
Emerging Therapies in AHF: Ularitide
Stefan D. Anker
Innovative Clinical Trials, University Medicine Göttingen (UMG) at Göttingen, [email protected]
Sevilla, 23 May, 2015
Conflict of Interest:Consultancy, honoraria for speaking and/or research grants fromBayer, BG Medicine, BioVentrix, Brahms GmbH, Cardiorentis,LonestarHeart, Novartis, Vifor.
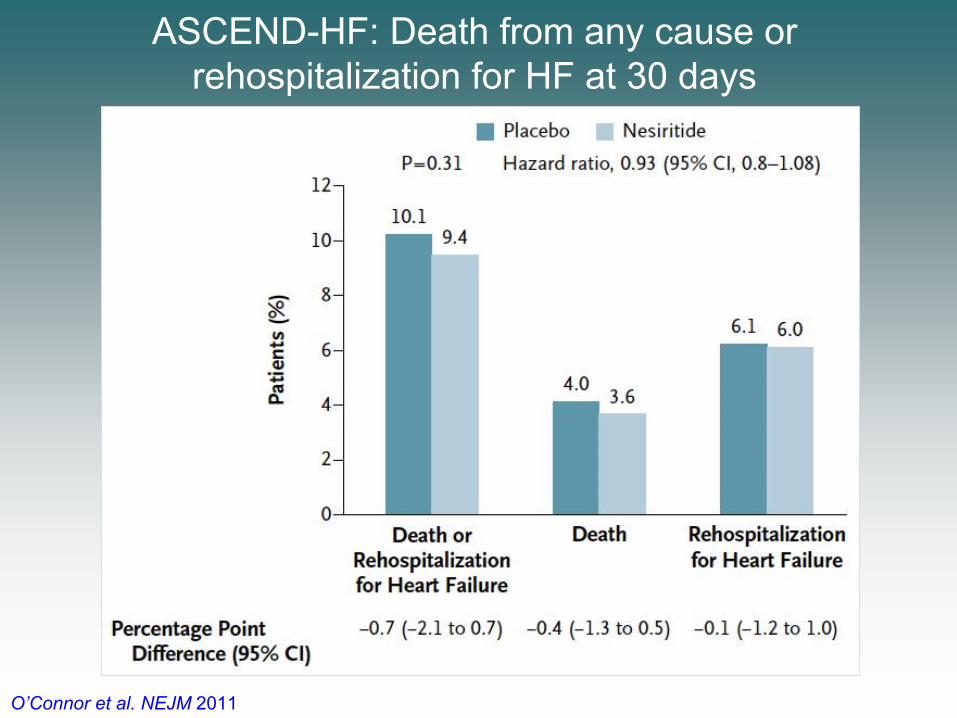
ASCEND-HF: Death from any cause or rehospitalization for HF at 30 days
O’Connor et al. NEJM 2011
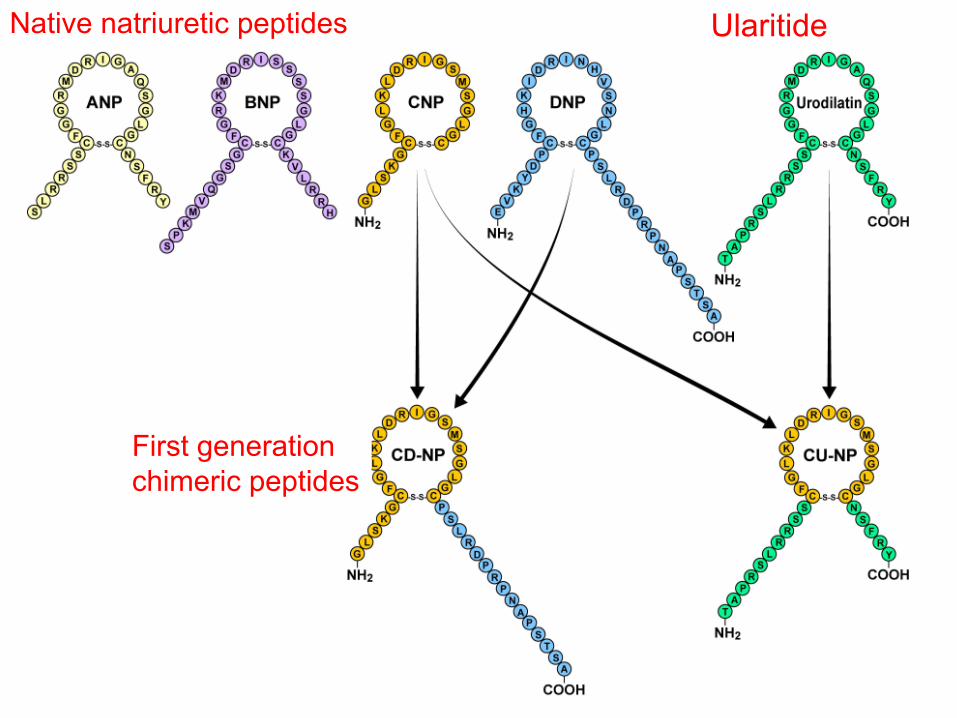
Native natriuretic peptides
First generationchimeric peptides
Ularitide
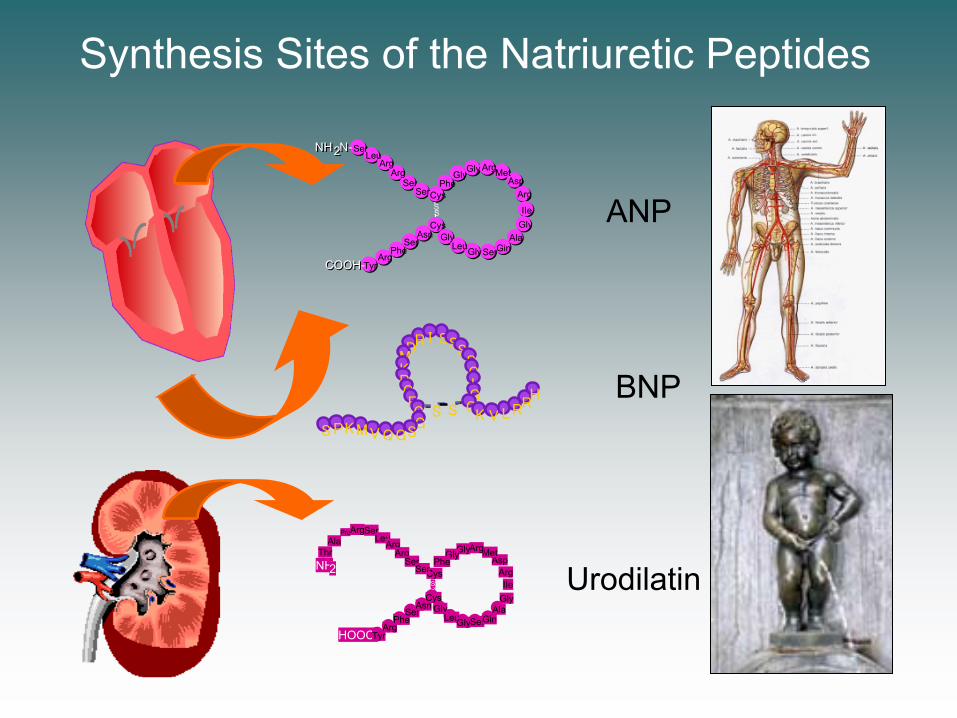
Synthesis Sites of the Natriuretic Peptides
DRI
MKRG
SSSSGLGF
C CS SGSGQVM
K VLRRH
KPS
NH2
HOOC-
ThrAla
ProArgSerLeuArg
Arg
TyrArg
PheSer
AsnCys
GlyLeuGlySerGin
AlaGlyIIe
ArgAsp
MetArgGlyGlyPhe
CysSer
Ser
SS
NH 2N-
COOH-
NH 2N-SerLeu
ArgArg
SerSerCys
Phe
Gly
Gly Arg
CysGly
ArgTyr
Asn
PheSer
Gly
Leu SerGinAla
GlyIIe
ArgAsp
Met
COOH-
SS ANP
BNP
Urodilatin

Urodilatin is synthesized in the distal tubulus cells
is luminally secreted
binds downstream in inner medullar-collecting duct to NPR-A and acts via cGMP
and inhibits
Na-reabsorption
Physiology of Urodilatin (INN: Ularitide)
NPR-A
NatriuresisDiuresis
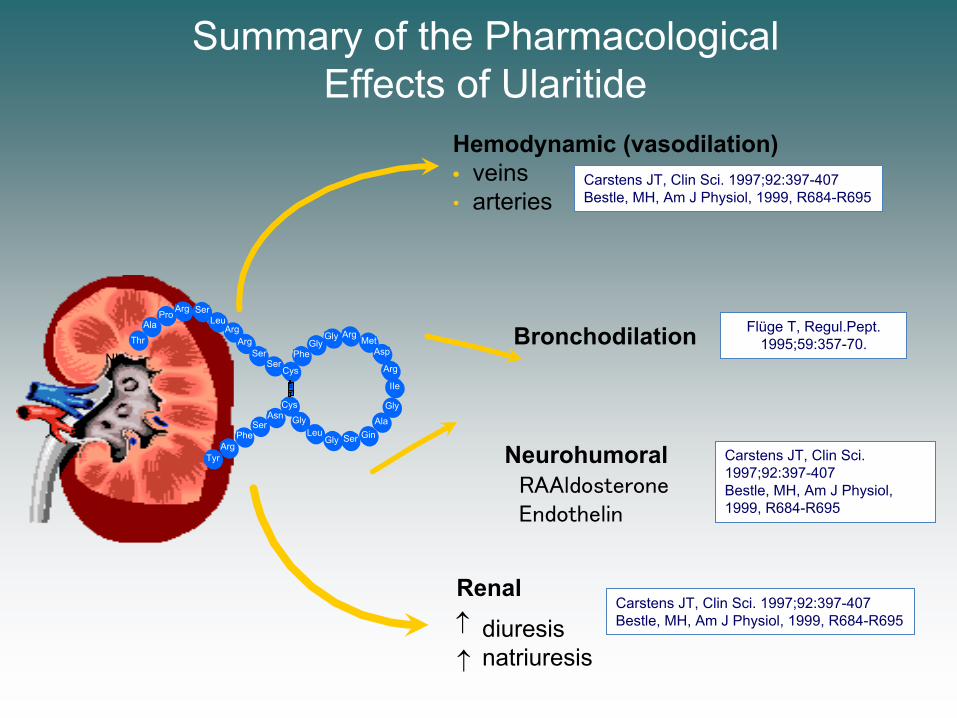
Summary of the Pharmacological Effects of Ularitide
Hemodynamic (vasodilation)• veins• arteries
Neurohumoral¯RAAldosterone¯Endothelin
diuresisnatriuresis
Renal
Thr
AlaPro Arg Ser
LeuArg
Arg
TyrArg
PheSer
AsnCys
GlyLeu
Gly Ser GinAla
Gly
IIe
Arg
AspMet
ArgGlyGly
Phe
Cys
SerSer
SS
NH2 Bronchodilation Flüge T, Regul.Pept.
1995;59:357-70.
Carstens JT, Clin Sci. 1997;92:397-407Bestle, MH, Am J Physiol, 1999, R684-R695
Carstens JT, Clin Sci. 1997;92:397-407Bestle, MH, Am J Physiol, 1999, R684-R695
Carstens JT, Clin Sci. 1997;92:397-407Bestle, MH, Am J Physiol, 1999, R684-R695

SIRIUS I Trial – Study Design Design:• In total, 24 patients with decompensated heart failure requiring hospitalisation as well as right heart catheterisation were included into the study (6 pts in each group)• Infusion of Ularitide 7.5, 15, and 30 ng/kg body weight/min, or placebo over 24 hours
Main Inclusion Criteria • Symptomatic, decompensated chronic heart failure• Dyspnea at rest or during minimal activity• PCWP 18 mmHg, CI 2.5 l/min/m2
Primary Endpoints:• Change in PCWP at 6 hrs compared to placebo• Change in patient-assessed dyspnea at 6 hrs compared to placebo
Mitrovic et al, Am Heart J, 2005, 150: 1239Am Heart J 2005; 150:1239.e1-1239.e8
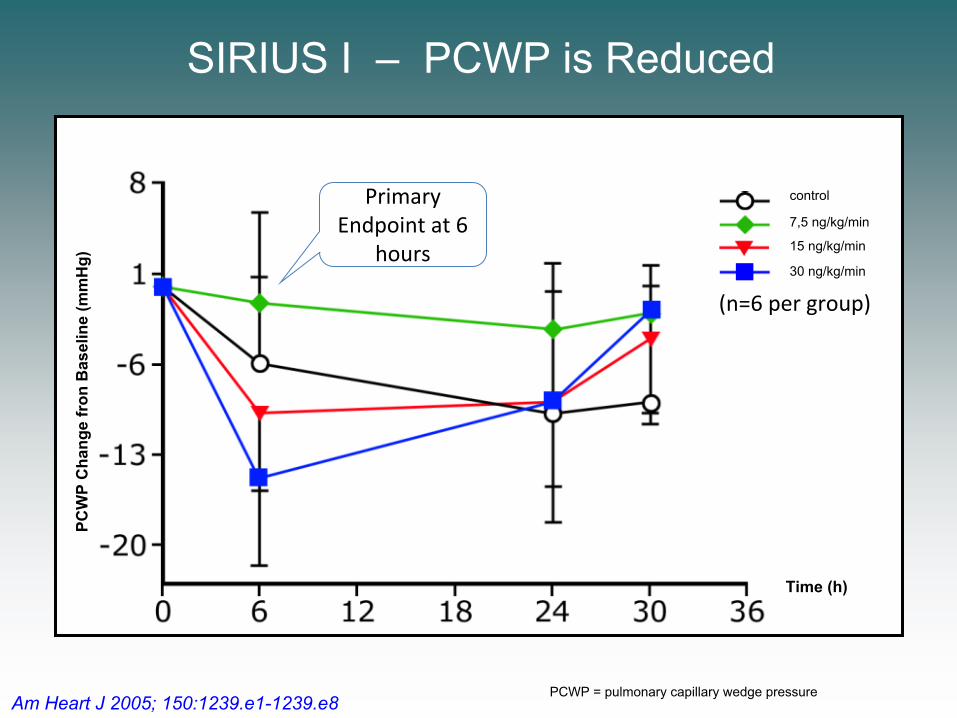
SIRIUS I – PCWP is ReducedPC
WP
Cha
nge
fron
Bas
elin
e (m
mH
g)
Time (h)
control
30 ng/kg/min
15 ng/kg/min
7,5 ng/kg/min
PCWP = pulmonary capillary wedge pressure
Primary Endpoint at 6
hours
(n=6 per group)
Am Heart J 2005; 150:1239.e1-1239.e8

SIRIUS II Trial – Study EndpointsDesign:• Infusion of Ularitide 7.5, 15, and 30 ng/kg body weight/min, or placebo over 24 hours• In total, 221 patients with decompensated heart failure requiring hospitalisation as well as right heart catheterisation were included into the study (6 pts in each group)
Main Inclusion Criteria: • Symptomatic, decompensated chronic heart failure• Dyspnea at rest or during minimal activity• PCWP 18 mmHg, CI 2.5 l/min/m2
Primary Endpoints:• Change in PCWP at 6 hrs compared to placebo• Change in patient-assessed dyspnea at 6 hrs compared to placebo
Placebo: 53 pts 7.5 ng: 60 pts 15 ng: 53 pts 30 ng: 55 pts
EHJ 2006; 27:2823–2832
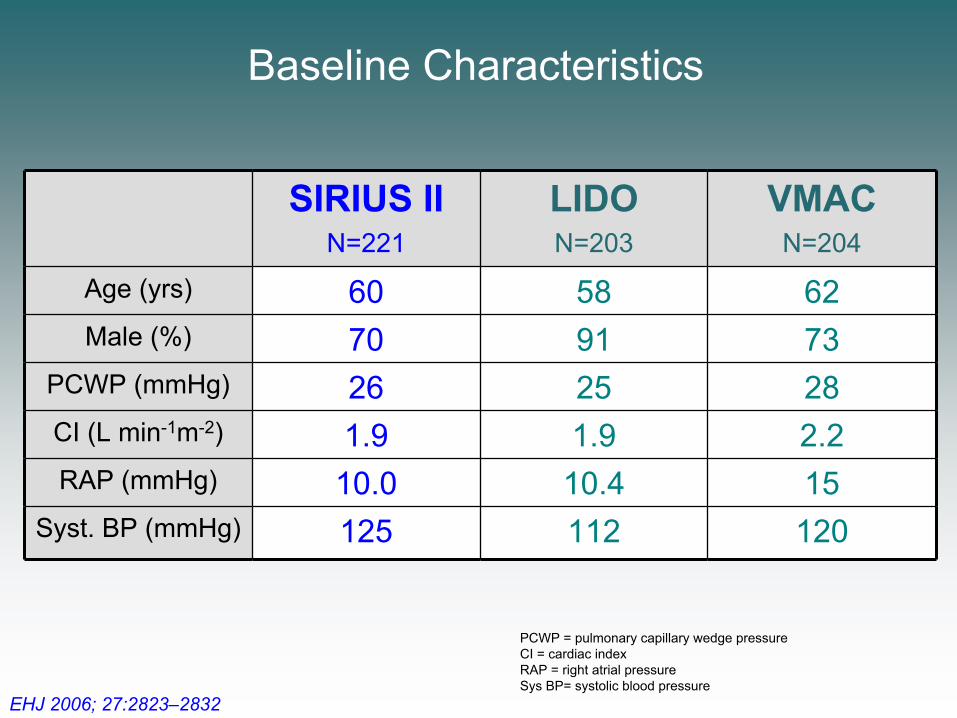
Baseline Characteristics
SIRIUS IIN=221
LIDON=203
VMACN=204
Age (yrs) 60 58 62Male (%) 70 91 73
PCWP (mmHg) 26 25 28CI (L min-1m-2) 1.9 1.9 2.2RAP (mmHg) 10.0 10.4 15
Syst. BP (mmHg) 125 112 120
PCWP = pulmonary capillary wedge pressureCI = cardiac indexRAP = right atrial pressureSys BP= systolic blood pressure
EHJ 2006; 27:2823–2832
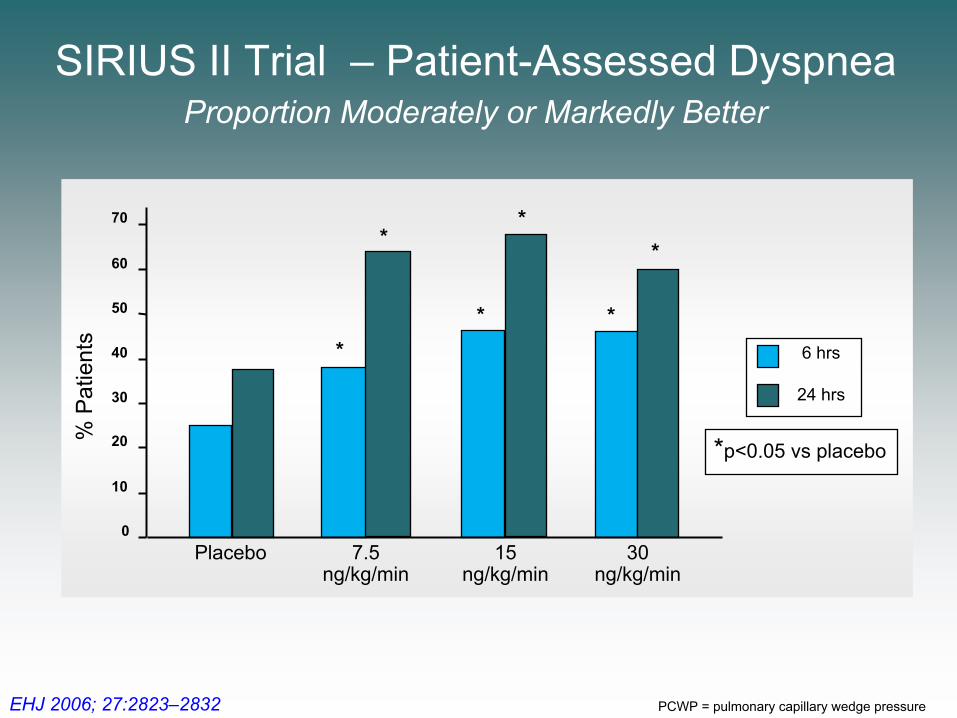
*p<0.05 vs placebo
24 hrs
6 hrs
% P
atie
nts
0
10
20
30
40
50
60
70
Placebo
** *
**
*
7.5ng/kg/min
15ng/kg/min
30ng/kg/min
SIRIUS II Trial – Patient-Assessed DyspneaProportion Moderately or Markedly Better
PCWP = pulmonary capillary wedge pressureEHJ 2006; 27:2823–2832

Ularitide improves the Cardiac Index
Time (Hours) -1 0 1 2 4 6 8 24 26
1.8
2.0
2.2
2.4
CI (
l/min
/m2 )
*
** *
* *** † †
† Placebo
7.5 ng /kg/min15 ng /kg/min
30 ng /kg/min
Ularitide Decreases Myocardial Consumption (Change from BL)
Placebo
7.5 ng /kg/min
15 ng /kg/min
30 ng /kg/min
EHJ 2006; 27:2823–2832

SIRIUS II Trial – Ularitide Reduces PCWPPrimary Endpoint at 6 hours
Placebo
7.5 ng /kg/min
15 ng /kg/min
30 ng /kg/min
* p<0.01 vs Placebo
*
*
*
*
*
**
**
*
*
*
†
† p<0.05 vs Placebo
- 12
- 10
- 8
- 6
- 4
- 2
0
0 2 4 6 8 10 12 14 16 18 20 22 24 26Time (Hours)
PCW
P (m
mH
g)
††
†
PCWP = pulmonary capillary wedge pressureEHJ 2006; 27:2823–2832

Ularitide does not worsen renal function – analyses through 72 hours –
1000
1200
1400
1600
1800
2000
2200
2400
ml /
24
h
Placebo 7.5 15 30
Urine Output / 24 h
-8-7
-6-5-4-3-2-1012
ml /
min
Creatinine Clearance
Placebo 7.5 ng 15 ng 30 ng
24 h
48 h72 h Total Incidences of
Creatinine Increases (> 25%)
% P
atie
nts
0
5
10
15
20
25
30
Placebo 7.5 ng 15 ng 30 ng
Serum Creatinine
-0.10
-0.05
0.00
0.05
0.10
0.15
0.20
Placebo 7.5 15 30
mg/
dL
EHJ 2006; 27:2823–2832
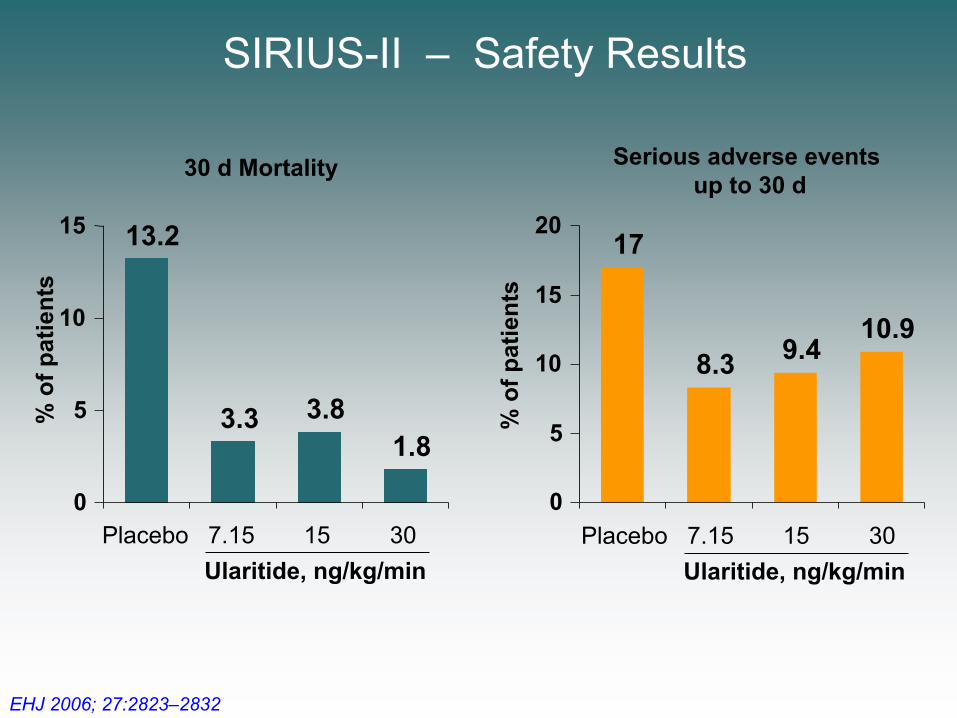
SIRIUS-II – Safety Results
30 d Mortality
13.2
3.3 3.81.8
0
5
10
15
% o
f pat
ient
s
Placebo 7.15 15 30Ularitide, ng/kg/min
Serious adverse events up to 30 d
17
8.3 9.410.9
0
5
10
15
20
% o
f pat
ient
sPlacebo 7.15 15 30
Ularitide, ng/kg/min
EHJ 2006; 27:2823–2832

The TRUE-AHF programme: Ularitide in patients with AHF
shifting a paradigm

• Multicenter, randomized, double blind, placebo-controlled trial, to evaluate the efficacy and safety of intravenous (IV) ularitide in patients suffering from AHF
• Patient enrolment has started across approximately 190 centres in the US, Europe and Canada
• Treatment: placebo or ularitide (15 ng/kg/min), 48 hrs. on top of standard care• Patients: up to 4,304 patients with AHF, randomisation 1:1• Screening: AHF, symptoms at rest, congestion, SBP ≥116mmHg, BNP ≥500 or
NT-BNP ≥2000 pg/mL, GFR ≥30, Furosemide i.v. bolus ≥40mg
Placebo i.v. (n=1,076–2,152)
Ularitide i.v. (n=1,076–2,152)

TRUE-AHF – Key Efficacy MeasuresPrim
ary
Endp
oint
Second
ary
Endp
oint
2,157 patients recruited as off 20th May, 2015

TRUE-AHFfinished
recruitment

Thank you !
Recommended

















