
Venous Thromboembolism
“VTE”:
A Preventable Problem
NoCVA Safe Surgery Collaborative August 19, 2013
Sharon McNamara, MSN, RN, CNOR
Erica Preston-Roedder, PhD, MSPH, Director of Quality Meaurement, NCQC
1

NoCVA Safe Surgery
Collaborative Goals
• Reduce post-surgical DVT and PE rates by 40% from the 2011 baseline.
• Reduce SSI SIR for COLO and HYST procedures by 40% compared to Q1-Q2 2012.
• 3% improvement in dimension scores on the Surgical Safety Culture Survey (Safe Surgery 2015)
• 80% completion of observation tools , using the standard observation instruments provided by the collaborative.

Collaborative Tools and Strategies
• Brief teamwork training customized to OR
• Implementation of the NoCVA Surgical Safety Checklist or derivative
• Observational assessment of checklist use and teamwork behaviors
• Defect analysis of events
• Process for gathering issues from debriefing and using that info for improvement
• Executive safety rounding
• Safety culture assessment

Post-surgical VTE (PSI 12)
• AHRQ PSIs are a series of claims-based indicators for patient safety
• PSI #12 = Post-surgical VTE
• Definition on AHRQ website:
http://www.qualityindicators.ahrq.gov/Modules/PSI_TechSpec.aspx
• Risk factors for adjustment found at:
http://www.qualityindicators.ahrq.gov/Downloads/Modules/PSI/V45/Parameter_Estimates_PSI_45.pdf

PSI 12
Patients w/PE or DVT which is not present on admission
(excludes vena cava & MDC 14)
------------------------------------------
Surgical patients

Numerator (case definition)
• Numerator: Any patient with a DVT or PE
• ICD-9-CM Deep vein thrombosis diagnosis codes:
• 45111 FEMORAL VEIN PHLEBITIS
• 45119 DEEP PHLEBTIS-LEG NEC
• 4512 THROMBOPHLEBITIS LEG NOS
• 45181 ILIAC THROMBOPHLEBITIS
• 4519 THROMBOPHLEBITIS NOS
• 45340 AC DVT/EMBL LOW EXT NOS
• 45341 AC DVT/EMB PROX LOW EXT
• 45342 AC DBT/EMB DISTL LOW EXT
• 4538 VENOUS THROMBOSIS NEC
• 4539 VENOUS THROMBOSIS NOS
• ICD-9-CM Pulmonary embolism diagnosis codes:
• 4151 PULMON EMBOLISM/INFARCT
• 41513 SADDLE EMBOL PULMON ART
• 41511 IATROGEN PULM EMB/INFARC
• 41519 PULM EMBOL/INFARCT NEC

Denominator (Population)
• Denominator: All surgical patients
• Exclude cases:
• with a principal ICD-9-CM diagnosis code (or secondary diagnosis present on admission)
for deep vein thrombosis (see above)
• with a principal ICD-9-CM diagnosis code (or secondary diagnosis present on admission)
for pulmonary embolism (see above)
• where the only operating room procedure is interruption of vena cava
• where a procedure for interruption of vena cava occurs before or on the same day as the
first operating room procedure
• MDC 14 (pregnancy, childbirth, and puerperium)
• with missing gender (SEX=missing), age (AGE=missing), quarter (DQTR=missing), year
(YEAR=missing), or principal diagnosis (DX1=missing)
NOTE: If you are not coding POA, this will affect your rates by ~110%! (HCUP study)

Venous Thromboembolism
“VTE”
A Preventable Problem

“Pulmonary embolism “PE” resulting from deep vein thrombosis “DVT” collectively referred to as Venous Thromboembolism is the most common preventable cause of hospital deaths.”
Preventing hospital-acquired venous thromboembolism: a guide for effective quality improvement. Agency for Healthcare Research and Quality. 2007

Relevance in USA
• 2 Million Patients suffer VTE annually
• Half develop VTE in hospital or 30 days post hospital
• Most hospitalized patients have at least one risk factor for VTE
• 23 Million surgeries performed annually
• 20% of patients in high risk category (ie. Hip & knee arthroplasty, hip fractures) develop proximal DVTs
• Proximal DVT is most dangerous and frequently lead to PE without anticoagulant prophylaxis
• One in ten surgical patients develop a DVT and go on to die from a PE = 20,000 patients yearly, this represents more deaths than those from breast cancer, AIDS, and traffic accidents combined.
Preventing hospital-acquired venous thromboembolism: a guide for effective quality improvement. Agency for Healthcare Research and Quality. http//www.ahrq.gov/QUAL/vtguide/. Accessed July 2, 2013.

Cost Estimates
• Increases cost in treatment and length of stay
• DVT = $10,000
• PE = $20,000
Preventing hospital-acquired venous thromboembolism: a guide for effective
quality improvement. Agency for Healthcare Research and Quality. http//www.ahrq.gov/QUAL/vtguide/. Accessed July 2, 2013.
VTE
Primary Causative
Factors
• Venous stasis
• Vessel wall injury
• Hypercoagulability
Ahoen J. Day surgery and
thromboembolic complications: time for
structured assessment and prophylaxis.
Curr Opin Anaesthesiol.
2007;20(6):535-539.
Risk Factors
• Immobility
• Tissue Trauma
• Surgical positioning
requirements
Rawat A, Huynh TT, et al. Primary
prophylaxis of venous thromboembolism
in surgical patients. Vas Endovascular
Surg. 2008;42(3):205-216.
12

AORN Recommended
Practices for Prevention of
Deep Vein Thrombosis
Recommended Practices for Prevention of Deep Vein Thrombosis. Perioperative Standards and Recommended Practices For Inpatient
and Ambulatory Settings. 2013 Edition: 365-374.

I. A healthcare organization wide PROTOCOL for the
prevention of DVT that includes care of the
perioperative patient should be developed and
implemented.
• Developed by a multidisciplinary team
• Supported by evidence-based model (risk based, group specific)
• Accessible to all healthcare providers
• Contain links to evidence-based treatment options
• Provide alternatives to suggested treatment
• List contraindications
• Simple to apply
• Apply to all patients within the health care organizations scope of service

II. The perioperative RN should complete a
PERIOPERATIVE PATIENT ASSESSMENT to determine
DVT RISK FACTORS.
Venous Stasis:
• Age > 40 years (>50 years)
• Cancer & associated therapy
• Cardiac disease history (CHF &
MI)
• Obesity
• Pregnancy & postpartum period
• Prolonged bed rest or
immobilization
• Prolonged travel (4-10 hours in
previous 8 weeks)
• Surgery > 30 minutes
• Varicose veins
Vessel Wall Injury:
• Cancer & associated therapy
• Central venous catheters
• Extensive burns
• Previous history of VTE or
stroke
• Surgery
• Trauma

Additional Risk Factors
Hypercoagulability:
• Cancer & associated therapy
• Inherited or acquired
thrombophilia
• Oral contraceptive use of
hormone replacement
therapy
• Pregnancy and the
postpartum period
• Trauma
Other:
• Acute medical illness
• Acute infectious processes
• Inflammatory conditions
• Smoking
• Dehydration
• Inflammatory bowel disease
• Active rheumatic disease
• Sickle cell disease
• Acute & chronic lung diease

III. The perioperative RN should IMPLEMENT SPECIFIC INTERVENTIONS when the
patient is receiving MECHANICAL DVT PROPHYLAXIS.
• Early ambulation
• Active & passive foot & ankle exercises
• Use of graduated compression stockings
• Intermittent pneumatic compression devices

Contraindications & Possible
Complications in Mechanical DVT
Prophylaxis
Contraindications
1. Conditions affecting lower extremities
2. Conditions compromising lower extremity venous flow
3. Sensitivity to latex, unless wraps & tubing are latex free
4. Severe congestive heart failure
5. Thigh circumference exceeds limit of manufacturers directions for use
Complications
1. Compartment syndrome
2. Latex sensitivity or allergy
3. Peroneal nerve injury/palsy
4. Skin injury

IV. The perioperative RN should IMPLEMENT SPECIFIC
INTERVENTIONS when the patient is receiving
PHAMACOLOGIC DVT PROPHYLAXIS.
Contraindications
1. Complex trauma
2. Hemorrhage
3. Infective endocarditis
4. Neurosurgery
5. Ocular surgery
6. Preganacy
7. Recent intracranial, gastric,
GU bleeding
8. Recent surgery
9. Recent lumbar/neuraxial
anesthesia (24 hours)
Complications
1. Bleeding
2. Compartment syndrome
3. Hematoma formation
4. Heparin induced
thrombocytopenia
5. Osteoporosis & osteopenia
6. Skin neucrosis
7. Thrombocytopenia
8. Urticaria at injection site

Develop Adequate
Prophylaxis Regimens
for Each Level of VTE
Risk
Following table taken from an audit tool not intended to
be used for order sets or protocols

Low Risk Moderate Risk High Risk
Early
ambulation
Heparin 5,000 units SC q 8 h or Dalteparin 5,000 units
SC daily or
Heparin 7,500 units SC q 12 h or Enoxaparin 30 mg SC q
12 hours or
Dalteparin 5,000 units SC daily or Enoxaparin 40 mg SC q
day or
Enoxaparin 40 mg SC daily or
Heparin 5,000 units SC q 12 hours
(only for patients with weight <50
kg
or age >75 years)
Fondaparinux 2.5 mg SC
daily or
Suggest adding SCD’s
Warfarin, INR 2-3
Add SCD’s (unless not
feasible)
Preventing hospital-acquired venous
thromboembolism: a guide for effective quality
improvement. Agency for Healthcare Research and
Quality. (Appendix D Chart Audit Form)
Table taken from audit tool not
intended to be used for order
sets or protocols

Cape Fear Valley Health
Dana Jackson, PharmD, BCPS
Clinical Informatics Pharmacist
Marcia Smith, RN, BSN
Nursing Quality Coordinator
22

Cape Fear Valley Health System
23

24

V. The perioperative RN should PROVIDE THE PATIENT
AND HIS OR HER DESIGNATED CAREGIVER(S)
INSTRUCTIONS regarding prevention of DVT and the
prescribed prophylactic measures.
Mechanical
• Mechanism of mechanical prophylaxis
• Importance of compliance
• Wearing properly sized graduated compression stockings (GCS)
• Application, removal & reapplication of GCS
Pharmacological
• Follow-up MD appointments and lab work
• Continuing medications
• Avoid activities that may cause injury
• Do not use over-the-counter medications (eg, aspirin, ibuprofin)
• Aware of medication & food interactions
• Use soft toothbrush, electric razor
• Report bruising
• Inform dentist, lab tech re VTE prophylaxis

Patient & Family Education &
Engagement Should Include
1. Current & future risk factors
2. Maintaining adequate hydration
3. Common signs & symptoms of DVT & PE
4. Avoid constrictive clothes
5. Avoid sitting with legs crossed, knees bent or standing, sitting for long periods
6. Elevate legs when sitting
7. Perform passive & active exercise (lower extremities)
8. Comply with VTE Prophylaxis
9. Perform frequent coughing & deep breathing exercises while in bed
10. Physiology of blood flow & clot formation

VI. PERSONNEL should receive INITIAL EDUCATION & COMPETENCY VALIDATION, as applicable to their roles, on patient care measures to prevent DVT.
VII. DOCUMENTATION should include a patient assessment, plan of care, nursing diagnosis, identification of desired outcomes and interventions, as well as an evaluation of the patient’s response to care.
VIII. POLICIES AND PROCEDURES for DVT prophylaxis should be developed, reviewed periodically, revised as necessary, and readily available in the practice setting.
IX. A QUALITY IMPROVEMENT PROGRAM should be in place to evaluate the outcomes of DVT prophylaxis and protocol compliance.

Agency for Healthcare Research and Quality.
(AHRQ) Recommendations
.
1. QI Program should include a study time frame
2. Compare the HCO DVT prevention protocol (PP) to current research & established, research based guidelines
3. Determine the HCO DVT PP rate of use
4. Determine & explore barriers to the use of the protocol
5. Determine the rate of readmissions for DVT or complications related to DVT
Preventing Hospital-Acquired Venous Throboembolism A Guide for Effective Quality Improvement. See Appendix D Chart Audit Form
29
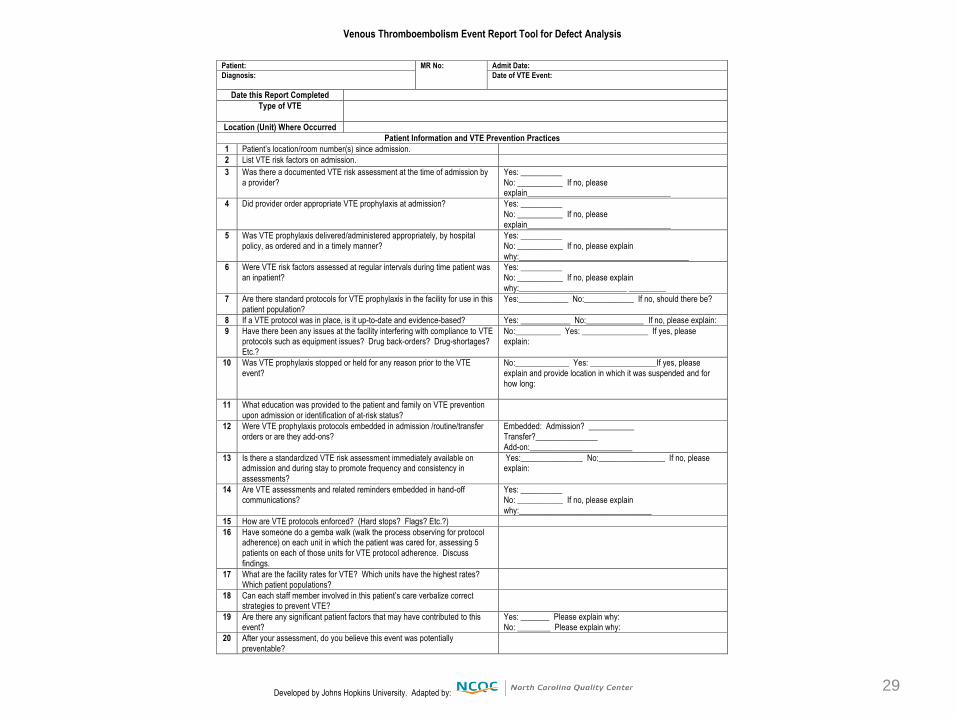
Venous Thromboembolism Event Report Tool for Defect Analysis
Developed by Johns Hopkins University. Adapted by:
Patient: MR No: Admit Date:
Diagnosis: Date of VTE Event:
Date this Report Completed
Type of VTE
Location (Unit) Where Occurred
Patient Information and VTE Prevention Practices
1 Patient’s location/room number(s) since admission.
2 List VTE risk factors on admission.
3 Was there a documented VTE risk assessment at the time of admission by
a provider?
Yes: __________
No: ___________ If no, please explain___________________________________
4 Did provider order appropriate VTE prophylaxis at admission? Yes: __________
No: ___________ If no, please
explain___________________________________
5 Was VTE prophylaxis delivered/administered appropriately, by hospital policy, as ordered and in a timely manner?
Yes: __________ No: ___________ If no, please explain
why:_________________________________________
6 Were VTE risk factors assessed at regular intervals during time patient was an inpatient?
Yes: __________ No: ___________ If no, please explain
why:__________________________ _________
7 Are there standard protocols for VTE prophylaxis in the facility for use in this patient population?
Yes:____________ No:____________ If no, should there be?
8 If a VTE protocol was in place, is it up-to-date and evidence-based? Yes: ____________ No:______________ If no, please explain:
9 Have there been any issues at the facility interfering with compliance to VTE protocols such as equipment issues? Drug back-orders? Drug-shortages? Etc.?
No:___________ Yes: ________________ If yes, please explain:
10 Was VTE prophylaxis stopped or held for any reason prior to the VTE
event?
No:_____________ Yes: ________________If yes, please
explain and provide location in which it was suspended and for
how long:
11 What education was provided to the patient and family on VTE prevention
upon admission or identification of at-risk status?
12 Were VTE prophylaxis protocols embedded in admission /routine/transfer orders or are they add-ons?
Embedded: Admission? ___________ Transfer?_______________
Add-on:_________________________
13 Is there a standardized VTE risk assessment immediately available on admission and during stay to promote frequency and consistency in
assessments?
Yes:_______________ No:________________ If no, please explain:
14 Are VTE assessments and related reminders embedded in hand-off communications?
Yes: __________ No: ___________ If no, please explain
why:________________________________
15 How are VTE protocols enforced? (Hard stops? Flags? Etc.?)
16 Have someone do a gemba walk (walk the process observing for protocol adherence) on each unit in which the patient was cared for, assessing 5
patients on each of those units for VTE protocol adherence. Discuss
findings.
17 What are the facility rates for VTE? Which units have the highest rates? Which patient populations?
18 Can each staff member involved in this patient’s care verbalize correct strategies to prevent VTE?
19 Are there any significant patient factors that may have contributed to this event?
Yes: _______ Please explain why: No: ________ Please explain why:
20 After your assessment, do you believe this event was potentially
preventable?

VTE Resources
Ahoen J. Day surgery and thromboembolic complications: time for structured assessment and prophylaxis. Curr Opin
Anaesthesiol. 2007;20(6):535-539.
Eisenstein D. Anticoagulation Management in the Ambulatory Surgical Setting. AORN Journal. 2012;95(4): 510-524.
Rawat A, Huynh TT, et al. Primary prophylaxis of venous thromboembolism in surgical patients. Vas Endovascular
Surg. 2008;42(3):205-216.
Recommended Practice for Prevention of Deep Vein Thrombosis. AORN Perioperative Standards and Recommended
Practices For Inpatients and Ambulatory Settings. AORN 2013: 365-373.
Partnership for Patient Care. Failure mode and effects analysis venous thromboembolism prophylaxis. ECRI Institute
Healthcare Improvement Foundation. 2007.
https://www.ecri.org/Documents/Patient_Safety_Center/PPC_VTE_Prophylaxis.pdf. Accessed 7/2/13.
Preventing Hospital-acquired venous throboembolism a guide for effective quality improvement. Agency for Healthcare
Research and Quality. www.ahrq.gov/.../quality-patient-safety/patient-safety-
resources/resources/vtguide/vtguide.pdf - 312k - 2013-06-18. Accessed 7/3/13.
Venou tromboembolism prophylaxis in orthopedic surgery. Effective Health Care Program Comparative Effectiveness
Review #49. Agency for Healthcare Research and Quality.
http://www.effectivehealthcare.ahrq.gov/ehc/products/186/992/CER-49_VTE_20120313.pdf. Accessed 6/12/13.
Venous thromboembolism in adult hospitalizations – united states 2007-2009. Morbidity and Mortality Weekly Report.
2012;61(22):401-404.
Guyatt GH, Crowther M, Gutterman DD, etal. Antimicrobial therapy and prevention of thrombosis, 9th ed. American
college of chest physicians evidence-based clinical practice guidelines.
http://journal.publications.chestnet.org/data/Journals/CHEST/23443/1412S3.pdf. Accessed 7/8/13.

Next Steps
Learning from Defects homework September 16
Webinar: Learning from Defects
Case Study and Report Out
September 16
1:00
Learning Session 2:
Chapel Hill, NC
October 2
Webinar: Executive Partnerships:
Walkrounds
October 26 1:00
Invite your Executive Sponsor
Continue implementing checklist
and completing observations
Continue teamwork training

Project Contacts
Laura Maynard, MDiv
Director of Collaborative Learning
919-677-4121
Jan Mangun, MT(ASCP), MSA, CPHRM
Exec Director, Quality and Pt. Safety, VHHA
804-965-1202
Erica Preston-Roedder, PhD, MSPH
Director of Quality Measurement
919-677-4125
Dean Higgins, BA
Project Manager
919-677-4212
James Hayes
Project Coordinator
919-677-4140
Recommended

















