
British Journal of Plastic Surgery (2000), 53, 30-36 �9 2000 The British Association of Plastic Surgeons Article no. BJPS. 1999.3250 _ / .....
B R I T I S H J O U R N A L OF P L A S T I C S U R G E R Y
The versatile anterolateral thigh flap: a musculocutaneous flap in disguise in head and neck reconstruction
E Demirkan, H.-C. Chen, E-C. Wei, H.-H. Chen, S.-G. Jung*, S.-E Hau* and C.-T. Liao*
Department of Plastic and Reconstructive Surgery and *Department of Otorhinolaryngology, Chang Gung Memorial Hospital and College of Medicine, Chang Gung University, Taipei, Taiwan
SUMMARY. In search of an alternative soft tissue free flap donor site to radial forearm flap and rectus abdominis flap in head and neck reconstruction, we used the anterolateral thigh flap for reconstruction of various defects in the head and neck in 59 patients. The aim was to demonstrate the versatility of this donor site and propose a new approach to achieve a safer flap dissection. With the exception of three cases, all defects resulted from excision of malignant tumours. The defects were categorised as full thickness defects of the mandible (33.9%), full thickness defects of the cheek (52.5%) and others (13.6%). During the flap dissection a direct septocutaneous pedicle was observed in 12% of the cases. In the remaining cases there were only musculocutaneous perforators and the flaps were raised either as a split vastus lateralis musculocutaneous flap (72%) or as a perforator flap (16%), depending on the required thickness. Total flap survival was 96.7% with one total and one partial failure and two re-explo- rations (3.3%). The mean follow-up time was 7.1 months (range: 1-12 months). In conclusion, the anterolateral thigh flap is a versatile and dependable flap that can be adapted to any type of defect by modifying the flap design and composition. It should be considered to be a musculocutaneous flap of the vastus lateralis muscle that can also be raised as a perforator flap. When harvested and used in this context, the flap dissection becomes very safe and consistent, nullifying the only major disadvantage associated with this donor site. �9 2000 The British Association of Plastic Surgeons
Keywords: anterolateral thigh flap, head and neck reconstruction, musculocutaneous flap.
The qualities of the ideal soft tissue free flap for head and neck reconstruction may be defined as: l versatil- ity in design, adequate tissue stock, superior texture, minimal donor site morbidity, availability of diverse tissue types on one pedicle, potential for reinnerva- tion, large and long pedicle, feasibility of two team approach, and most importantly, consistent anatomy for an easy and safe flap dissection. The anterolateral thigh flap, which was first described by Song et al in 1984, had all of these qualifications except for the last one. z4 It was originally described as a septocutaneous flap based on the descending branch of the lateral femoral circumflex artery. 2 However, it was later found that in the majority of cases there were only musculocutaneous perforators, 5 7 and moreover, both septocutaneous 8 and musculocutaneous perforators 9 could originate from vessels other than the descending branch of the lateral femoral circumflex artery. This variability in the vascular anatomy is the main factor which precludes widespread clinical use of this donor site despite reports of some successful series in the literature.3,10-13
Two years ago, we began to use the anterolateral thigh flap in head and neck reconstruction in search of a new donor site that was versatile and had minimal donor site morbidity. After our initial experience with the flap dissection, we felt that this flap should be con- sidered to be a musculocutaneous flap of the vastus
lateralis muscle rather than a septocutaneous flap with frequently missing septocutaneous perforators. Then, we began to use this donor site mainly as a musculo- cutaneous flap alternative to rectus abdominis flap in reconstruction of medium to large size oromandibular defects. When required, a skin flap could always be harvested and even thin flaps could be obtained, obviating the use of radial forearm flaps. Here, we present 59 consecutive head and neck reconstructions illustrating the versatile use of the anterolateral thigh flap and propose a new dissection approach that makes the flap harvest easier and safer.
Patients and methods
Between January 1997 and March 1998, 59 patients underwent oral reconstruction using 60 anterolateral thigh flaps. Patients' ages ranged from 13 to 79 years with an average of 56 years. There were 55 males and 4 females. In 56 cases the defects resulted from excision of malignant tumours. In the other three, stricture of the cervical oesophagus due to corrosive injury, soft tissue defect in the cheek due to foreign body excision and secondary soft tissue deficit following previous microsurgical oromandibular reconstruction were the pathologic lesions. In oncologic cases most of the tumours were located in the buccal mucosa (67%)
30
Anterolateral thigh musculocutaneous flap 31
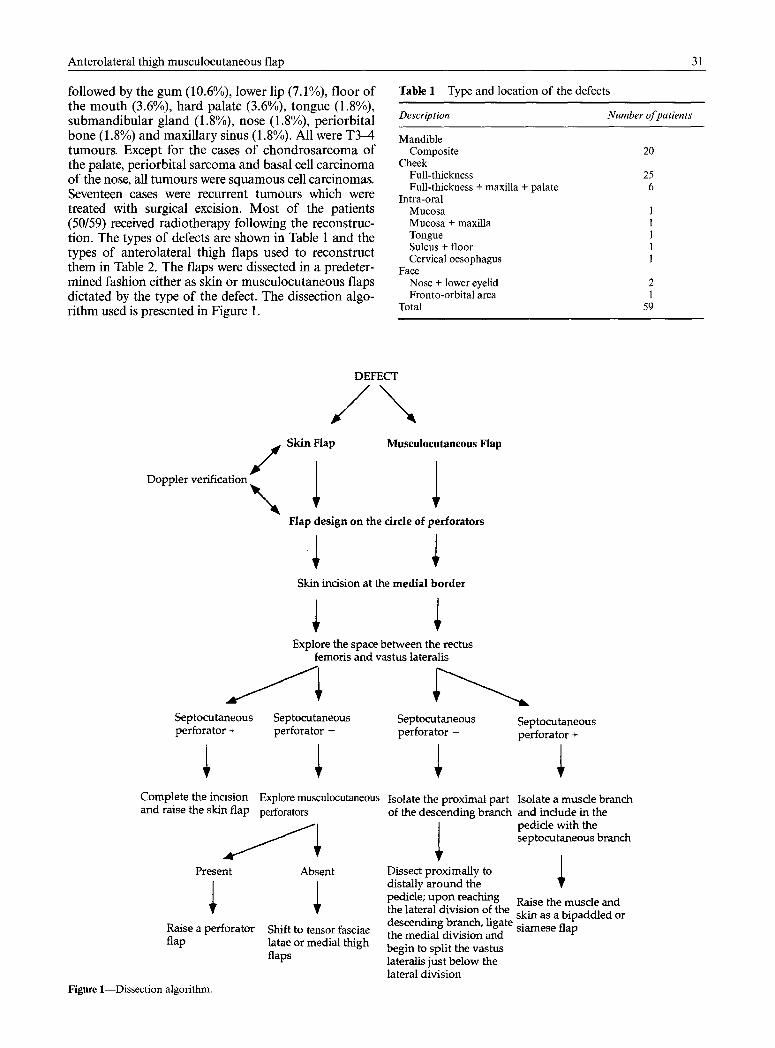
followed by the gum (10.6%), lower lip (7.1%), floor of the mouth (3.6%), hard palate (3.6%), tongue (1.8%), submandibular gland (1.8%), nose (1.8%), periorbital bone (1.8%) and maxillary sinus (1.8%). All were T3-4 tumours. Except for the cases of chondrosarcoma of the palate, periorbital sarcoma and basal cell carcinoma of the nose, all tumours were squamous cell carcinomas. Seventeen cases were recurrent tumours which were treated with surgical excision. Most of the patients (50/59) received radiotherapy following the reconstruc- tion. The types of defects are shown in Table 1 and the types of anterolateral thigh flaps used to reconstruct them in Table 2. The flaps were dissected in a predeter- mined fashion either as skin or musculocutaneous flaps dictated by the type of the defect. The dissection algo- rithm used is presented in Figure 1.
Table 1 Type and location of the defects
Description Number of patients
Mandible Composite 20
Cheek Full-thickness 25 Full-thickness + maxilla + palate 6
Intra-oral Mucosa 1 Mucosa + maxilla 1 Tongue l Sulcus + floor 1 Cervical oesophagus 1
Face Nose + lower eyelid 2 Fronto-orbital area 1
Total 59
Doppler verification / \
DEFECT
/ \ Skin F l a p Musculocutaneous Flap
Flap design on the circle of perforators
Skin incision at the medial border
Explore the space between the rectus femoris and vastus lateralis
Septocutaneous perforator -
Explore musculocutaneous perforators
Septocutaneous perforator +
Complete the incision and raise the skin flap
J l Present
Raise a perforator flap
Figure 1--Dissection algorithm.
Absent
Shift to tensor fasciae latae or medial thigh flaps
Septocutaneous Septocutaneous perforator - perforator +
Isolate the proximal part Isolate a muscle branch of the descending branch and include in the
pedicle with the septocutaneous branch
Dissect proximally to / distally around the T pedicle; upon reaching Raise the muscle and the lateral division of the skin as a bipaddled or descending branch, ligate siamese flap the medial division and begin to split the vastus lateralis just below the lateral division

32 British Journal of Plastic Surgery
Table 2 Flap types used
Type Number
Skin Septocutaneous 7 Perforator 10
Musculocutaneous 43 Total 60
Flap dissection
With the patient in the supine position, a line is drawn from the anterior superior iliac spine to the supero- lateral border of the patella. This line represents the intermuscular septum between the rectus femoris and vastus lateralis muscles. Next, a circle with a 3 cm radius is marked at the midpoint of this line. When a musculocutaneous flap is going to be raised, it is cen- tred on this circle (Fig. 2A). Wolff and Grundmann's anatomic dissections in 60 cadavers showed that the main septocutaneous perforator was located within 3 cm of the midpoint of this line proximally and dis- tally in 95% of the cases. TM Recently, Kimata et al
reported a similar preponderance of perforators at the same location. 6 If a skin-only flap is required, then a Doppler verification of the perforators is performed and the skin flap is designed to include all of these per- forators. The inferolateral quadrant of this circle is the location of at least one perforator in 80% of the cases according to the Doppler studies of Xu et a l :
Dissection begins at the medial border of the flap, which should be located over the rectus femoris muscle for two reasons: first to prevent injury to cutaneous perforators that may originate from the intermuscular septum, and second to have access to the anteromedial thigh flap region. The incision is made through the deep fascia and the flap is raised laterally for a short distance until the intermuscular septum between the rectus femoris and vastus lateralis is reached. At that point the descending branch of the lateral femoral cir- cumflex artery is explored and the presence of a direct septocutaneous perforator is verified (Fig. 2B). However, the chance of finding an isolated septocuta- neous perforator is quite low (12% of the cases in this study). Most of the time there is indeed a prominent branch taking off from the descending branch at the described location but it is either partially or com- pletely buried in the vastus lateralis muscle on its course to the skin (Fig. 2C). This musculocutaneous branch is called the lateral division of the descending branch. It is well described in the study of Xu et aP and
Rectus F~cr ts
Figure 2 (A) Flap design. The flap is centred on the lower lateral quadrant of a line drawn from the anterior superior iliac spine to the lateral border of the patella. The anterior border of the flap should be located on the rectus femoris muscle which is medial to this line. (B) A scptocutaneous perfbrator may be found in the intermuscular septum between the vastus lateralis and rectus femoris muscles in only 12% of the cases. (C) A prominent branch taking off from the descending branch may be found in the intermuscular septum proximally but it is usually buried into the vastus lateralis muscle (arrow) in its distal course to the skin. It is called the lateral division. (D) A musculocutaneous flap can be raised by splitting the muscle tangentially just below the lateral division in a proximal to distal direction. The motor nerve of the muscle (arrow) should be preserved.

Anterolateral thigh musculocutaneous flap 33
referred to as the proximal muscular branch by Wolff and Howaldt. is It usually enters the muscle at the junc- tion of its cranial and middle thirds and about halfway in its thickness. It is always accompanied by a branch of the motor nerve. If some muscle is desired to be included in the flap, then with a proximal to distal dis- section from the pedicle, the muscle is split tangentially on its long axis just below the lateral division and the upper portion is raised with the skin flap (Fig. 2D). Musculocutaneous perforators are not explored b u t the part of the muscle under the circle of perforators is always included. Peripheral to this only the deep fascia needs to be included. By raising the flap in a centripetal fashion from the lateral division of the descending branch, it is always possible to identify all perforators and further trim the muscle for a custom fit to the indi- vidual defect. The largest flap raised in this way with- out partial loss was 34 x 14 cm in dimension.
When a skin-only flap is planned and no septocuta- neous perforators can be found, then the largest musculocutaneous perforator is explored. The perfora- tor is usually found in the cranial one third or at the junction of the cranial and middle thirds of the muscle. The possibility of finding a major perforator that may descend from the transverse branch and enter the muscle from its superior aspect quite superficially (described as the horizontal perforator by Zhou et al) 9 should be kept in mind while incising the upper border of the flap. If there is more than one perforator the largest one should be followed and after verification of its origin others can be divided and the incision can be completed. One musculocutaneous perforator is suffi- cient to raise a large skin flap (largest 20 x 12 cm in this study). Perforators can be skeletonised as described by Kimura and SatohJ 6 The musculocutaneous perfora- tor originated from the transverse branch of the lateral femoral circumflex artery in 10% of the cases in this study.
If a musculocutaneous flap is planned and dissec- tion reveals a septocutaneous perforator, then the skin and muscle parts may be raised on different branches of the same vascular pedicle as a bipaddled composite flap.
If no septo- or musculocutaneous perforators are found or if they are inadvertently divided, the dissected skin island can be salvaged as a tensor fascia lata flap based on the transverse branch by extending the inci- sion and flap design laterally to include the fasciae latae zone. Alternatively, an anteromedial thigh flap can be raised through the same incision. The skin flap medial to the initial vertical incision on the rectus femoris muscle can be undermined below the deep fas- cia to explore the anteromedial thigh flap perforators that are located between the rectus femoris and vastus intermedius muscles. They originate from the innomi- nate artery, which is a direct branch of the lateral femoral circumflex artery or an extension of its descending branch. Therefore it is better to avoid a cir- cumferential incision at the beginning of the flap dis- section until the vascular pedicle is clearly identified and preserved. The main trunk of the motor nerve to the vastus lateralis muscle and its branches to
the remaining parts of the muscle should also be preserved. If a sensory flap is desired lateral femoral musculocutaneous nerve innervating the anterolateral thigh region may be dissected on its course above the deep fascia and included in the flap. Motor reinnerva- tion of the myocutaneous flap is also possible by means of the motor branch accompanying the vascular pedicle.
Results
Total flap survival rate was 96.6% with one total and one partial failure. The total failure occurred in a case where the flap was dissected as a perforator flap. In this case, as an anatomical variant, the artery of the lateral division did not follow the vein and the flap was inad- vertently raised on the part of the pedicle that con- tained only the vein and the nerve. The defect was reconstructed with the contralateral anterolateral thigh flap. The partial flap loss was due to infection. Two re-explorations were done due to venous congestion (3.3%: 2 out of 60 flaps). One was found to be related to tight skin sutures and the other to a haematoma in the neck. Both flaps were salvaged. Two patients experienced wound dehiscence and were treated conservatively.
The donor sites were closed by a skin graft in 18 cases. Primary closure was possible in the remaining cases when the flap width was under 8 cm. Two partial graft losses were encountered due to local infection (3.3%). These defects were closed with a second skin grafting procedure. There was no impairment in knee extension in evaluations done on patients who reached the sixth postoperative month.
The mean follow-up time was 7.1 months (range: 1-12 months). Two reconstruction plates were exposed during the second postoperative month (10%: 2 out of 20 cases where a reconstruction plate was used). One patient was receiving radiotherapy when the plate was exposed at the anterolateral margin. A deltopectoral flap was used to cover the plate. In the other case, rearrangement of the anterolateral thigh flap allowed primary soft tissue closure over the exposed plate at the posterior margin.
Case report
A 52-year-old male patient was admitted for treatment of a T4NOM0 squamous cell carcinoma of the right buccal rnucosa. During the tumour excision a right functional neck dissection with a full-thickness cheek excision and marginal mandibulectomy was performed. The mucosal defect was 13 • 7 cm, the skin defect measured 9 x 6 cm. The left anterolateral thigh flap was harvested with a muscle strip. The flap was folded over to cover both the inner and outer linings. Anastomoses were performed to the right superior thyroid artery and a tributary of the internal jugular vein. The postop- erative period was uncomplicated. A commissuroplasty was performed to prevent occasional drooling. The patient received 4680 cGy radiotherapy. He was still alive at the eighth postoperative month and was on regular diet, had oral conti- nence and an interincisal opening of 3.2 cm (Fig. 3 A D).

34 British Journal of Plastic Surgery
Figure 3~(A) Full-thickness cheek defect with marginal mandibulectomy. (B) A musculocutaneous flap raised with minimal amount of muscle (only the muscle part that underlies the circle of perforators was included). (C) Postoperative appearance at 8 months following radiotherapy. Facial contour preserved. (D) Mouth opening preserved.
Discussion
There may be no single ideal soft tissue free flap in head and neck reconstruction as the defects in this region can vary tremendously in composition and tex- ture within short distances. Therefore bulk and pliabil-
ity represent two opposing features critical in flap selection for this area. I f a donor site could provide variable types of soft tissue flaps when required it would be closer to the ideal. The most important aspect of the anterolateral thigh flap in reconstruction of head and neck carcinoma is its versatility in design

Anterolateral thigh musculocutaneous flap 35
and composition. While a very thin, pliable innervated flap for intraoral reconstruction may be harvested in one patient, the whole vastus lateralis muscle can be included to reconstruct a massive perioral defect in another. Furthermore, composite bipaddled flaps can be designed including the anteromedial thigh flap or the tensor fasciae latae flap on the same vascular pedicle 4 and chimeric and mosaic flaps where a vascularised bone or another soft tissue flap can be anastomosed to a side branch or the distal run off of the skin f l a p . 6'7'17 19 Myofascial or functional neuro- muscular flaps of the vastus lateralis muscle may also be raised. 14,16
With this diversity in design and composition, the anterolateral thigh musculocutaneous flap can cover most of the indications of two commonly used soft tissue free flaps in head and neck reconstruction, namely the radial forearm flap 2~ and the rectus abdo- minis musculocutaneous flaps. 21 Recently Ao et al have also indicated that the morbidity resulting from these two donor sites cannot be overlooked when a versatile alternative such as the anterolateral thigh flap is pre- sent? The radial forearm flap is successful when used as a thin intraoral lining flap 22 but it commonly leads to a sunken appearance when used for defects of the cheek or face, particularly following gadiotherapy. 23,26 Soft tissue augmentation with dermofat grafts or even with a second free flap may be necessary in those cases. 23 Moreover, the flap size is limited and a conspic- uous donor site scar may not be avoidable as primary closure is almost never possible. On the other hand, a defect of 8 cm in the anterolateral thigh region may be closed primarily and looks more acceptable aestheti- cally. Should a skin graft be harvested, the adjacent part of the same thigh is readily available. Disposal of a major artery to the hand is another drawback of the long abused radial forearm donor site.
In the case of rectus abdominis musculocutaneous flaps, the subcutaneous fat usually creates excessive bulk which requires either intraoperative reduction or multiple postoperative debulking procedures. Although thin extended rectus abdominis flaps have been described, 24 the best thin flap according to Kimura and Satoh is the anterolateral thigh flap, because more uni- form thinning is allowed by the anatomy of its perfora- tor. 16 Donor site morbidity may be significant with the rectus abdominis flap such as hernia development 2~ and deterioration of the pulmonary function in certain patients. 2s The functional deficit following flap eleva- tion was minimal and temporary in this series even when a significant portion of the vastus lateralis muscle was included. The vastus lateralis muscle is a synergist of the other three knee extensors and its removal does not affect leg function. Wolff and Grundmann also stated that there was no motor dys- function following vastus lateralis muscle transfer in their series confirmed by clinical comparison of the load capacity of both legs. ~4 A similar study is being carried out on our patients for anterolateral musculo- cutaneous flaps.
The major problem with the anterolateral thigh donor site has been the variation in the origin and
course of the supplying perforators. Following the ini- tial description of this flap as a constant septocuta- neous flap based on the descending branch of the lateral femoral circumflex artery, 2 a septocutaneous perforator from that source was identified in only 10-40% of the cases in various studies. 3-9,12,13 Additionally, Koshima et al stated that in some cases the septocutaneous perforators originated from the transverse branch of the lateral circumflex femoral artery or directly from the deep femoral artery. 4 According to Zhou et al musculocutaneous perforators had also a variable source and in 6.3% of the cases they arose from the transverse branch of the lateral circum- flex femoral artery. 9 In the largest series in the litera- ture, Kimata et al reported that the perforators originated from the descending branch in 84.3% of the cases and the proportion of septocutaneous perfora- tors to all perforators in 70 cases was 18.1~ 6 In our series of 60 flaps, the anatomical findings recorded during the flap dissection revealed that a septo- cutaneous perforator was present in only 12% of the cases and was always from the descending branch of the lateral circumflex femoral artery. The remaining flaps had musculocutaneous perforators which were derived either from the descending or transverse branch of the lateral femoral circumflex artery. In our opinion, a skin flap supplied by musculocutaneous perforators in 88% of the cases should be classified as a musculocutaneous flap. Accepting this high incidence of musculocutaneous perforators as a variation of a septocutaneous flap is confusing and may result in errors in dissection if the preoperative plan is to raise a septocutaneous flap.
The types of defects reconstructed with the antero- lateral thigh flap varied significantly in the presented series. However, the most common application was the reconstruction of middle to large sized full-thickness cheek and mandibular defects (85% of cases). Excellent space filling and contour were obtained with the musculocutaneous version of the flap. Ao et al used partially de-epithelialised or chimerically com- bined anterolateral thigh flaps for the same purpose, 7 however, similar results were achieved in our study with the musculocutaneous anterolateral thigh flap which is technically much easier and faster. There were 20 cases of composite mandibular defects (33%) in this series but no vascularised bone transfers were per- formed and a reconstruction plate was used instead in combination with the anterolateral thigh flap. This was a select group of patients with multiply recurrent tumours and poor prognosis, as for all other cases a vascularised bone transfer is the standard reconstruc- tive procedure in our department. 2~28
The only two minor disadvantages of this flap are the high incidence of hairy skin in that area in male patients, and donor site scars associated with the use of skin grafts in large defects. The latter may preclude its use, particularly in female patients.
In conclusion, at our institution the anterolateral thigh flap is replacing the other two commonly used soft tissue free flaps in head and neck reconstruction, as it is an extremely versatile flap with multiple advan-

36 British Journal of Plastic Surgery !
tages. By c o n s i d e r i n g this f lap as a m u s c u l o c u t a n e o u s f lap o f t he vas tus la tera l i s musc le tha t can a lso be ra i sed as a p e r f o r a t o r f lap, a safer a n d fas te r d i s sec t ion c a n be done . We p r o p o s e the an t e ro l a t e r a l t h igh f lap as the n e w w o r k h o r s e in r e c o n s t r u c t i o n o f any type o f ab la t ive defec ts in h e a d a n d neck c a r c i n o m a .
References
i. Hayden RE. Microvascular free flaps for soft-tissue defects. Otolaryngol Clin N Am 199t; 24: 1343-59.
2. Song YG, Chert GZ, Song YLI The free thigh flap: a new free flap concept based on the septocutaneous artery. Br J Hast Surg 1984; 37: 149-59.
3. Koshima I, Fukuda H, Yamamoto H, Moriguchi T, Soeda S, Ohta S. Free anterolateral thigh flaps for reconstruction of head and neck defects. Hast Reconstr Surg 1993; 92:42 l-8.
4. Koshima I, Hosoda M, Moriguchi T, Hamanaka T, Kawata S, Hata T. A combined anterolateral thigh flap, anteromedial thigh flap, and vascularized iliac bone graft for a full-thick- ness defect of the mental region. Ann Hast Surg 1993; 31: 175-80.
5. Xu DC, Zhong SZ, Kong JM, et al. Applied anatomy of the anterolateral femoral flap. Plast Reconstr Surg 1988; 82: 305-10.
6. Kimata Y, Uchiyama K, Ebihara S, Nakatsuka T, Harii K. Anatomic variations and technical problems of the anterolat- eral thigh flap: a report of 74 cases. Hast Reconstr Surg 1998; 102: 1517-23.
7. Ao M, Uno K, Maeta M, Nakagawa E Saito R, Nagase Y. De- epithelialised anterior (anterolateral and anteromedial) thigh flaps for dead space filling and contour correction in head and neck reconstruction. Br J Plast Surg 1999; 52: 261-7.
8. Koshima I, Fukuda H, Utunomiya R, Soeda S. The antero- lateral thigh flap; variations in its vascular pedicle. Br J Hast Surg 1989; 42: 260-2.
9. Zhou G, Qiao Q, Chen GY, Ling YC, Swift R. Clinical experi- ence and surgical anatomy of 32 free anterolateral thigh flap transplantations. Br J Plast Surg 1991; 44: 91-6.
10. Walton RL. Discussion in Koshima I, Fukuda H, Yamamoto H, Moriguchi T, Soeda S, Ohta S. Free anterolateral thigh flaps for reconstruction of head and neck defects. Hast Reconstr Surg 1993; 92: 429-30.
11. Cormack G. Anterolateral thigh flap: technical tip to facilitate elevation. Br J Plast Surg 1992; 45: 74.
12. Kimata Y, Uchiyama K, Ebihara S, et al. Versatility of the free anterolateral thigh flap for reconstruction of head and neck defects. Arch Otolaryngol Head Neck Surg 1997; 123: 1325-31.
13. Pribaz J J, Orgill DR Epstein MD, Sampson CE, Hergrueter CA. Anterolateral thigh fi'ee flap. Ann Hast Surg 1995; 34: 58592.
14. Wolff K-D, Grundmann A. The free vastus lateralis flap: an anatomic study with case reports. Hast Reconstr Surg 1992; 89: 469-75.
15. Wolff K-D, Howaldt H-R Three years of experience with the free vastus lateralis flap: an analysis of 30 consecutive reconstruc- tions in maxillofacial surgery. Ann Hast Surg 1995; 34: 35-42.
16. Kimura N, Satoh K. Consideration of a thin flap as an entity and clinical applications of the thin anterolateral thigh flap. Hast Reconstr Surg 1996; 97: 985-92.
17. Hallock GG. Simultaneous transposition of anterior thigh muscle and fascia flaps: an introduction to the chimera flap principle. Ann Plast Surg 1991; 27: 126-31.
18. Koshima I, Yamamoto H, Hosoda M, Moriguchi T, Orita Y, Nagayama H. Free combined composite flaps using the lat-
eral circumflex femoral system for repair of massive defects of the head and neck regions: an introduction to the chimeric flap principle. Plast Reconstr Surg 1993; 92:411-20.
19. Koshima I, Yamamoto H, Moriguchi T, Orita Y. Extended ante- rior thigh flaps for repair of massive cervical defects involving pharyngoesophagus and skin: an introduction to the 'mosaic' flap principle. Ann Hast Surg 1994; 32: 321-7.
20. Vaughan ED. The radial forearm free flap in orofacial recon- struction. J Craniomaxillofac Surg 1990; 18: 2-7.
21. Nakatsuka T, Harii K, Yamada A, Asato H, Ebihara S. Versatility of a free inferior rectus abdominis flap for head and neck reconstruction: analysis of 200 cases. Hast Reconstr Surg 1994; 93: 76~9.
22. Evans GRD, Schusterman MA, Kroll SS, et al. The radial fore- arm free flap for head and neck reconstruction: a review. Am J Surg 1994; 168: 446-50.
23. Wei F-C, Demirkan F, Chen H-C, Chen I-H, Liao C-T, Hau S-R Management of secondary soft-tissue deficits following microsurgical head and neck reconstruction by means of another free flap. Hast Reconstr Surg 1999; 103:1158-67.
24. Akizuki T, Harii K, Yamada A. Extremely thinned inferior rectus abdorninis free flap. Hast Reconstr Surg 1993; 91: 936-41.
25. Kroll SS, Baldwin BJ. Head and neck reconstruction with the rectus abdominis free flap. Clin Hast Surg 1994; 21: 97-108.
26. Wei F-C, Demirkan F, Chen H-C, Chen I-H. Double free flaps in reconstruction of extensive composite mandibular defects in head and neck cancer. Hast Reconstr Surg 1999; 103: 39-47.
27. Chen H-C, Demirkan F, Wei F-C, Cheng S-L, Cheng M-H, Chen I-H. Free fibula osteoseptocutaneous-pedicled pec- toralis major myocutaneous flap combination in reconstruc- tion of extensive composite mandibular defects. Hast Reconstr Surg 1999; 103: 839-45.
28. Demirkan F, Wei F-C, Chen H-C, Chen I-H, Hau S-R Liau C-T. Microsurgical reconstruction in recurrent oral cancer: use of a second free flap in the same patient. Hast Reconstr Surg 1999; 103: 829-38.
The Authors
Ferit Demirkan MD, Consultant Plastic Surgeon,
Mevki Ankara Hospital, A. Ayranci, Yaylagtil Sok. 8-13, 06540, Ankara, Turkey.
Hung-chi Chen MD, FACS, Professor, Fu-ehan Wel MD, FACS, Professor and Chief, Hern-hsin Chen MD, Attending Plastic Surgeon,
Department of Plastic and Reconstructive Surgery
Sung-gyung Jung MD, Assistant Professor, Sheng-po Hau MD, Associate Professor, Chun-ta Liao MD, Associate Professor,
Department of Otorhinolaryngology,
Chang Gung Memorial Hospital, University of Chang Gung, College of Medicine, 5 Fu-Hsing Street, Kwei-Shan, Tao-Yuan 333, Taiwan.
Correspondence to Dr Hung-Chi Chen
Paper received 26 February 1999. Accepted 13 September 1999, after revision.
Recommended

















