Using Smart Forms to Discretely Capture Stroke Data for Electronic Reporting
Elaine Tsiakopoulos, RN, MSN, Shondralis Allen, BS, Janet Gervasio, MSN, RN-BC,PMP James R. Brorson, MD, Cedric McKoy, APN, Pedro Vivar Cruz, MD, Susan Richter, RN, MS
Background Aims
The Intervention
Lessons Learned
• To accurately capture discrete data for reporting on Stroke Quality Measures for the CMS IQR program • To maximize compliance with the MU-EH EHR incentive payment program • To decrease manual abstraction times
• Collaboration between the Epic team, Quality team, CBIS team, and Neurology team to coordinate capturing discrete data components necessary for reporting • Methods had to fit Neurology providers workflow & capture data discretely according to MU specifications.
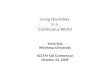
• The Smart Form and NIHSS can be pulled into any Notewriter on the fly by a provider with the use of a Smart Phrase:
• .NEUROSTROKE (Figure 1). • .NIHSTROKESCALE (Figure 4).
• Designed as intuitive one click documentation (Figures 1& 2), auto-generating text for note (Figure 3) while capturing discrete data for 2 areas of required reporting use: MU-EH CQMs and CMS IQR Core Measures. • Auto Cascading of Reasons Not Given for intervention, allowing for at a glance view of all Quality Measures required for documentation (Figure 2). • Auto Calculation of NIHSS total score (Figure 4). • ‘Hover to discover’ functionality detailed the definition and the descriptions for documentation for both the Rankin Scale and NIHSS score (Figure 4).
• Education was provided on October 29th, 2013 to all Neurology Residents with a TipSheet • Use was measured through abstraction of Core Measures and validation of MU CQMs
• Provider participation and buy-in was essential to the success and usefulness of the Smart Form • Adding additional meaningful components requested by the providers to the Smart Form maximized participation
Next Steps
Results
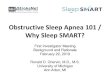
• After the implementation of the Smart Form in October 2013, measure performance was at 100% for 3 consecutive months. • Prior to the implementation of the Smart Form, there were 1 – 3 outliers per month with low performance in March & April 2013 below the mean.
• Beginning with January 2013 discharges, the Center for Medicare & Medicaid Services (CMS) Inpatient Quality Reporting (IQR) Program required reporting on the new Stroke Quality Measures:
• STK2 Antithrombotic at discharge • STK3 Anticoagulant at discharge • STK4 Thrombolytic therapy • STK5 Antithrombotic by hospital day 2 • STK 6 Statin at discharge • STK10 Assessed for rehabilitation
• The measures were also a part of the CMS Electronic Heath Record (EHR) Incentive Program called Meaningful Use (MU) Eligible Hospitals (EH) Clinical Quality Measures (CQMs) which required discrete data. • Data was manually abstracted and required discrete elements to participate in the EHR Incentive Program.
• Continue to audit & validate data capture and measure performance for meaningful change
Contact: [email protected]
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Week 8
G4P Std. Campaign Baseline
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Week 8
G4P Std. Campaign Baseline
Baseline: 58.0% Standard HH Campaign: 72.3%, p<0.001 Giving for Performance: 83.9%, p=0.003
Figure 1. Smart Form Figure 2. Reasons Not Given
Figure 3. Complete Note Figure 4. NIHSS ONLY (Hover to Discover funcPonality, AutoCalculates total scale score )
Definition: Patients receiving all Stroke-audited care for which they were eligible. Measures evaluating stroke education and Venous Thromboembolism (VTE) Prophylaxis were excluded in the calculation of the composite score. Encounter counts are based on total number of qualifying measures per encounter. Sampling: Yes, based on CMS guidelines. Data Source: Clinical documentation nurse chart review from Epic / MR View Control charts are used to identify statistically significant change by applying a standard set of rules against the 3 sigma limits. Red square: meaningful change. White square: contribute to change. Blue circle: no change
Recommended