Embed Size (px)
Citation preview

ATTENTION SLIDESHARERS:This presentation is part 2 of a 2 part presentation.
The first half of this presentation can be viewed at:www.slideshare.net/stephenpa
Travel Network User Experience | sabreux.comhttp://flickr.com/photos/juanignaciosl/237734498/
CASESTUDIES

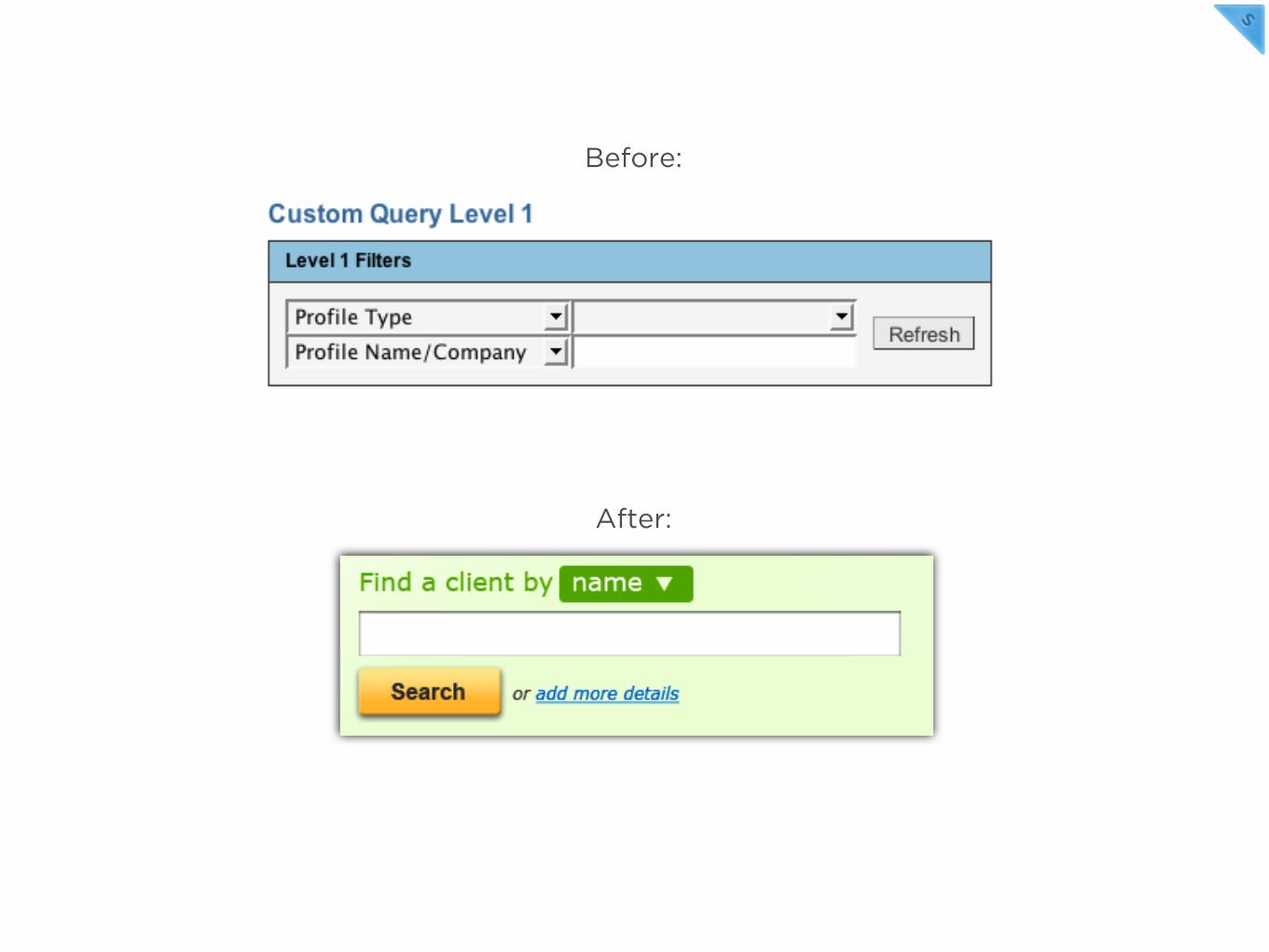
After:
Before:

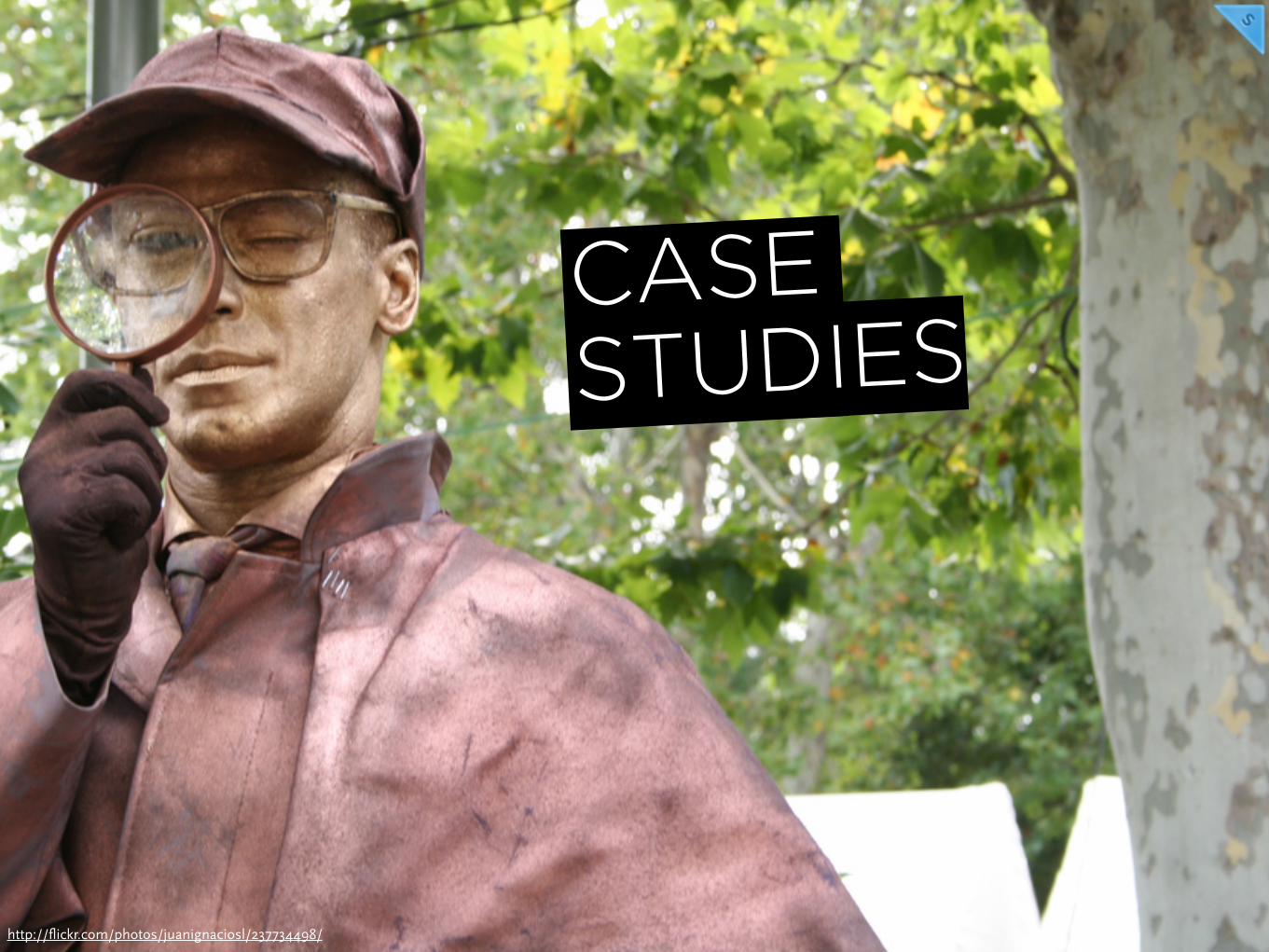
Before:

Before:
This was uneccesary
Hid Additional Filter
Before:

Before:
Changed label
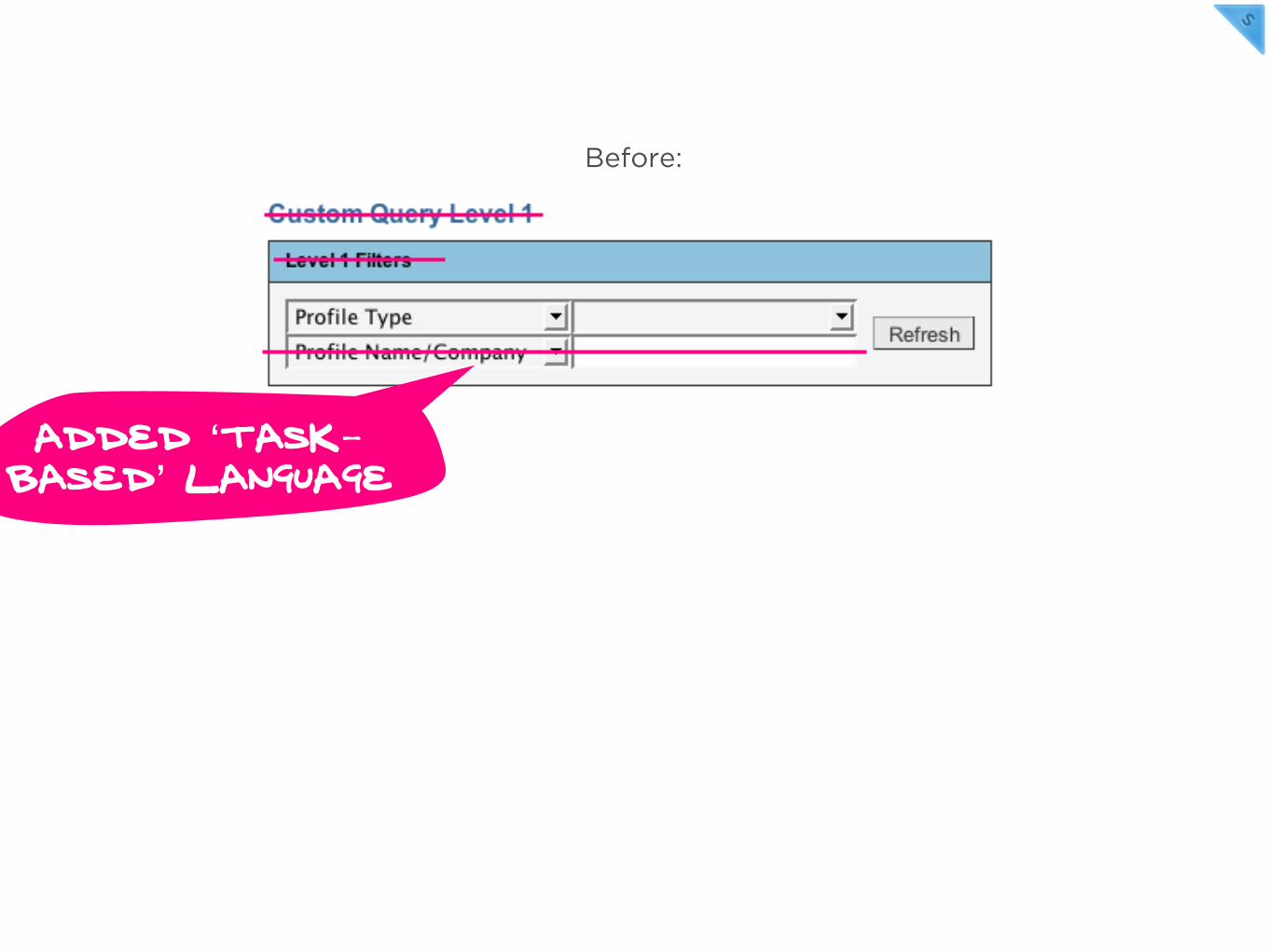
Added ‘task-based’ language
Before:
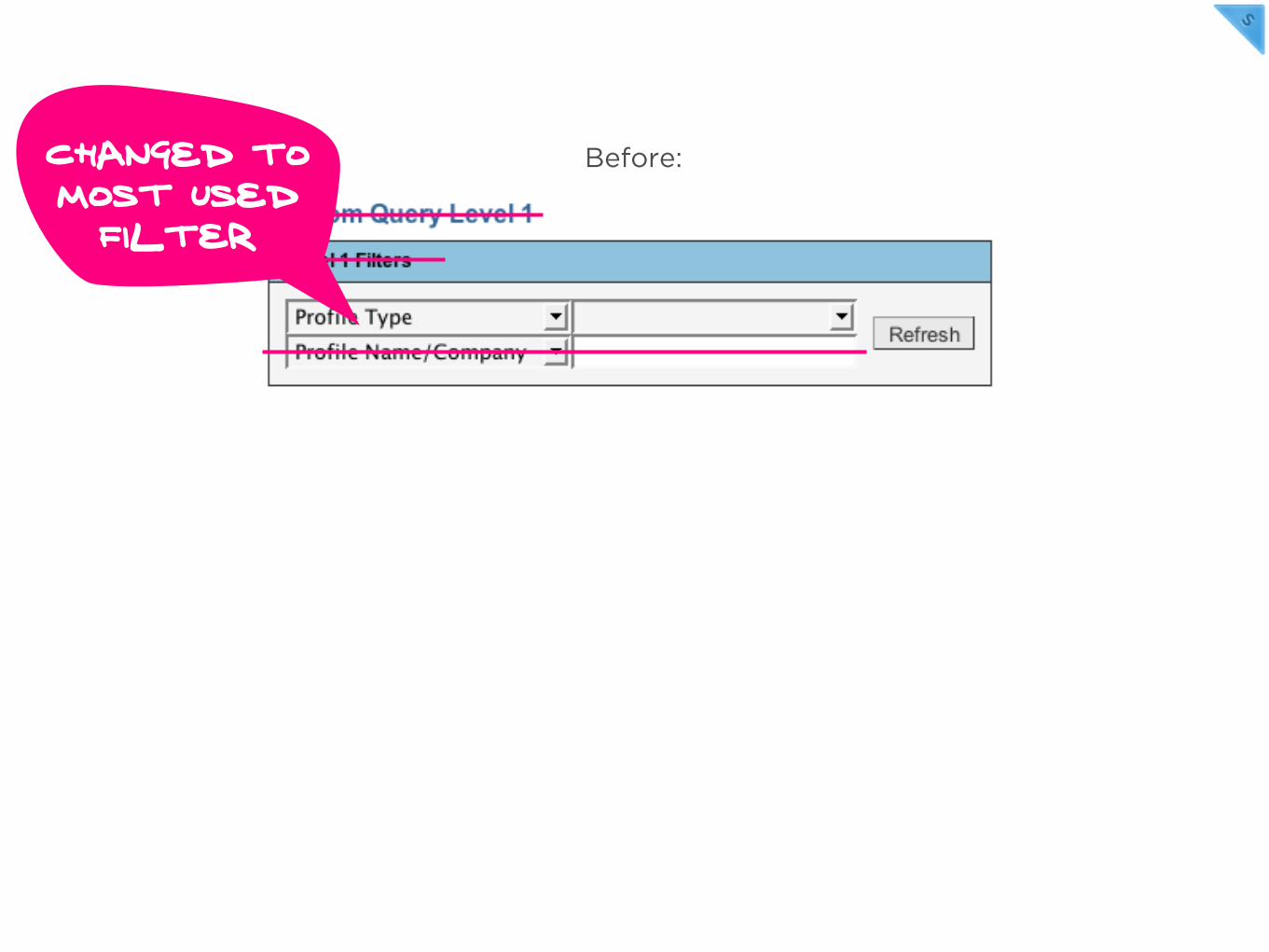
Changed to most used
filter
Before:
After:
Before:

INFO DESIGN & TATTOOS

INFO DESIGN & TATTOOSHELLO.
I’m Travis’s Dad


Scary looking monsterthing on my forearm. Don’t tell mom.
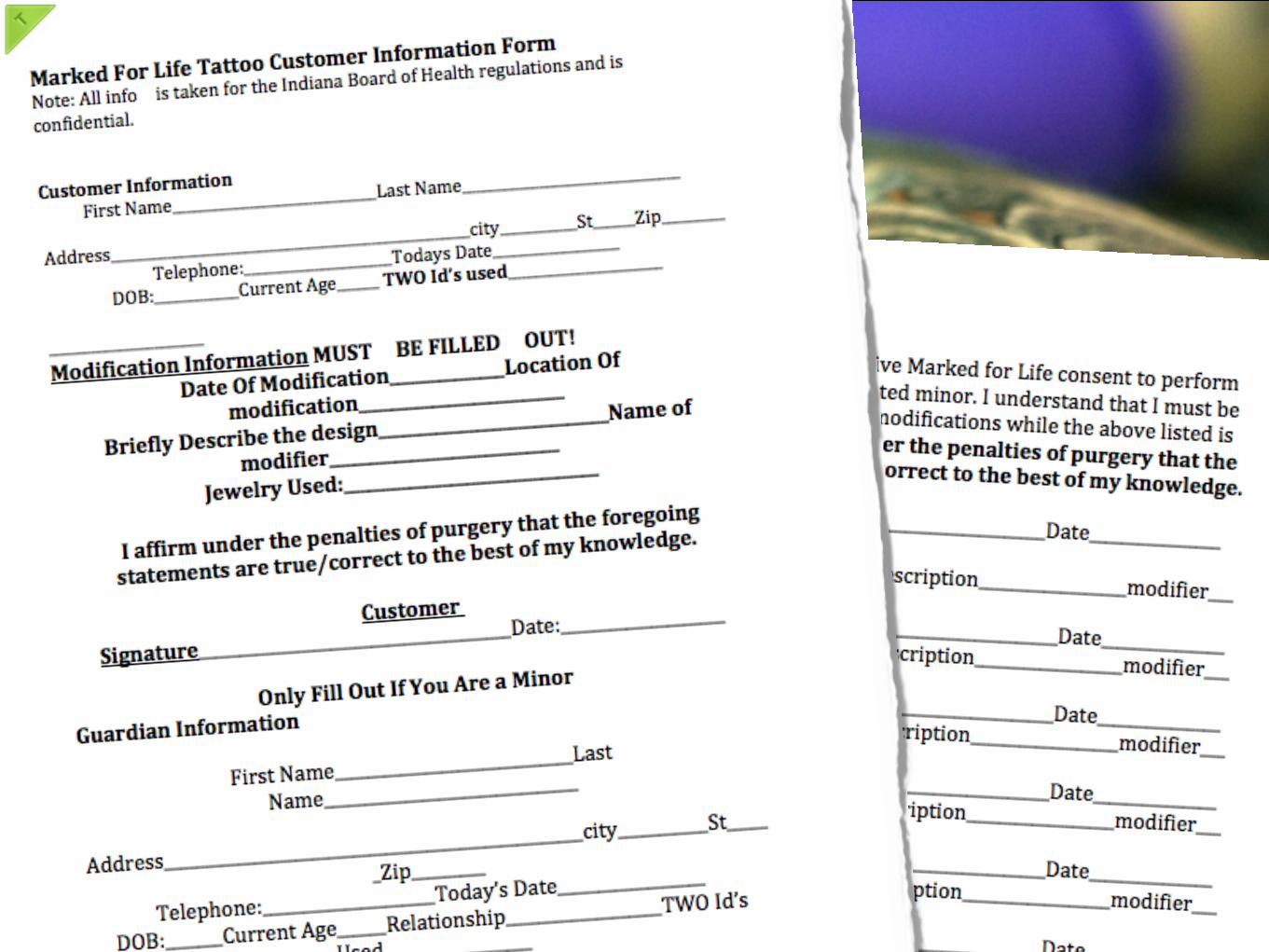

Confusing language
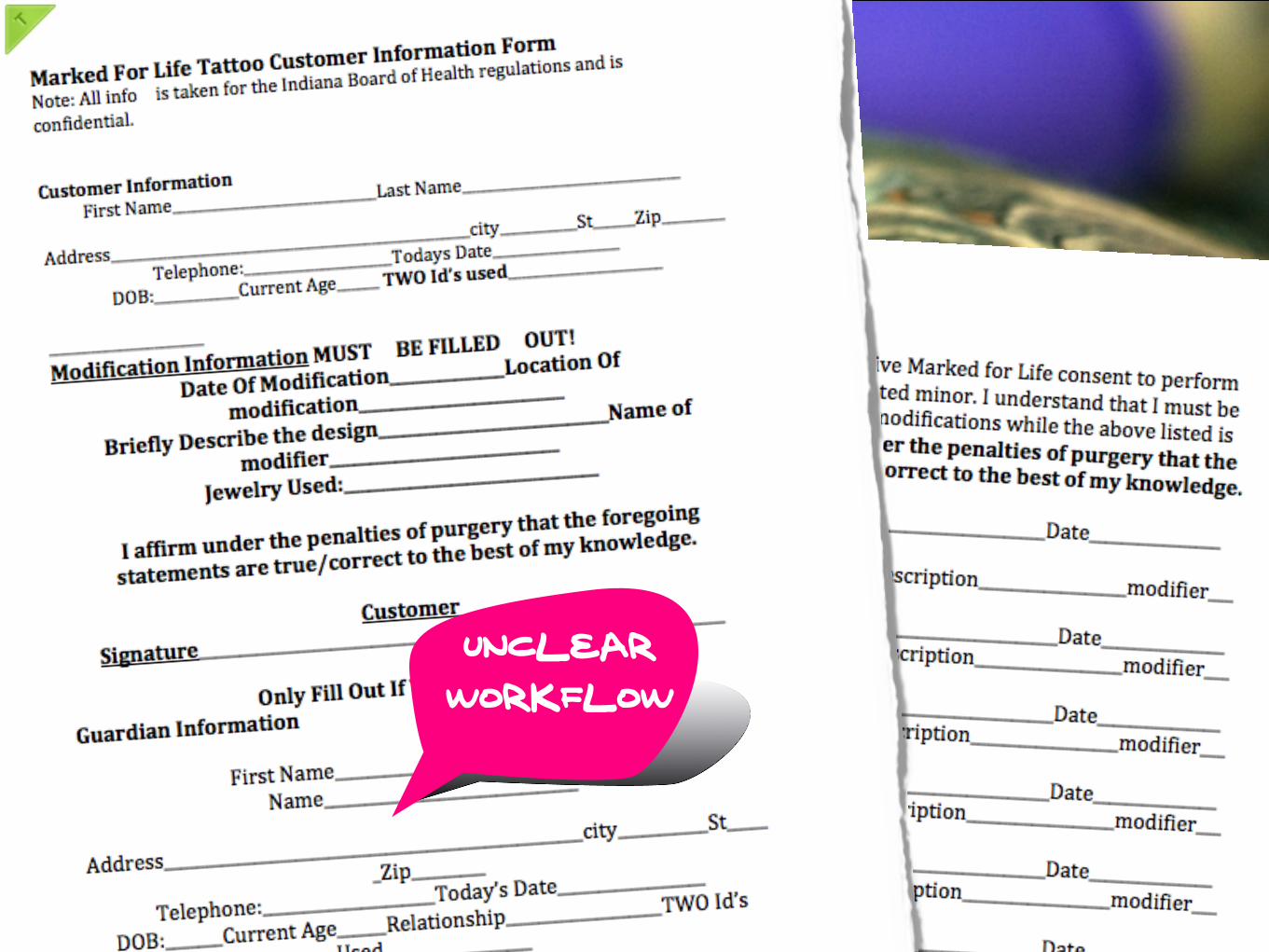
Unclear workflow

HUH?
INDIANA?
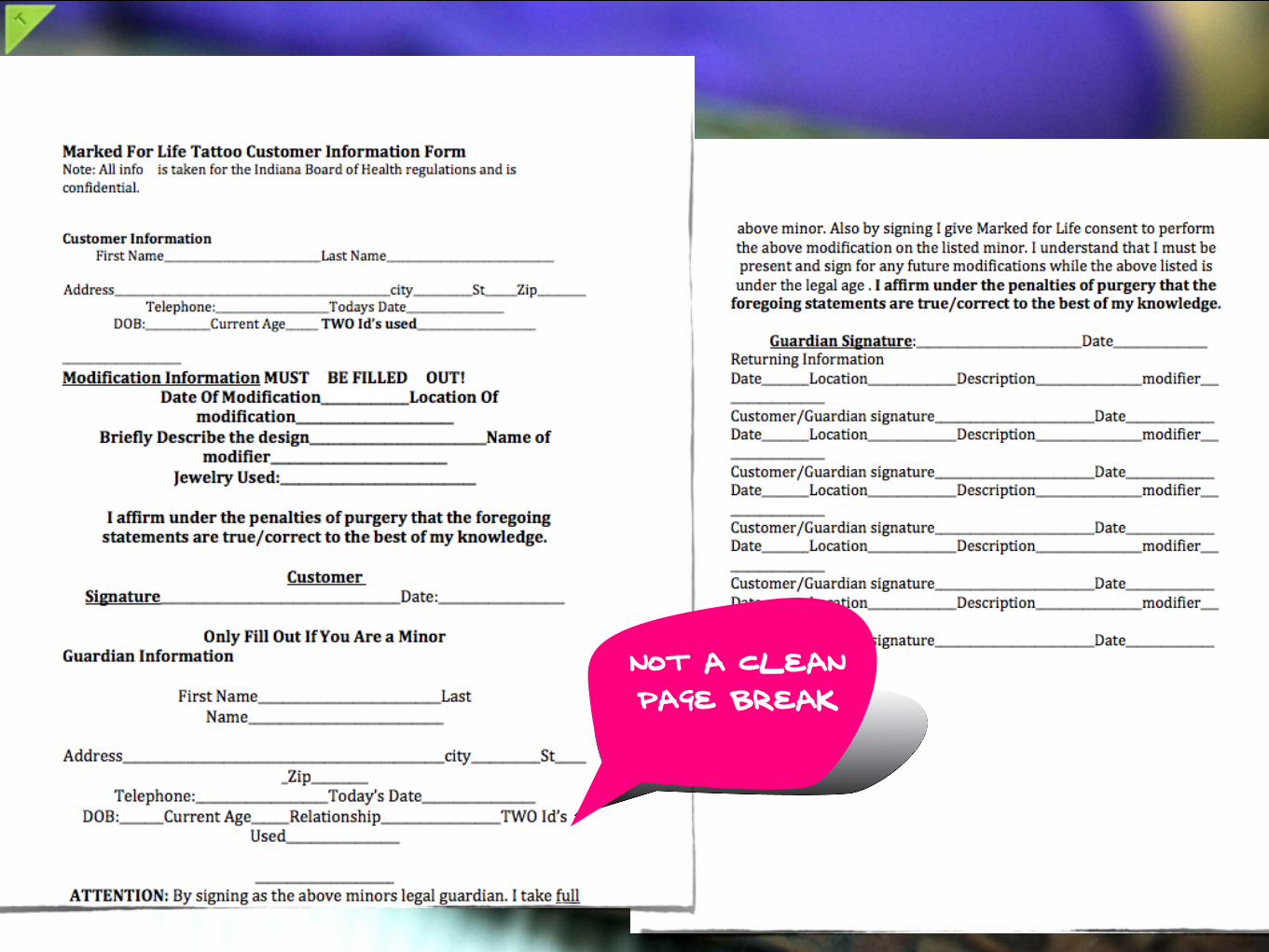
Not a cleanpage break
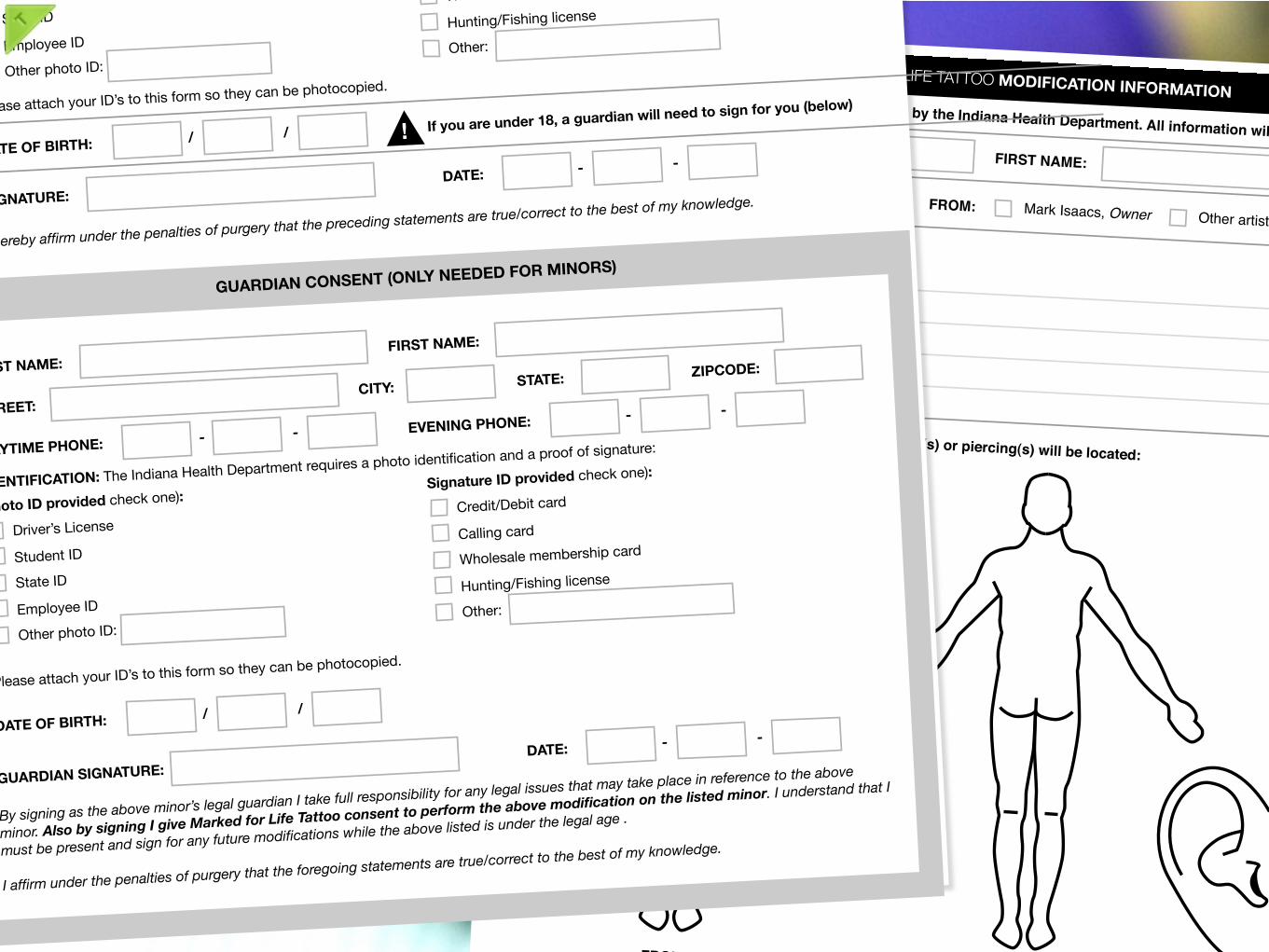
MARKED FOR LIFE TATTOO MODIFICATION INFORMATIONNOTE: The information below is required by the Indiana Health Department. All information will kept confidential.LAST NAME:1
FIRST NAME:
I!M GETTING A:2
Tattoo Piercing FROM: Mark Isaacs, Owner Other artist:
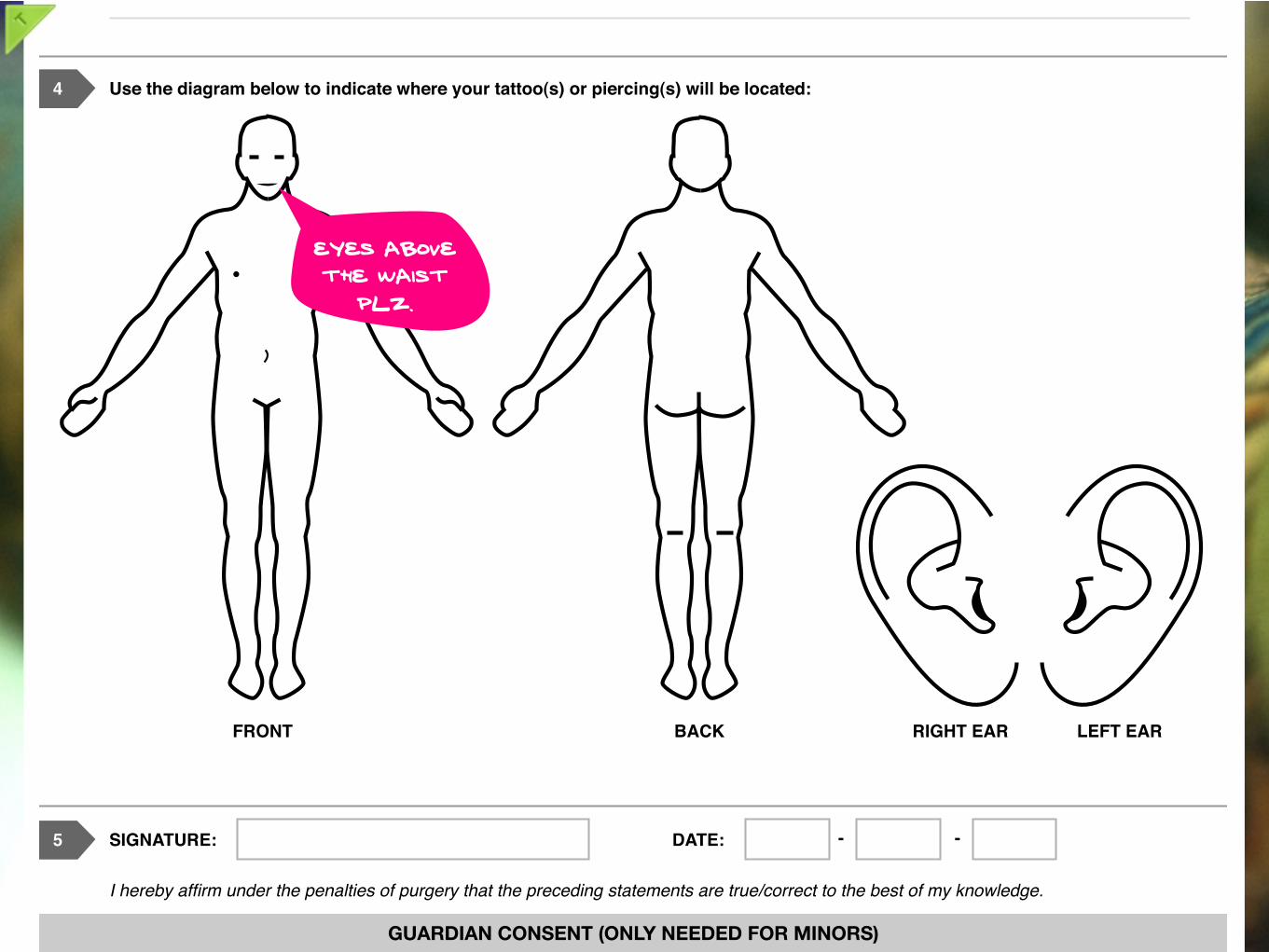
4 Use the diagram below to indicate where your tattoo(s) or piercing(s) will be located:
FRONTBACK
RIGHT EAR LEFT EAR
SIGNATURE:5
DATE: - -I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge. GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
GUARDIAN SIGNATURE:
DATE: - -By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age . I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
3 Please describe your Tattoo(s) or Piercing(s):
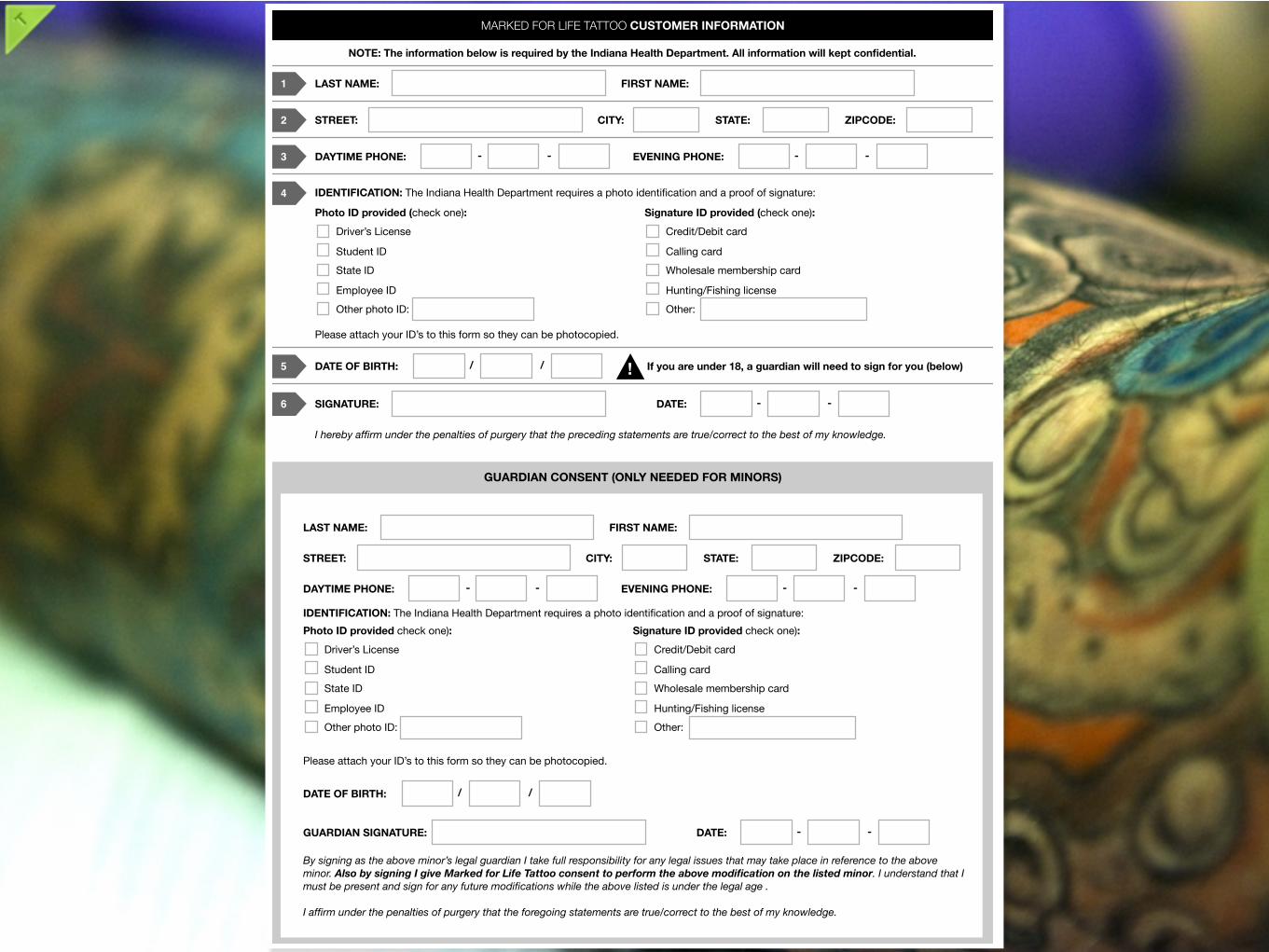
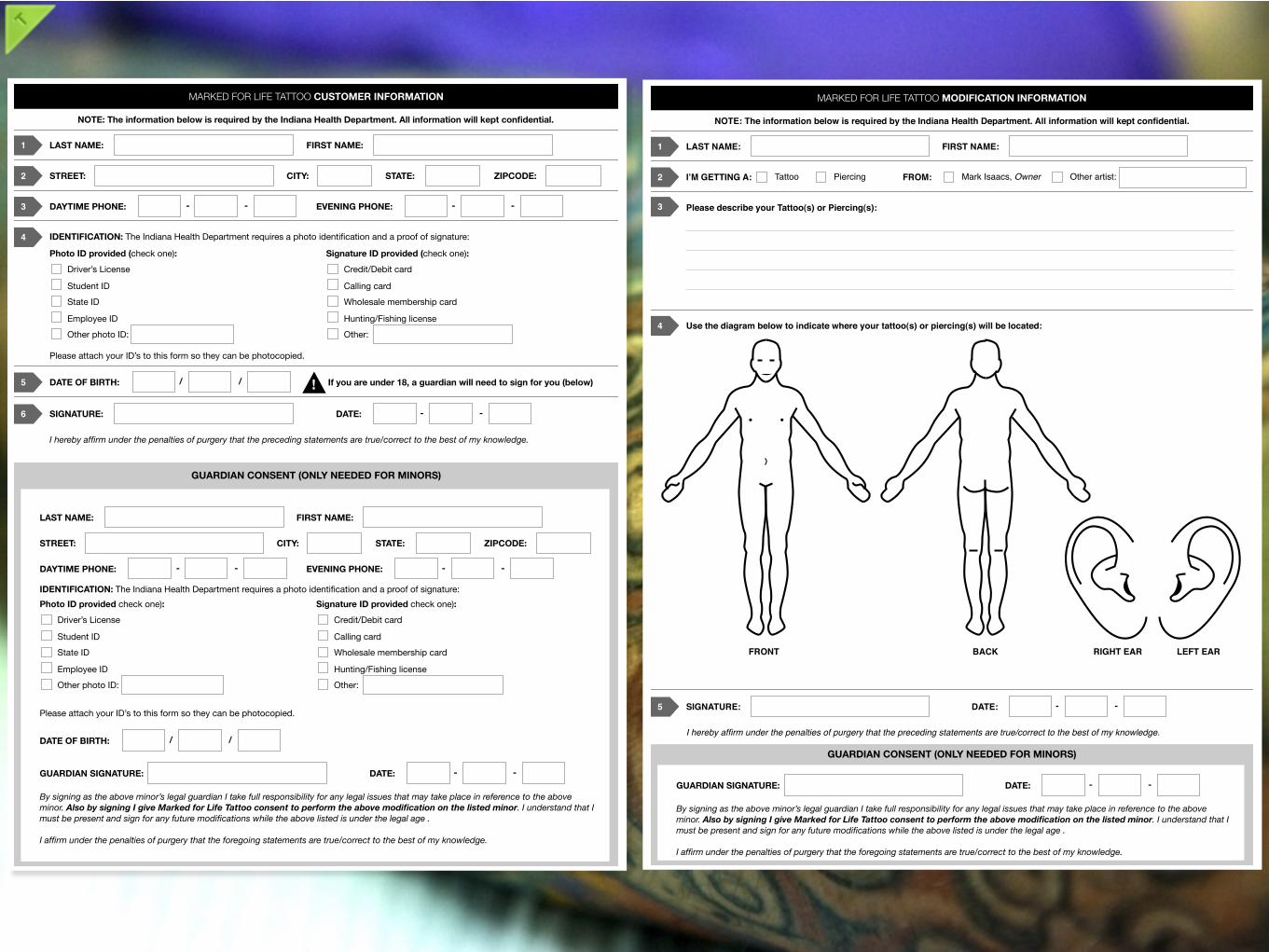
MARKED FOR LIFE TATTOO CUSTOMER INFORMATION
LAST NAME:1
FIRST NAME:
STREET:2
CITY:STATE:
ZIPCODE:
DAYTIME PHONE:3
EVENING PHONE:- -
- -
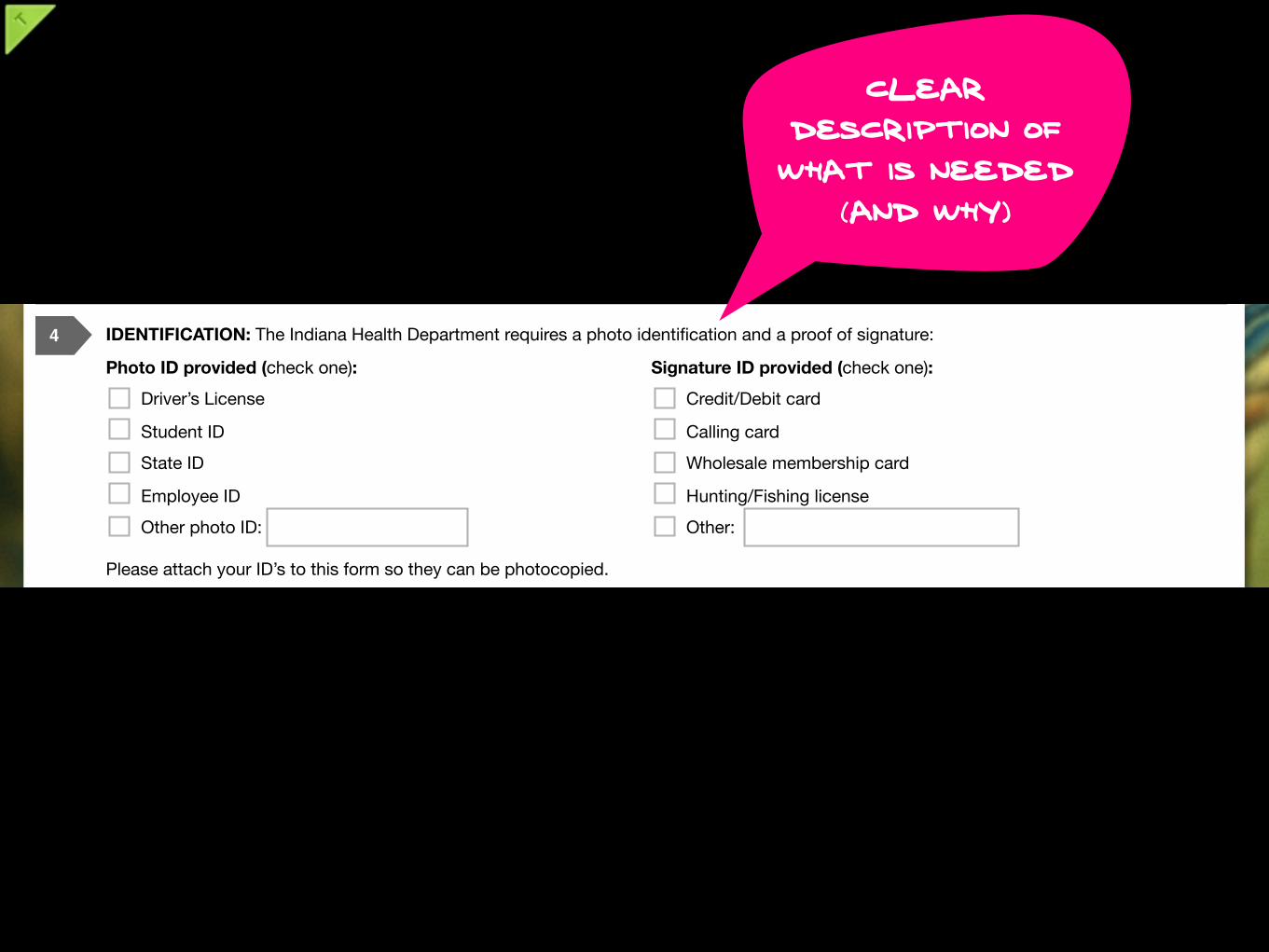
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:
4
Photo ID provided (check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided (check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
SIGNATURE:6
DATE:- -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
DATE OF BIRTH:5
/ / If you are under 18, a guardian will need to sign for you (below)
!
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
LAST NAME:
FIRST NAME:
STREET:
CITY:STATE:
ZIPCODE:
DAYTIME PHONE:EVENING PHONE:
- -
- -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:
Photo ID provided check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
GUARDIAN SIGNATURE:
DATE:- -
DATE OF BIRTH:/ /
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
MARKED FOR LIFE TATTOO CUSTOMER INFORMATION
LAST NAME:1 FIRST NAME:
STREET:2 CITY: STATE: ZIPCODE:
DAYTIME PHONE:3 EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:4
Photo ID provided (check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided (check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
SIGNATURE:6 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
DATE OF BIRTH:5 / / If you are under 18, a guardian will need to sign for you (below)!
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
LAST NAME: FIRST NAME:
STREET: CITY: STATE: ZIPCODE:
DAYTIME PHONE: EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:
Photo ID provided check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
GUARDIAN SIGNATURE: DATE: - -
DATE OF BIRTH: / /
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.

MARKED FOR LIFE TATTOO CUSTOMER INFORMATION
LAST NAME:1 FIRST NAME:
STREET:2 CITY: STATE: ZIPCODE:
DAYTIME PHONE:3 EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:4
Photo ID provided (check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided (check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
SIGNATURE:6 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
DATE OF BIRTH:5 / / If you are under 18, a guardian will need to sign for you (below)!
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
LAST NAME: FIRST NAME:
STREET: CITY: STATE: ZIPCODE:
DAYTIME PHONE: EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:
Photo ID provided check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
GUARDIAN SIGNATURE: DATE: - -
DATE OF BIRTH: / /
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
Guided workflow
MARKED FOR LIFE TATTOO CUSTOMER INFORMATION
LAST NAME:1 FIRST NAME:
STREET:2 CITY: STATE: ZIPCODE:
DAYTIME PHONE:3 EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:4
Photo ID provided (check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided (check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
SIGNATURE:6 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
DATE OF BIRTH:5 / / If you are under 18, a guardian will need to sign for you (below)!
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
LAST NAME: FIRST NAME:
STREET: CITY: STATE: ZIPCODE:
DAYTIME PHONE: EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:
Photo ID provided check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
GUARDIAN SIGNATURE: DATE: - -
DATE OF BIRTH: / /
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.clear
description of what is needed
(and why)

MARKED FOR LIFE TATTOO CUSTOMER INFORMATION
LAST NAME:1 FIRST NAME:
STREET:2 CITY: STATE: ZIPCODE:
DAYTIME PHONE:3 EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:4
Photo ID provided (check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided (check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
SIGNATURE:6 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
DATE OF BIRTH:5 / / If you are under 18, a guardian will need to sign for you (below)!
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
LAST NAME: FIRST NAME:
STREET: CITY: STATE: ZIPCODE:
DAYTIME PHONE: EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:
Photo ID provided check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
GUARDIAN SIGNATURE: DATE: - -
DATE OF BIRTH: / /
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
Previously this was looked
over
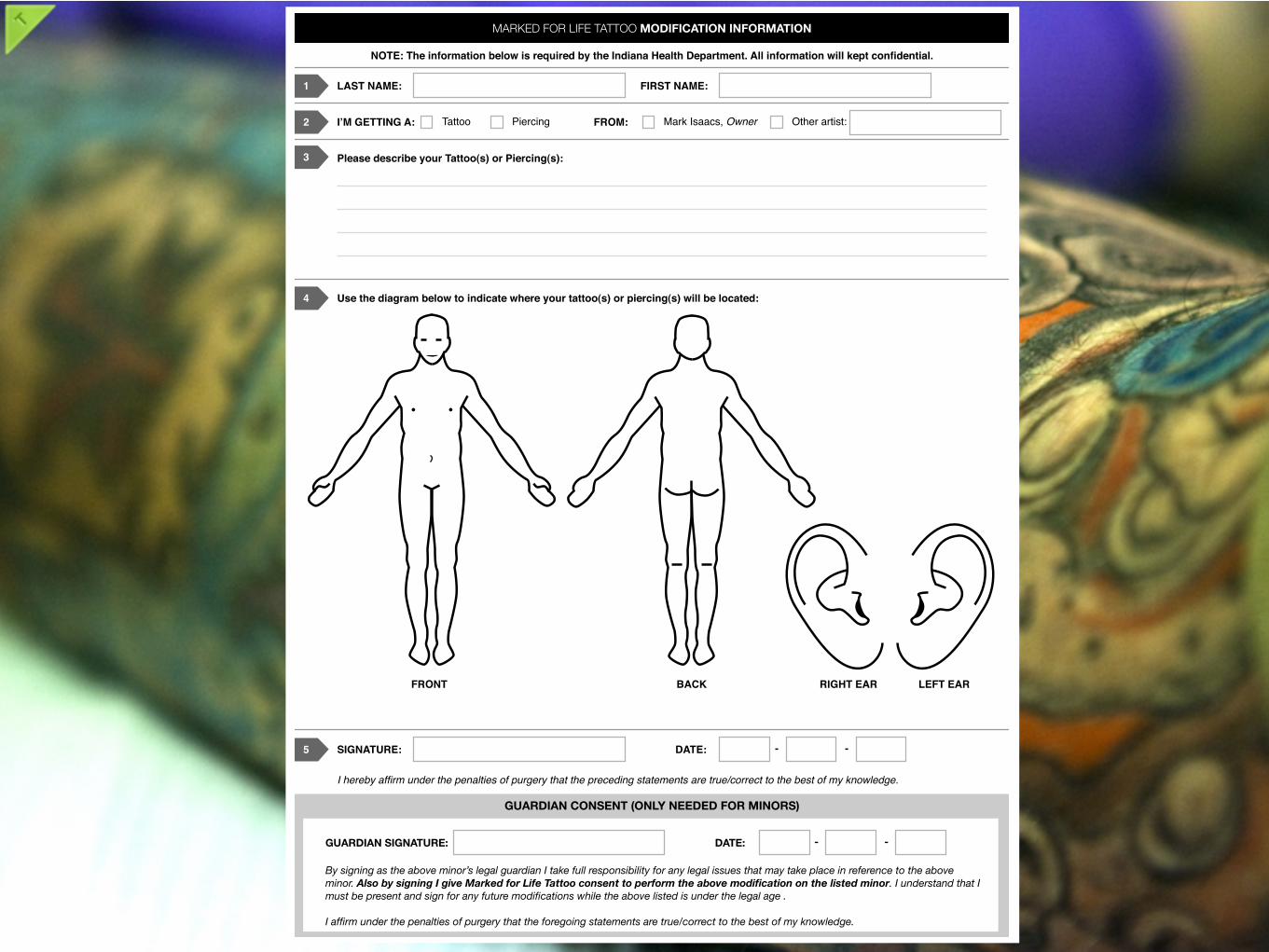
MARKED FOR LIFE TATTOO MODIFICATION INFORMATION
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
LAST NAME:1 FIRST NAME:
I!M GETTING A:2 Tattoo Piercing FROM: Mark Isaacs, Owner Other artist:
4 Use the diagram below to indicate where your tattoo(s) or piercing(s) will be located:
FRONT BACK RIGHT EAR LEFT EAR
SIGNATURE:5 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
GUARDIAN SIGNATURE: DATE: - -
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
3 Please describe your Tattoo(s) or Piercing(s):

MARKED FOR LIFE TATTOO MODIFICATION INFORMATION
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
LAST NAME:1 FIRST NAME:
I!M GETTING A:2 Tattoo Piercing FROM: Mark Isaacs, Owner Other artist:
4 Use the diagram below to indicate where your tattoo(s) or piercing(s) will be located:
FRONT BACK RIGHT EAR LEFT EAR
SIGNATURE:5 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
GUARDIAN SIGNATURE: DATE: - -
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
3 Please describe your Tattoo(s) or Piercing(s):
Type of “modification”
MARKED FOR LIFE TATTOO MODIFICATION INFORMATION
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
LAST NAME:1 FIRST NAME:
I!M GETTING A:2 Tattoo Piercing FROM: Mark Isaacs, Owner Other artist:
4 Use the diagram below to indicate where your tattoo(s) or piercing(s) will be located:
FRONT BACK RIGHT EAR LEFT EAR
SIGNATURE:5 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
GUARDIAN SIGNATURE: DATE: - -
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
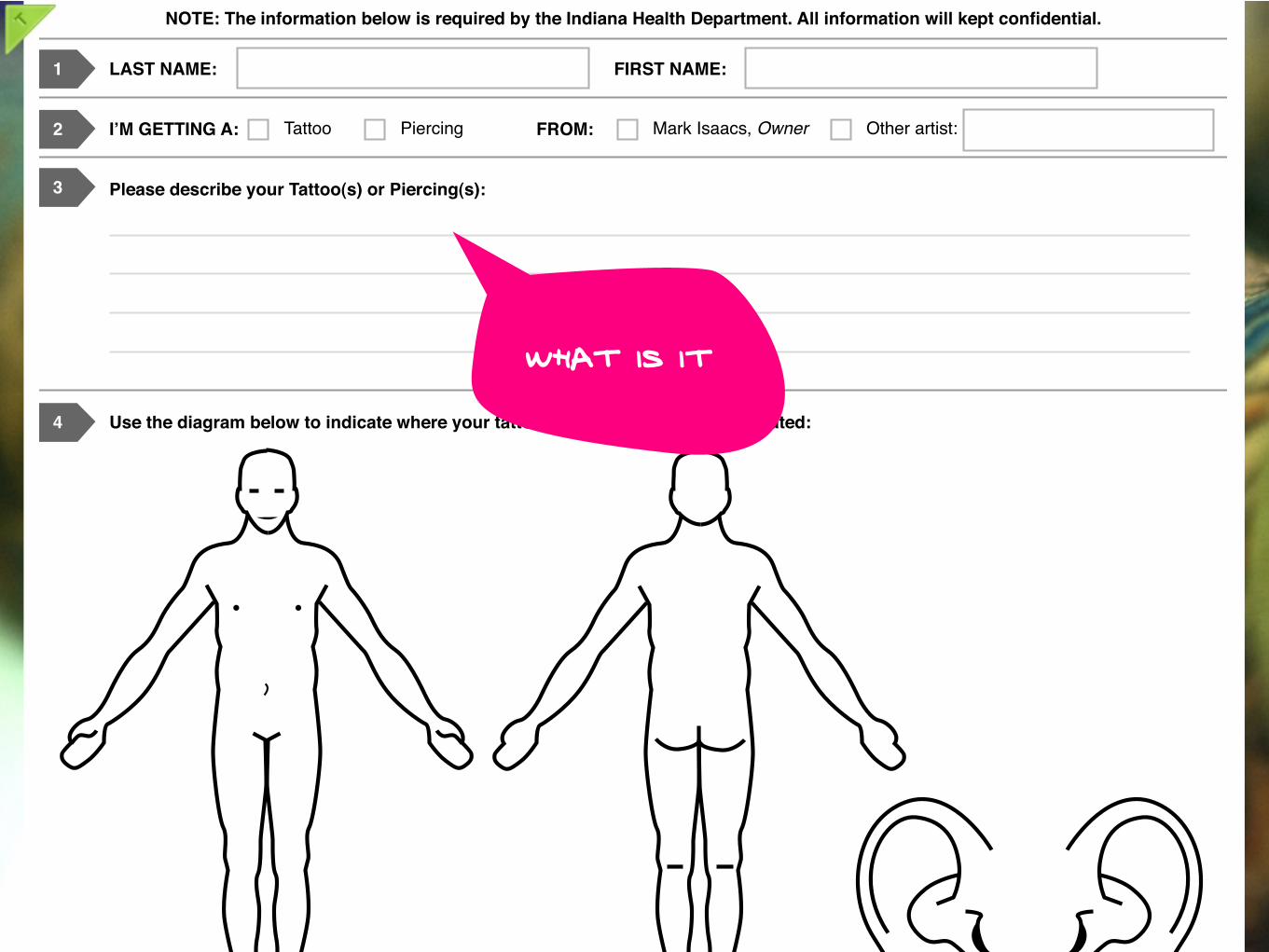
3 Please describe your Tattoo(s) or Piercing(s):
What is it
MARKED FOR LIFE TATTOO MODIFICATION INFORMATION
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
LAST NAME:1 FIRST NAME:
I!M GETTING A:2 Tattoo Piercing FROM: Mark Isaacs, Owner Other artist:
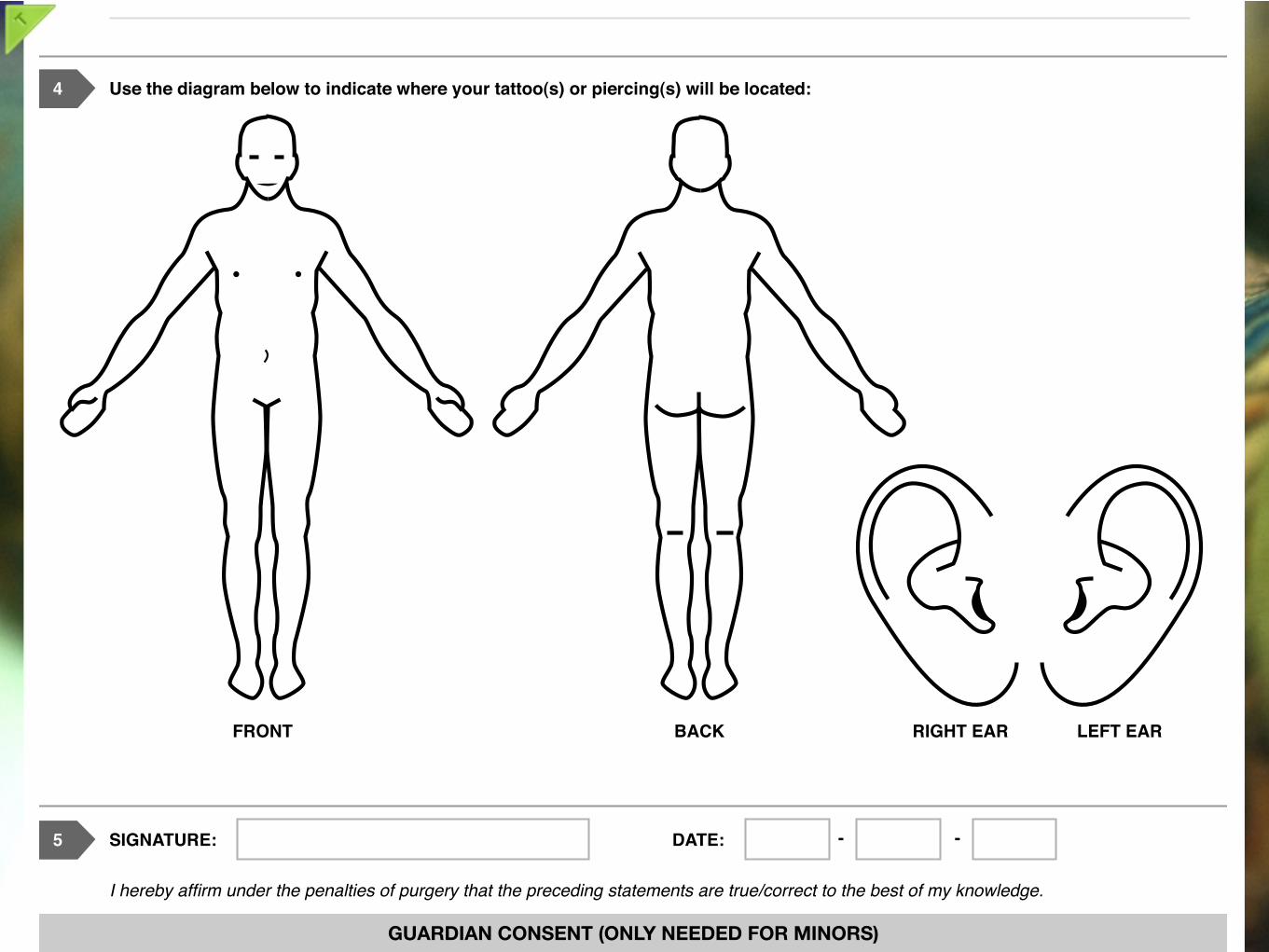
4 Use the diagram below to indicate where your tattoo(s) or piercing(s) will be located:
FRONT BACK RIGHT EAR LEFT EAR
SIGNATURE:5 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
GUARDIAN SIGNATURE: DATE: - -
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
3 Please describe your Tattoo(s) or Piercing(s):
MARKED FOR LIFE TATTOO MODIFICATION INFORMATION
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
LAST NAME:1 FIRST NAME:
I!M GETTING A:2 Tattoo Piercing FROM: Mark Isaacs, Owner Other artist:
4 Use the diagram below to indicate where your tattoo(s) or piercing(s) will be located:
FRONT BACK RIGHT EAR LEFT EAR
SIGNATURE:5 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
GUARDIAN SIGNATURE: DATE: - -
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
3 Please describe your Tattoo(s) or Piercing(s):
Eyes abovethe waist
PLZ.
MARKED FOR LIFE TATTOO MODIFICATION INFORMATION
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
LAST NAME:1 FIRST NAME:
I!M GETTING A:2 Tattoo Piercing FROM: Mark Isaacs, Owner Other artist:
4 Use the diagram below to indicate where your tattoo(s) or piercing(s) will be located:
FRONT BACK RIGHT EAR LEFT EAR
SIGNATURE:5 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
GUARDIAN SIGNATURE: DATE: - -
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
3 Please describe your Tattoo(s) or Piercing(s):
MARKED FOR LIFE TATTOO CUSTOMER INFORMATION
LAST NAME:1 FIRST NAME:
STREET:2 CITY: STATE: ZIPCODE:
DAYTIME PHONE:3 EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:4
Photo ID provided (check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided (check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
SIGNATURE:6 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
DATE OF BIRTH:5 / / If you are under 18, a guardian will need to sign for you (below)!
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
LAST NAME: FIRST NAME:
STREET: CITY: STATE: ZIPCODE:
DAYTIME PHONE: EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:
Photo ID provided check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
GUARDIAN SIGNATURE: DATE: - -
DATE OF BIRTH: / /
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
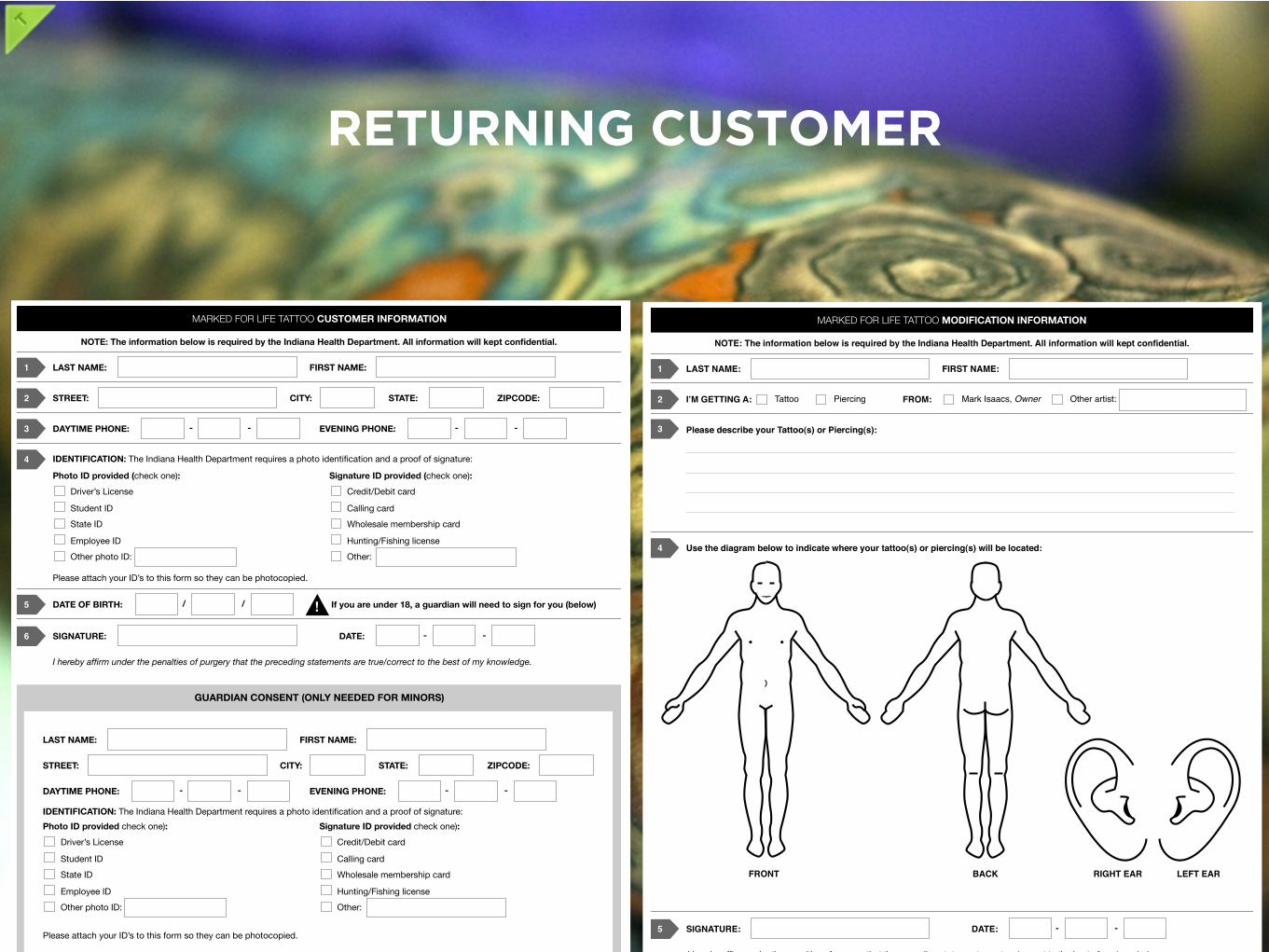
MARKED FOR LIFE TATTOO MODIFICATION INFORMATION
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
LAST NAME:1 FIRST NAME:
I!M GETTING A:2 Tattoo Piercing FROM: Mark Isaacs, Owner Other artist:
4 Use the diagram below to indicate where your tattoo(s) or piercing(s) will be located:
FRONT BACK RIGHT EAR LEFT EAR
SIGNATURE:5 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
GUARDIAN SIGNATURE: DATE: - -
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
3 Please describe your Tattoo(s) or Piercing(s):
MARKED FOR LIFE TATTOO CUSTOMER INFORMATION
LAST NAME:1 FIRST NAME:
STREET:2 CITY: STATE: ZIPCODE:
DAYTIME PHONE:3 EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:4
Photo ID provided (check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided (check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
SIGNATURE:6 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
DATE OF BIRTH:5 / / If you are under 18, a guardian will need to sign for you (below)!
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
LAST NAME: FIRST NAME:
STREET: CITY: STATE: ZIPCODE:
DAYTIME PHONE: EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:
Photo ID provided check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
GUARDIAN SIGNATURE: DATE: - -
DATE OF BIRTH: / /
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
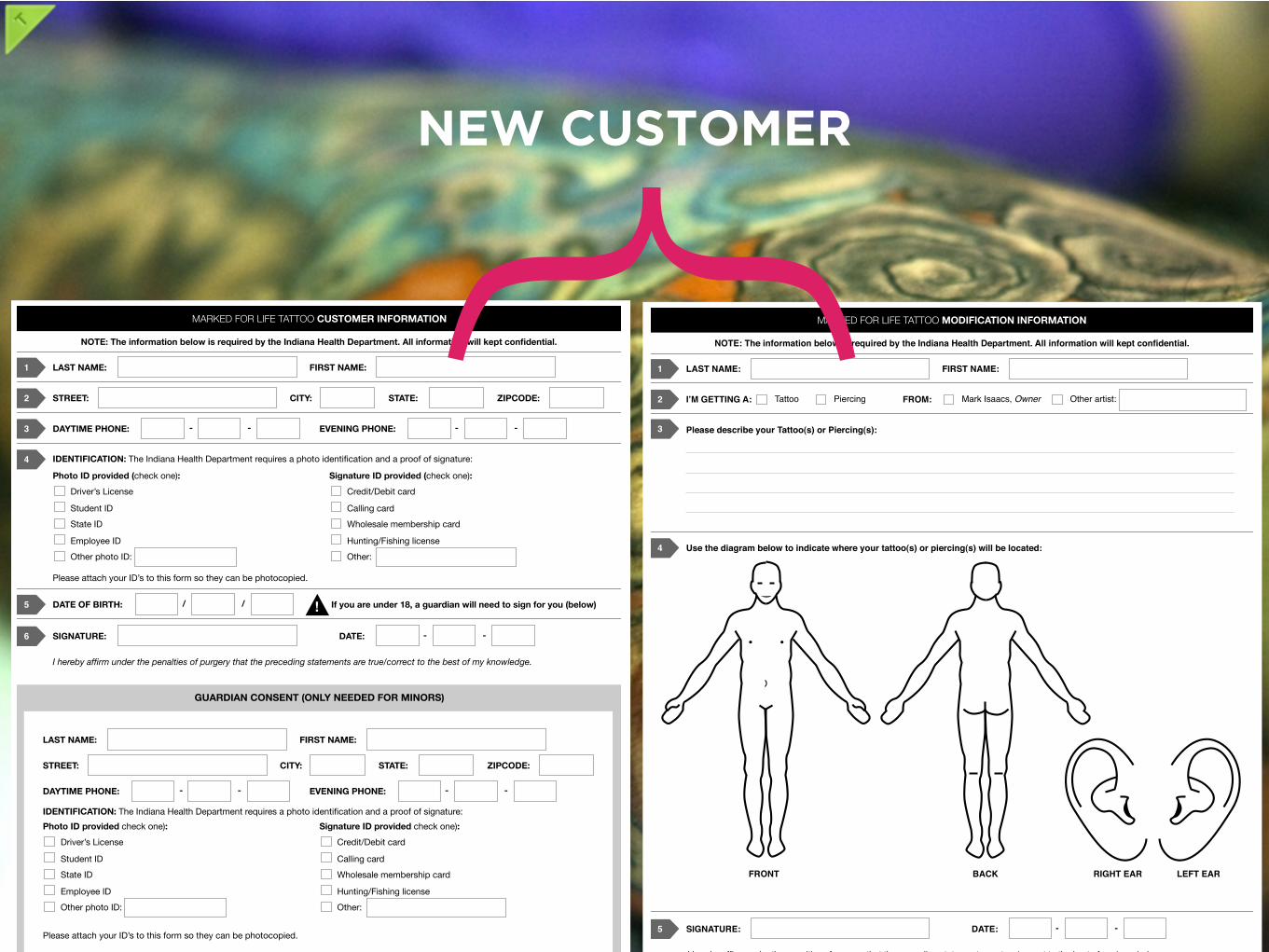
{NEW CUSTOMER
MARKED FOR LIFE TATTOO MODIFICATION INFORMATION
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
LAST NAME:1 FIRST NAME:
I!M GETTING A:2 Tattoo Piercing FROM: Mark Isaacs, Owner Other artist:
4 Use the diagram below to indicate where your tattoo(s) or piercing(s) will be located:
FRONT BACK RIGHT EAR LEFT EAR
SIGNATURE:5 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
GUARDIAN SIGNATURE: DATE: - -
By signing as the above minor’s legal guardian I take full responsibility for any legal issues that may take place in reference to the above
minor. Also by signing I give Marked for Life Tattoo consent to perform the above modification on the listed minor. I understand that I
must be present and sign for any future modifications while the above listed is under the legal age .
I affirm under the penalties of purgery that the foregoing statements are true/correct to the best of my knowledge.
3 Please describe your Tattoo(s) or Piercing(s):
MARKED FOR LIFE TATTOO CUSTOMER INFORMATION
LAST NAME:1 FIRST NAME:
STREET:2 CITY: STATE: ZIPCODE:
DAYTIME PHONE:3 EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:4
Photo ID provided (check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided (check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
SIGNATURE:6 DATE: - -
I hereby affirm under the penalties of purgery that the preceding statements are true/correct to the best of my knowledge.
DATE OF BIRTH:5 / / If you are under 18, a guardian will need to sign for you (below)!
GUARDIAN CONSENT (ONLY NEEDED FOR MINORS)
LAST NAME: FIRST NAME:
STREET: CITY: STATE: ZIPCODE:
DAYTIME PHONE: EVENING PHONE:- - - -
IDENTIFICATION: The Indiana Health Department requires a photo identification and a proof of signature:
Photo ID provided check one):
Driver’s License
Student ID
State ID
Employee ID
Other photo ID:
Signature ID provided check one):
Credit/Debit card
Calling card
Wholesale membership card
Hunting/Fishing license
Other:
Please attach your ID’s to this form so they can be photocopied.
NOTE: The information below is required by the Indiana Health Department. All information will kept confidential.
RETURNING CUSTOMER

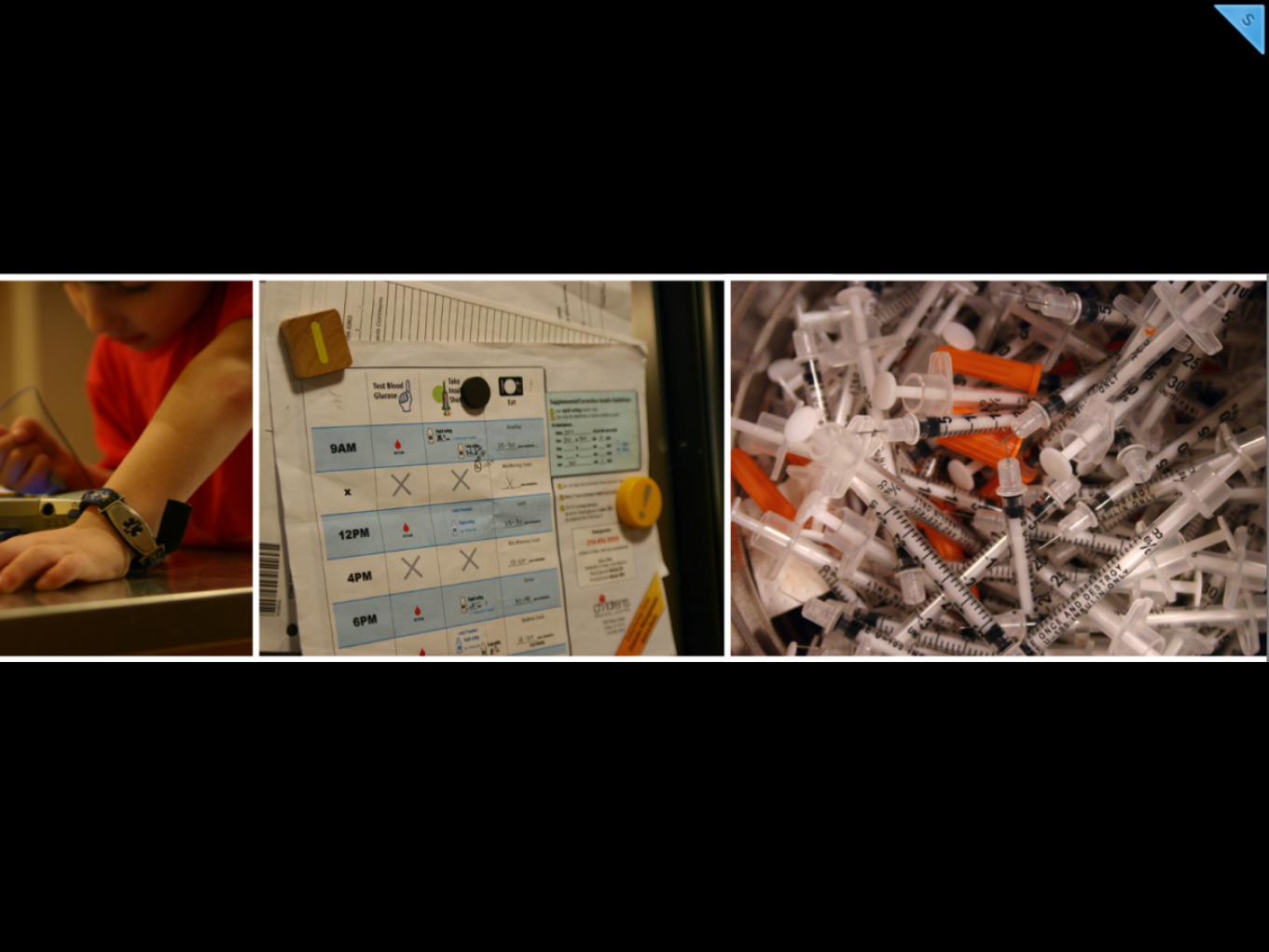
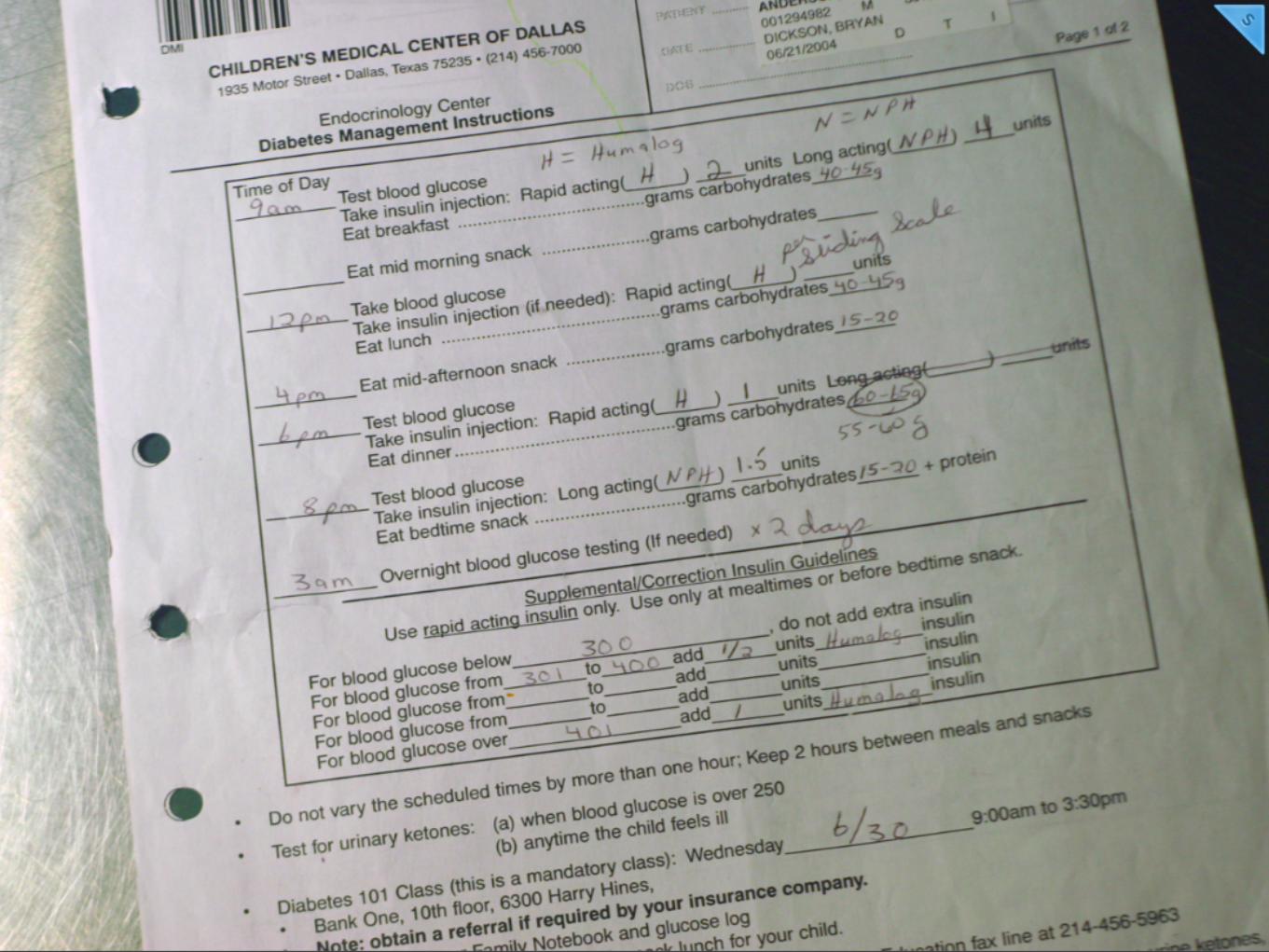
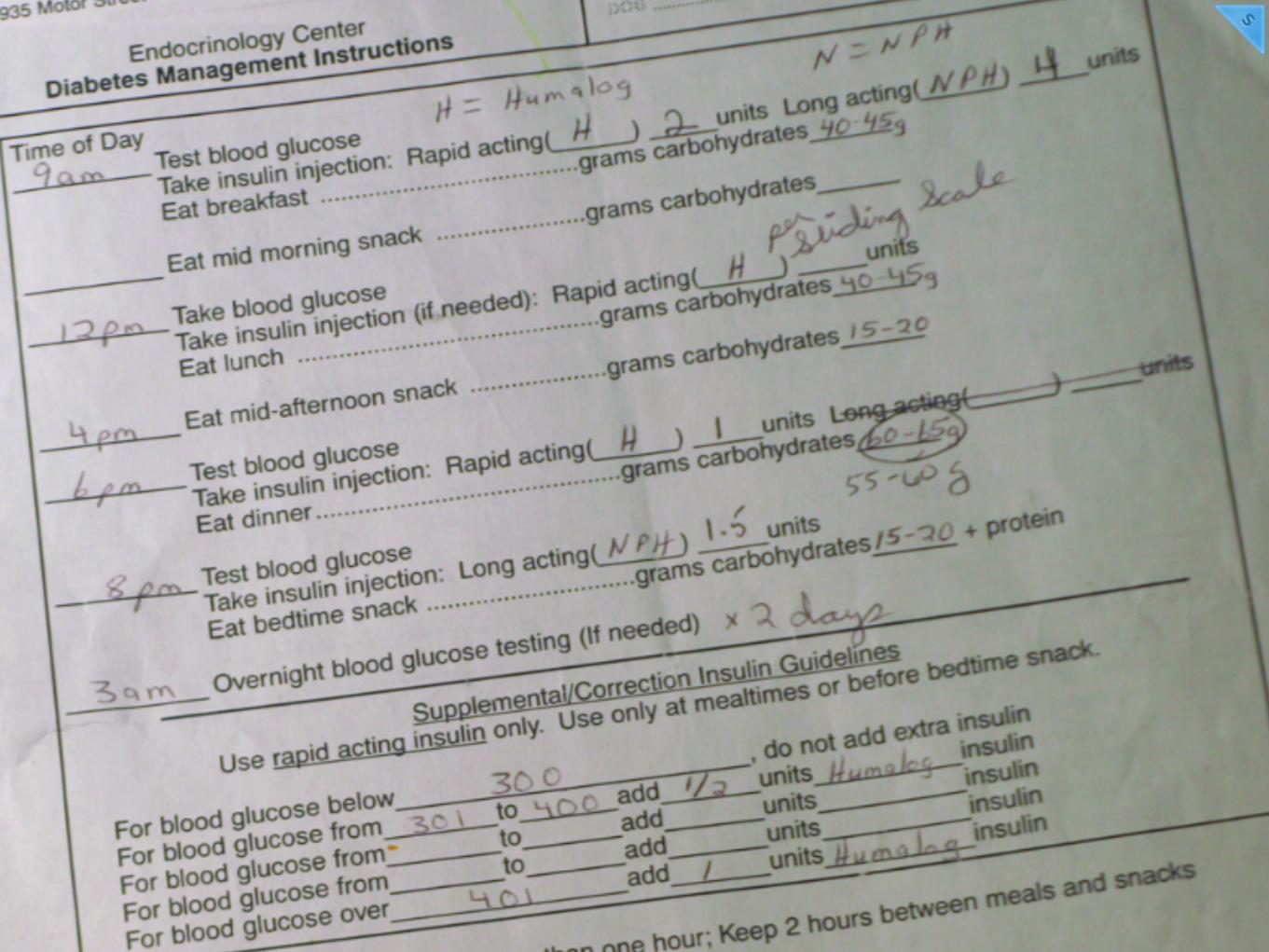
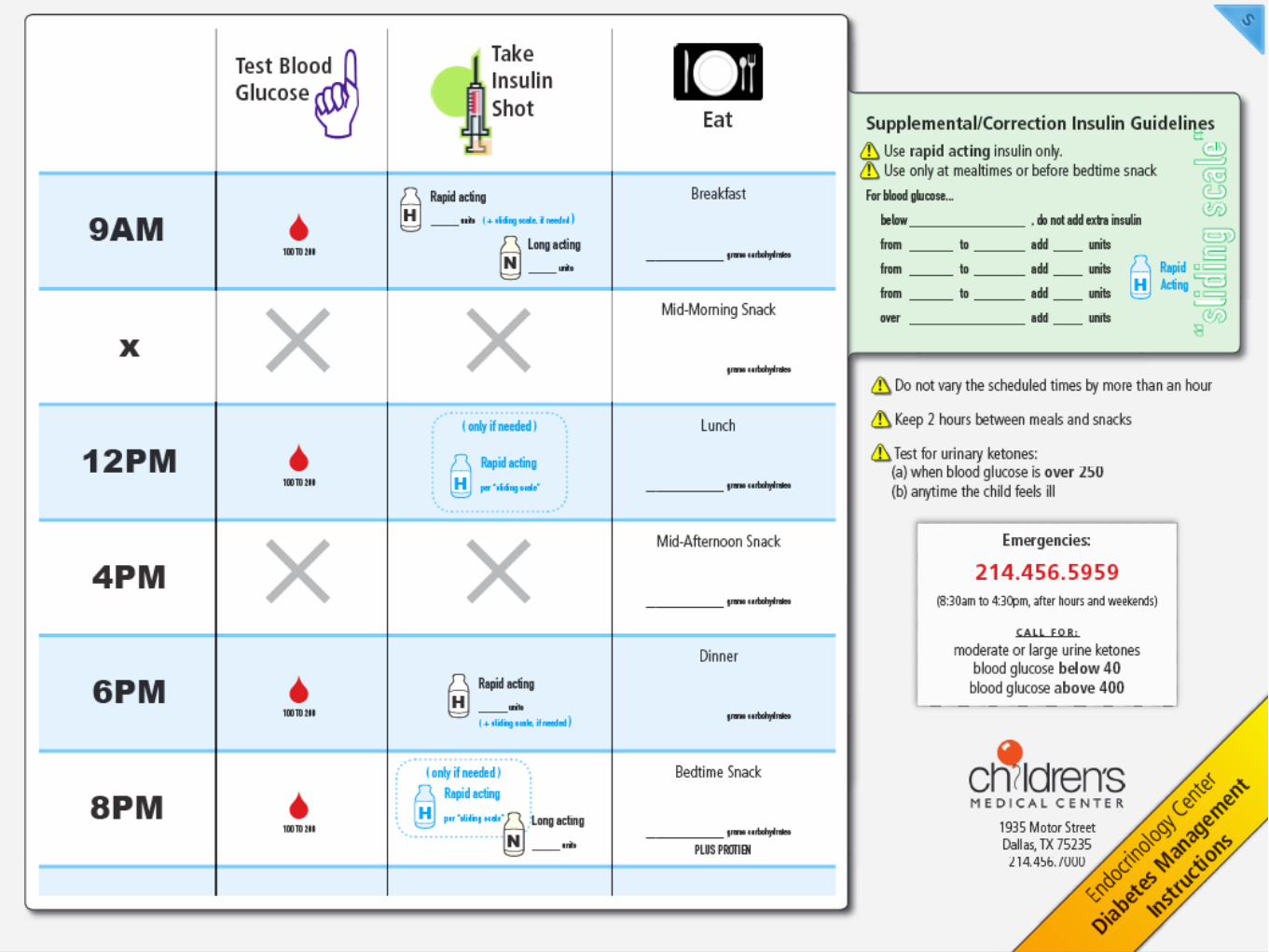
In June 2004, my 4-year-old son was diagnosed with Type I Diabetes...

SHOPPING FOR A DIGITAL CAMERA
http://picasaweb.google.com/buddah.425/SingaporeHolidayJuly2007/photo#5095105074289463458
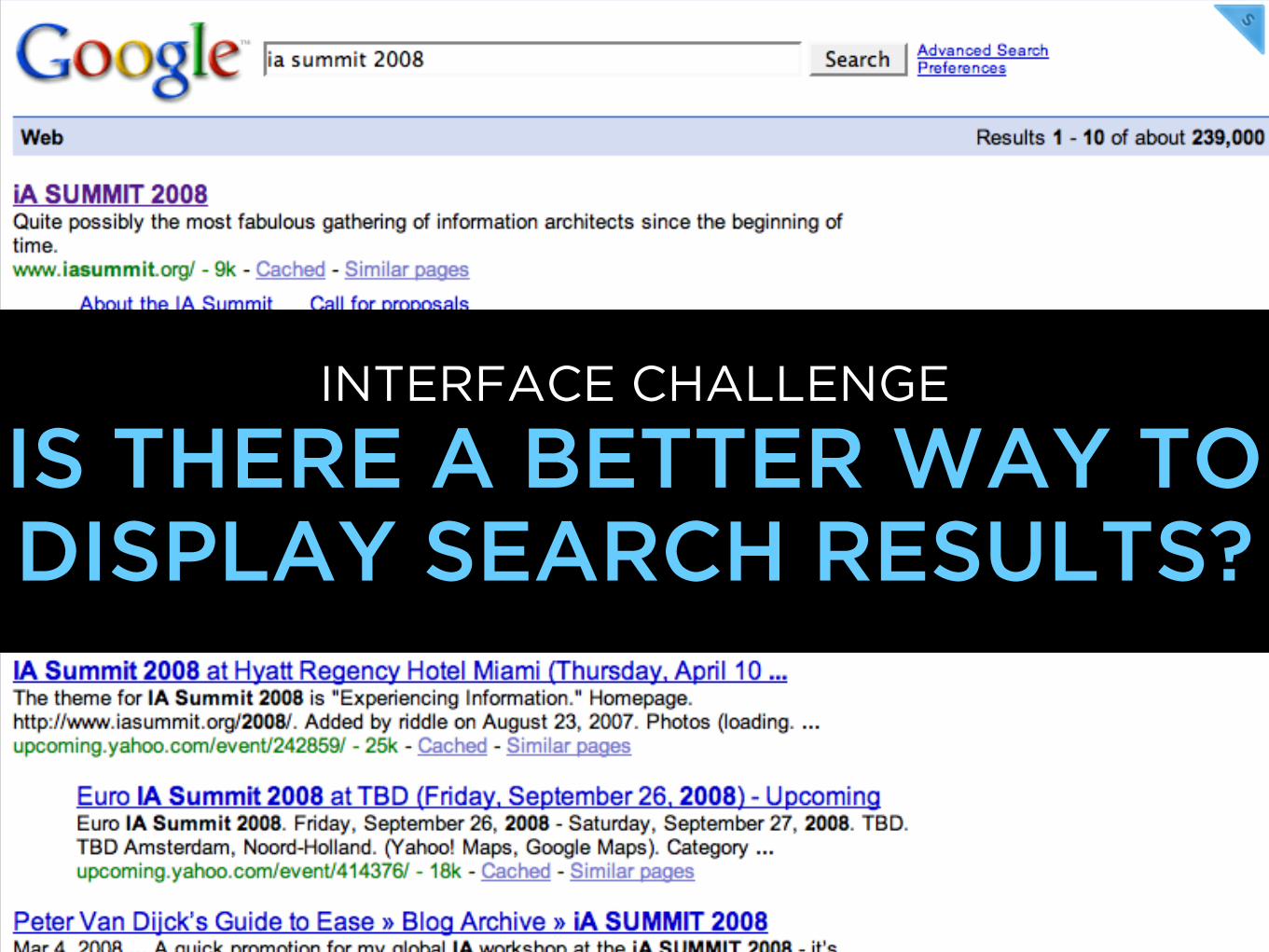
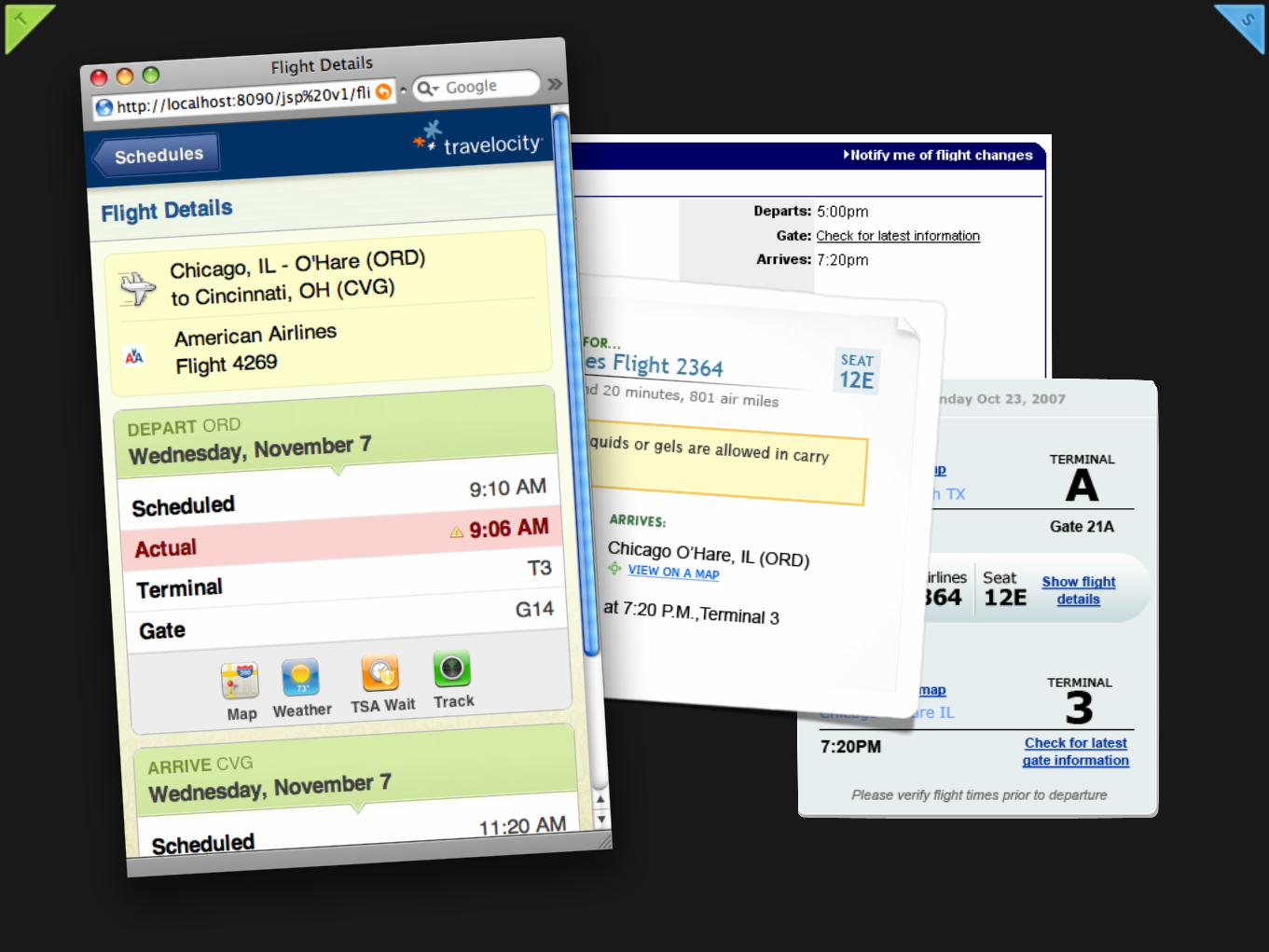
INTERFACE CHALLENGE
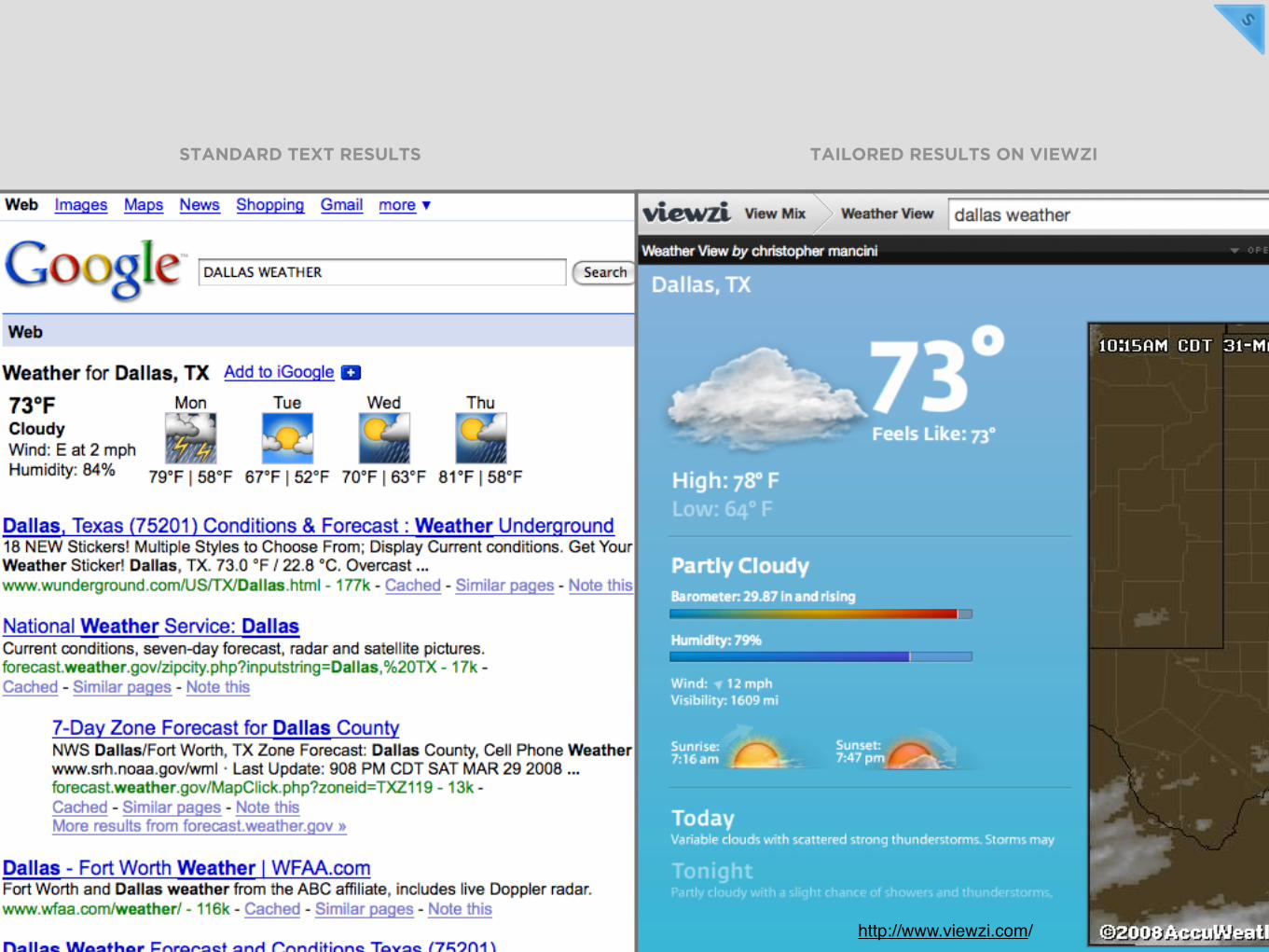
IS THERE A BETTER WAY TO DISPLAY SEARCH RESULTS?
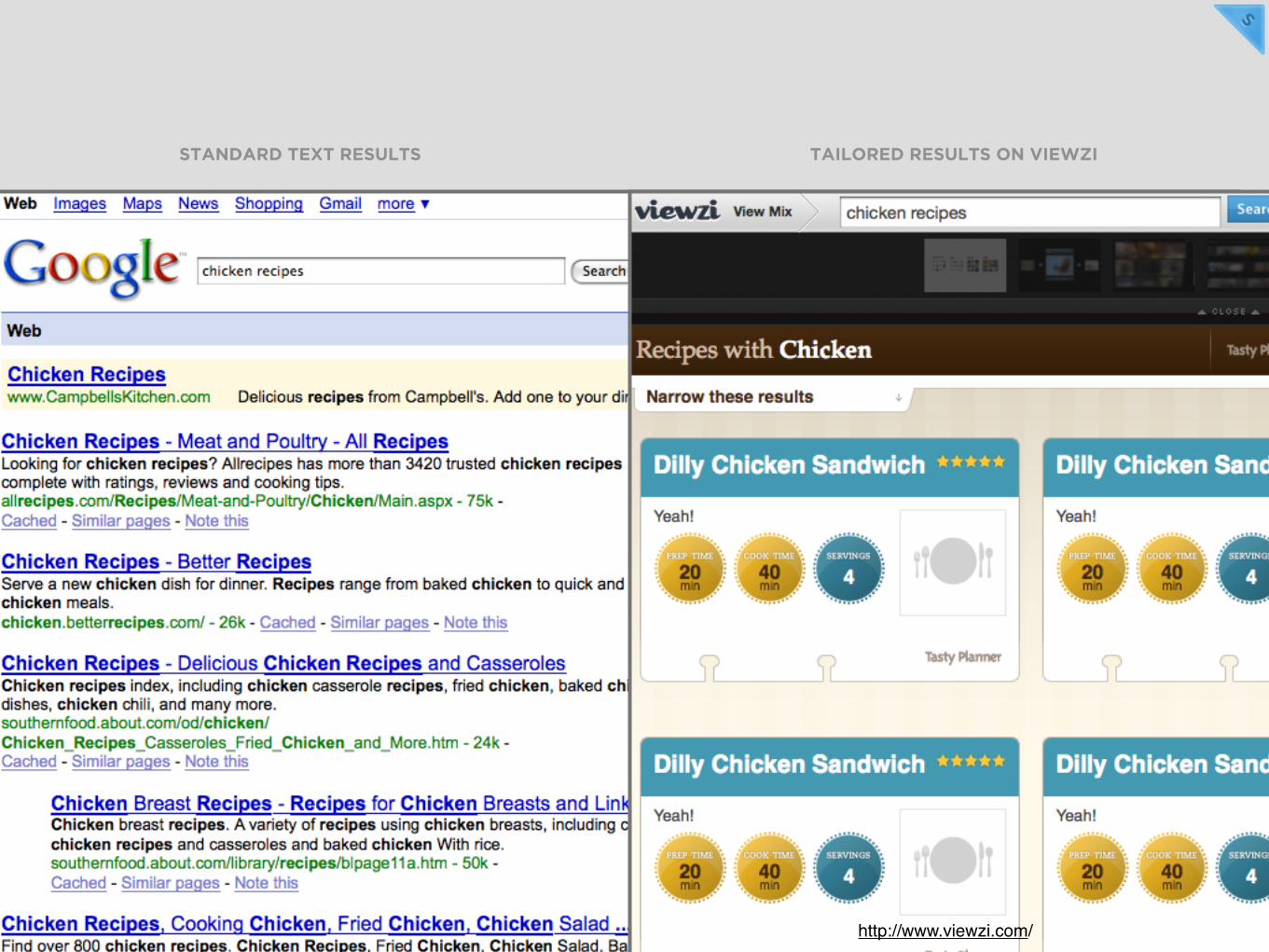
STANDARD TEXT RESULTS TAILORED RESULTS ON VIEWZI
http://www.viewzi.com/
http://www.viewzi.com/
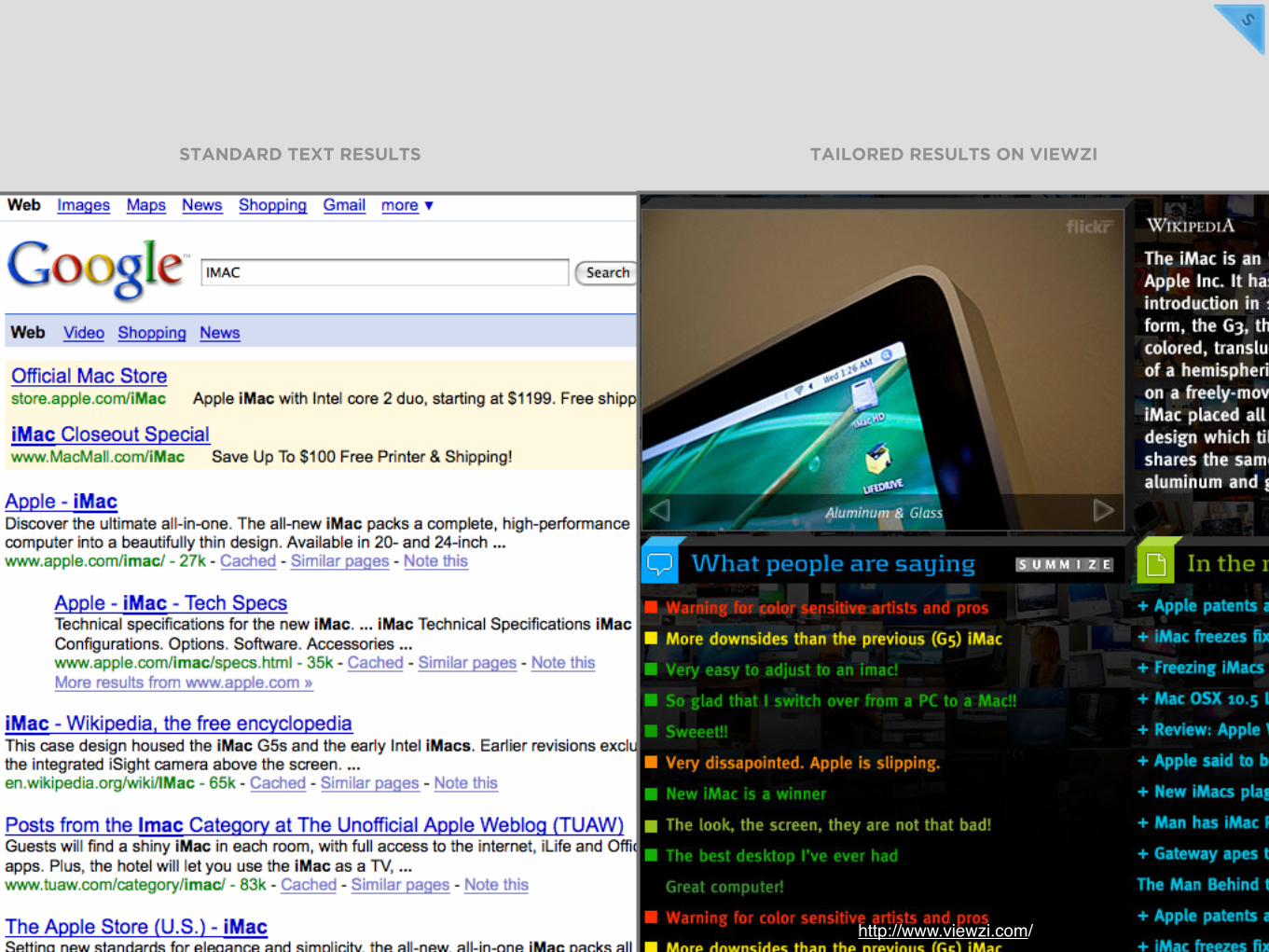
STANDARD TEXT RESULTS TAILORED RESULTS ON VIEWZI
http://www.viewzi.com/
STANDARD TEXT RESULTS TAILORED RESULTS ON VIEWZI

SHOPPING FOR A DIGITAL CAMERA
http://picasaweb.google.com/buddah.425/SingaporeHolidayJuly2007/photo#5095105074289463458

My shopping patterns...
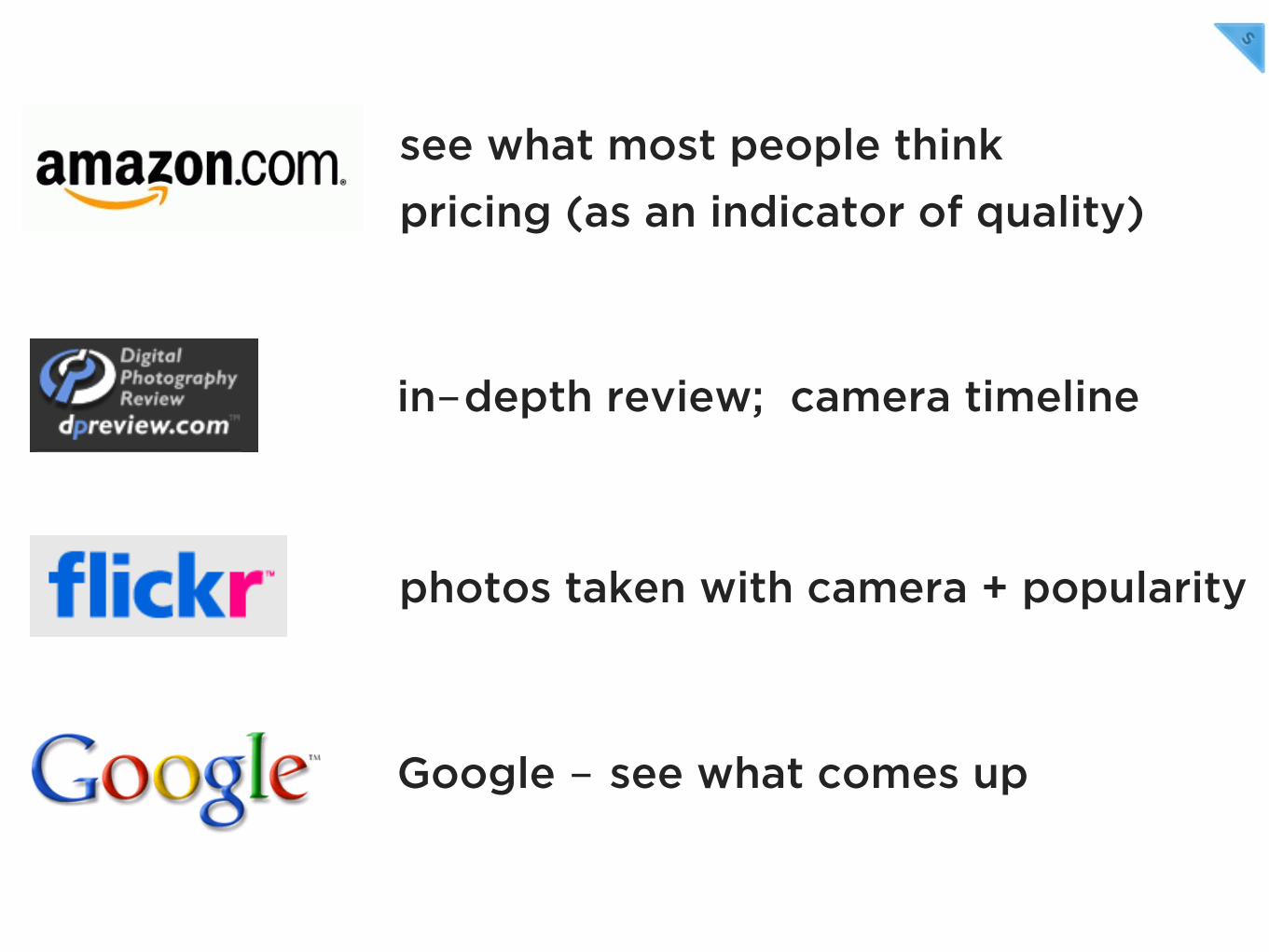
Google - see what comes up
see what most people think
in-depth review; camera timeline
photos taken with camera + popularity
pricing (as an indicator of quality)
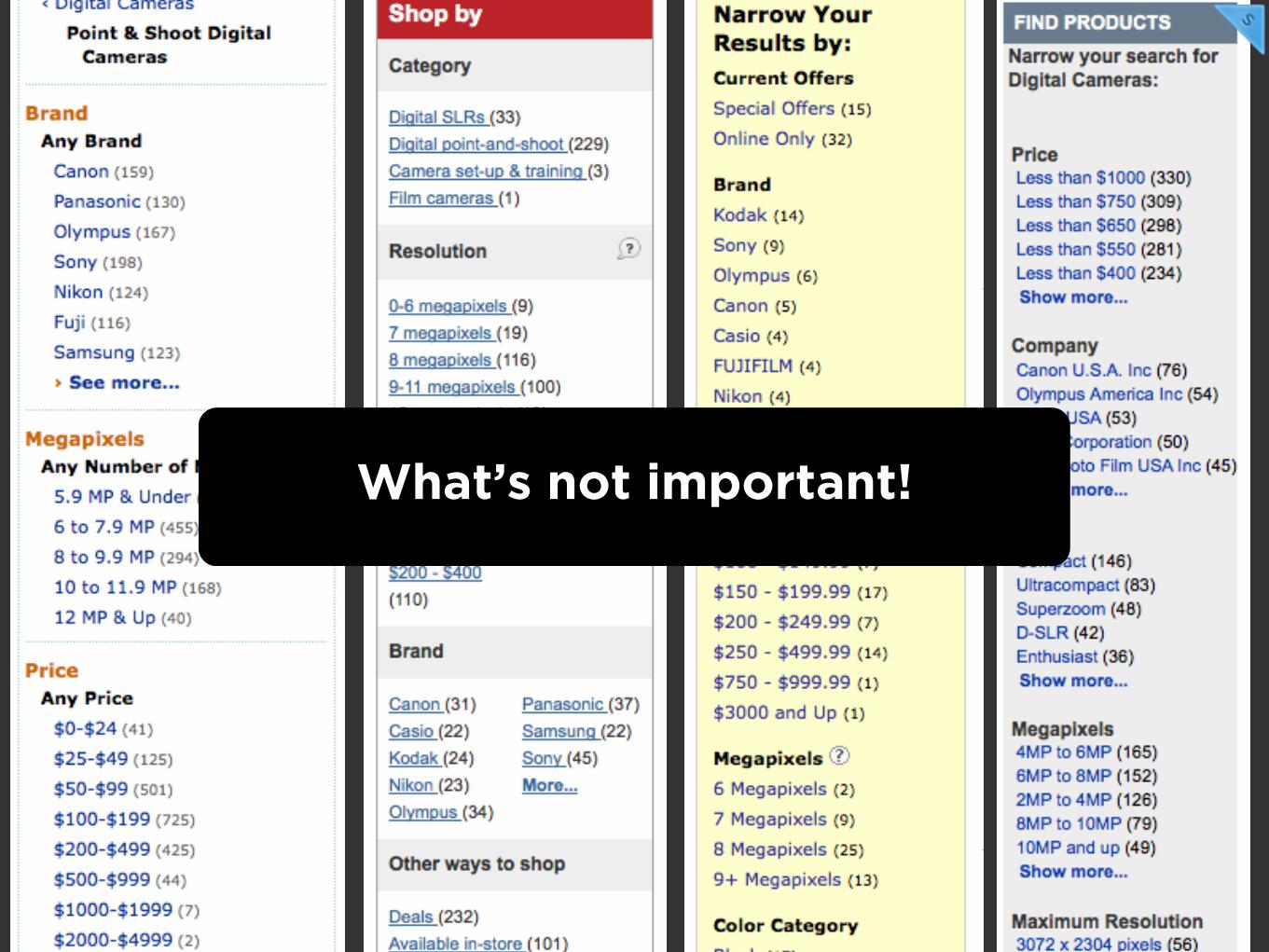
What’s not important!
cameras older than ‘x’ years!
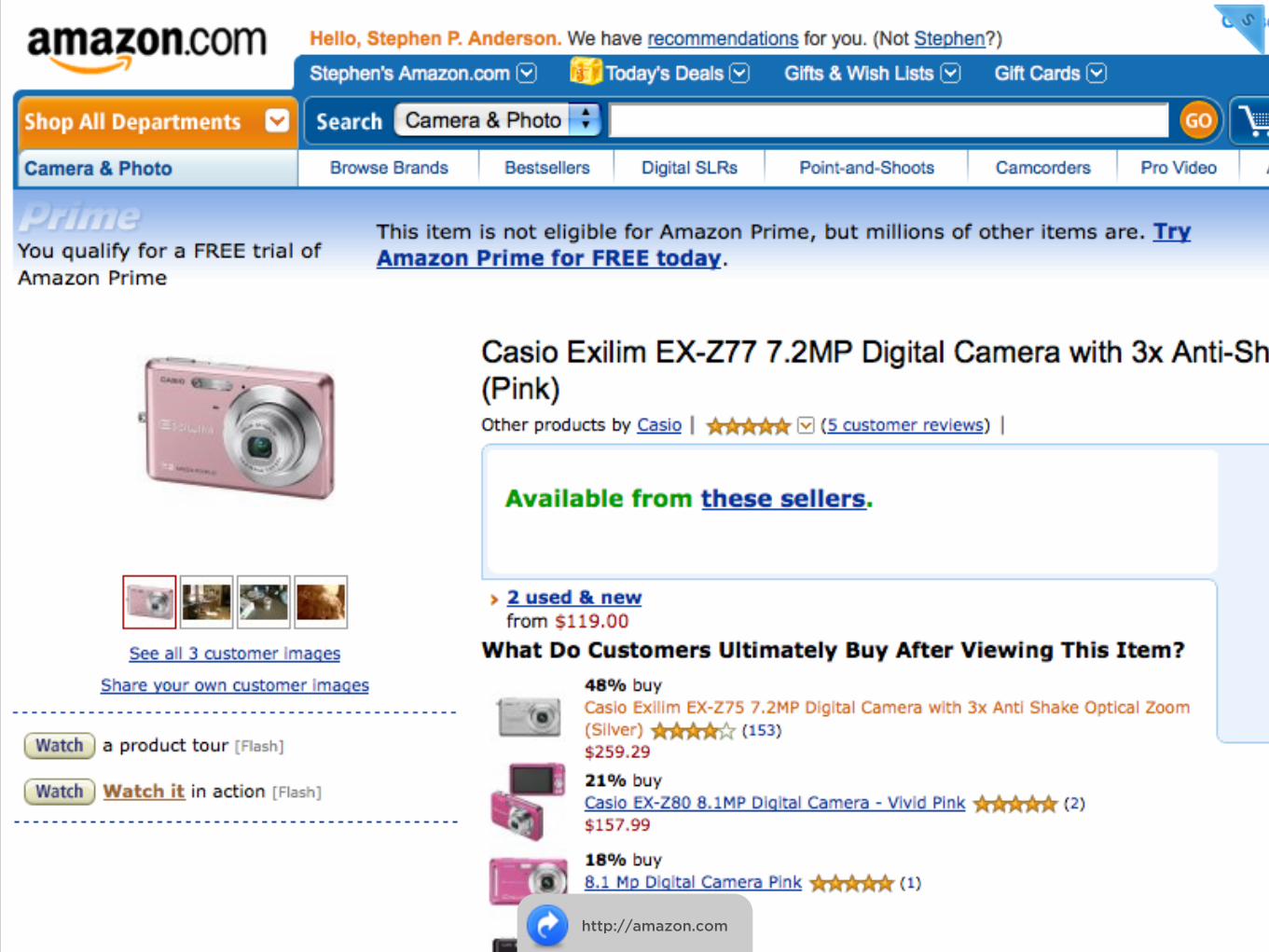
http://amazon.com
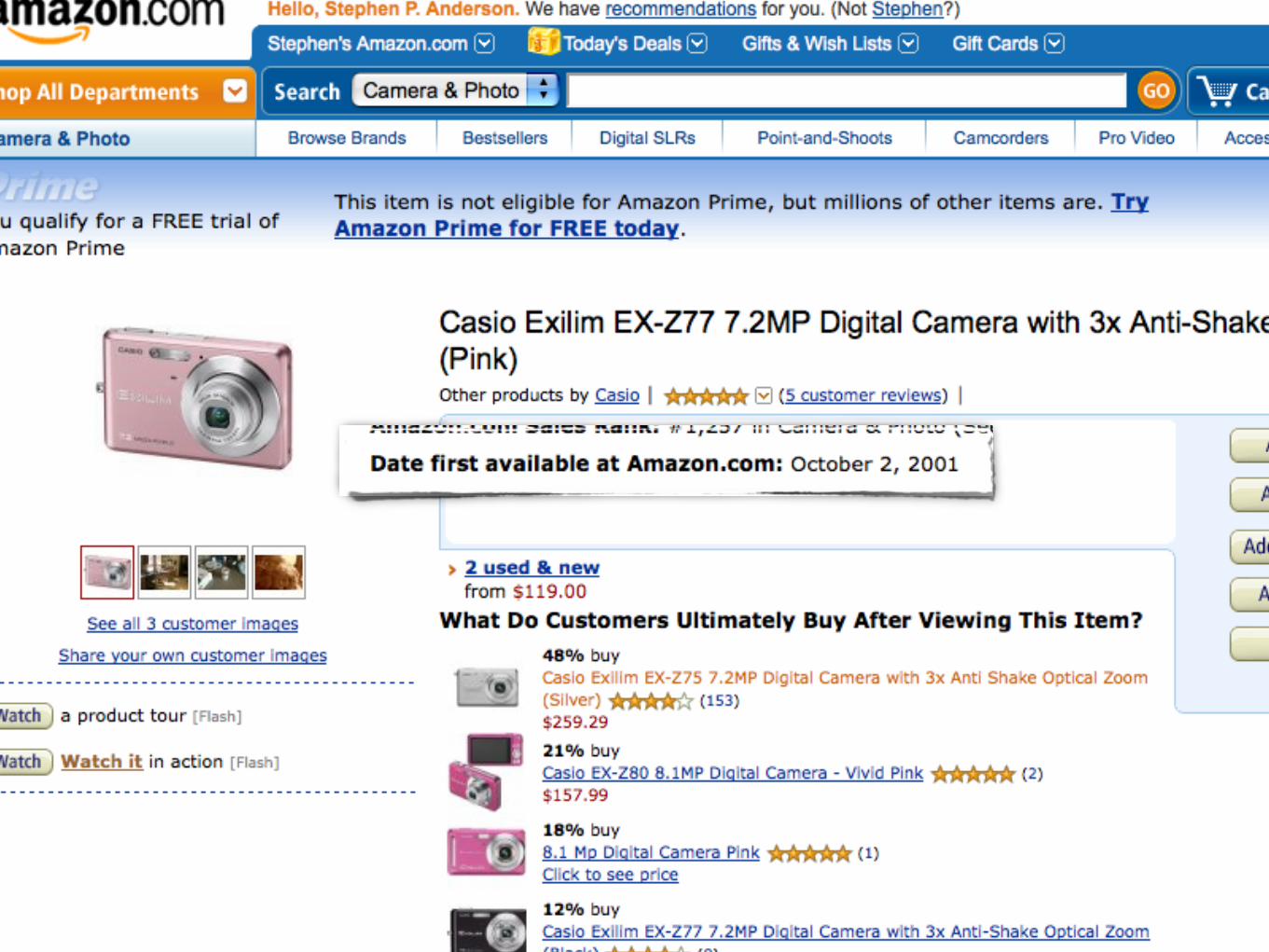

Inspiration!
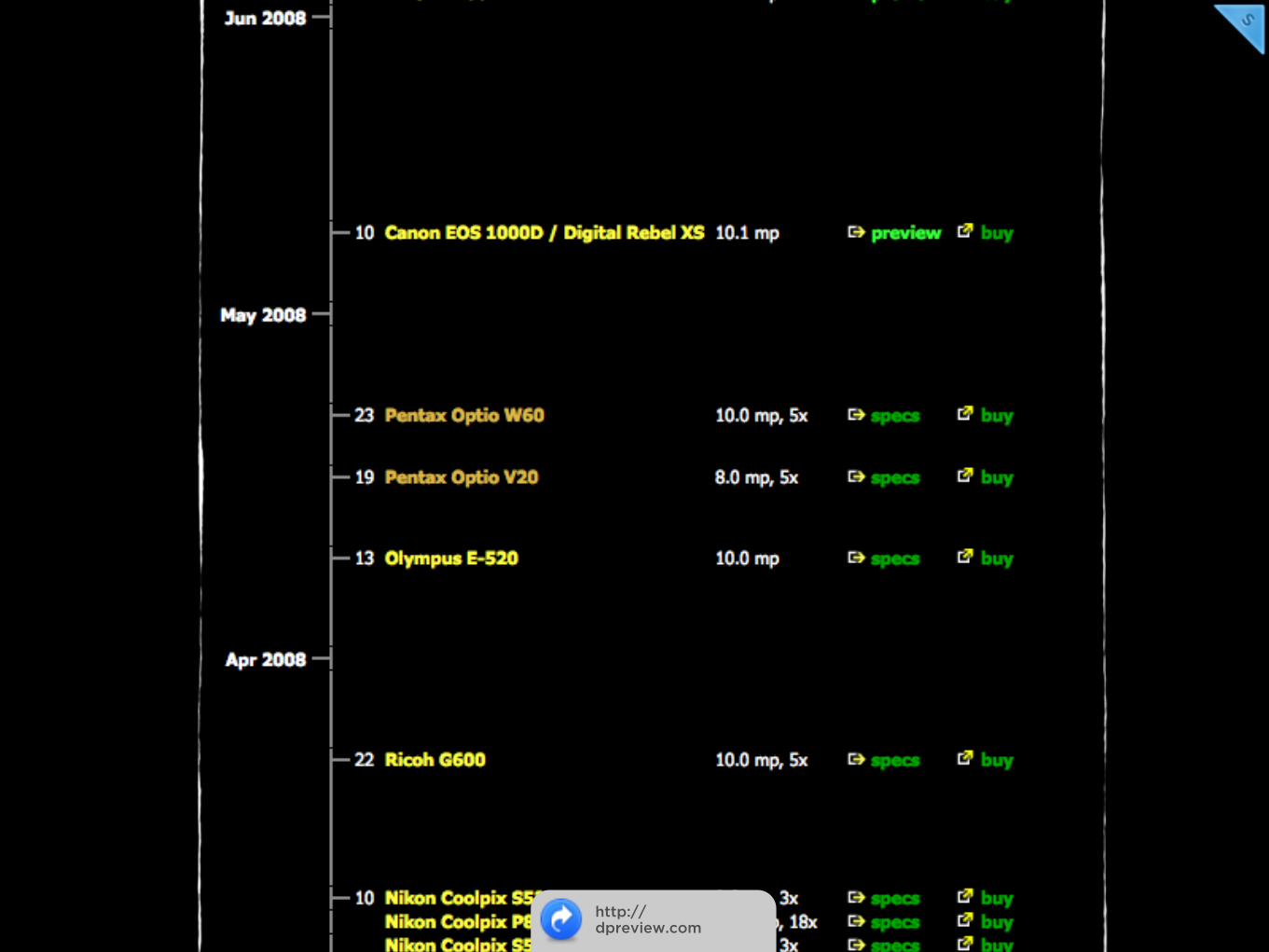
http://dpreview.com

http://viewzi.com
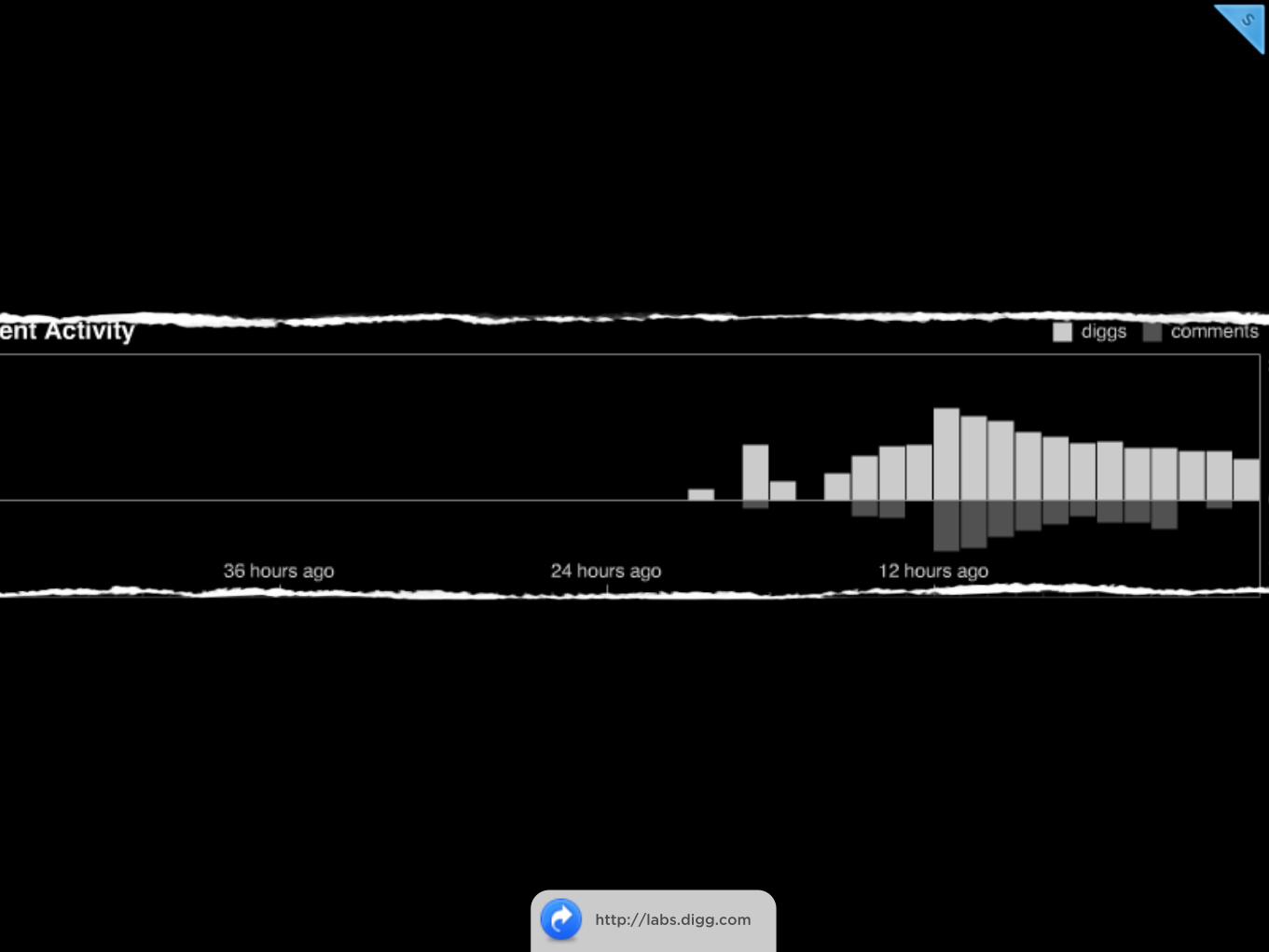
http://labs.digg.com
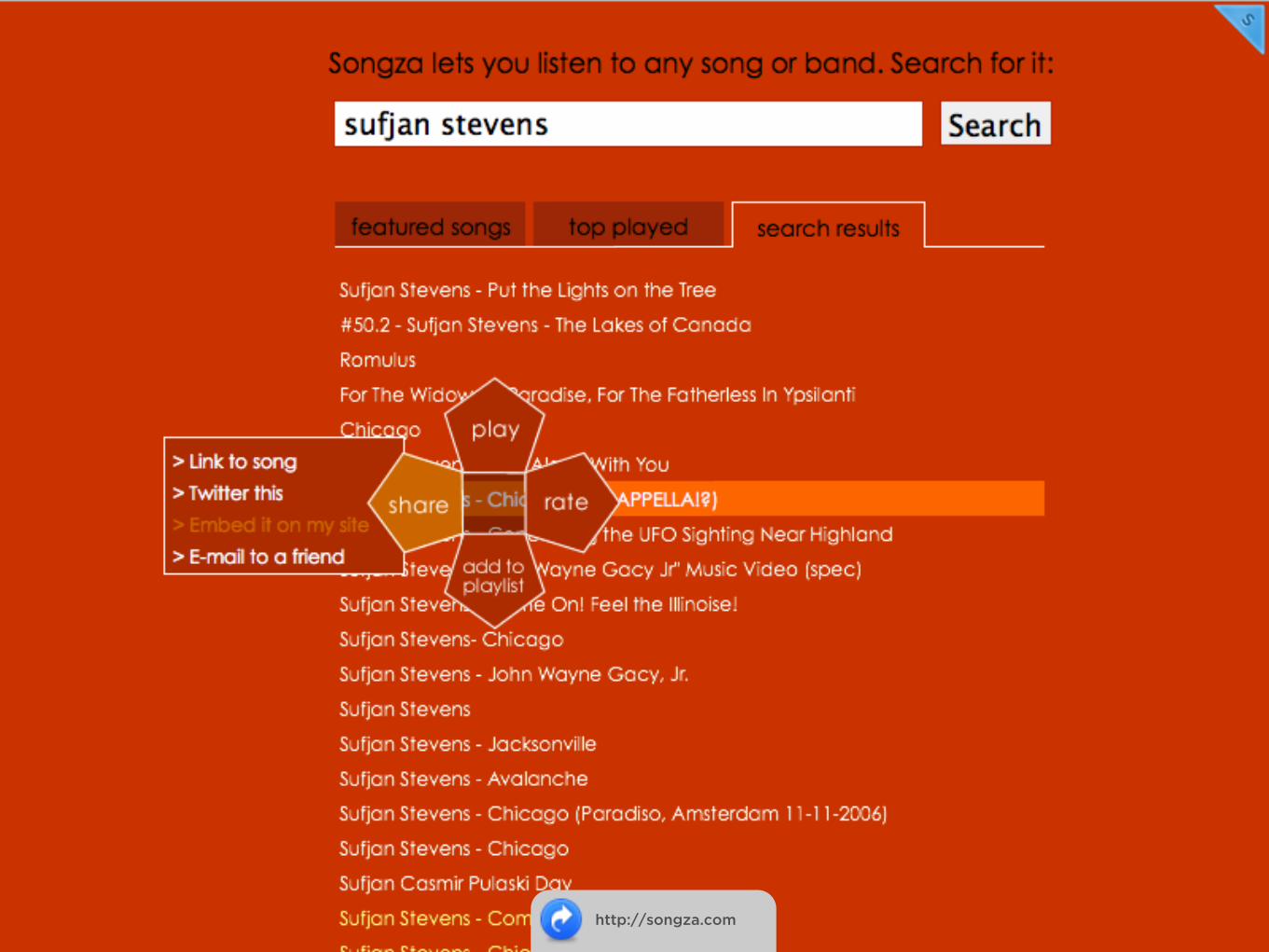
http://songza.com
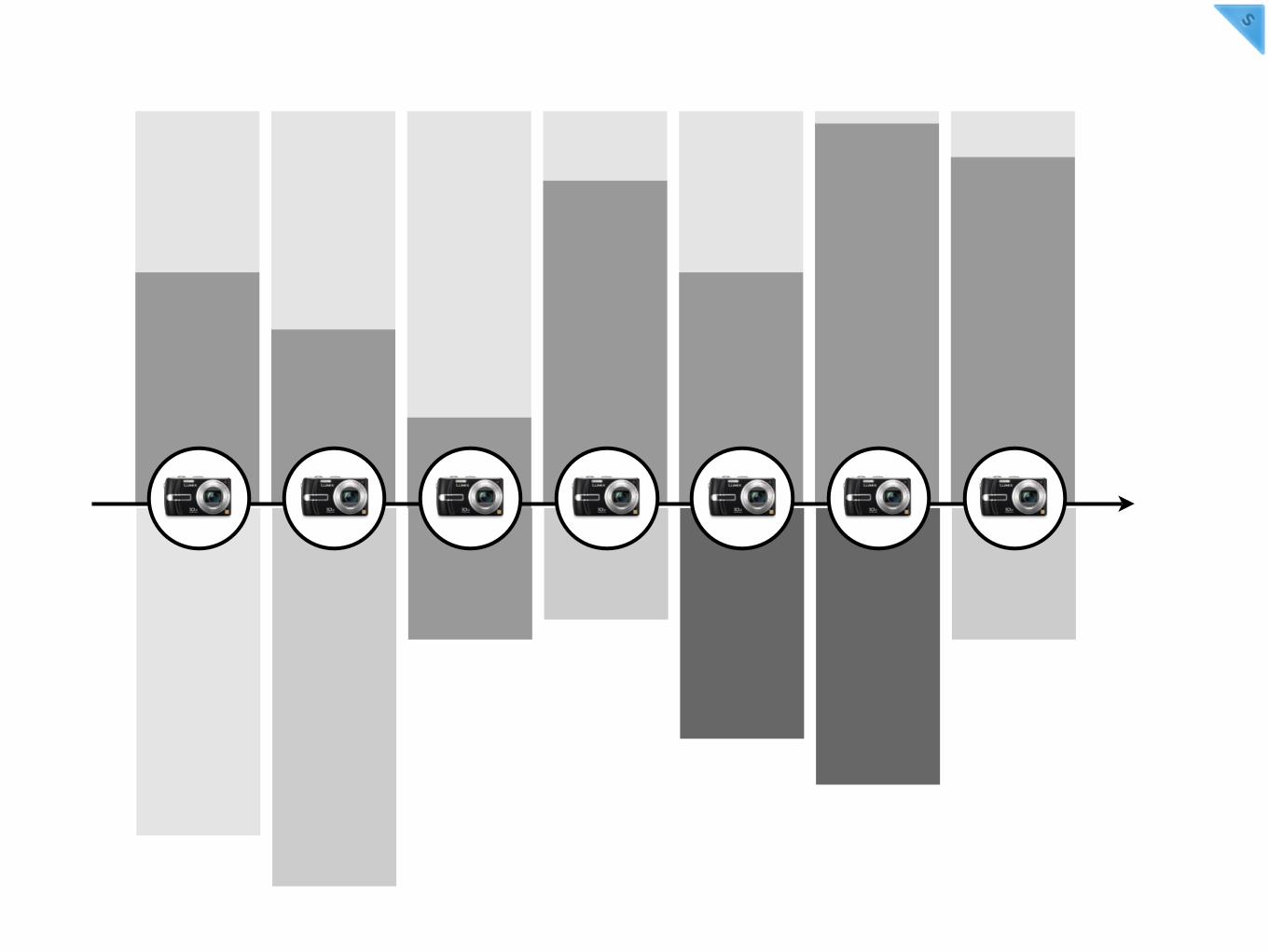

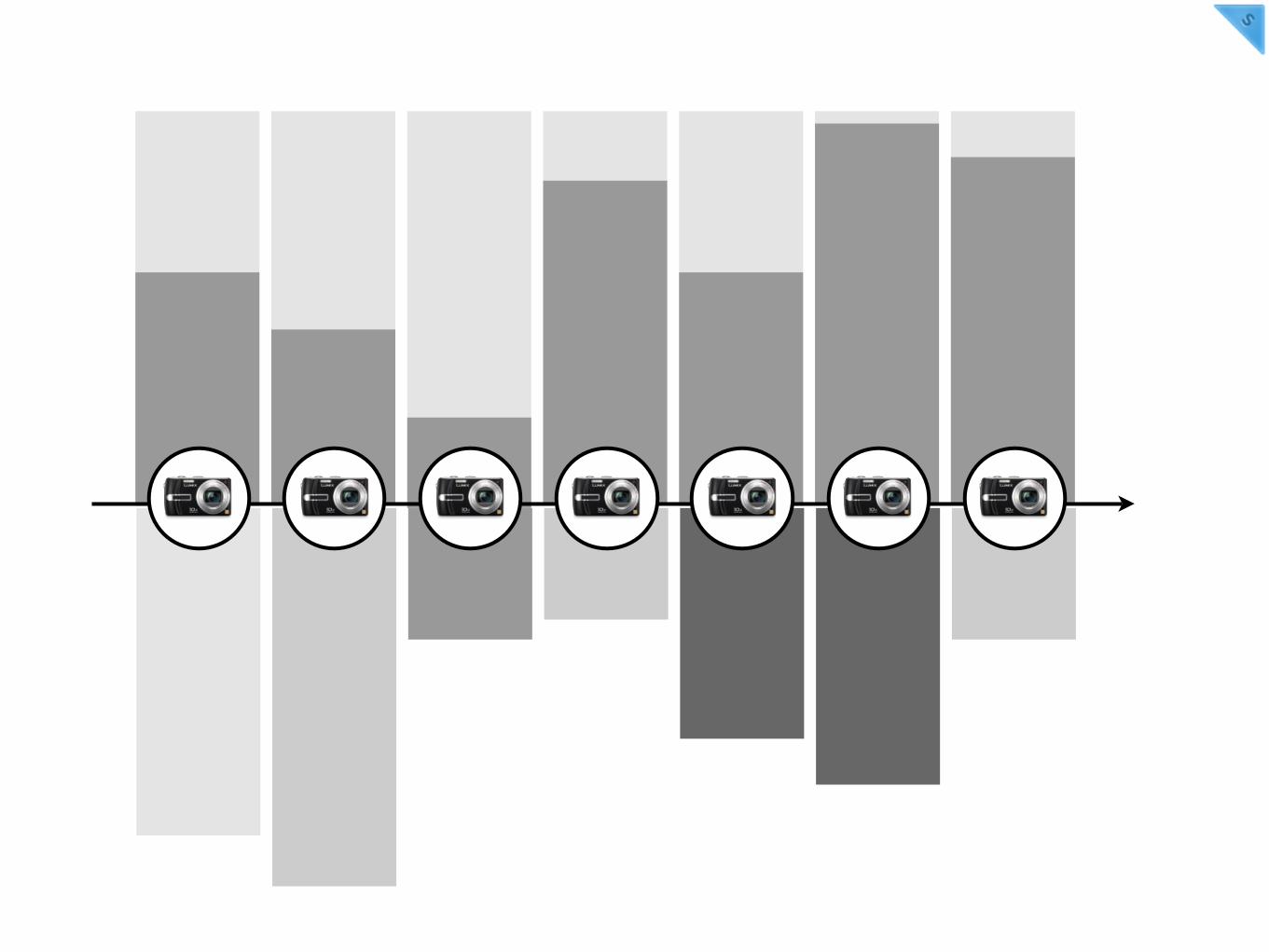
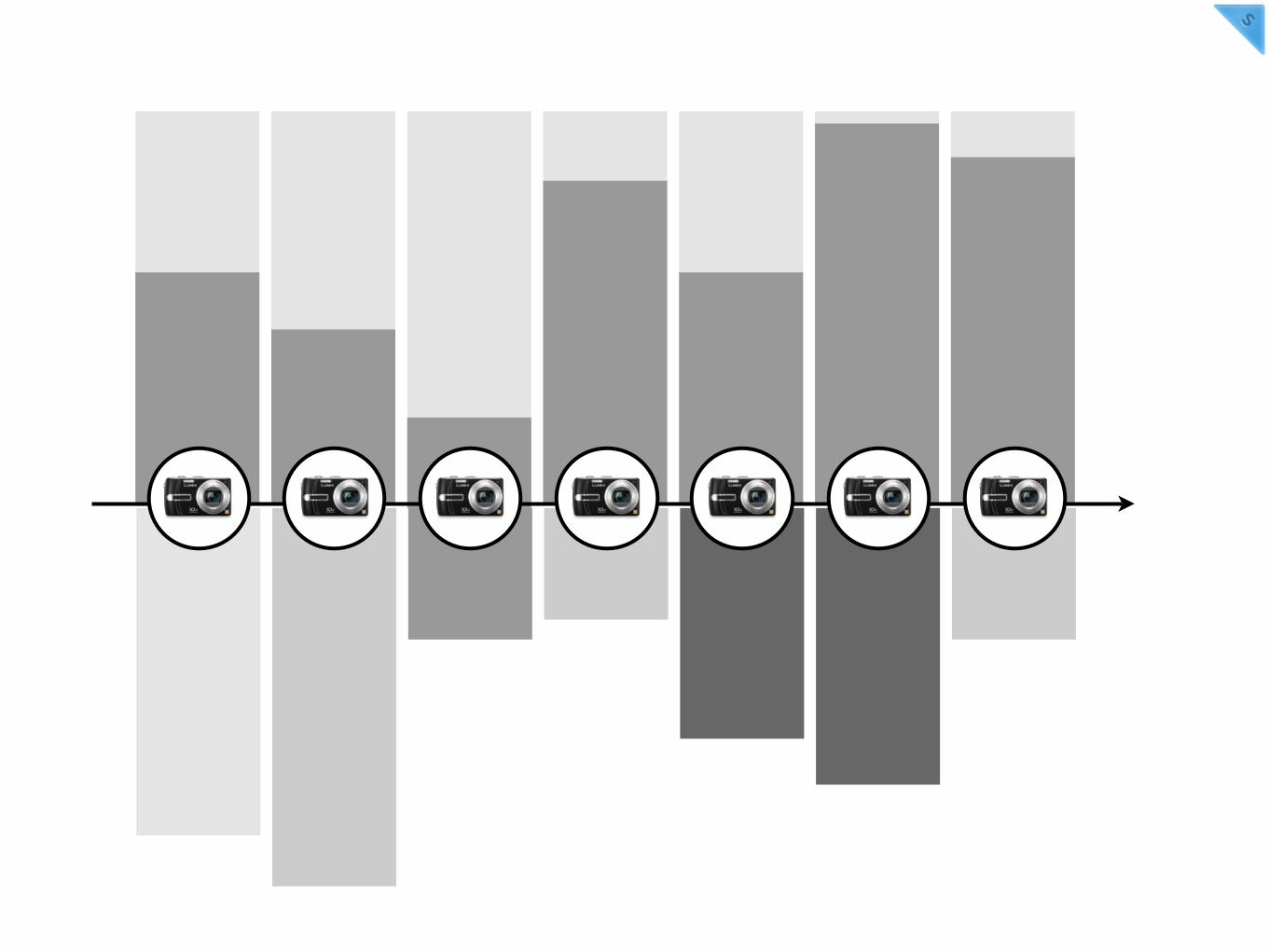
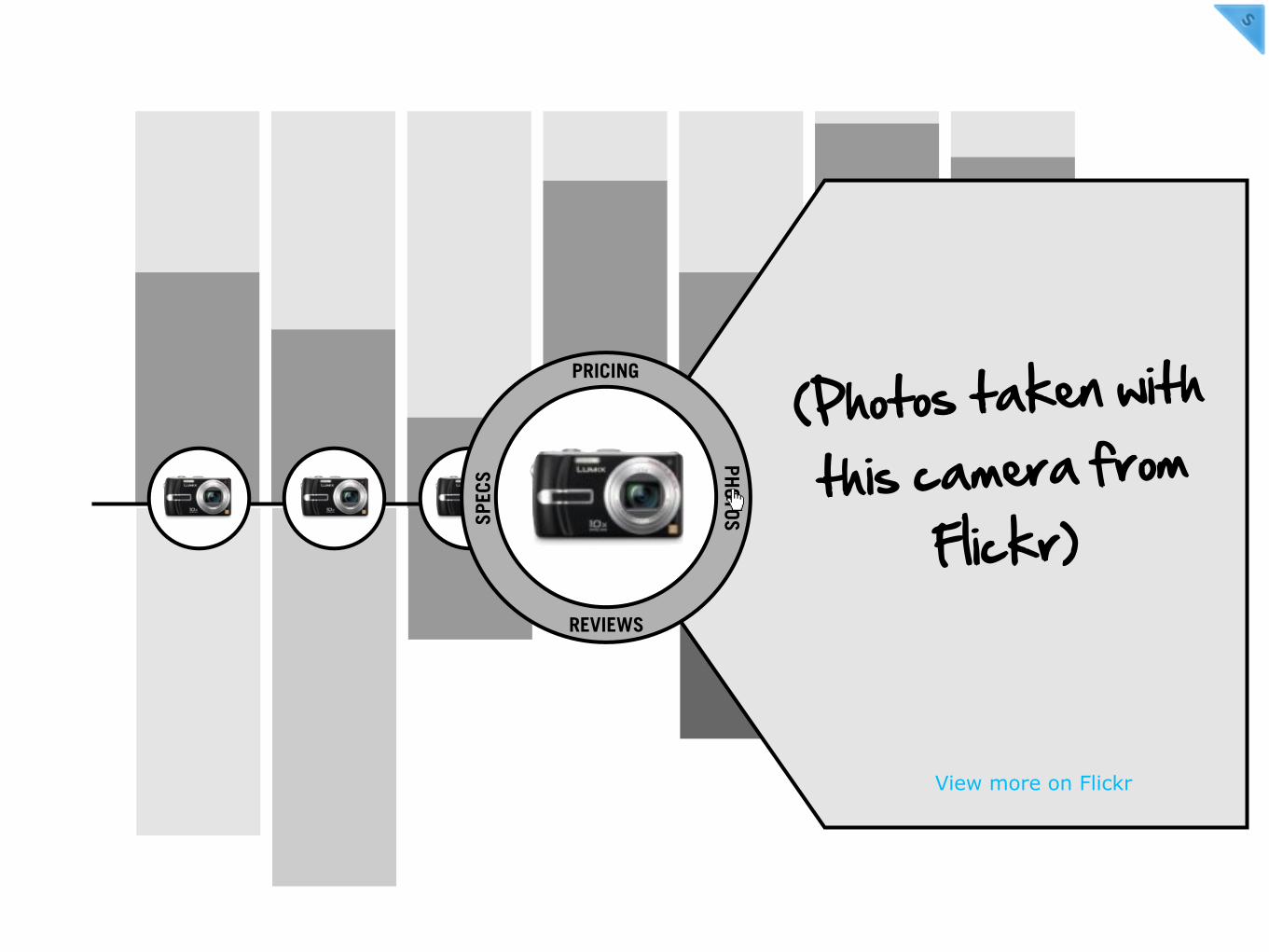
Results arranged on a
timelineOLDER NEWEST
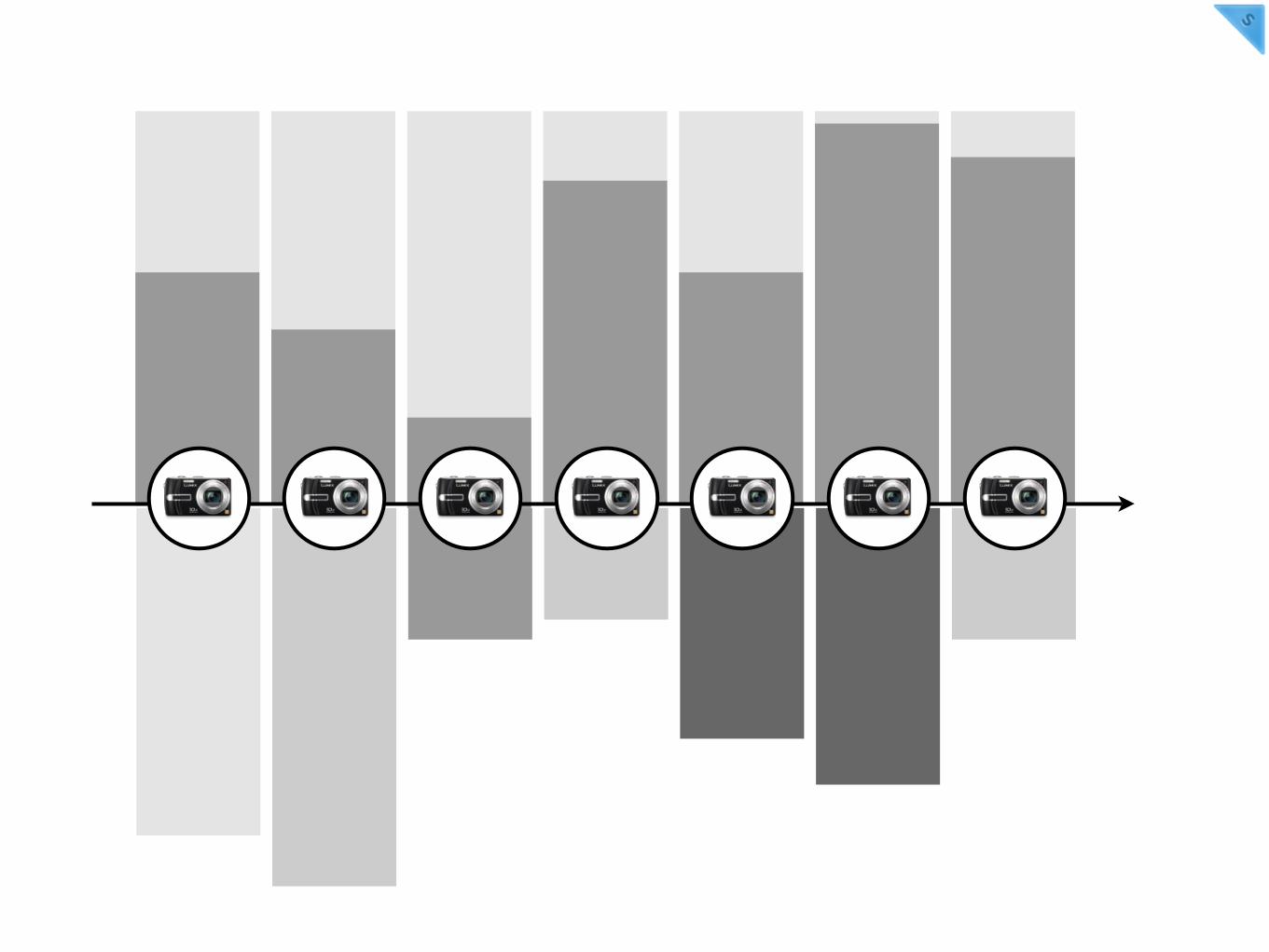
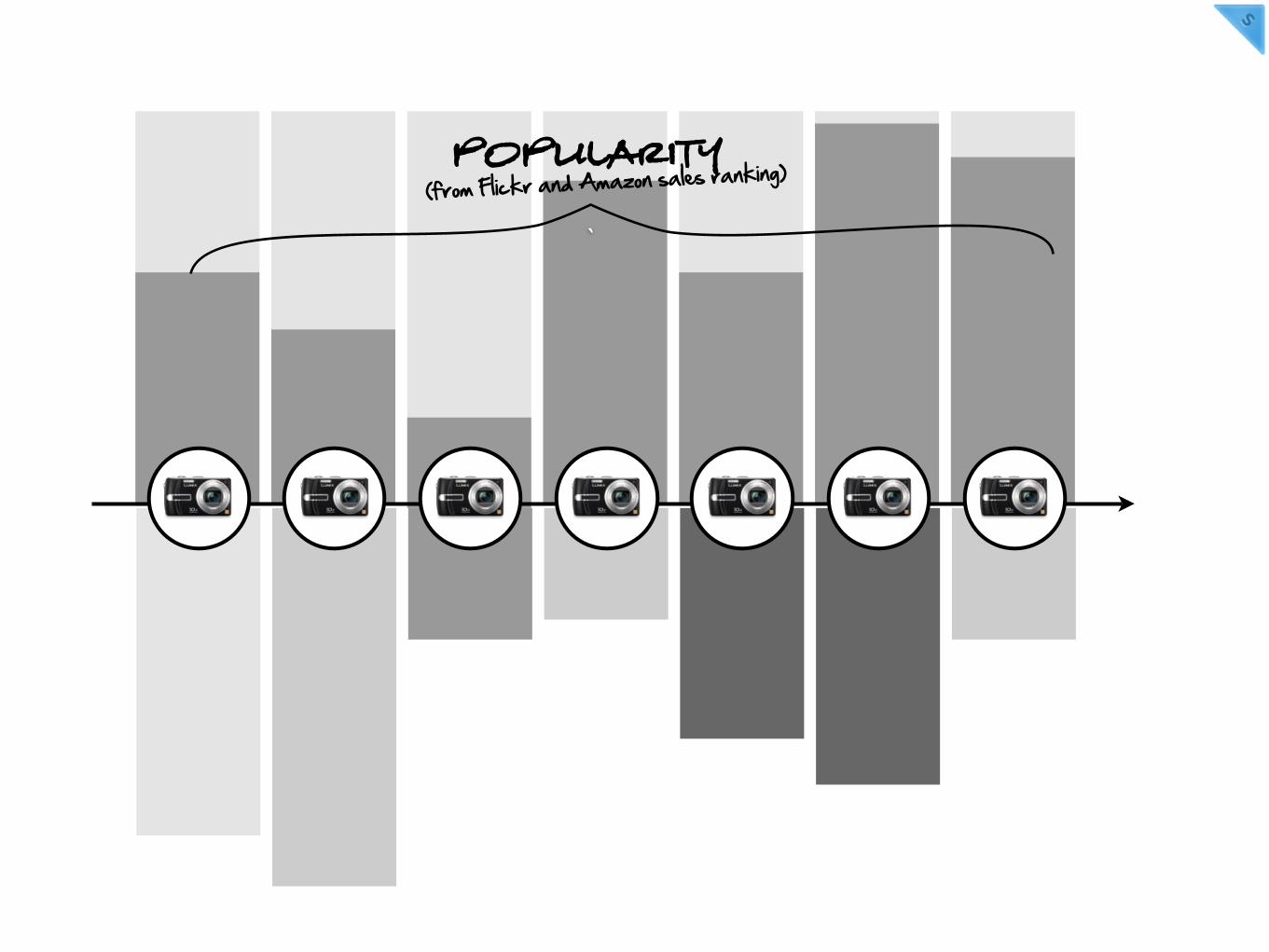
(from Flickr and Amazon sales ranking)POPULARITY
`
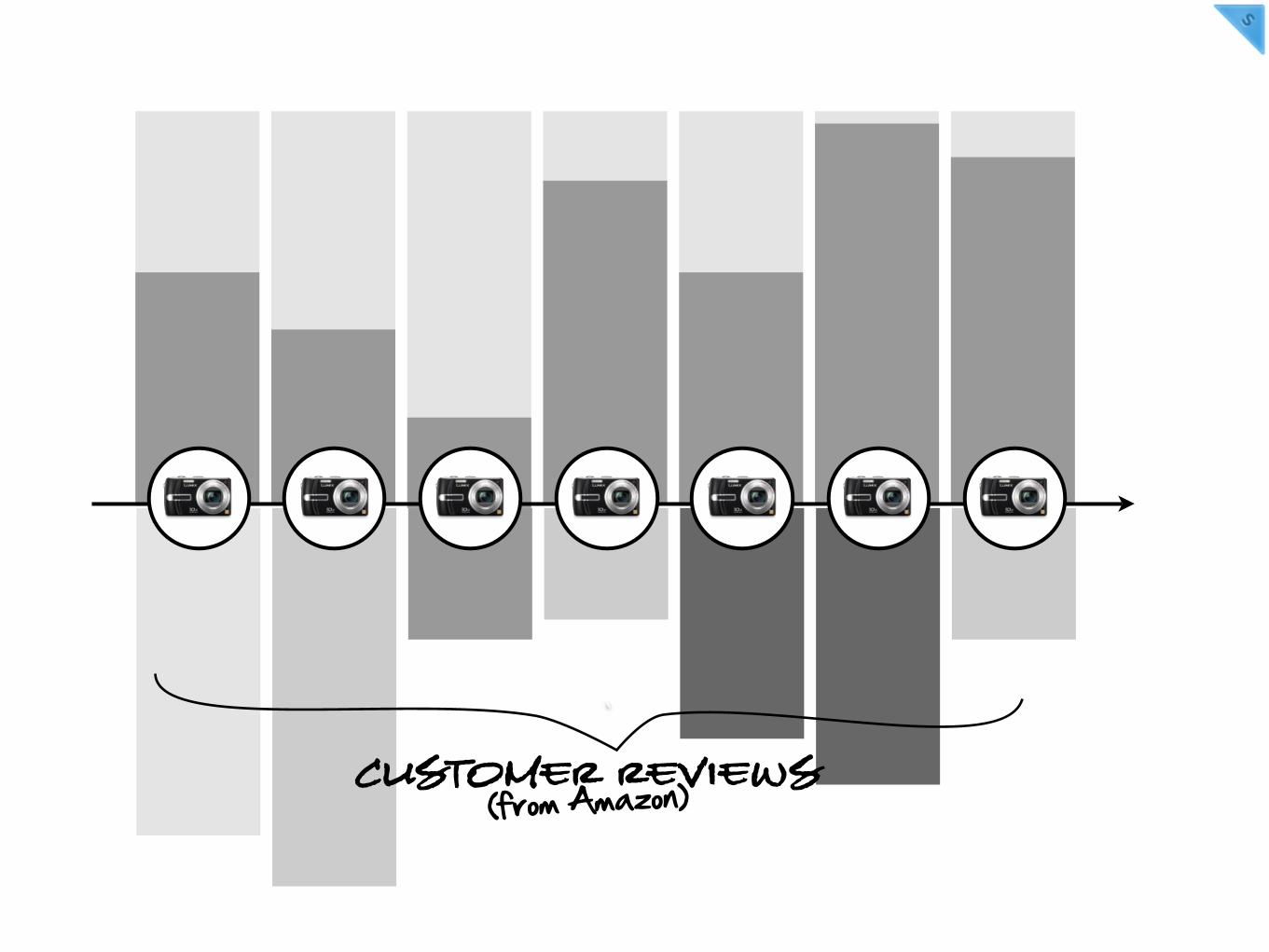
(from Amazon)Customer Reviews`
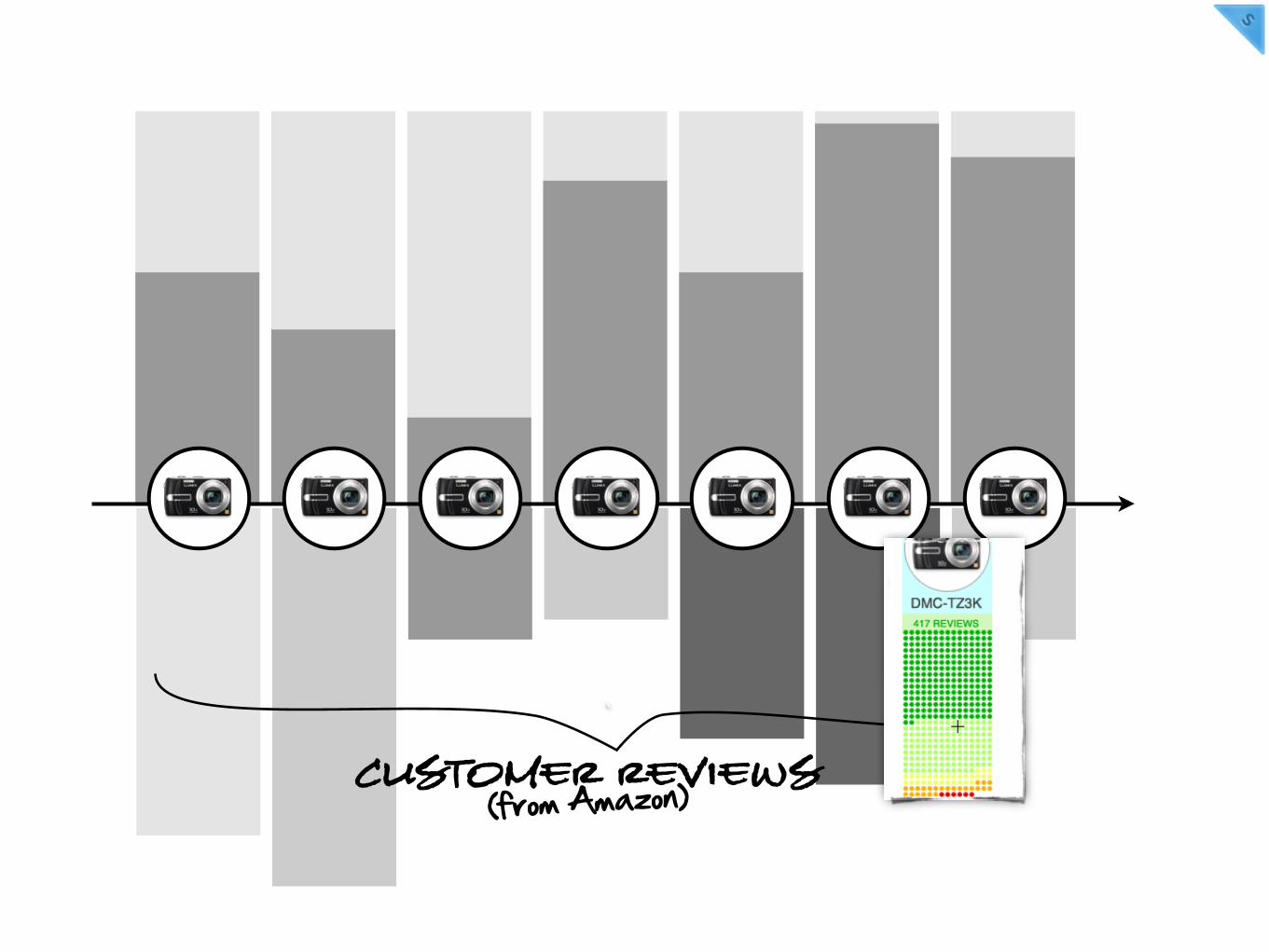
(from Amazon)Customer Reviews`
REVIEWS
PRICING
SPECS
PH
OTOS
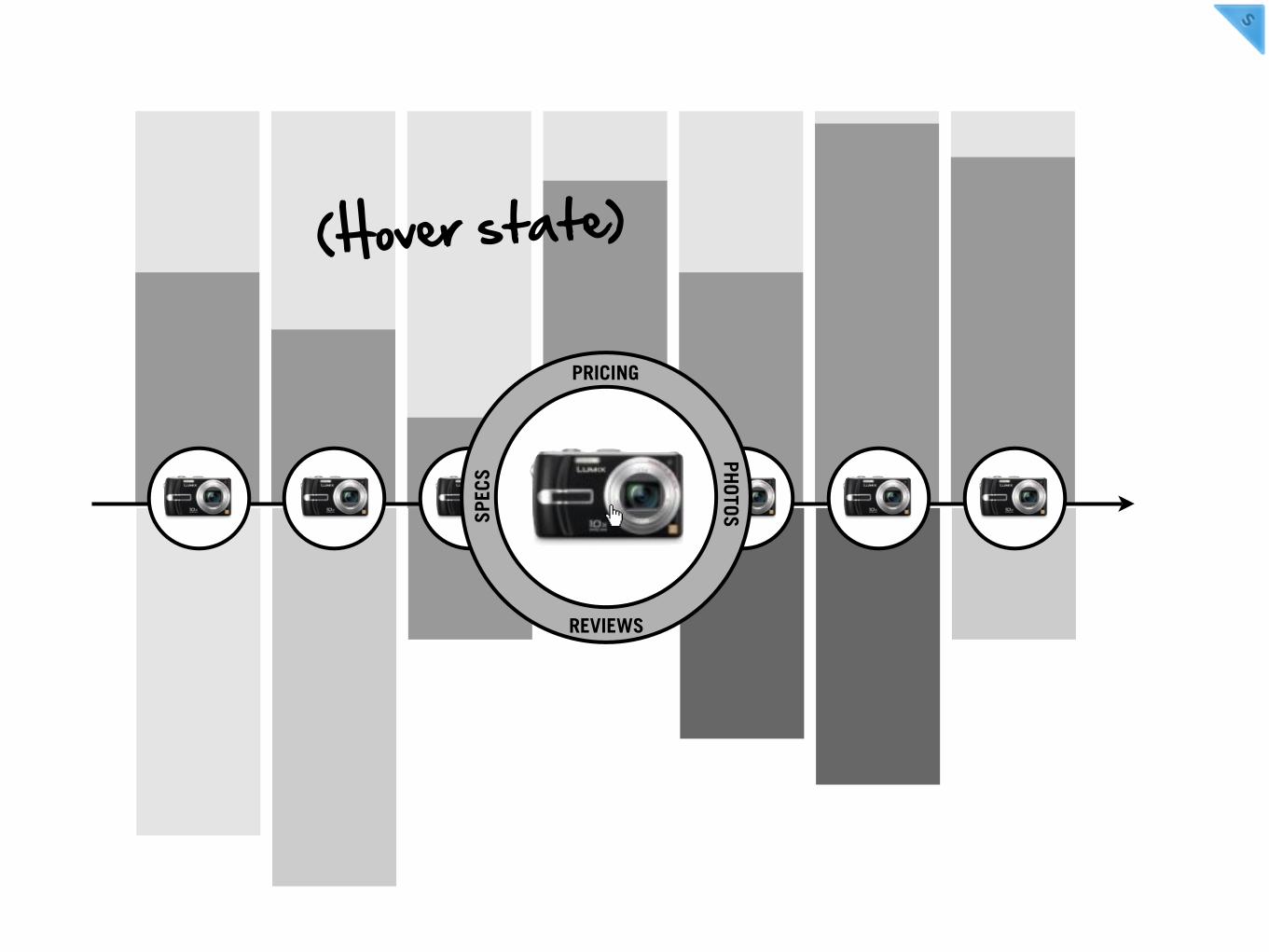
(Hover state)
REVIEWS
PRICING
SPECS
PH
OTOS
View more on Flickr
(Photos taken with
this camera from Flickr)

etc.
REVIEWS
PRICING
SPECS
PH
OTOS

Sneak Peek:
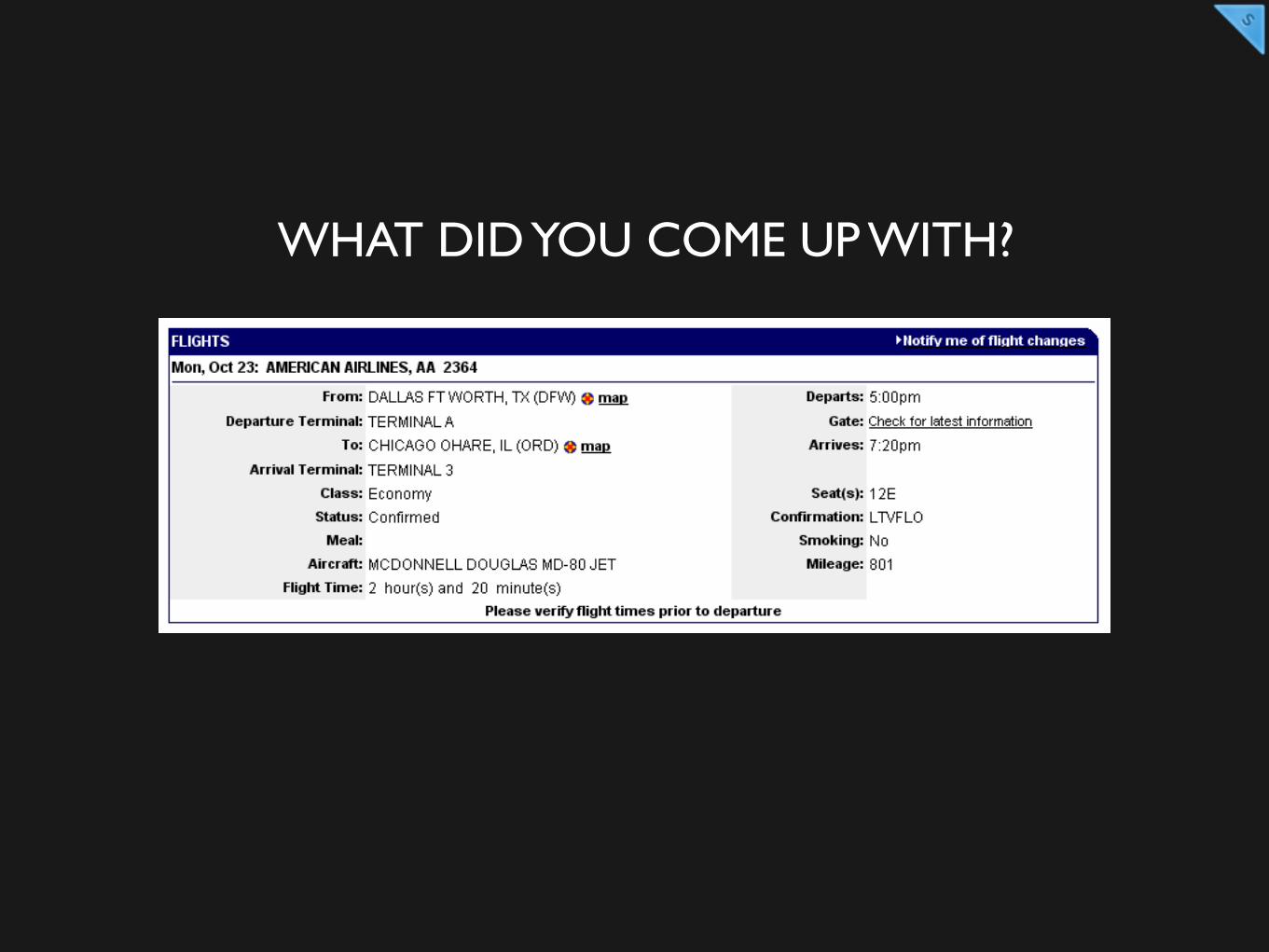
WHAT DID YOU COME UP WITH?
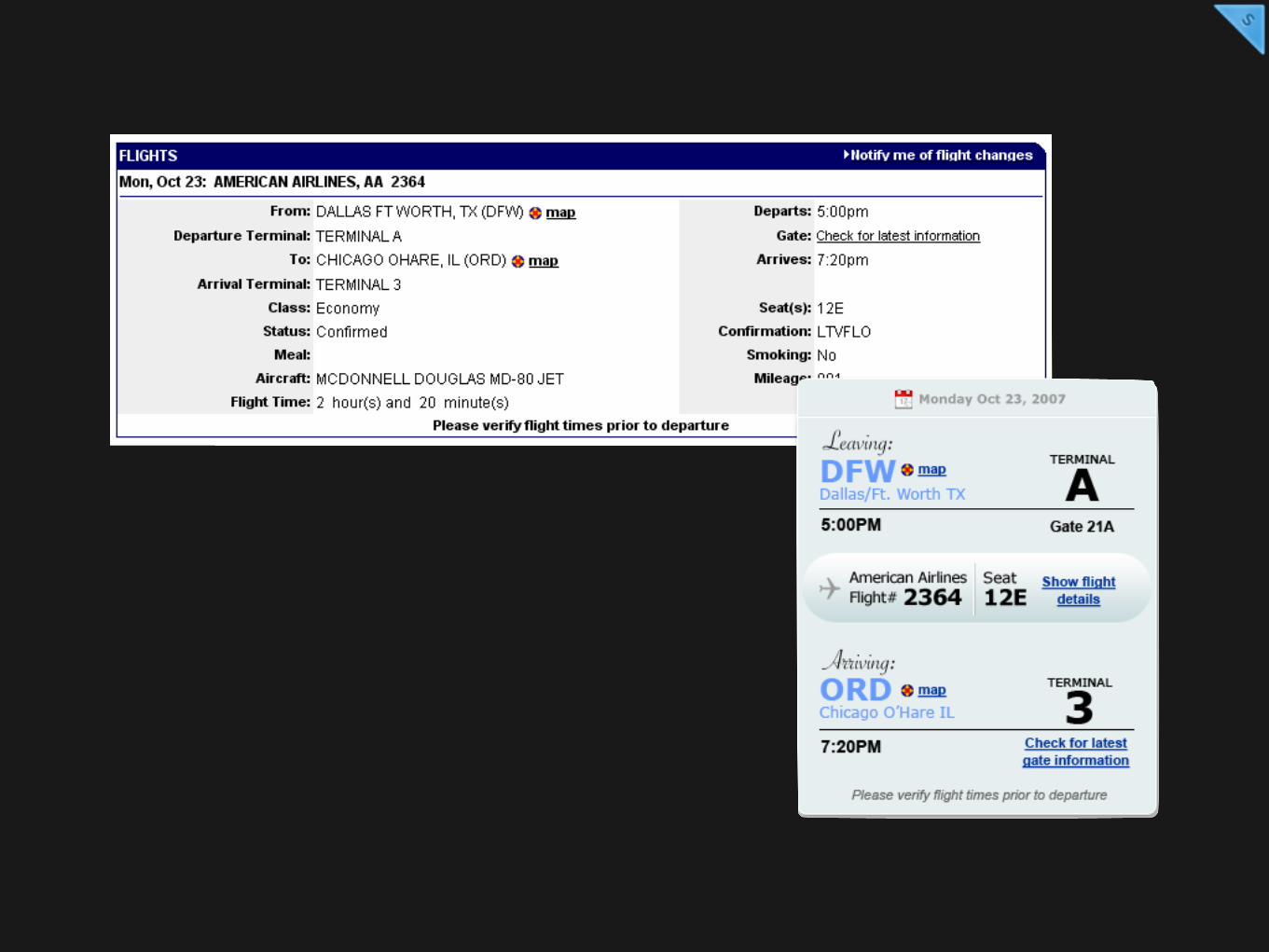
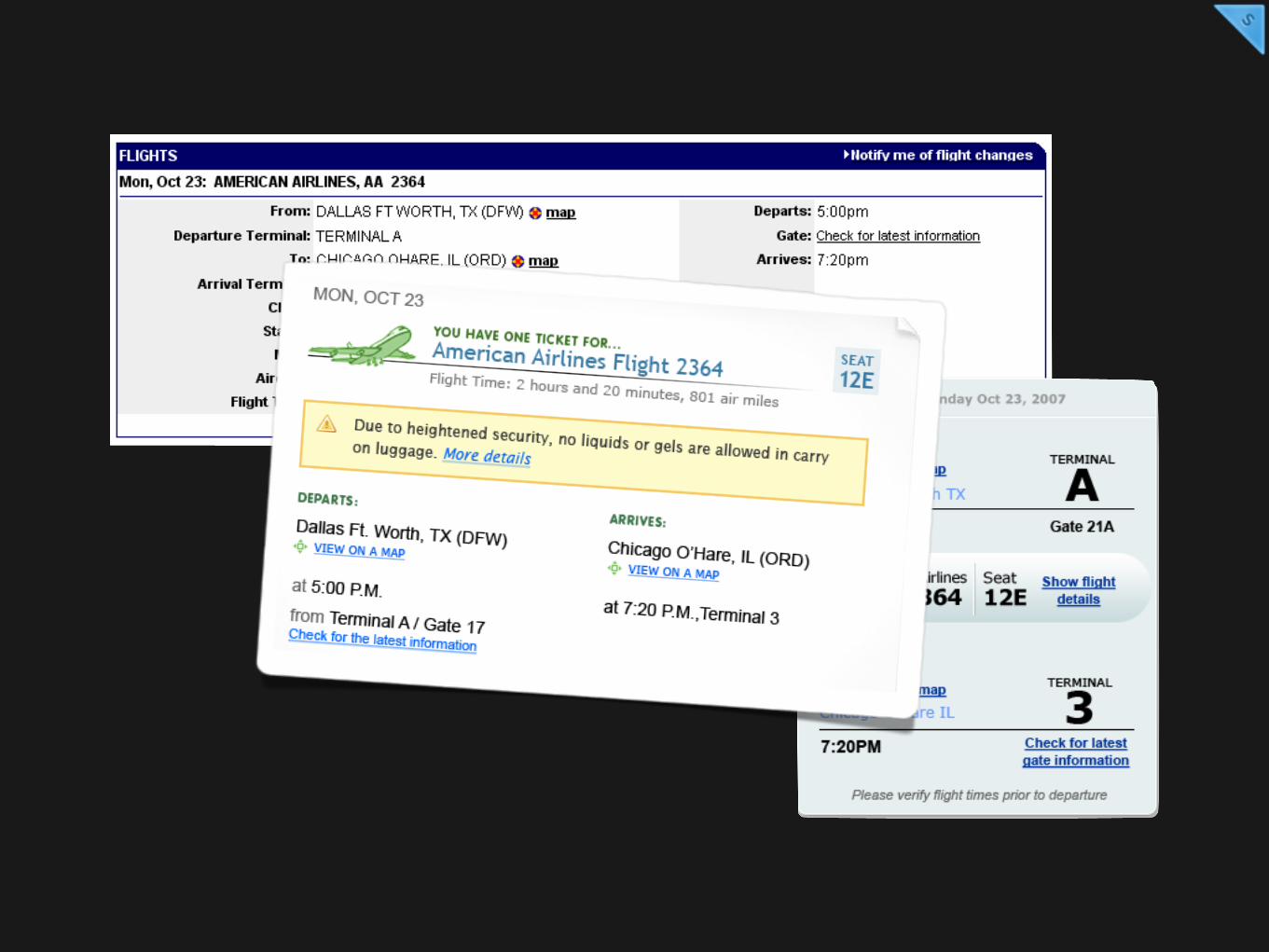
CREATE A CONSISTENT VISUAL LANGUAGE
HEY!
“I said something worth remembering”
Stephen Anderson

Thanks!STEPHEN P. ANDERSON
poetpainter.comslideshare.net/stephenpa
TRAVIS ISAACS
travisisaacs.comslideshare.net/tbisaacs