UROGENITAL INFECTIONS
BYPROF/ GOUDA ELLABBAN
ORGANISMS THAT CAUSEURINARY TRACT INFECTION
• Non-specific organisms:– E. coli (common)
– Klebsiella (common)
– Staph. aureus (rare)
• Specific organisms: – Gonococci (not uncommon)
– Schistosoma hematobium (rare)
– Mycobacteria tuberculosis (rare)
ROUTES OF INFECTIONS
• Ascending Infection– Through the urethra
• Hematogenous Infection– Through the kidneys– Through the prostate
ASCENDING INFECTION
• More common in females because of– The short urethra– Close proximity of the urethra to the vagina
• Organisms that cause ascending infection– Non-specific (e. coli, klebsiella)
– Specific (gonococcus, chlamydea)
HEMATOGENOUS INFECTION(rare)
• Non-Specific Organisms– Staph. aureus (commonest)
• Kidney ⇒ renal cortical abscess (renal carbuncle)• Prostate ⇒ prostatitis
• Specific Organisms– Schistosoma hematobium– Tubercle bacilli
CYSTITIS
• Acute cystitis– Acute onset of severe symptoms– It usually resolves completely within 2-5 days with
adequate antimicrobial therapy
• Chronic cystitis– Mild but persistent symptoms– Predisposed by presence of chronic infravesical
obstruction with retained urine in the bladder (chronic retention); e.g. BPH
– Treatment must include removal of infravesical obstruction
CYSTITIS (cont.)
• Urinary symptoms– Irritative urinary symptoms: burning, frequency (day and
night), urgency– Hematuria (usually microscopic, but occasionally gross)
• Diagnosis– Urine analysis: pyuria (WBC in significant amount)
• Treatment– Appropriate antibiotic based on urine culture and
sensitivity (ampicillin, quinolones are usually effective)
– In chronic cystitis, any obstructive lesion must be removed
PYELONEPHRITIS
• Acute pyelonephritis– Acute onset of severe symptoms– it usually resolves completely within 4-8 days with
adequate antimicrobial therapy
• Chronic pyelonephritis– Mild but persistent symptoms– Predisposed by presence of chronic obstructive uropathy
in the ureter, bladder neck or urethra– Treatment must include removal of any obstructive lesion
PYELONEPHRITIS (cont.)
• Clinical presentation– Dull aching renal pain– Fever, malaise, nausea, vomiting (only in acute
pyelonephritis)
• Diagnosis– Urine analysis: pyuria (WBC in significant amount)
• Treatment– Appropriate antibiotic based on urine culture and
sensitivity (ampicillin, quinolones are usually effective)– In chronic pyelonephritis, any obstructive lesion must be
removed
ACUTE PROSTATITIS
• Symptoms– Acute onset of fever with severe irritative and obstructive urinary
symptoms– DRE (digital rectal examination): a very tender, firm and swollen
prostate
• Diagnosis– Urine analysis: pyuria (WBC in significant amount)– Prostatic secretions obtained by prostatic massage: absolutely
contraindicated from fear of septicemia
• Treatment– Appropriate antibiotic (ampicillin, quinolones)– Given empirically
CHRONIC PROSTATITIS
• Etiology– Same organisms as for acute prostatitis– Chronic low grade and persistent bacterial infection
• Clinical Presentation– Mild irritative urinary symptoms– Pain referring to the anterior urethra, lower abdomen, peri-anal
region, testis or perineum– DRE: prostate is very firm and mildly painful
• Diagnosis– Prostatic secretions by prostatic massage: WBC >15WBC/HPF
• Treatment– Antibiotics based on culture and sensitivity of the expressed prostatic
secretions

EPIDIDYMO-ORCHITIS
• Acute epididymo-orchitis– Bacterial spread from the urethra and along the vas to the
epididymis and testis– Acute onset of severely painful huge tender firm scrotal swelling– Differential diagnosis with testicular torsion by Doppler ultrasound– Treatment: parental antibiotics, pain killers and bed rest
• Chronic epididymo-orchitis – Chronic non-specific epididymo-orchitis does not occur– Chronic specific epididymitis: T.B. (review under Specific Infections)
MALE GENITAL GONORRHEA
• Cause– Ascending infection of gonococcal bacilli in the urethra following
sexual intercourse with an infected partner
• Presentation– Yellow urethral discharge in the acute stage (differential diagnosis:
prostatorrhea: colorless urethral discharge; not a disease)
• Complications– Chronic urethritis, chronic prostatitis– Stricture of the bulbous urethra
• Treatment– Medical treatment: tetracyclines, quinolones– Surgical treatment of urethral stricture: endoscopic visual
urethrotomy, or excision of the strictured urethral segment
UROGENITAL BILHARZIASIS
• Bilharzial cystitis (commonest)
• Bilharzial ureteritis (2nd common; only in the lower third)
• Bilharzial urethritis (rare)
• Bilharzial genital lesions (esp. the seminal vesicles; very rare)
• The kidneys and upper 2 thirds of the ureters are
NEVER directly affected by bilharzia
ACUTE BILHARZIAL CYSTITIS
• Symptoms– Symptoms of cystitis (burning, frequency, urgency) – Terminal hematuria
• Urine analysis– Living bilharzial ova
• Treatment– Oral tablets (Praziquantel; 40mg/kg in a single dose)– Good prognosis
CHRONIC BILHARZIALCYSTITIS (AND URETERITIS)
• Thousands of bilharzial ova are retained in the suburothelium and die
• The dead bilharzial ova in the suburothelium undergo calcification, and appear as “linear calcification”

CHRONIC BILHARZIAL CYSTITIS“COMPLICATIONS”
• Fibrosis of the bladder muscles– Chronic bladder ulcer (localized fibrosis in the detrusor with
ischemic atrophy of the overlying mucosa)
– Contracted bladder (fibrosis of the entire detrusor)
• Chronic irritation of the urothelium– Metaplasia (to squamous epithelium)
– Leukoplakia (squamous metaplasia with hyperkeratosis)
– Carcinoma

CHRONIC BILHARZIAL URETERITIS“COMPLICATIONS”
• Stricture of the lower third of the ureter– Caused by fibrosis of the ureteral muscle by the bilharzial
reaction
• Vesico-ureteral reflux– Caused by derangement of the uretero-vesical junction by
the bilharzial reaction


TREATMENT OF COMPLICATIONS
• Chronic bladder ulcer: partial cystectomy• Bladder neck obstruction: endoscopic incision of the bladder
neck• Contracted bladder: ileocystoplasty or colocystoplasty• Bladder cancer: radical cystectomy• Stricture of the ureter: resection of the strictured segment,
and anastomosis of the 2 healthy ends of the ureter• Vesico-ureteral reflux: re-implantation of the ureter in the
bladder by an anti-reflux technique
UROGENITAL TUBERCULOSIS
• Incidence• Age (20-40 years); Sex (same)
• Mode of infection (hematogenous)• From the lungs (2ry infection) or from other organs (3ry
infection)
• Kidneys and prostate are first affected (infection then spreads to other urogenital organs)
• Pathology• Tuberculomatous reaction
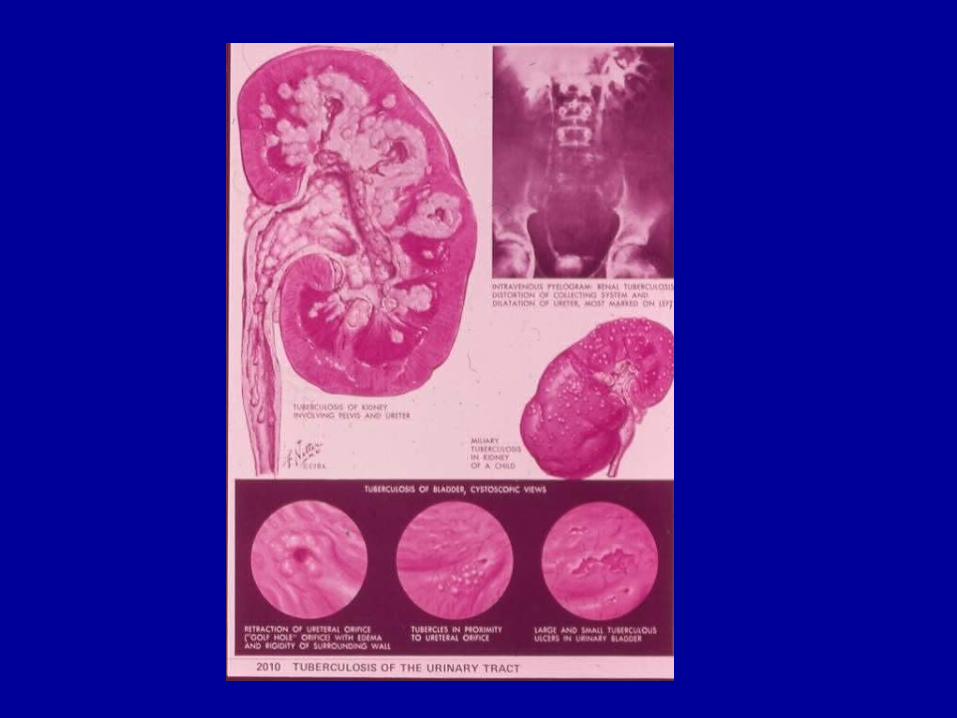
KIDNEY INVOLVEMENT
• Acute stage– Acute tuberculous pyelonephritis– Usually no symptoms
• Chronic stage– Chronic interstitial nephritis with papillary necrosis– Autonephrectomy: kidney lost its continuity with:
• the urinary tract from complete ureteral stricture, and • the circulation from end arteritis obliterans
– Mild renal pain (late presentation)
ACUTE TUBERCULOUS CYSTITIS
• Tubercle bacilli move from the kidney (in the acute stage), along the ureter, and to the bladder causing acute tuberculous cystitis and positive urinary symptoms
• Urinary symptoms are the first complaint by the patient:– Frequency of micturition (+++)– Urgency (+)– Burning (+)– Hematuria (+)
• Kidney pain is a late symptom that appears during the chronic stage of pyelonephritis
CHRONIC TUBERCULOUS CYSTITIS
– Linear calcification: a symptomless condition
– Chronic ulcers: burning and frequency
– Contracted bladder: severe frequency – Widely refluxing ureteric orifices (golf hole
appearance): hydronephrosis and UTI
CHRONIC TUBERCULOUS URETERITIS
• Stricture of the ureter at the lower third– In bilharzial ureteritis: the same
• Entire ureter is dilated, rigid, straight, and has a thick wall– In bilharzial ureteritis, the dilated ureter is tortuous and
has a thin wall
GENITAL TUBERCULOSIS
• Vas deferens involvement– Very rare– Beading of the vas
• Chronic epididymitis– Very rare– It is symptomless or causes mild pain– Induration of the epididymis
UROGENITAL TUBERCULOSIS“DIAGNOSIS”
• Urine analysis– Pyuria– Urine culture for non-specific organisms: negative (sterile
pyuria)– Urine culture for tubercle bacilli: positive
• Biopsy from the bladder or kidney– Tuberculomatous reaction seen in biopsy specimen

UROGENITAL TUBERCULOSIS“INVESTIGATIONS”
• KUB: calcification of the renal parenchyma, linear calcification of the bladder wall
• IVU: ureteral stricture, contracted bladder, non-functioning kidney (autonephrectomy)
• Ascending cystogram: vesico-ureteral reflux
• Cystoscopy: tubercles (confirmed by biopsy), bladder ulcers, widely dilated (golf-hole) ureteric orifice, contracted bladder

UROGENITAL TUBERCULOSIS“TREATMENT”
• Anti-tuberculous treatment – For 6 months
• Surgical reconstruction– Ureteral stricture (resection of the strictured segment and re-
anastomosis of the 2 healthy ends of the ureter)– Vesico-ureteral reflux (ureteral re-implantation in the bladder
by an anti-reflux)– Contracted bladder (ileocystoplasty or colocystoplasty)
• Nephrectomy if there is autonephrectomy
Recommended