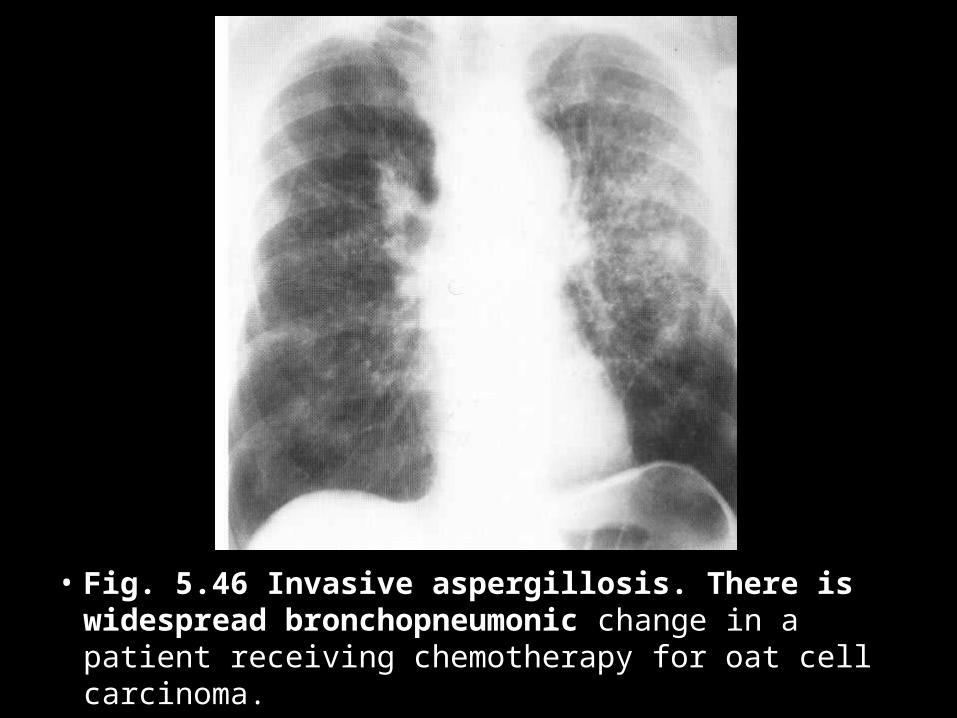
• Fig. 5.46 Invasive aspergillosis. There is widespread bronchopneumonic change in a patient receiving chemotherapy for oat cell carcinoma.
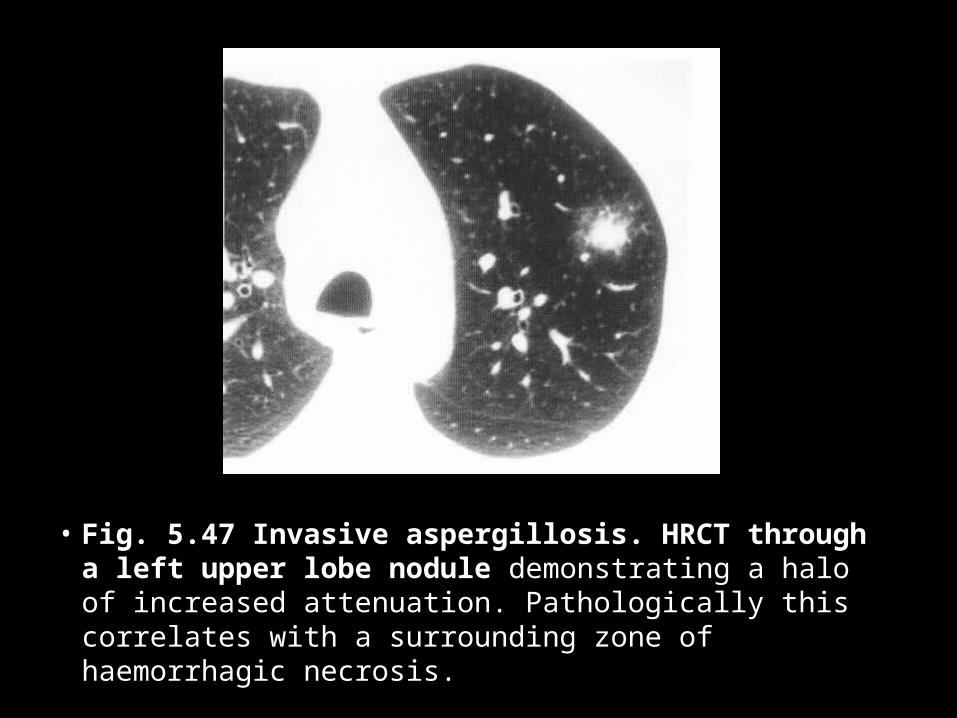
• Fig. 5.47 Invasive aspergillosis. HRCT through a left upper lobe nodule demonstrating a halo of increased attenuation. Pathologically this correlates with a surrounding zone of haemorrhagic necrosis.
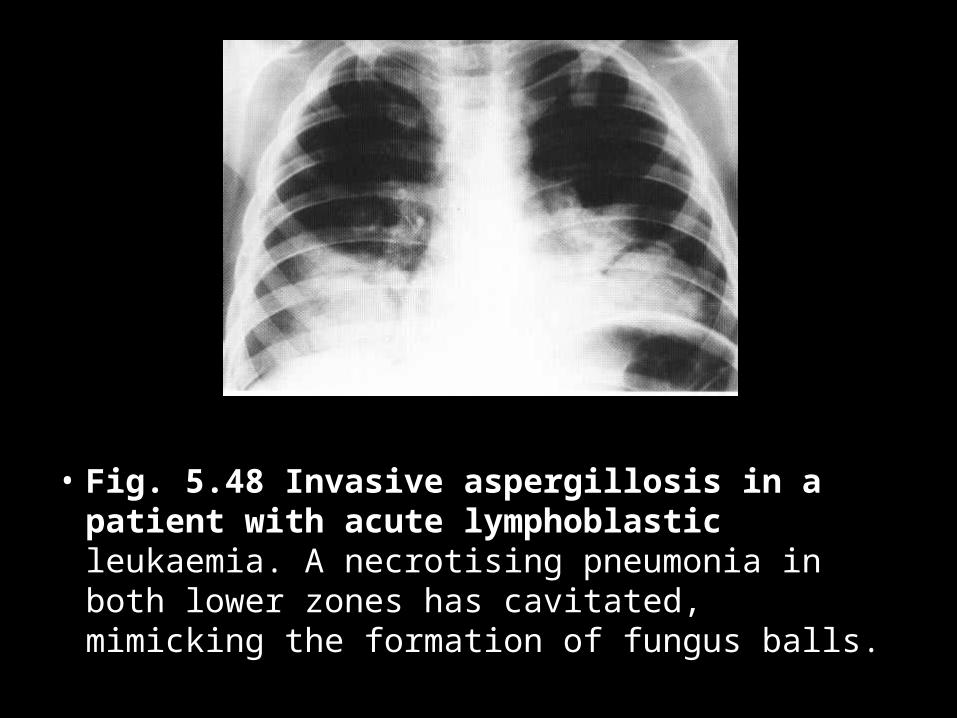
• Fig. 5.48 Invasive aspergillosis in a patient with acute lymphoblastic leukaemia. A necrotising pneumonia in both lower zones has cavitated, mimicking the formation of fungus balls.
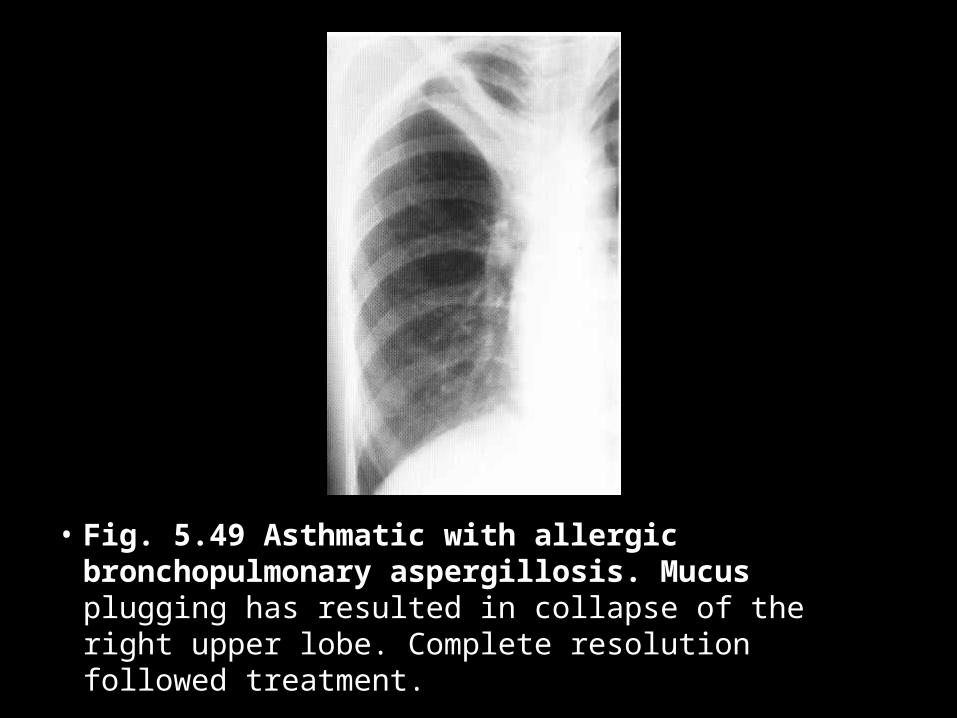
• Fig. 5.49 Asthmatic with allergic bronchopulmonary aspergillosis. Mucus plugging has resulted in collapse of the right upper lobe. Complete resolution followed treatment.
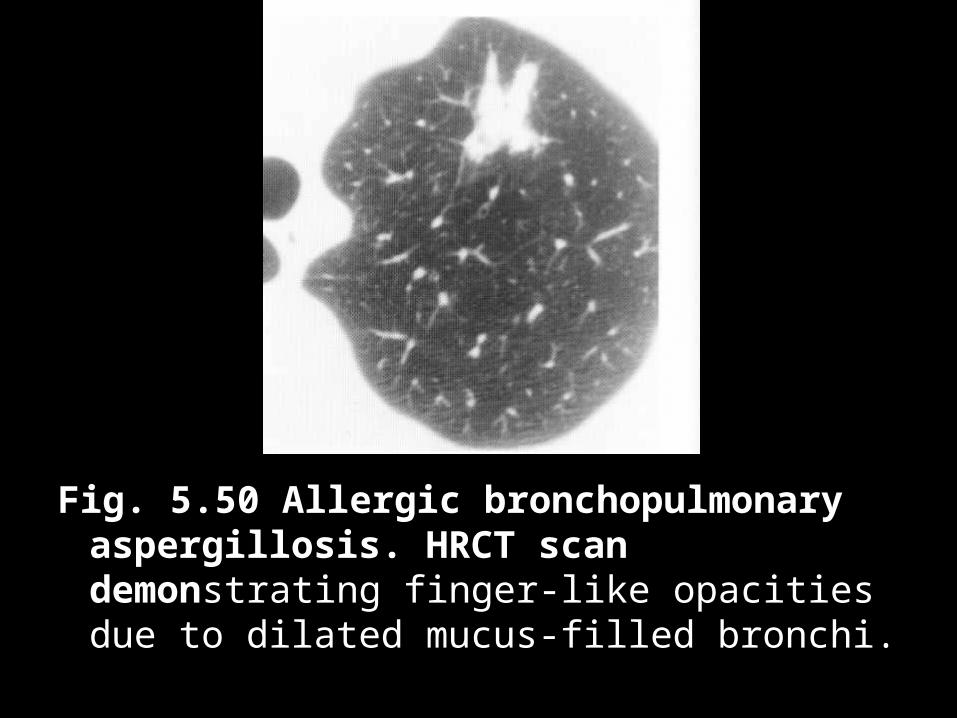
Fig. 5.50 Allergic bronchopulmonary aspergillosis. HRCT scan demonstrating finger-like opacities due to dilated mucus-filled bronchi.
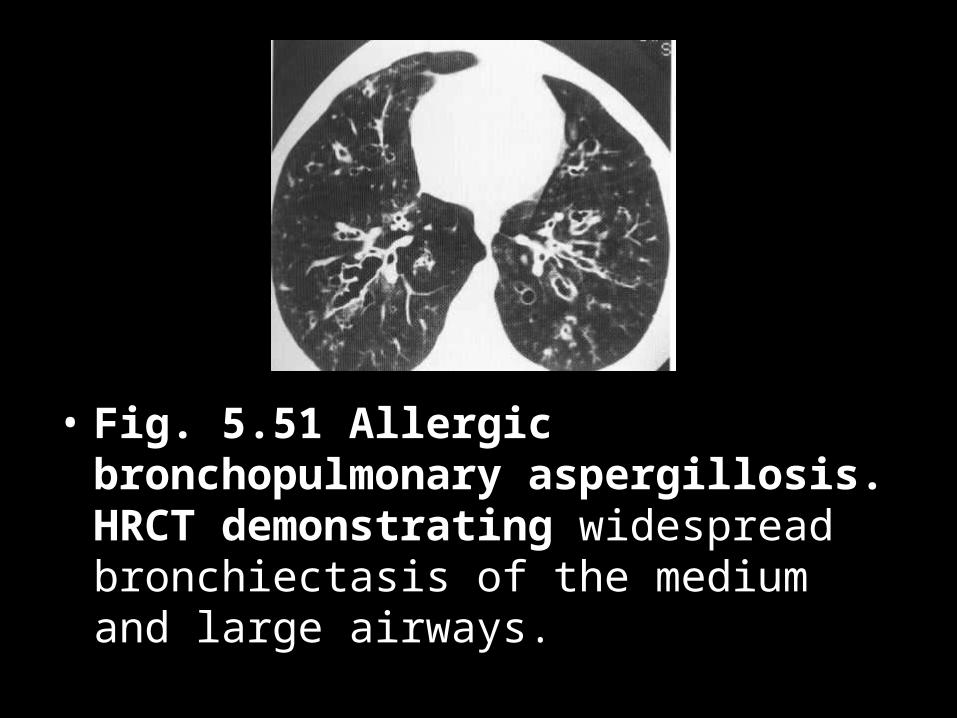
• Fig. 5.51 Allergic bronchopulmonary aspergillosis. HRCT demonstrating widespread bronchiectasis of the medium and large airways.
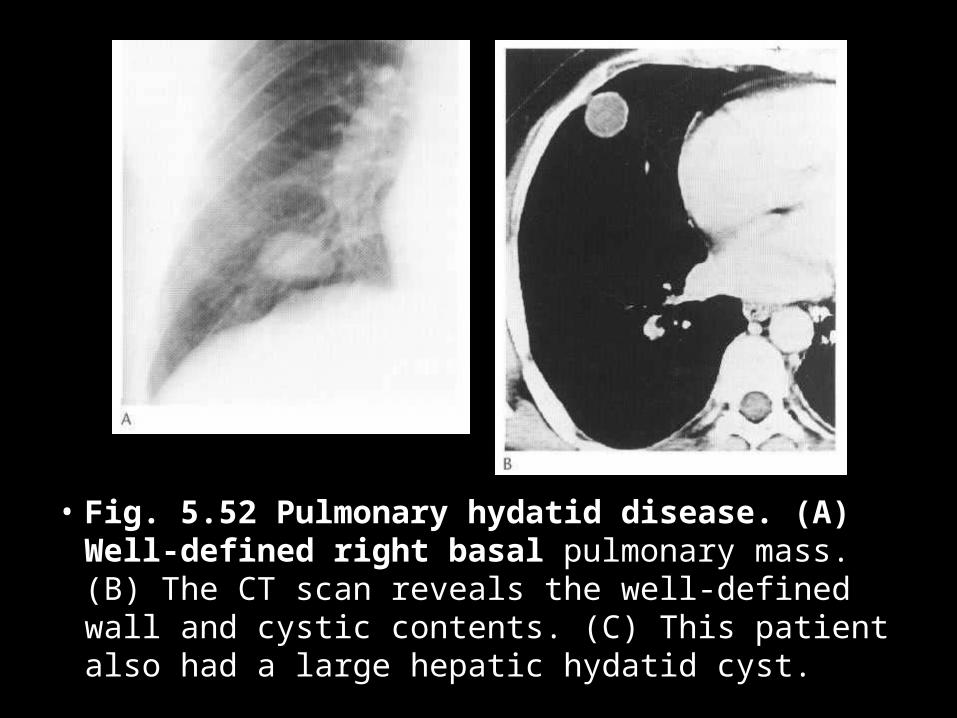
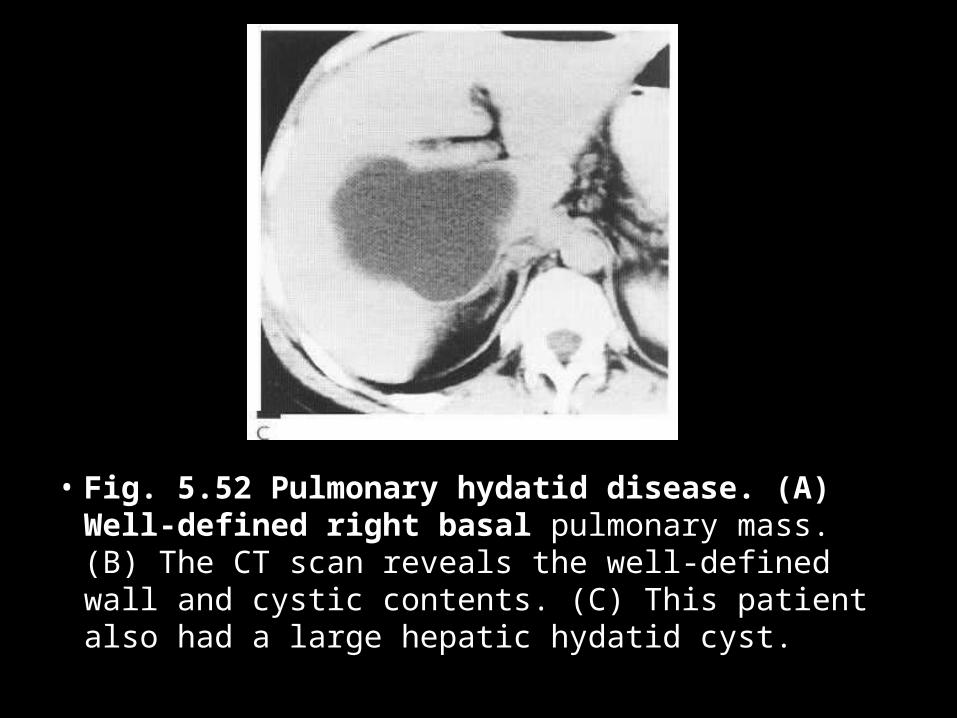
• Fig. 5.52 Pulmonary hydatid disease. (A) Well-defined right basal pulmonary mass. (B) The CT scan reveals the well-defined wall and cystic contents. (C) This patient also had a large hepatic hydatid cyst.
• Fig. 5.52 Pulmonary hydatid disease. (A) Well-defined right basal pulmonary mass. (B) The CT scan reveals the well-defined wall and cystic contents. (C) This patient also had a large hepatic hydatid cyst.
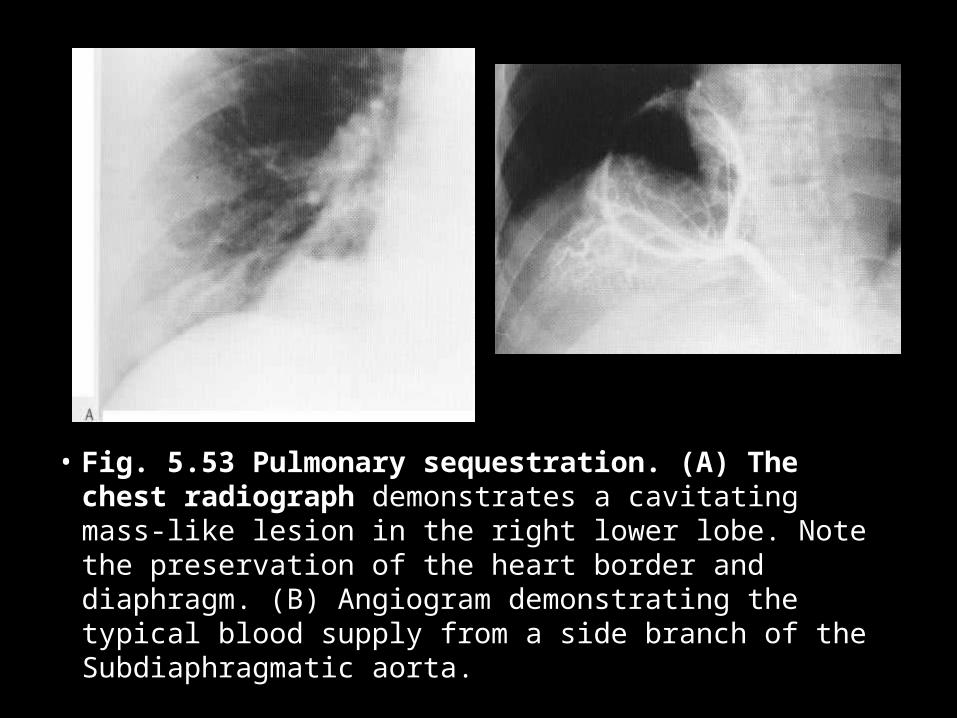
• Fig. 5.53 Pulmonary sequestration. (A) The chest radiograph demonstrates a cavitating mass-like lesion in the right lower lobe. Note the preservation of the heart border and diaphragm. (B) Angiogram demonstrating the typical blood supply from a side branch of the Subdiaphragmatic aorta.
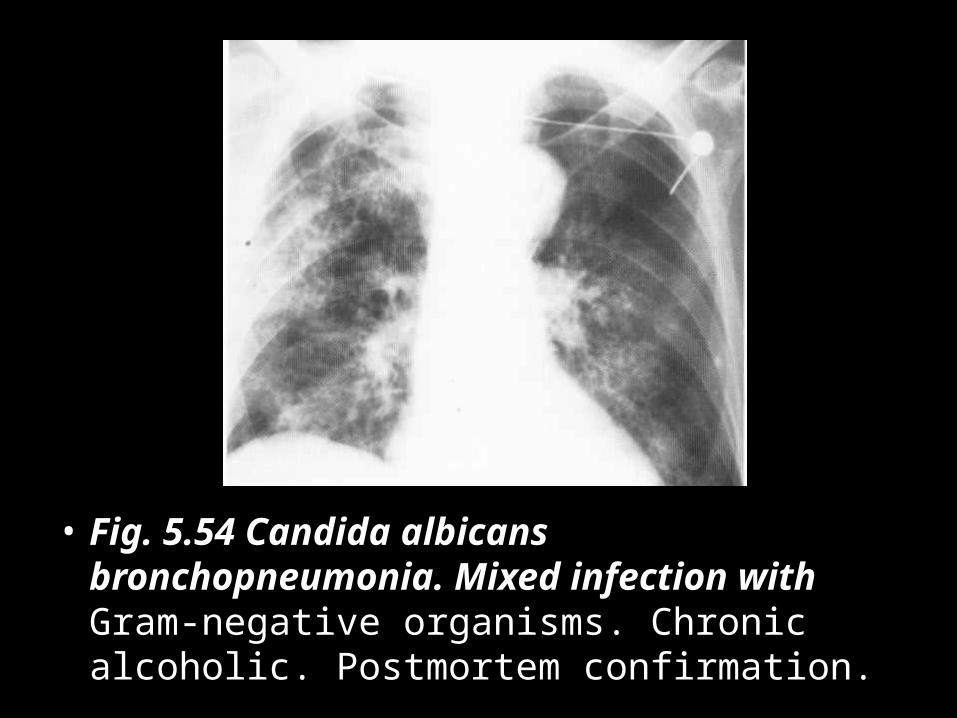
• Fig. 5.54 Candida albicans bronchopneumonia. Mixed infection with Gram-negative organisms. Chronic alcoholic. Postmortem confirmation.
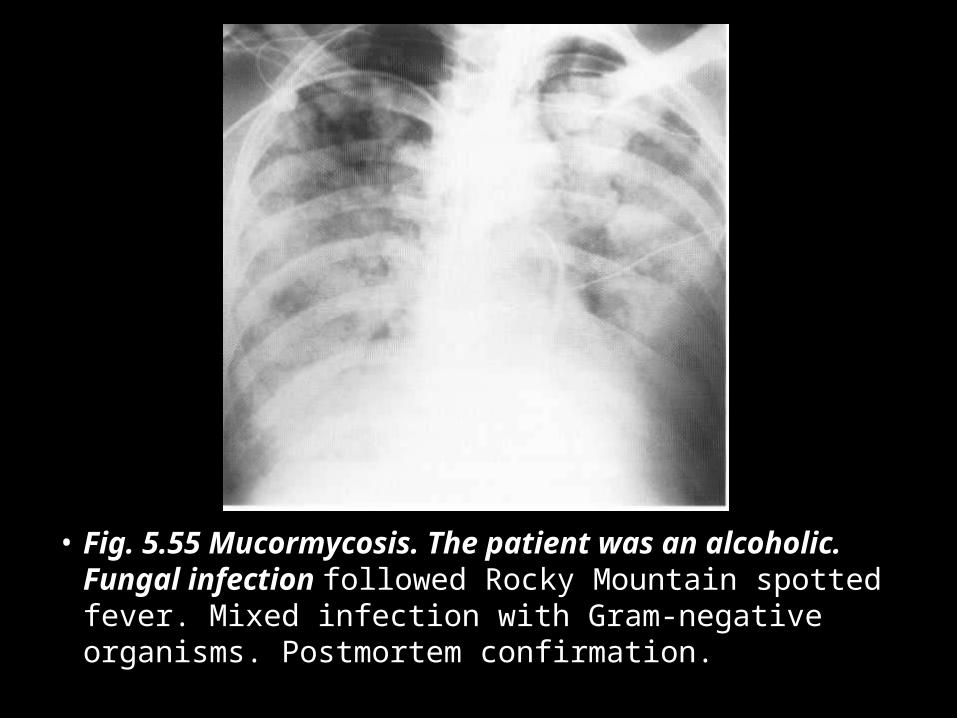
• Fig. 5.55 Mucormycosis. The patient was an alcoholic. Fungal infection followed Rocky Mountain spotted fever. Mixed infection with Gram-negative organisms. Postmortem confirmation.
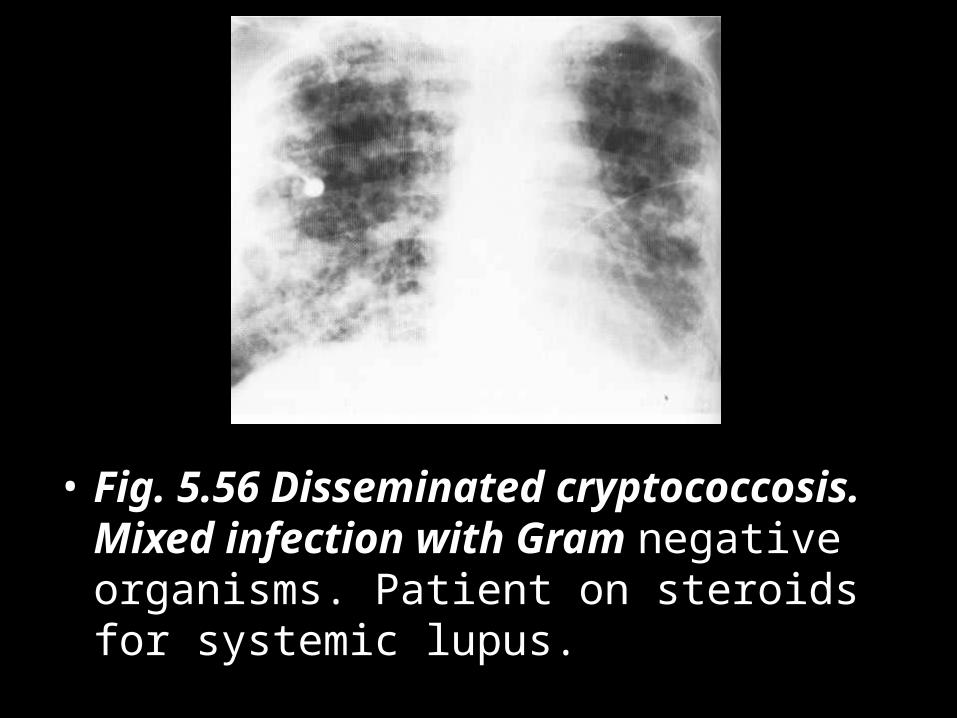
• Fig. 5.56 Disseminated cryptococcosis. Mixed infection with Gram negative organisms. Patient on steroids for systemic lupus.
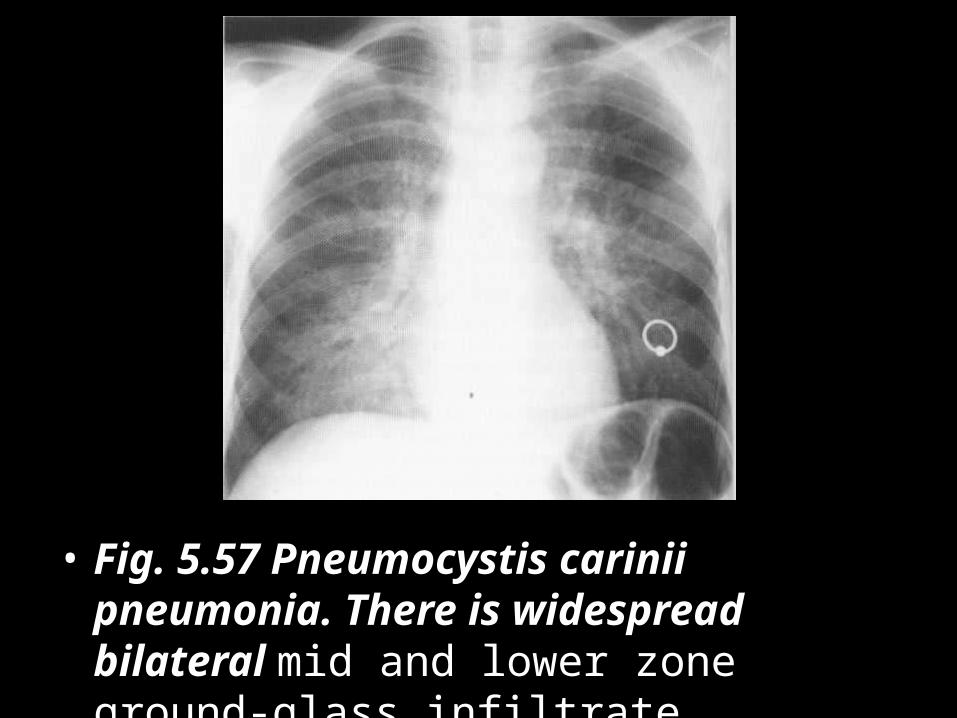
• Fig. 5.57 Pneumocystis carinii pneumonia. There is widespread bilateral mid and lower zone ground-glass infiltrate.
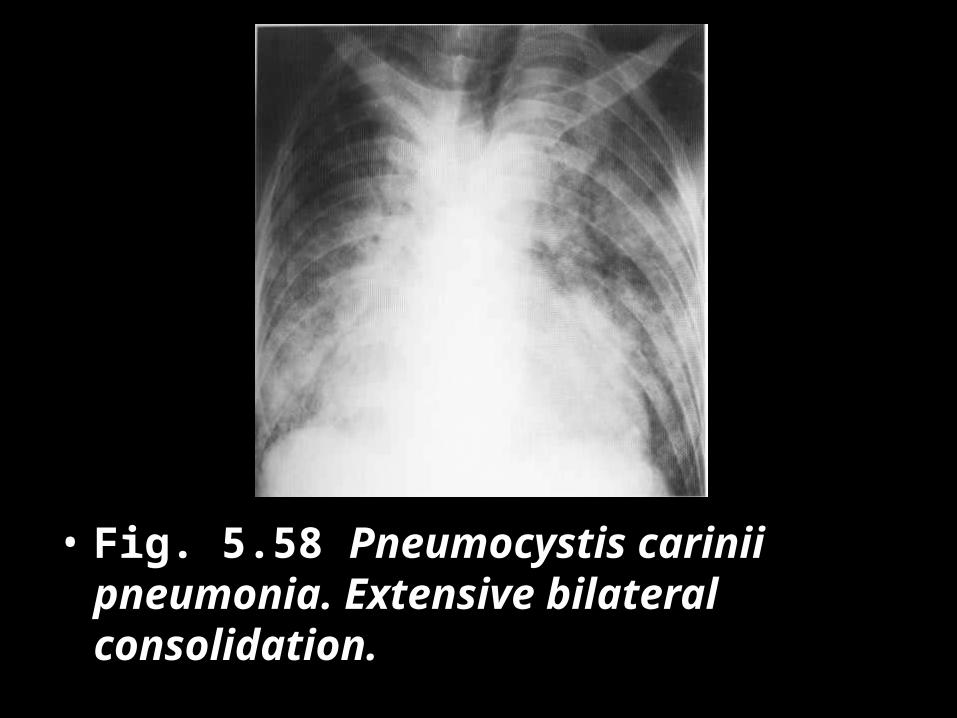
• Fig. 5.58 Pneumocystis carinii pneumonia. Extensive bilateral consolidation.
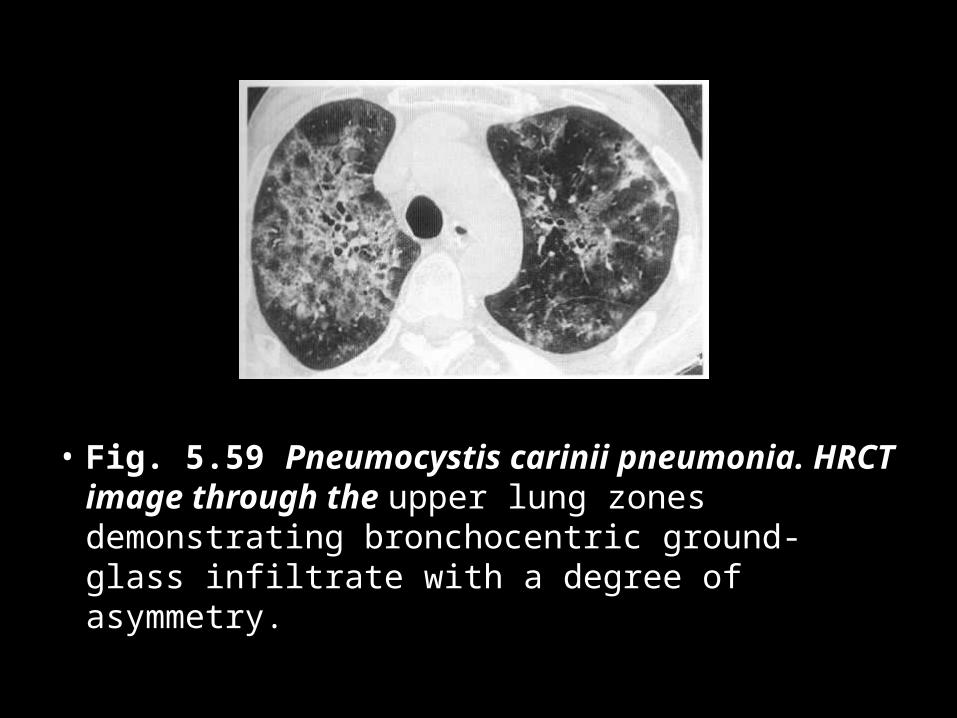
• Fig. 5.59 Pneumocystis carinii pneumonia. HRCT image through the upper lung zones demonstrating bronchocentric ground-glass infiltrate with a degree of asymmetry.
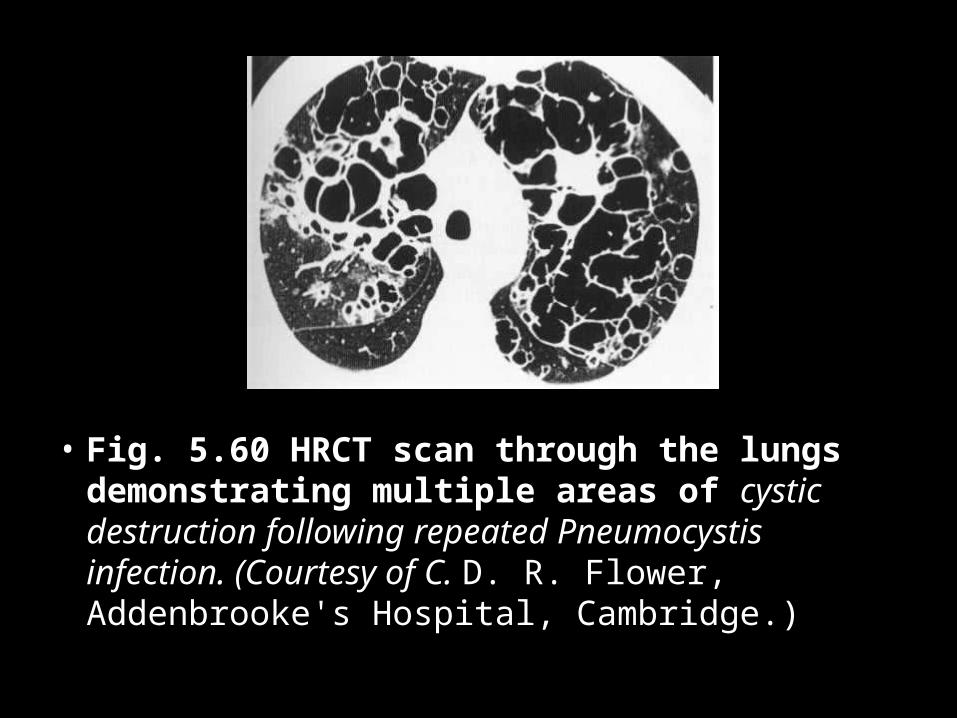
• Fig. 5.60 HRCT scan through the lungs demonstrating multiple areas of cystic destruction following repeated Pneumocystis infection. (Courtesy of C. D. R. Flower, Addenbrooke's Hospital, Cambridge.)
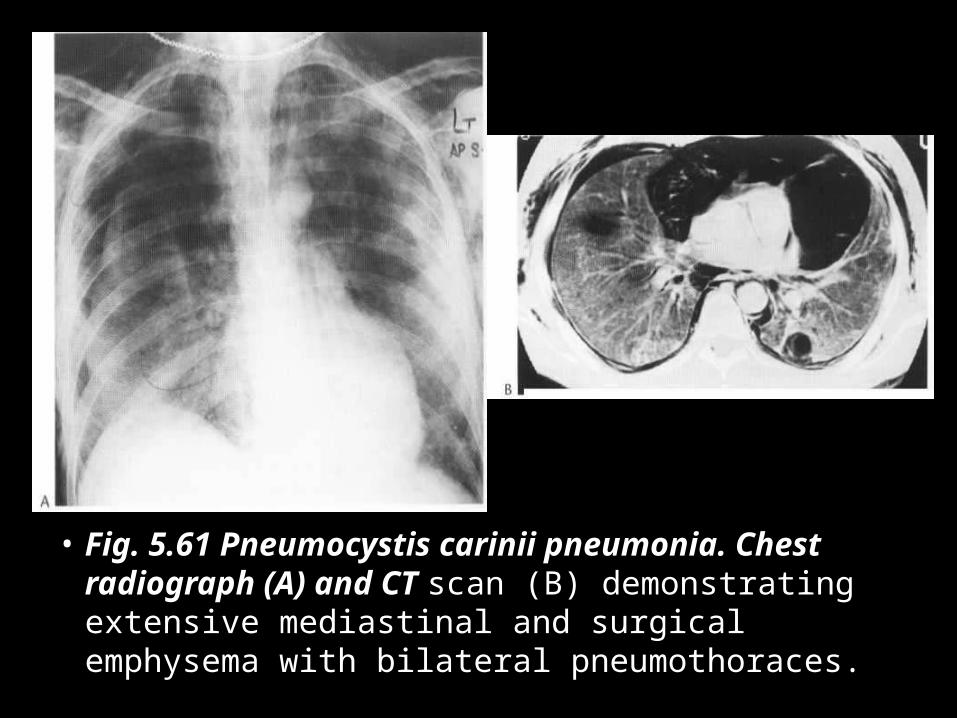
• Fig. 5.61 Pneumocystis carinii pneumonia. Chest radiograph (A) and CT scan (B) demonstrating extensive mediastinal and surgical emphysema with bilateral pneumothoraces.
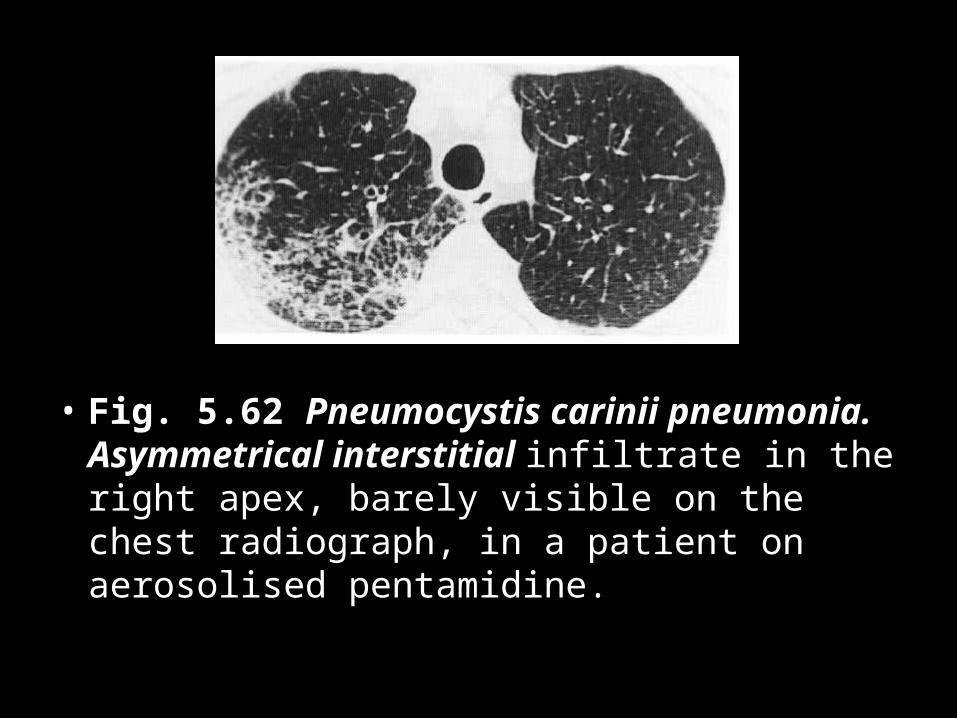
• Fig. 5.62 Pneumocystis carinii pneumonia. Asymmetrical interstitial infiltrate in the right apex, barely visible on the chest radiograph, in a patient on aerosolised pentamidine.
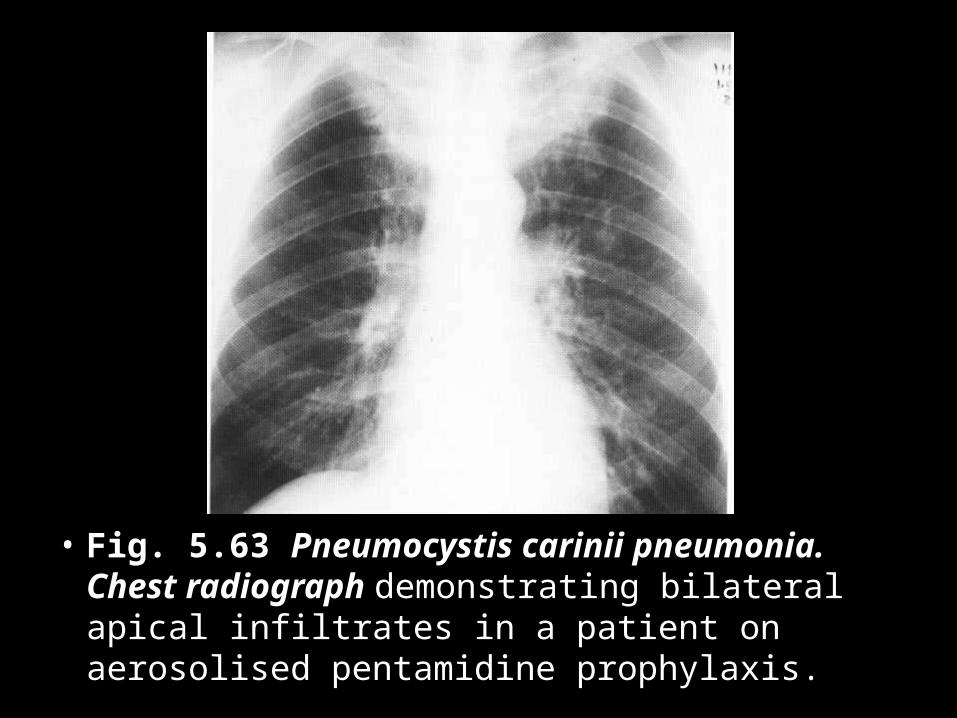
• Fig. 5.63 Pneumocystis carinii pneumonia. Chest radiograph demonstrating bilateral apical infiltrates in a patient on aerosolised pentamidine prophylaxis.
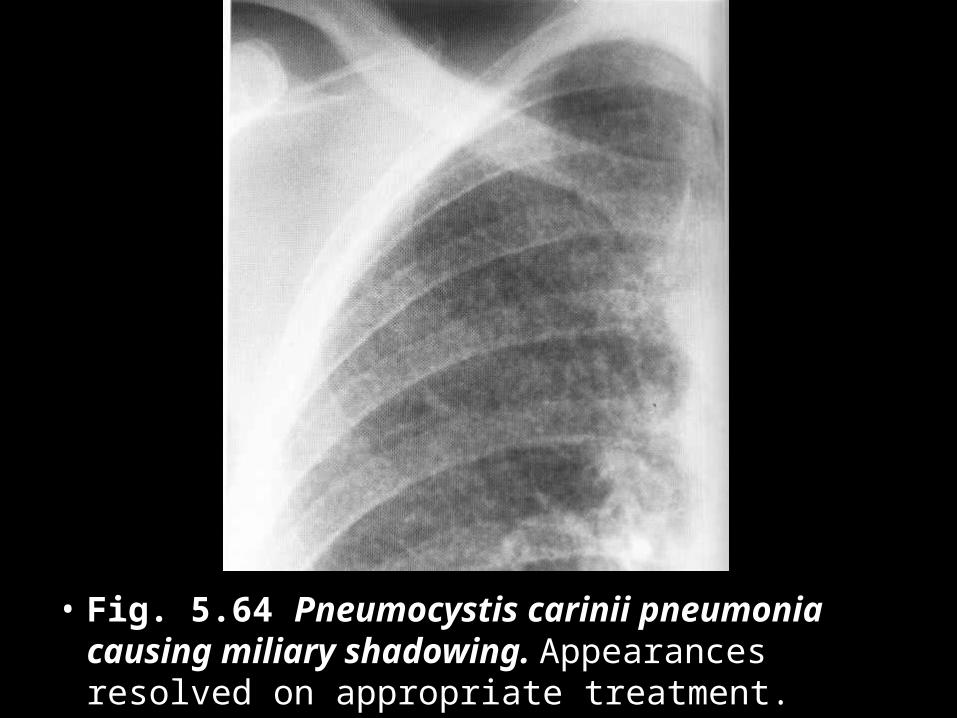
• Fig. 5.64 Pneumocystis carinii pneumonia causing miliary shadowing. Appearances resolved on appropriate treatment.
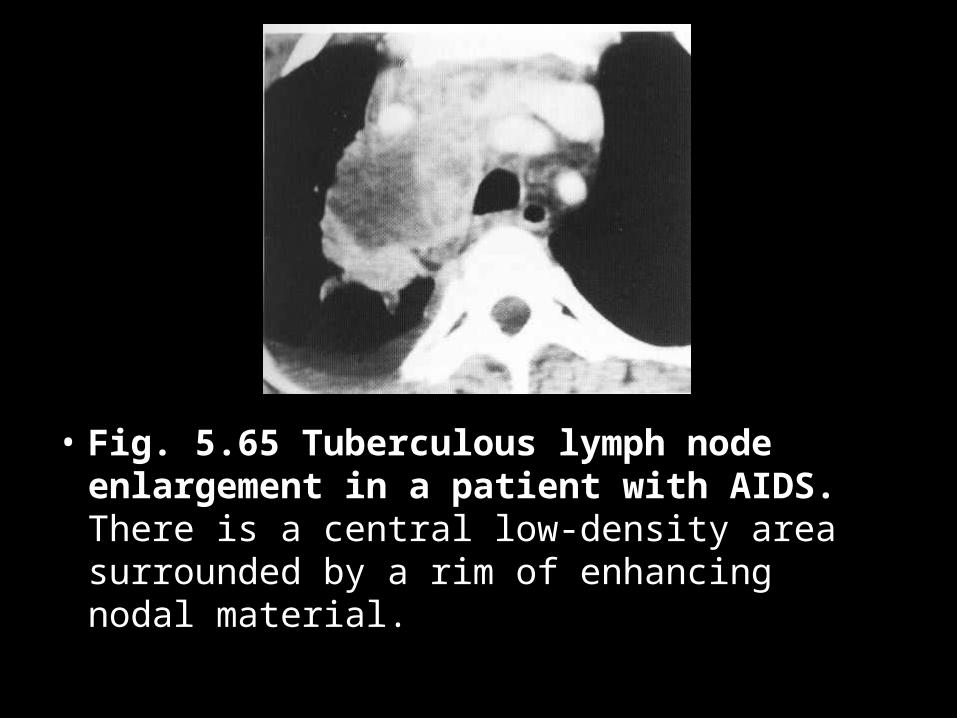
• Fig. 5.65 Tuberculous lymph node enlargement in a patient with AIDS. There is a central low-density area surrounded by a rim of enhancing nodal material.
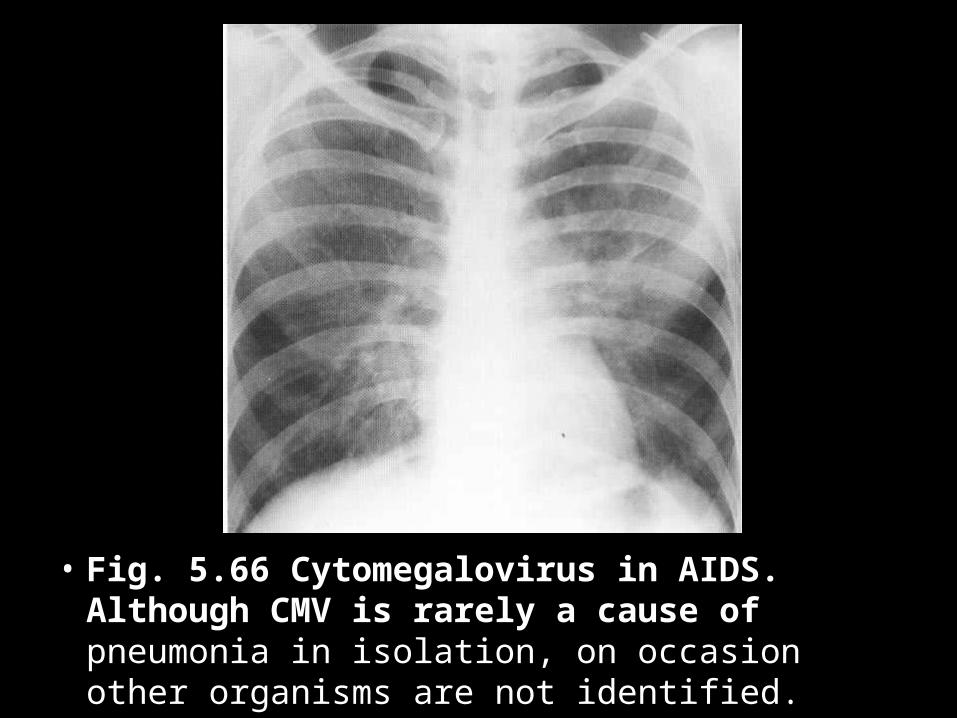
• Fig. 5.66 Cytomegalovirus in AIDS. Although CMV is rarely a cause of pneumonia in isolation, on occasion other organisms are not identified.
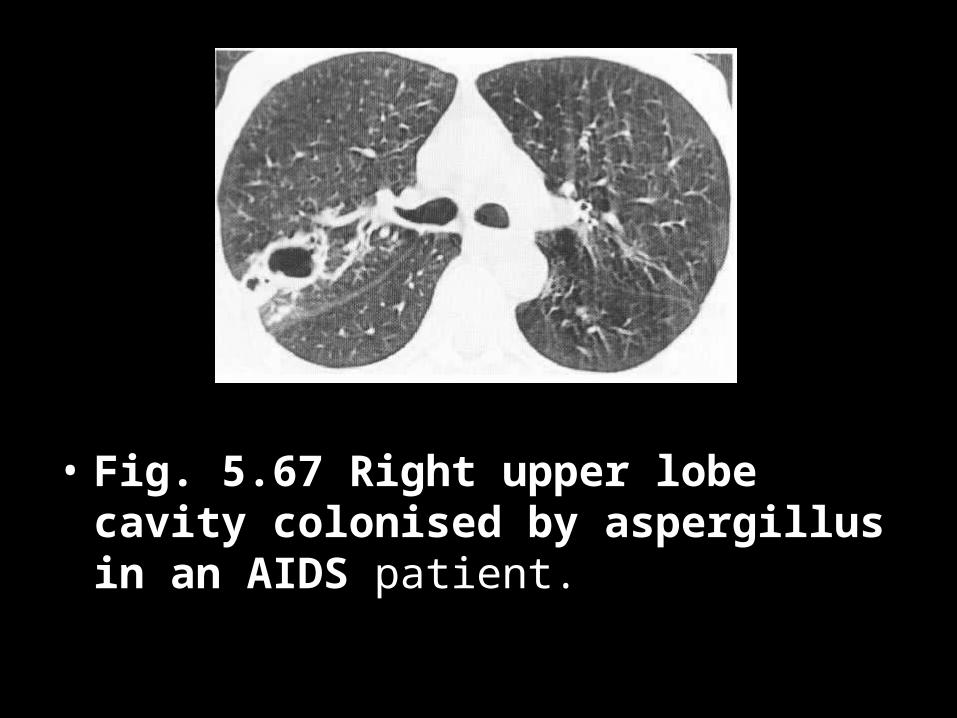
• Fig. 5.67 Right upper lobe cavity colonised by aspergillus in an AIDS patient.
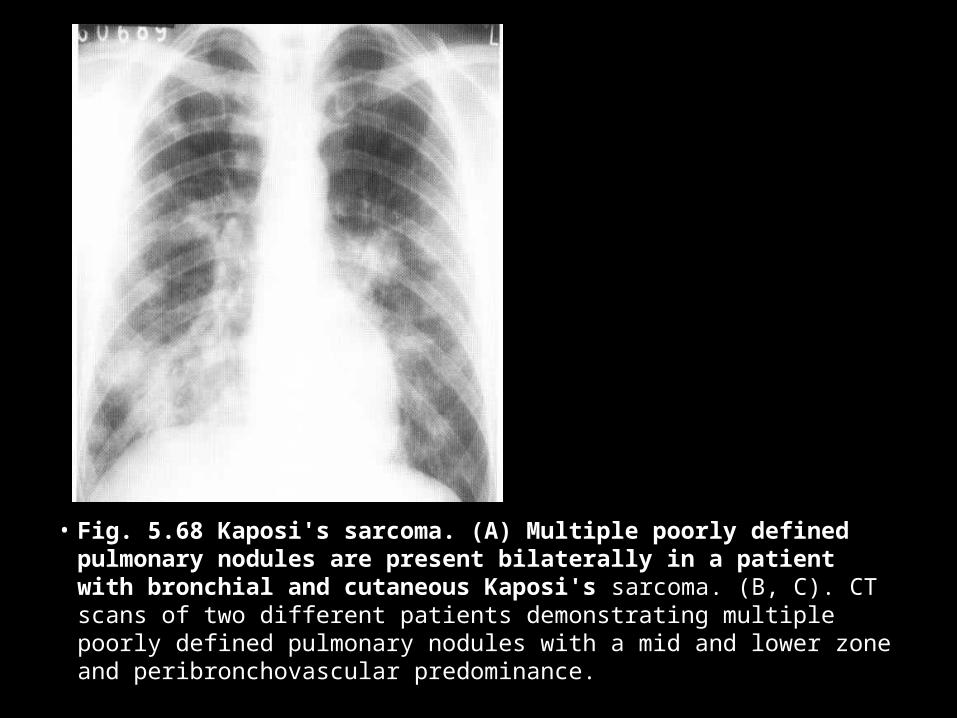
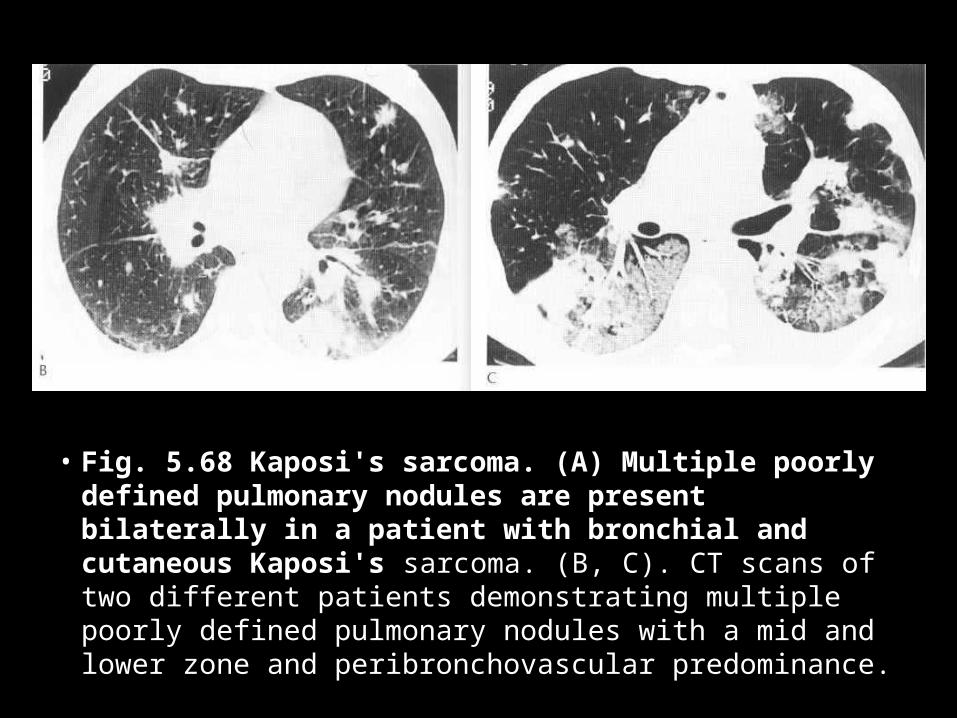
• Fig. 5.68 Kaposi's sarcoma. (A) Multiple poorly defined pulmonary nodules are present bilaterally in a patient with bronchial and cutaneous Kaposi's sarcoma. (B, C). CT scans of two different patients demonstrating multiple poorly defined pulmonary nodules with a mid and lower zone and peribronchovascular predominance.
• Fig. 5.68 Kaposi's sarcoma. (A) Multiple poorly defined pulmonary nodules are present bilaterally in a patient with bronchial and cutaneous Kaposi's sarcoma. (B, C). CT scans of two different patients demonstrating multiple poorly defined pulmonary nodules with a mid and lower zone and peribronchovascular predominance.
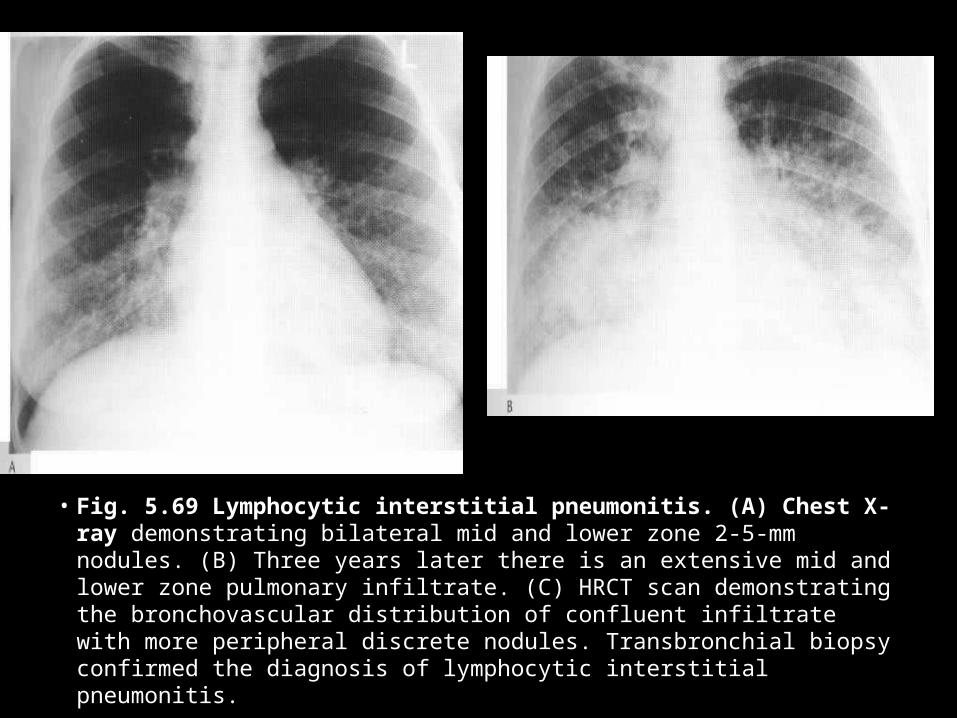
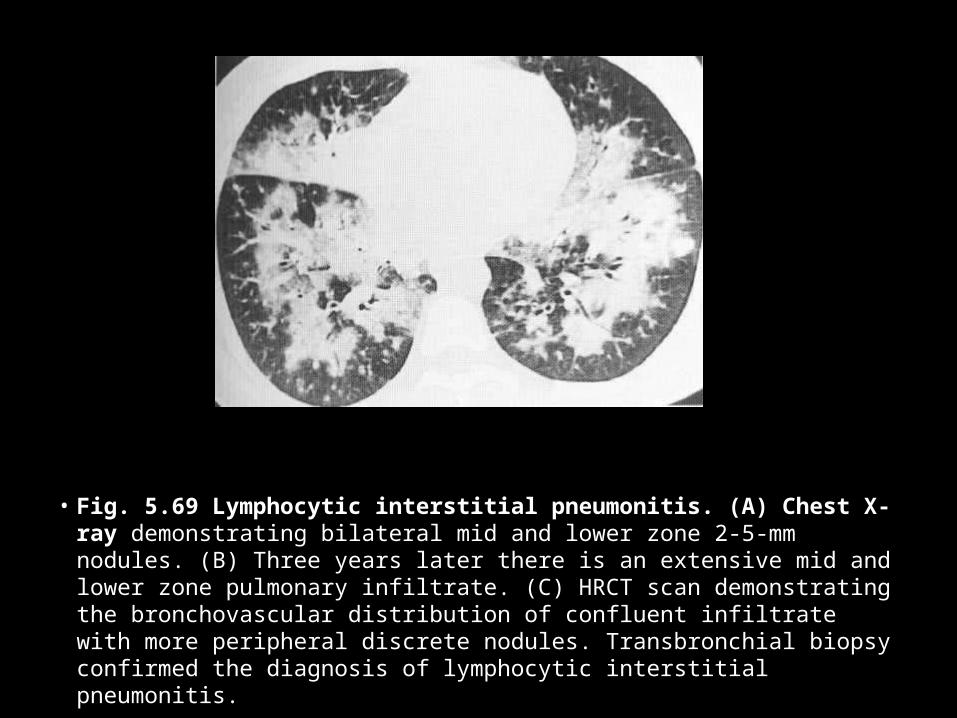
• Fig. 5.69 Lymphocytic interstitial pneumonitis. (A) Chest X-ray demonstrating bilateral mid and lower zone 2-5-mm nodules. (B) Three years later there is an extensive mid and lower zone pulmonary infiltrate. (C) HRCT scan demonstrating the bronchovascular distribution of confluent infiltrate with more peripheral discrete nodules. Transbronchial biopsy confirmed the diagnosis of lymphocytic interstitial pneumonitis.
• Fig. 5.69 Lymphocytic interstitial pneumonitis. (A) Chest X-ray demonstrating bilateral mid and lower zone 2-5-mm nodules. (B) Three years later there is an extensive mid and lower zone pulmonary infiltrate. (C) HRCT scan demonstrating the bronchovascular distribution of confluent infiltrate with more peripheral discrete nodules. Transbronchial biopsy confirmed the diagnosis of lymphocytic interstitial pneumonitis.
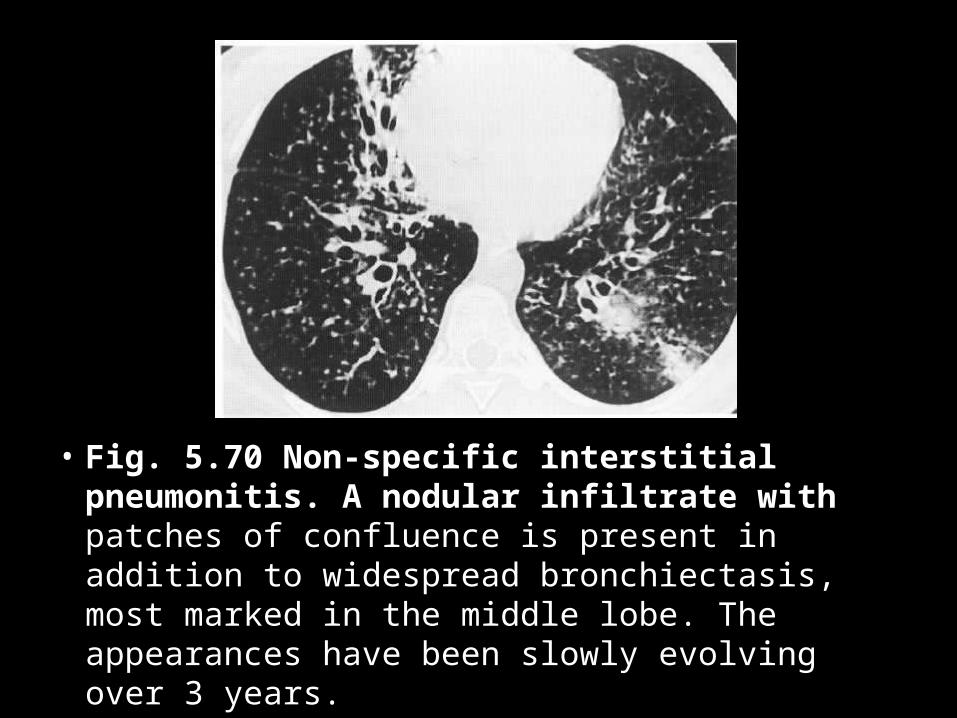
• Fig. 5.70 Non-specific interstitial pneumonitis. A nodular infiltrate with patches of confluence is present in addition to widespread bronchiectasis, most marked in the middle lobe. The appearances have been slowly evolving over 3 years.
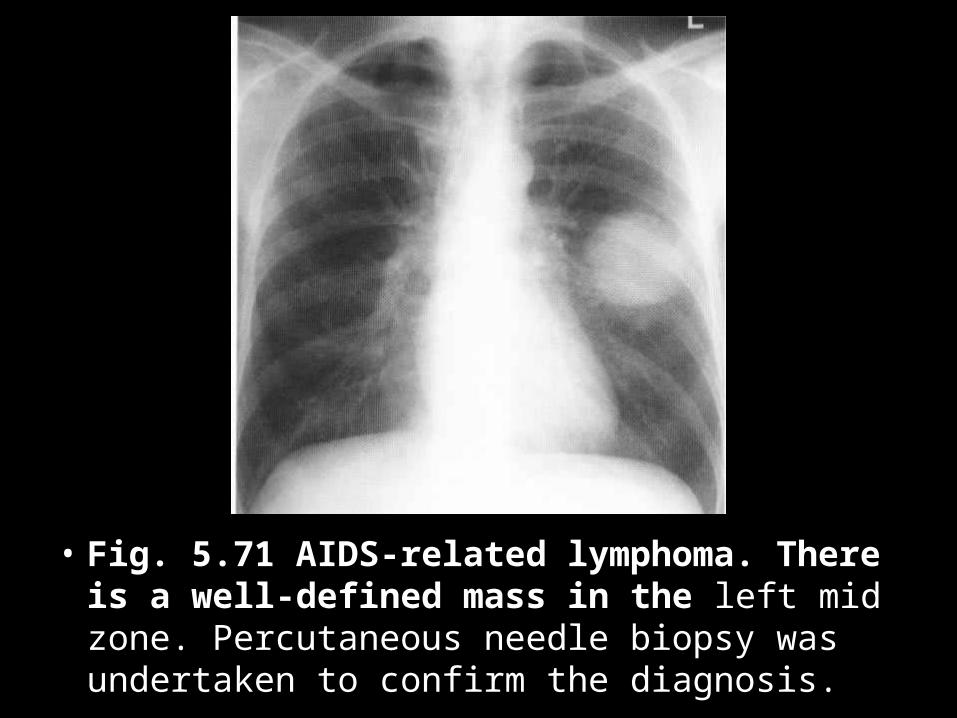
• Fig. 5.71 AIDS-related lymphoma. There is a well-defined mass in the left mid zone. Percutaneous needle biopsy was undertaken to confirm the diagnosis.
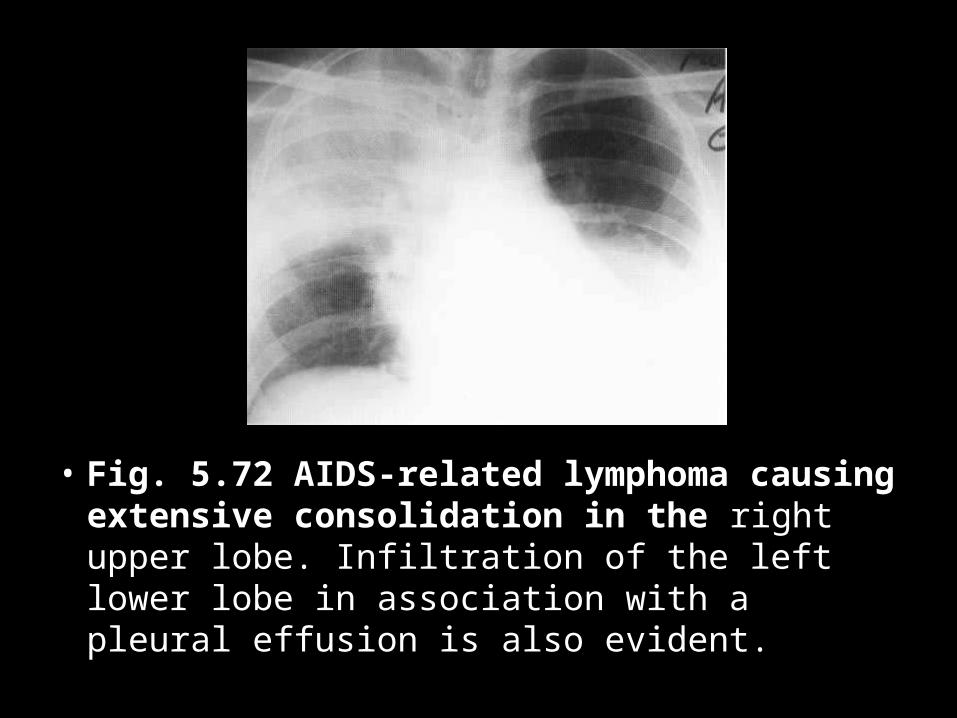
• Fig. 5.72 AIDS-related lymphoma causing extensive consolidation in the right upper lobe. Infiltration of the left lower lobe in association with a pleural effusion is also evident.






















![[Nestor L. Muller] Imaging of Pulmonary Infections](https://img.dokumen.tips/doc/110x75/577cd5ce1a28ab9e789ba8ac/nestor-l-muller-imaging-of-pulmonary-infections.jpg)






