
Archives of Gerontology and Geriatrics
26 (1998) 227–234
The prehospitalization functional and cognitivestatus and the course of acute infectious disease in
the elderly
Yichayaou Beloosesky *, Boris Grosman, Anatoly Katsen,Joseph Grinblat
Department of Geriatrics, Rabin Medical Center, Campus Golda, Hasharon Hospital, P.O.B. 121,Petah-Tiq6a 49372, Israel
Received 30 September 1997; received in revised form 8 January 1998; accepted 9 January 1998
Abstract
A total of 105 elderly patients hospitalized for acute infectious disease were classified intoprehospital demented and non demented groups and into dependent and independentgroups. Demographic data, clinical and biological parameters and previous health problemswere recorded. There was a significant difference between the two cognitive and functionalgroups in complications, length of stay, dehydration, confusion, albumin and hemoglobin. Alogistic regression analysis taking into account the epidemiologic parameters, functional andcognitive status and the medical health problems has shown that only age, dementia andprevious neurologic disease (mainly stroke) are independent risk factors for confusion andcomplications. Thus, the prehospitalization function, cognitive status and previous neuro-logic disease in elderly patients with acute infections may have a predictive and prognosticvalue. © 1998 Elsevier Science Ireland Ltd. All rights reserved.
Keywords: Acute infectious disease; Dementia; Ageing; Dependency
* Corresponding author.
0167-4943/98/$19.00 © 1998 Elsevier Science Ireland Ltd. All rights reserved.
PII S0167-4943(98)00005-3
Y. Beloosesky et al. / Arch. Gerontol. Geriatr. 26 (1998) 227–234228
1. Introduction
Infectious diseases are the leading cause of hospital admissions among frailelderly people, more than cardiovascular, gastrointestinal, orthopedic, or otherdiseases (Irvine et al., 1984; Jones, 1990). In geriatric institutions, the prevalence ofinfectious diseases is high, reaching 5–18% (Garibaldi et al., 1981; Price et al., 1985;Scheckler and Peterson, 1986; Michel et al., 1991). The main disabilities that definefrail and vulnerable elderly patients are immobility, incontinence, and dementia(Jones, 1990). The most frequent infections in the elderly are those of the respira-tory and urinary tracts, and of the skin (Nicolle et al., 1984; Jackson and Fierer,1985; Setia et al., 1985; Darnowski et al., 1991).
Several publications dealing with infections have shown that elderly patients needlonger hospitalization periods as compared to younger patients (Myhre, 1983;Clinton et al., 1992) and the prognosis in bacteremia is lower in dependent patients(McCue, 1987; Watanakunahorn et al., 1993) and in those with hypoalbuminemia(Azoulay et al., 1977; Whitelaw et al., 1992; Leibovici et al., 1993).
The aim of the present study was to examine the relationship between thefunctional and cognitive decline and the course of acute infectious diseases inhospitalized elderly patients.
2. Methods
The files of 105 elderly patients, hospitalized in the acute geriatric ward of ourhospital, between 1993–1994, for acute infectious diseases were reviewed. In ourstudy, we did not include the patients hospitalized for other diseases who laterdeveloped an infectious disease or patients about whom we had an incompletefunctional and cognitive information. We also excluded patients with plasmacreatinine equal to or higher than 1.5 mg/dl. The data included age, sex, living placeand health problems.
The prehospitalization functioning was established by a team composed of ageriatrician, a specialized nurse and a social worker, using the Modified RankinScale (MRS) (Bamford et al., 1989), and by interviewing the patients’ family andthe care givers.
The patients were divided into two groups: independent and dependent (0–2 and3–5 score, respectively, in the MRS). An additional classification into three groupswas also made: independent, partially dependent and dependent (0–1, 2–3, 4–5,respectively, in the MRS).
The prehospitalization cognitive estimation was done by the geriatrician and thespecialized nurse, according to the information given by the patients’ family, caregivers and especially by the physician in the community or the nursing home. Twocognitive groups of patients were determined: normal or mildly demented, andmoderate to severe demented patients.
In the first 24 h of hospitalization, the following clinical and laboratory data werenoted: maximal rectal fever, confusion, dehydration, hemodynamic changes andcomplete blood count, urea, electrolytes and albumin.

Y. Beloosesky et al. / Arch. Gerontol. Geriatr. 26 (1998) 227–234 229
The length of stay in hospital was calculated from the first hospitalization dayuntil they returned home, or to a nursing home or until they were transferred to arehabilitation service.
The complications encountered were: death, secondary infections, falls andtrauma just before and during hospitalization, cardiorespiratory complications(pulmonary edema,arrhythmia, myocardial infarction, mechanical ventilation),pressure sores, thromboembolic events, acute renal failure, drug reactions, surgicalinterventions and further deterioration necessitating a transfer to a rehabilitationservice.
The statistical analysis was done by the Student’s t-test for continuous variables(age, hemoglobin, albumin and length of stay), and the x2 for the categorialvariables (confusion, dehydration and complications). We also used the logisticregression analysis to emphasize the independent factors for length of stay, dehy-dration, confusion and complications.
3. Results
The age range was between 65 and 95 years, mean age 81.5 years and median age83 years. The age, sex, place of living, functional and cognitive states are summa-rized in Table 1. The infections are detailed in Table 2. The most frequent infectionswere the upper and lower respiratory tract infections (39 cases), urinary tractinfections and urosepsis (31 cases).
The patients’ medical problems are detailed in Table 3. Of the 25 patients withneurological problems, 23 have had a stroke and two suffered from Parkinson’sdisease. The six diabetic patients were treated with insulin, the other 28 patientswere treated orally. The orthopedic patients were mainly those after hip surgery andsevere gonarthrosis.
The fever range was between 36.4 and 40.6°C, the mean was 38.5°C, and tenpatients had a fever 537.5°C, while 22 had a fever ]39.1°C.
Table 1Baseline demographic, functional and cognitive status of the 105 patients studied
Parameters n %
PatientsMales 56 53.3
49 46.7Females
77.181Living at home24.924Living in nursing home37.139Independent patients (Rankin scale 0–2)62.966Dependent patients (Rankin scale 3–5)
61 58.0Non or mildly demented42.044Moderate to severely demented
Y. Beloosesky et al. / Arch. Gerontol. Geriatr. 26 (1998) 227–234230
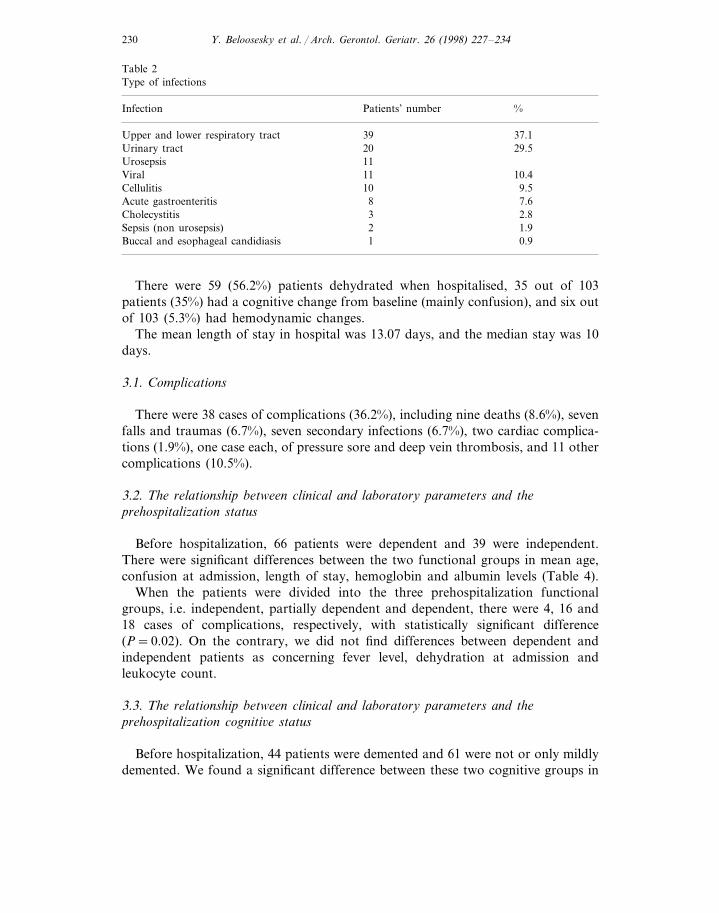
Table 2Type of infections
Patients’ number %Infection
39 37.1Upper and lower respiratory tractUrinary tract 29.520
11Urosepsis10.411Viral
9.510Cellulitis7.68Acute gastroenteritis2.83Cholecystitis1.92Sepsis (non urosepsis)0.91Buccal and esophageal candidiasis
There were 59 (56.2%) patients dehydrated when hospitalised, 35 out of 103patients (35%) had a cognitive change from baseline (mainly confusion), and six outof 103 (5.3%) had hemodynamic changes.
The mean length of stay in hospital was 13.07 days, and the median stay was 10days.
3.1. Complications
There were 38 cases of complications (36.2%), including nine deaths (8.6%), sevenfalls and traumas (6.7%), seven secondary infections (6.7%), two cardiac complica-tions (1.9%), one case each, of pressure sore and deep vein thrombosis, and 11 othercomplications (10.5%).
3.2. The relationship between clinical and laboratory parameters and theprehospitalization status
Before hospitalization, 66 patients were dependent and 39 were independent.There were significant differences between the two functional groups in mean age,confusion at admission, length of stay, hemoglobin and albumin levels (Table 4).
When the patients were divided into the three prehospitalization functionalgroups, i.e. independent, partially dependent and dependent, there were 4, 16 and18 cases of complications, respectively, with statistically significant difference(P=0.02). On the contrary, we did not find differences between dependent andindependent patients as concerning fever level, dehydration at admission andleukocyte count.
3.3. The relationship between clinical and laboratory parameters and theprehospitalization cogniti6e status
Before hospitalization, 44 patients were demented and 61 were not or only mildlydemented. We found a significant difference between these two cognitive groups in

Y. Beloosesky et al. / Arch. Gerontol. Geriatr. 26 (1998) 227–234 231
Tab
le3
The
med
ical
prob
lem
s
Hea
lth
prob
lem
s%
nC
lass
ifica
tion
Dep
ende
ntN
on-d
emen
ted
Dem
ente
dIn
depe
nden
t %n
%n
%n
%n
59.6
3268
.115
40.4
31.9
Isch
emic
hear
tdi
seas
e28
1944
.847 24
1354
.217
70.8
729
.222
.911
Con
gest
ive
hear
tfa
ilure
45.8
31.6
1368
.49
47.4
1052
.618
.1C
hron
icat
rial
fibri
llati
on6
1961
.822
64.7
1235
.321
Dia
bete
s38
.213
32.4
3445
.522
66.7
1133
.3C
hron
icob
stru
ctiv
elu
ngdi
seas
e33
31.4
1854
.515
91.6
1144
.024
56.0
23N
euro
logi
cde
ficit
8.4
322
.825
14.3
1285
.76
42.9
857
.1O
rtho
pedi
cdi
seas
e14
13.3
290
.95
45.5
654
.510
10.5
Ane
mia
and
othe
rha
emat
olog
icdi
seas
e11
9.1
1
Y. Beloosesky et al. / Arch. Gerontol. Geriatr. 26 (1998) 227–234232
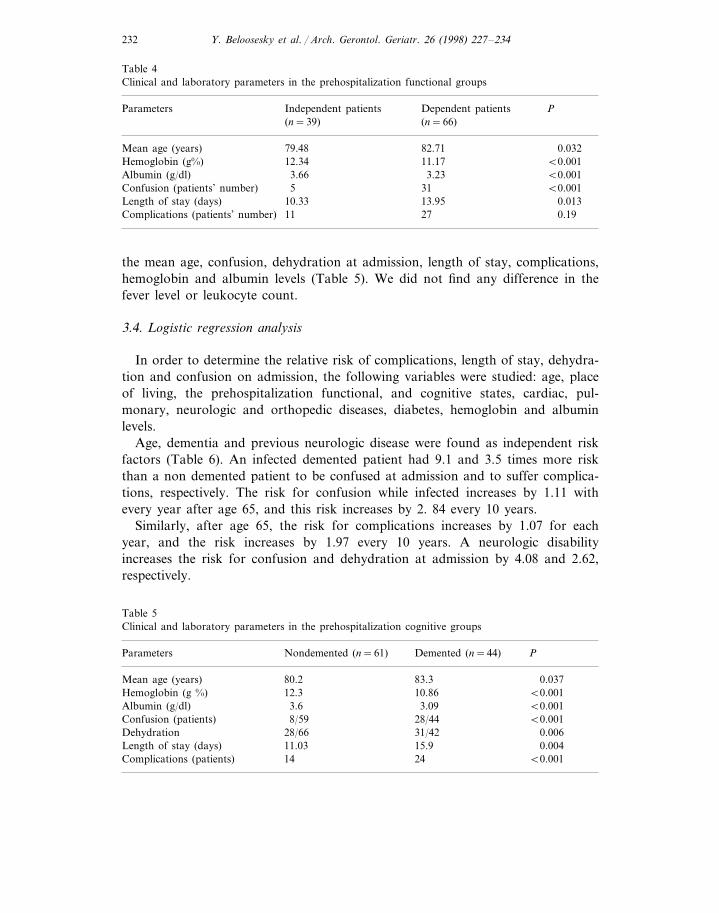
Table 4Clinical and laboratory parameters in the prehospitalization functional groups
Independent patients PParameters Dependent patients(n=39) (n=66)
Mean age (years) 0.03282.7179.4812.34Hemoglobin (g%) B0.00111.17
Albumin (g/dl) 3.66 3.23 B0.001Confusion (patients’ number) 5 31 B0.001Length of stay (days) 10.33 13.95 0.013
11Complications (patients’ number) 27 0.19
the mean age, confusion, dehydration at admission, length of stay, complications,hemoglobin and albumin levels (Table 5). We did not find any difference in thefever level or leukocyte count.
3.4. Logistic regression analysis
In order to determine the relative risk of complications, length of stay, dehydra-tion and confusion on admission, the following variables were studied: age, placeof living, the prehospitalization functional, and cognitive states, cardiac, pul-monary, neurologic and orthopedic diseases, diabetes, hemoglobin and albuminlevels.
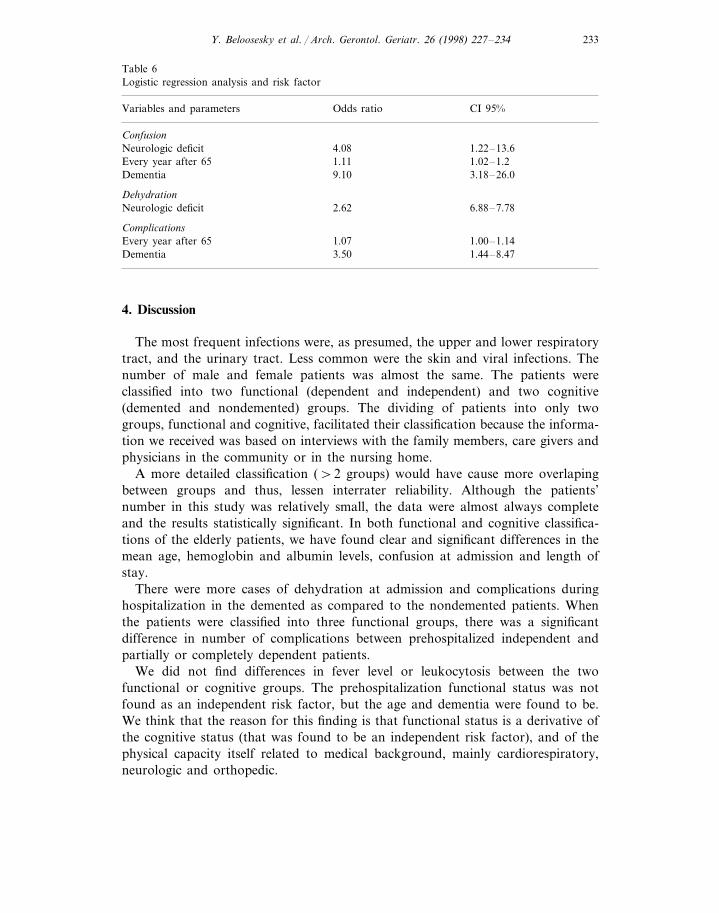
Age, dementia and previous neurologic disease were found as independent riskfactors (Table 6). An infected demented patient had 9.1 and 3.5 times more riskthan a non demented patient to be confused at admission and to suffer complica-tions, respectively. The risk for confusion while infected increases by 1.11 withevery year after age 65, and this risk increases by 2. 84 every 10 years.
Similarly, after age 65, the risk for complications increases by 1.07 for eachyear, and the risk increases by 1.97 every 10 years. A neurologic disabilityincreases the risk for confusion and dehydration at admission by 4.08 and 2.62,respectively.
Table 5Clinical and laboratory parameters in the prehospitalization cognitive groups
Nondemented (n=61) Demented (n=44)Parameters P
80.2 83.3 0.037Mean age (years)12.3Hemoglobin (g %) 10.86 B0.001
3.093.6Albumin (g/dl) B0.001B0.001Confusion (patients) 28/448/59
28/66Dehydration 31/42 0.00611.03 15.9 0.004Length of stay (days)14 24 B0.001Complications (patients)
Y. Beloosesky et al. / Arch. Gerontol. Geriatr. 26 (1998) 227–234 233
Table 6Logistic regression analysis and risk factor
Odds ratio CI 95%Variables and parameters
Confusion1.22–13.64.08Neurologic deficit1.02–1.21.11Every year after 653.18–26.09.10Dementia
Dehydration6.88–7.78Neurologic deficit 2.62
Complications1.00–1.141.07Every year after 651.44–8.473.50Dementia
4. Discussion
The most frequent infections were, as presumed, the upper and lower respiratorytract, and the urinary tract. Less common were the skin and viral infections. Thenumber of male and female patients was almost the same. The patients wereclassified into two functional (dependent and independent) and two cognitive(demented and nondemented) groups. The dividing of patients into only twogroups, functional and cognitive, facilitated their classification because the informa-tion we received was based on interviews with the family members, care givers andphysicians in the community or in the nursing home.
A more detailed classification (\2 groups) would have cause more overlapingbetween groups and thus, lessen interrater reliability. Although the patients’number in this study was relatively small, the data were almost always completeand the results statistically significant. In both functional and cognitive classifica-tions of the elderly patients, we have found clear and significant differences in themean age, hemoglobin and albumin levels, confusion at admission and length ofstay.
There were more cases of dehydration at admission and complications duringhospitalization in the demented as compared to the nondemented patients. Whenthe patients were classified into three functional groups, there was a significantdifference in number of complications between prehospitalized independent andpartially or completely dependent patients.
We did not find differences in fever level or leukocytosis between the twofunctional or cognitive groups. The prehospitalization functional status was notfound as an independent risk factor, but the age and dementia were found to be.We think that the reason for this finding is that functional status is a derivative ofthe cognitive status (that was found to be an independent risk factor), and of thephysical capacity itself related to medical background, mainly cardiorespiratory,neurologic and orthopedic.

Y. Beloosesky et al. / Arch. Gerontol. Geriatr. 26 (1998) 227–234234
Although it is common to think that debilitated patients are more prone todevelop complications and have longer periods of hospitalization, there are onlyfew papers dealing specifically with this issue and compare functional and cognitivegroups. Our findings show that functional and cognitive prehospitalization statusand previous neurologic disease (mainly stroke) may have a stronger predictive andprognostic value than the medical health problems, in acute infectious disease inelderly.
In conclusion, elderly patients hospitalized for acute infection can be classified intwo functional and cognitive groups. The demented and dependent patients have agreater risk for confusion and dehydration at admission and have more complica-tions and longer hospitalization periods.
References
Azoulay, G., Henry, J.F., Fosette, F., Bertaux, P., Acar, J.F., 1977. Les septicemies du sujet age. Nouv.Presse Med. 6, 3079–3081.
Bamford, J.M., Sandercock, P.A., Warlow, C.P., Slattery, J., 1989. Interobserver agreement for theassessment of handicap in stroke patients. Stroke 20, 828.
Clinton, M.J., Clinton, G.M., Irwin, G.A., 1992. The majority of patients with community acquiredpneumonia exceed their diagnosis-related group (DRG), predicted length of stay. Chest 102, 174S.
Darnowski, S.B., Gordon, M., Simor, A.E., 1991. Two years of infection surveillance in a geriatriclongterm care facility. Am. J. Infect. Control 19, 185–190.
Garibaldi, R.A., Brodine, S., Matsumiya, S., 1981. Infections among patients in nursing homes. NewEngl. J. Med. 305, 731–735.
Irvine, P.W., Van Buren, N., Crossley, K., 1984. Causes for hospitalization of nursing home residentsthe role of infection. J. Am. Geriatr. Soc. 32, 103–107.
Jackson, M.M., Fierer, J., 1985. Infections and infection risk in residents of long-term care facilities: Areview of the literature 1970–1984. Am. J. Infect. Control 13, 63–77.
Jones, S.R., 1990. Infections in frail and vulnerable elderly patients. Am. J. Med. 3c, 30–33.Leibovici, L., Pitlik, S.D., Konisberger, H., Drucker, M., 1993. Blood-stress infections in patients older
than eighty years. Age Ageing 22, 431–442.McCue, J.D., 1987. Gram-negative bacillary bacteraemia in the elderly: Incidence, ecology, etiology, and
mortality. J. Am. Geriatr. Soc. 35 (7), 213–218.Michel, J.P., Lesourd, E., Conne, P., Richard, D., Rapin, C.H., 1991. Prevalence of infections and their
risk factors in geriatric institutions: A one-day multicentre survey. Bull. Who 69, 35–41.Myhre, E.B., 1983. Hospital treatment of infectious diseases. Analysis of patients treated in an infection
disease clinic in a Swedish teaching hospital. Scand. J. Infect. Dis. 15, 215–220.Nicolle, L.E., McIntyre, M., Zacharias, H., MacDonell, J.A., 1984. Twelve-month surveillance of
infections in institutionalized elderly men. J. Am. Geriatr. Soc. 32, 513–519.Price, L.E., Sarubbi, F.A. Jr., Rutala, W.A., 1985. Infection control program in twelve North Carolina
extended care facilities. Infect. Control 6, 437–441.Scheckler, W.E., Peterson, P.J., 1986. Infections and infection control among residents of eight rural
Wisconsin nursing homes. Arch. Intern. Med. 146, 1981–1984.Setia, U., Serventi, I., Lorenz, P., 1985. Nosocomial infections among patients in a long-term care
facility: Spectrum, prevalence, and risk factors. Am. J. Infect. Control 13, 57–62.Watanakunahorn, C., Greifenstein, A., Strih, K., Blend, D., Cucino, A., Ognibene, A.J., 1993.
Pneumococcal bacteremia in three community teaching hospitals from 1980 to 1989. Chest 103,1152–1156.
Whitelaw, D.A., Rayner, B.L., Willcox, P.A., 1992. Community-acquired bacteremia in the elderly: Aprospective study of 121 cases. J. Am. Geriatr. Soc. 40, 996–1000..
Recommended

















