Transvenous Cardioversion—A NovelAsymmetric Rectangular BiphasicWaveform From a Radiofrequency
Defibrillator Compared WithConventional Waveforms in Atrial
Fibrillation
S.J. Walsh,* G. Manoharan,*,‡ O.J. Escalona,†,§ N. Evans,‡ J.D. Allen,‡
J. McC Anderson,† and A.A.J. Adgey*
Background: We investigated a novel device that delivered biphasic andmonophasic shocks without tilt, in transvenous cardioversion of atrial fibril-lation (AF). The device contains a radiofrequency (RF) transmitting primary, a15mm air gap and a passive secondary unit that produces the required directcurrent waveform. Methods: The device was assessed in 10 anaesthetised andventilated sheep (65 � SD 12kg). Defibrillation leads were positioned in thedistal coronary sinus and the lateral right atrium. The novel RF defibrillatorwas assessed using rectangular monophasic or biphasic pulses and compared toconventional (C) tilted waveforms (Ventritex HVS-02). During AF placeboshocks were delivered to a 50 � dummy load. Sustained AF was induced byrapid atrial pacing and 5 attempts at cardioversion were made for eachwaveform. Success was defined as reversion to sinus rhythm within 5 beats ofshock delivery. Results: No arrhythmic complications were observed for the400 shocks delivered. Conclusion: A reduction in phase 2 voltage does notaffect the efficacy of rectangular waveforms but does facilitate energy reduc-tion. Asymmetric rectangular biphasic waveforms with phase 2 voltage at 50%of phase 1 are more efficacious than equivalent voltage conventional wave-forms for transvenous cardioversion of AF. The novel defibrillator is safe andeffective. Design modifications will enable this device to be used as animplantable defibrillator with an external RF power source.
From the *Royal Victoria Hospital, Belfast; †University of Ulster, Jordanstown; ‡Queen’s University of Belfast,Northern Ireland; and §Universidad Simon Bolivar, Caracas, Venezuela.
© 2003 Elsevier Inc. All rights reserved.0022-0736/03/360S-0054$30.00/0doi:10.1016/j.jelectrocard.2003.09.057
Journal of Electrocardiology Vol. 36 Supplement 2003
191

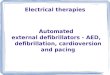
Fig. 2. Fluoroscopy image showing defibrillation elec-trode placement D-RAA, Active fixation electrode in theright atrial appendage; D-CS, Electrode in the distalcoronary sinus; S, Temporary pacing lead for stimulationof atrial fibrillation.
Table 1.
WaveformVoltage
(V)%
Success�
SEMMean
Energy (J)p for RF 6/6 ms
100/�50V versus
RF 12ms Monophasic 100 92 0.04 2.7 NSRF 6/6ms Biphasic 100/�100 88 0.05 2.5 NSRF 6/6ms Biphasic 100/�50 88 0.05 1.6 –RF 6/6ms Biphasic 50/�25 70 0.07 0.4 0.003C 12ms Monophasic 100 54 0.07 0.7 �0.001C 6/6ms Biphasic 100/�100 88 0.05 1.1 NSC 6/6ms Biphasic 100/�50 72 0.06 0.7 0.03Placebo 0 2 0.02 0 �0.001
Fig. 1. (A) Waveforms tested include an asymmetricrectangular biphasic waveform, (B) a rectangularmonophasic waveform, (C) a conventional monophasicwaveform, and (D) a conventional asymmetric biphasicwaveform.
192 Journal of Electrocardiology Vol. 36 Supplement 2003
Recommended