Embed Size (px)
Citation preview

46 Elevated Diaphragm

CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL

• Fig C 46-1 Partial eventration. Of the right hemidiaphragm (arrow).

• Fig C 46-2 Complete eventration. Of the right hemidiaphragm.

• Fig C 46-3 Phrenic nerve paralysis. Primary bronchogenic carcinoma (arrow) involving the phrenic nerve causes paralysis of the right hemidiaphragm

• Fig C 46-4 Intra-abdominal mass. (A) Acute gastric dilatation causes diffuse elevation of both leaves of the diaphragm. (B) Huge syphilitic gumma of the liver produces elevation of the right hemidiaphragm.

• Fig C 46-5 Acute pneumonia. Elevation of the right hemidiaphragm due to splinting secondary to a right lower lung infiltrate.

• Fig C 46-6 Subpulmonic effusion. The peak of the pseudodiaphragmatic contour (arrow) is lateral to that of a normal hemidiaphragm.

• Fig C 46-7 Morgagni hernia. (A) Frontal and (B) lateral views demonstrate barium-filled bowel in a hernia sac that lies anteriorly and to the right.

• Fig C 46-8 Bochdalek hernia. Gas-filled loop of bowel (arrow) is visible posteriorly in the thoracic cavity.

• Fig C 46-9 Traumatic rupture of the diaphragm. Herniation of a portion of the splenic flexure (arrow), with obstruction to the retrograde flow of barium.
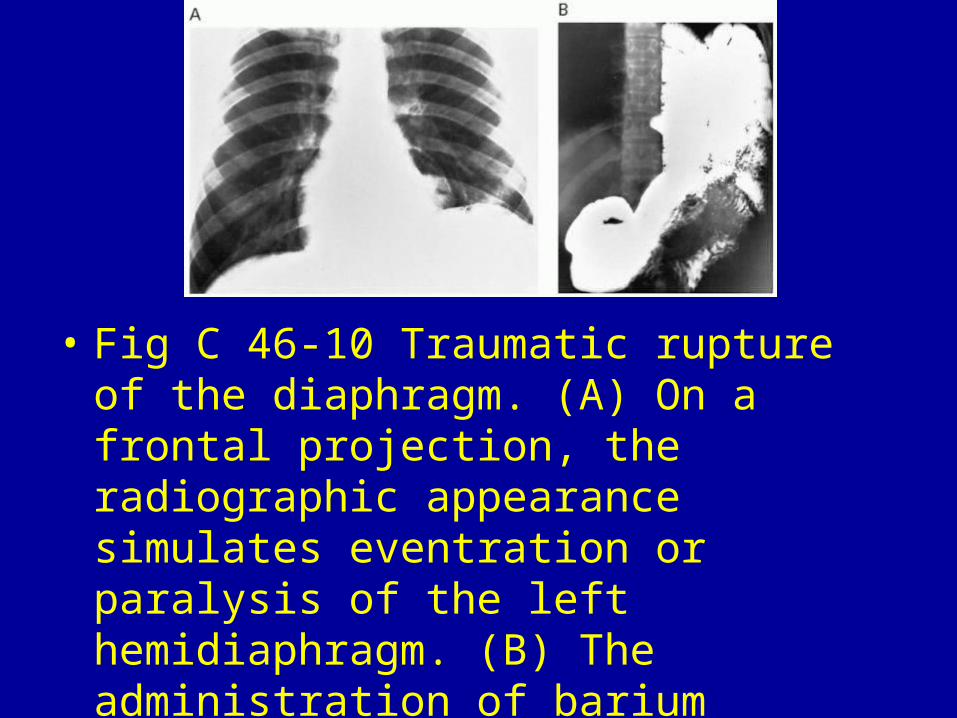
• Fig C 46-10 Traumatic rupture of the diaphragm. (A) On a frontal projection, the radiographic appearance simulates eventration or paralysis of the left hemidiaphragm. (B) The administration of barium clearly demonstrates the herniation of bowel contents into the chest.






























