Francisco J Hernandez-Ilizaliturri MD Professor of Medicine
Chief Lymphoma and Myeloma Section Associate Professor of Immunology
Departments of Medicine and Immunology Roswell Park Cancer Institute
The evolution of monoclonal antibodies in cancer medicine

Schulz, H et al. Blood 106; 2005:351a
Does combined rituximab/chemotherapy improve overall survival in the treatment of patients with indolent
Lymphoma?

Number of therapeutic mAbs entering clinical study per year (1980−2004)
Holliger P. et al. Nature Biotechnology 2005; 23:1073 - 1078
There are currently >22 mAbs approved by the FDA
By 2008 engineered mAbs are predicted to be account for more than 30% of the revenues in the biotechnology market
César Milst Georges Köhler and Niels Jerne
Monoclonal antibodies: the story of a discovery that revolutionized science and medicine
Nobel Prize in Physiology or Medicine 1984.

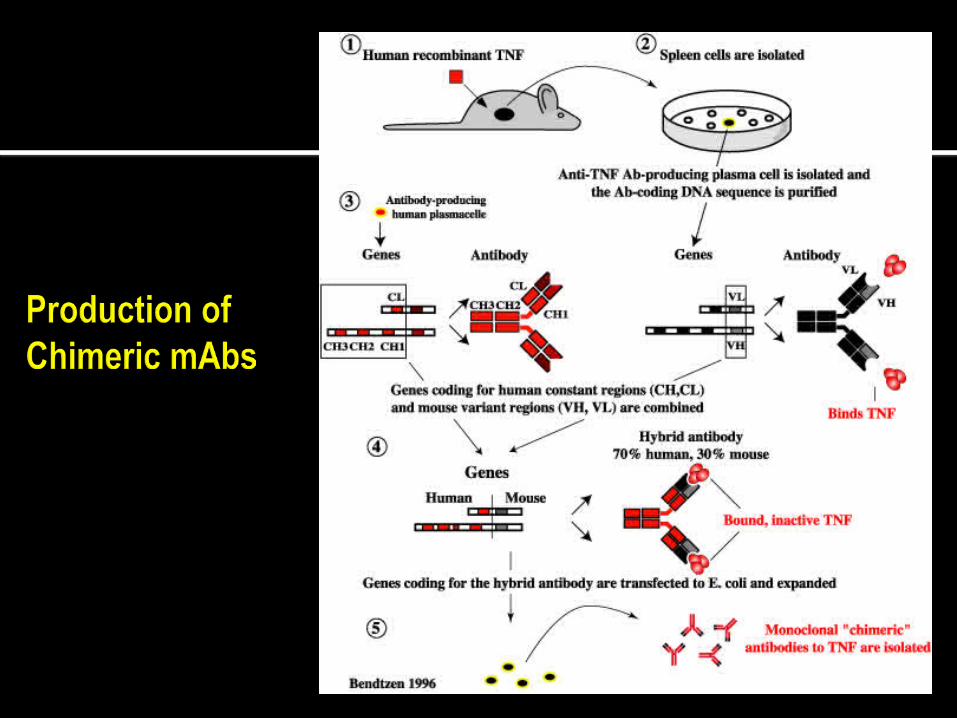
A schematic representation of
hydridoma technology Spleen cells from an immunized mice are fused, using polyethylene glycol, with myeloma cells that were rendered drug sensitive by a mutation in a growth essential gene hypoxanthine-guanine-phosphoribosyl transferase (HGPRT).
The cell mixture is then cultured in a medium containing the selective drug. As immune cells, although not sensitive to HGPRT, survive for only about one week in culture and the myeloma cells are drug sensitive they will all die within a week or so.
The only cells that can survive are those hybrid myeloma cells that obtained a normal HGPRT gene from the immune cells. These hybridomas can grow continuously in vitro and some secrete antibody.
By using appropriate screening technology, clones of cells that secrete antibody of interest can be identified and expanded in vitro or in vivo to obtain large quantities of monoclonal antibody that can subsequently be purified to homogeneity. Köhler G and Milst C. Nature 1975; 256: 495–497.

Lonberg N. Nature Biothecnology 2005; 23: 1117.
The Evolution of mAbs in Clinical Medicine

Therapeutic antibody technologies
Carter P. Nature Cancer Reviews 2001; 1: 118
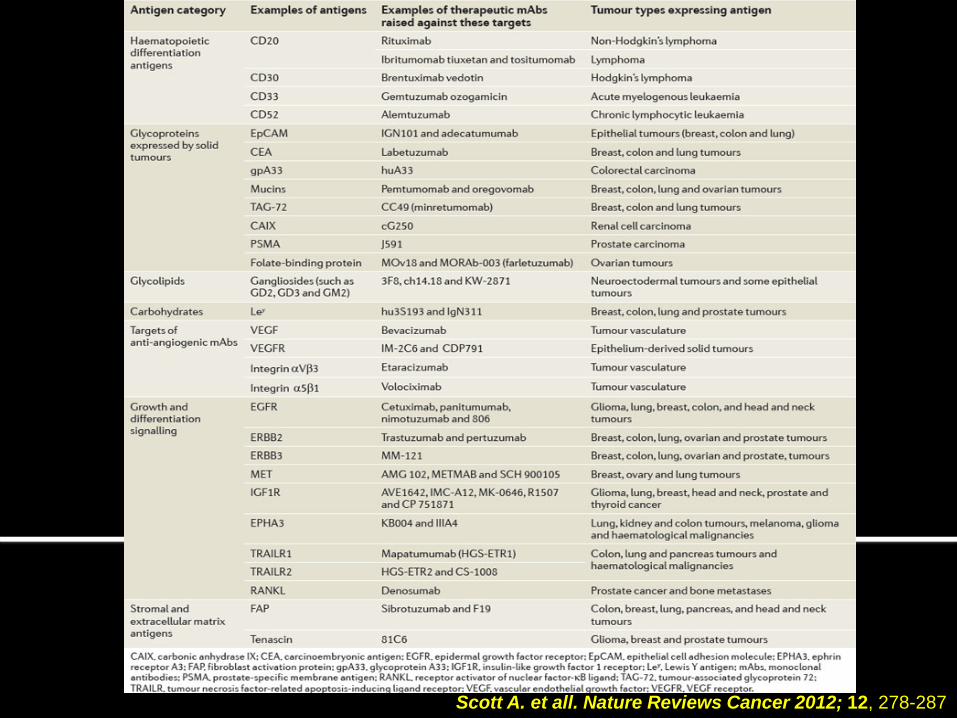
Scott A. et all. Nature Reviews Cancer 2012; 12, 278-287

Antigen (target) expression variable
Most involved in B-cell growth, differentiation, proliferation, and activation
Many are targets for treatment of B-cell cancers
B-Cell
CD19
CD20
CD21
CD22
CD23
CD38
B-cell receptor (BCR)
CD40
CD52
CD46, CD55, CD59
CD74
CD80
Marker

Expressed: Exclusively on B-cells
Stable on B-cell surface, allowing sustained MAb binding
Function not well understood but believed to contribute to B-cell growth, proliferation, differentiation, and activation
B-Cell
CD20

Small Loop
Large Loop
2 extracellular loops to which monoclonal antibodies may bind1,2
MAb binding sites are near cell membrane, facilitating recruitment of cytotoxic effectors, both cells and proteins, to the B-cell surface1,2
B-Cell Membrane
1Cragg MS, et al. Curr Dir Autoimmun. 2005;8:140-174. 2Glennie MJ, et al. Mol Immunol. 2007;44(16):3823-3837.

Pre-B Early B Mature B Plasmacytoid B
±CD5
CD19
CD20
CD22
CD52
Plasma Intermediate B
? ? ?
Stem cell
Burkitt’s, FL, DLCL, HCL
ALL CLL, PLL
WM MM
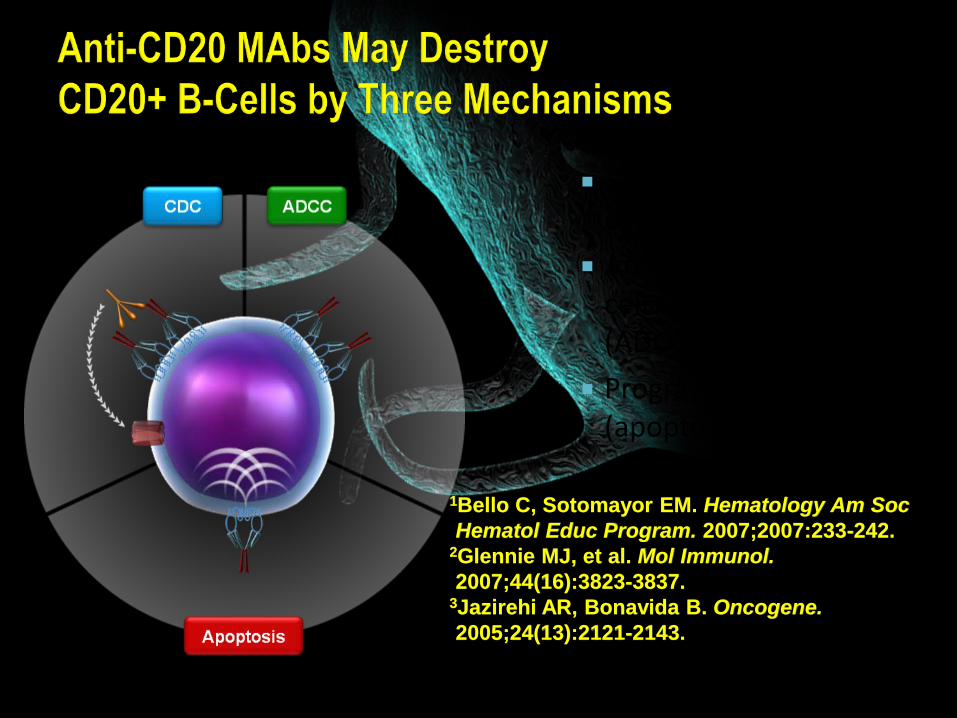
Complement-dependent cytotoxicity (CDC)1-3
Antibody-dependent cellular cytotoxicity (ADCC)1-3
Programmed cell death (apoptosis)1-3
1Bello C, Sotomayor EM. Hematology Am Soc Hematol Educ Program. 2007;2007:233-242.
2Glennie MJ, et al. Mol Immunol. 2007;44(16):3823-3837.
3Jazirehi AR, Bonavida B. Oncogene. 2005;24(13):2121-2143.
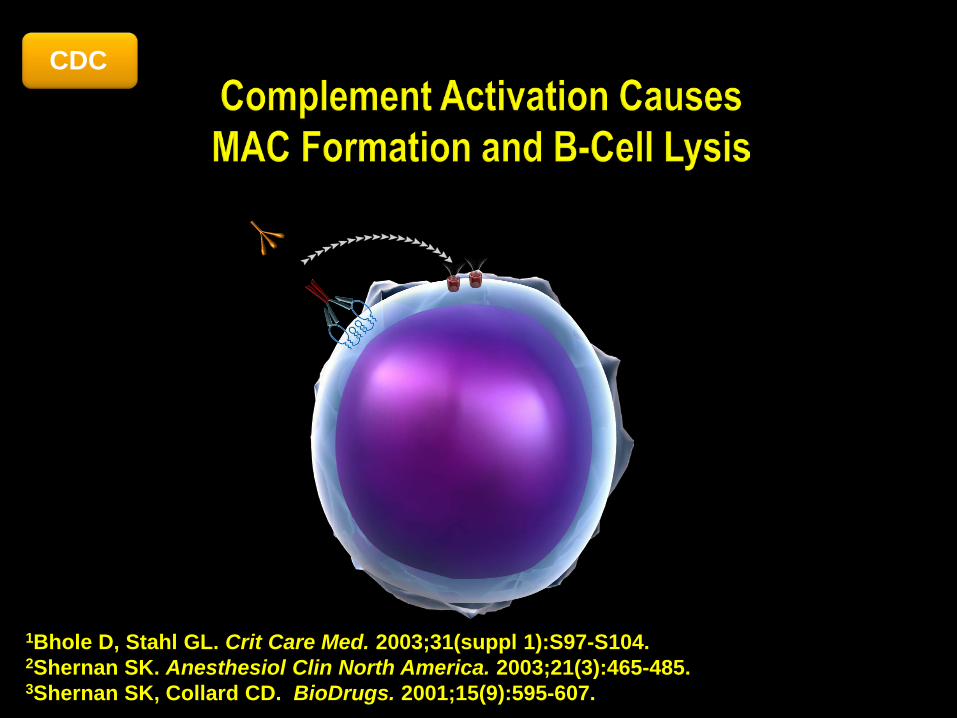
CDC
1Bhole D, Stahl GL. Crit Care Med. 2003;31(suppl 1):S97-S104. 2Shernan SK. Anesthesiol Clin North America. 2003;21(3):465-485. 3Shernan SK, Collard CD. BioDrugs. 2001;15(9):595-607.
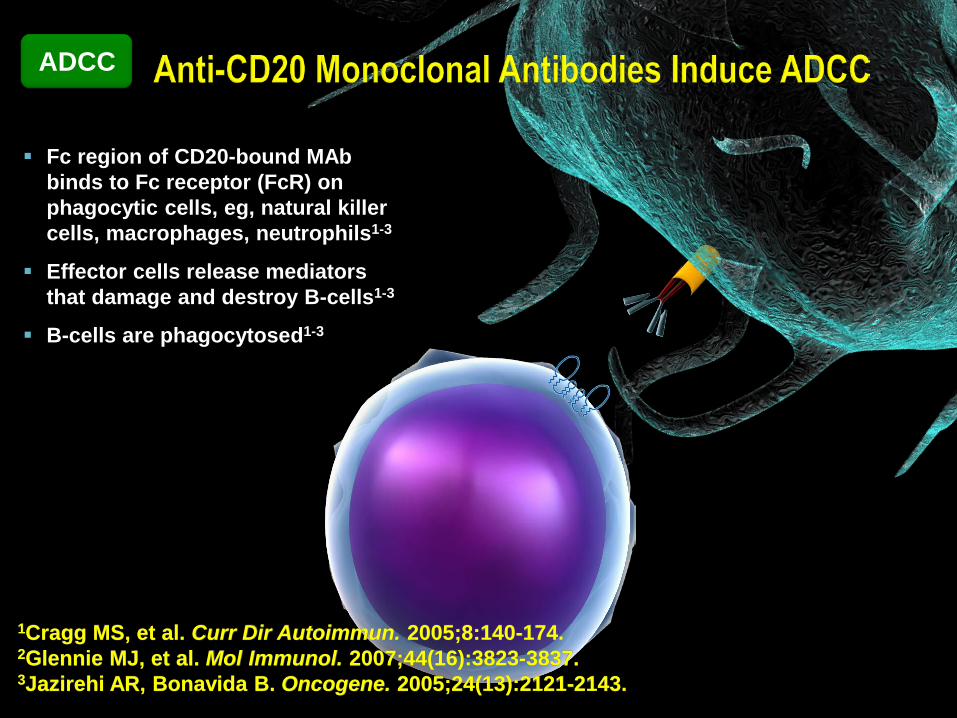
ADCC
Fc region of CD20-bound MAb binds to Fc receptor (FcR) on phagocytic cells, eg, natural killer cells, macrophages, neutrophils1-3
Effector cells release mediators that damage and destroy B-cells1-3
B-cells are phagocytosed1-3
1Cragg MS, et al. Curr Dir Autoimmun. 2005;8:140-174. 2Glennie MJ, et al. Mol Immunol. 2007;44(16):3823-3837. 3Jazirehi AR, Bonavida B. Oncogene. 2005;24(13):2121-2143.
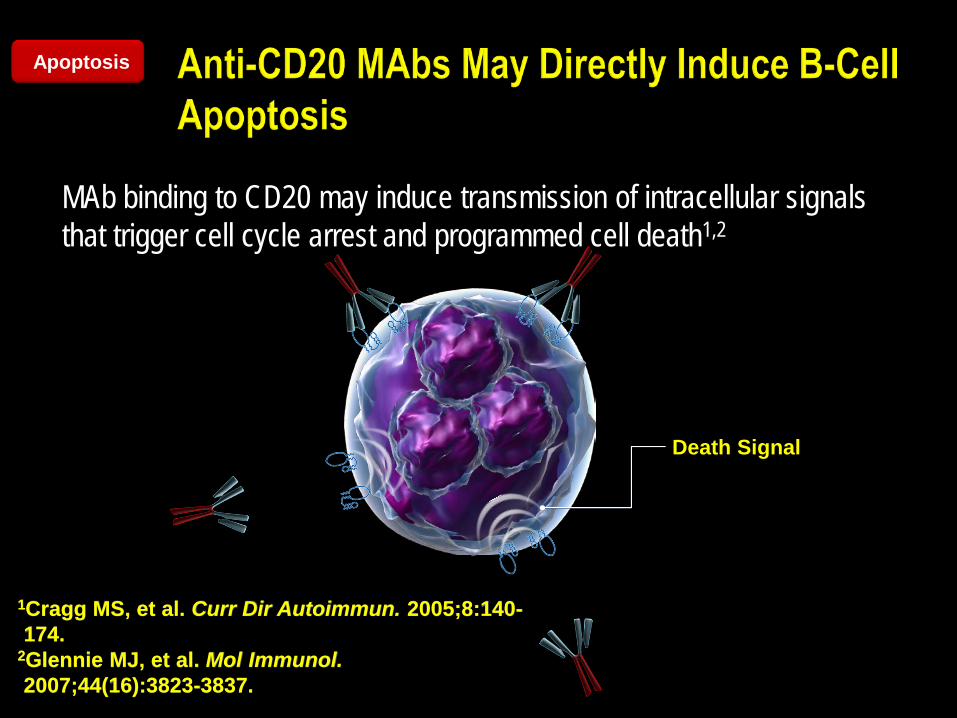
MAb binding to CD20 may induce transmission of intracellular signals that trigger cell cycle arrest and programmed cell death1,2
Death Signal
Apoptosis
1Cragg MS, et al. Curr Dir Autoimmun. 2005;8:140-174.
2Glennie MJ, et al. Mol Immunol. 2007;44(16):3823-3837.
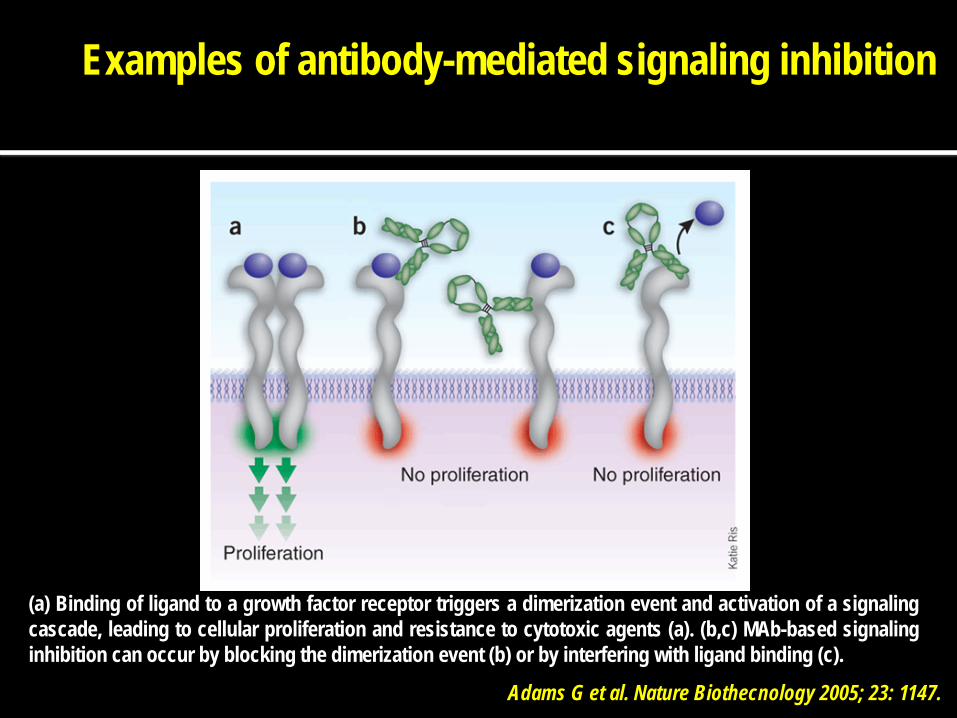
(a) Binding of ligand to a growth factor receptor triggers a dimerization event and activation of a signaling cascade, leading to cellular proliferation and resistance to cytotoxic agents (a). (b,c) MAb-based signaling inhibition can occur by blocking the dimerization event (b) or by interfering with ligand binding (c).
Examples of antibody-mediated signaling inhibition
Adams G et al. Nature Biothecnology 2005; 23: 1147.

A prerequisite first step for CDC is recruitment of the complement component C1q by IgG bound to the tumour cell surface. Tumour-cell-bound C1q can bind to complement receptors, such as C1qR, CR1 (CD35) and CR3 (CD11b/CD18), on effector cells, such as neutrophils, macrophages and natural killer cells.
Human antibodies, particularly IgG1 and IgG3, can potentially direct the killing of tumour cells by ADCC or CDC
ADCC is triggered by an interaction between the Fc region of an antibody that has bound, through its antigen-binding region, to a tumour cell and the Fc receptors (Fc Rs), particularly Fc RI and Fc RIII, on immune effector cells such as neutrophils, macrophages and natural killer cells.
Carter P. Nature Cancer Reviews 2001; 1: 118
Clynes et al. Nat Med 2000; 6:443-6
Hernandez-Ilizaliturri et al Clin Can Res 2003; 9:5866-73
Hernandez-Ilizaliturri et al. Leu & Lymphoma, 2006;

Clynes et al. Nat Med 2000; 6:443-6
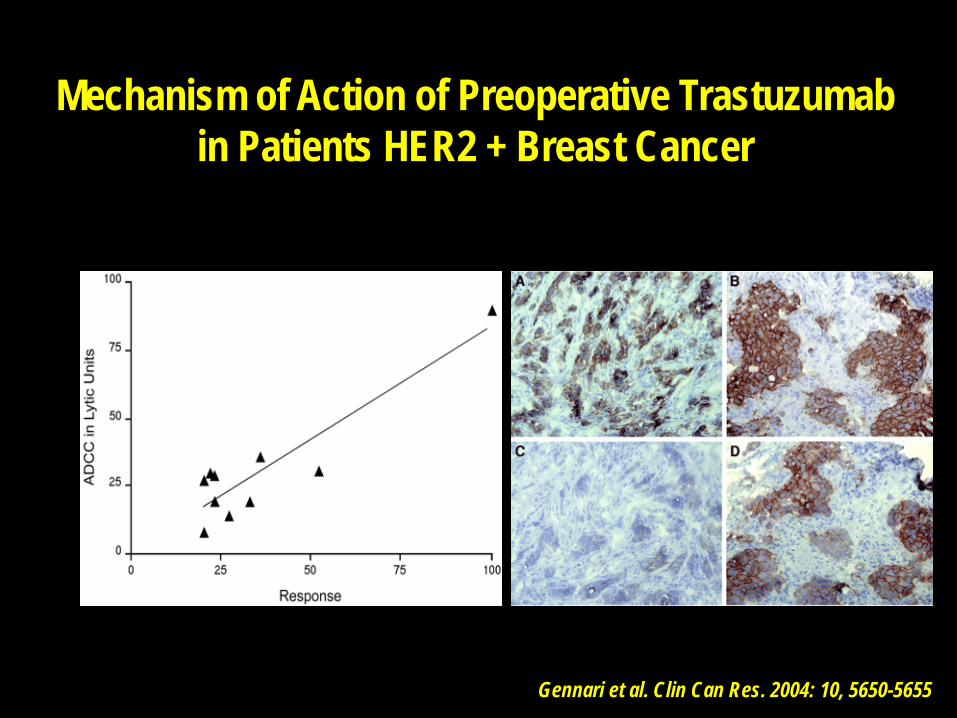
Rituximab and Trastuzumab activity is mediated by ADCC
Recruitment of natural killer (NK) cells,macrophages/monocytes, and PMNs by rituximab is via binding to their Fcγ receptors By increasing the number and/or activation state of effector cells,mAb-associated cytotoxicity may be increased
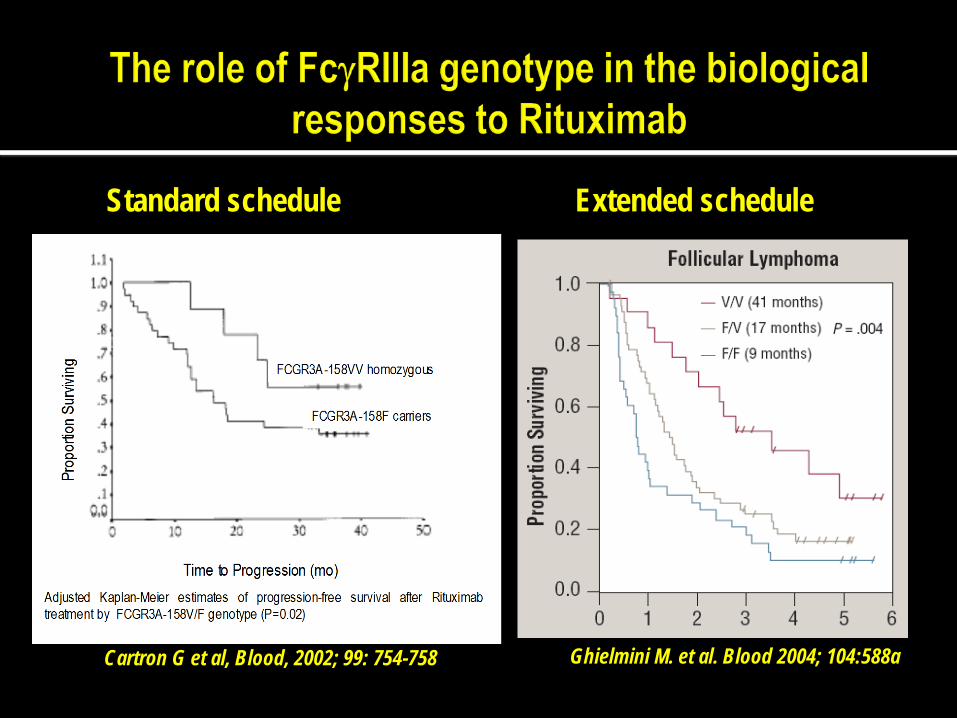
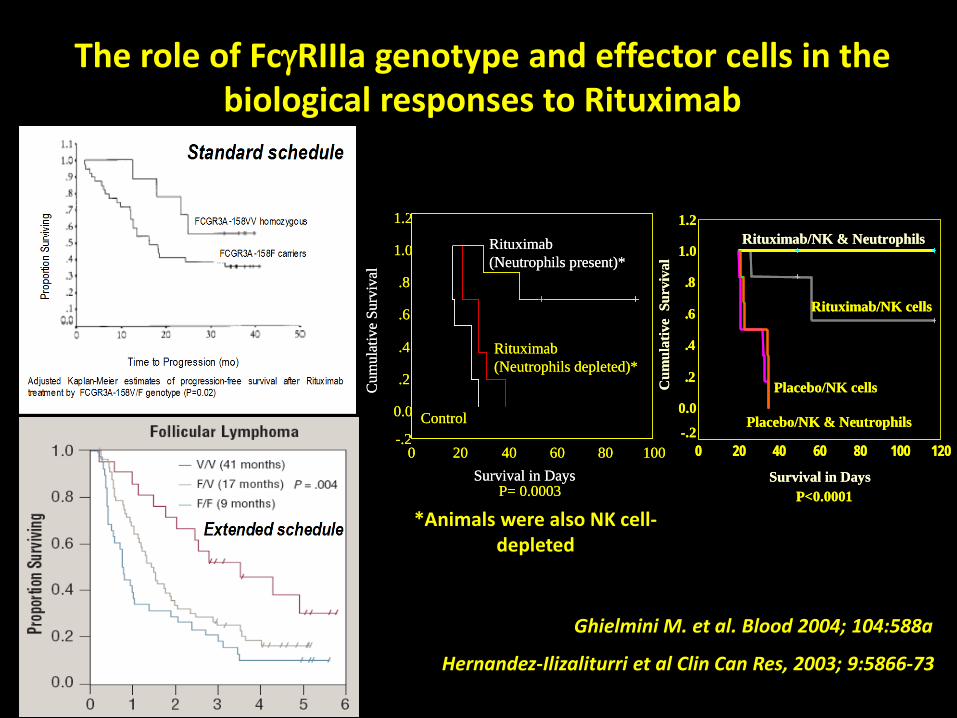
Cartron G et al, Blood, 2002; 99: 754-758 Ghielmini M. et al. Blood 2004; 104:588a
Standard schedule Extended schedule
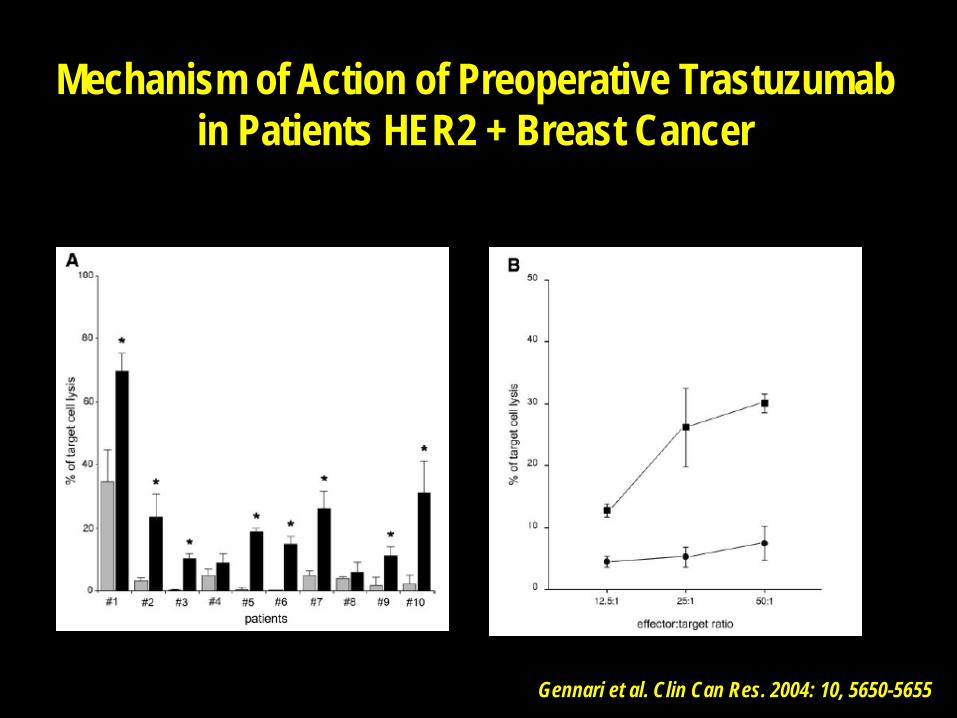
Mechanism of Action of Preoperative Trastuzumab in Patients HER2 + Breast Cancer
Gennari et al. Clin Can Res. 2004: 10, 5650-5655
Gennari et al. Clin Can Res. 2004: 10, 5650-5655
Mechanism of Action of Preoperative Trastuzumab in Patients HER2 + Breast Cancer
Novel strategies to improve the anti-tumor activity of Monoclonal antibodies

Transgenic mice producing human mAbs
Weiner L. J Immunother 2006; 29:1-9
Sehn L. al. ASH 2011: 269
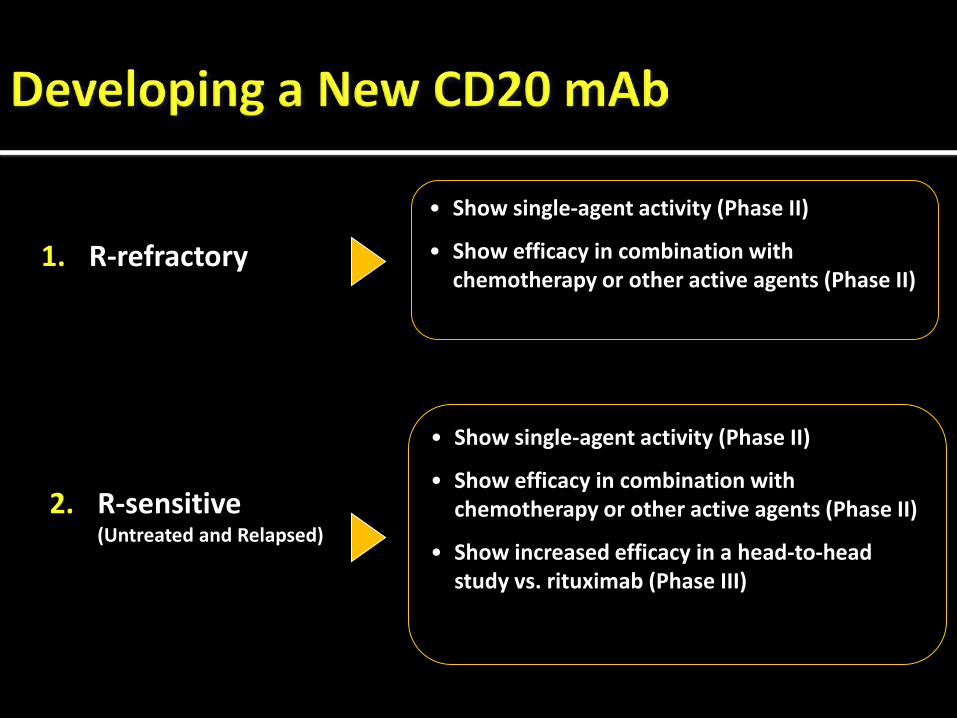
• Show single-agent activity (Phase II)
• Show efficacy in combination with chemotherapy or other active agents (Phase II)
• Show single-agent activity (Phase II)
• Show efficacy in combination with chemotherapy or other active agents (Phase II)
• Show increased efficacy in a head-to-head study vs. rituximab (Phase III)
1. R-refractory
2. R-sensitive (Untreated and Relapsed)
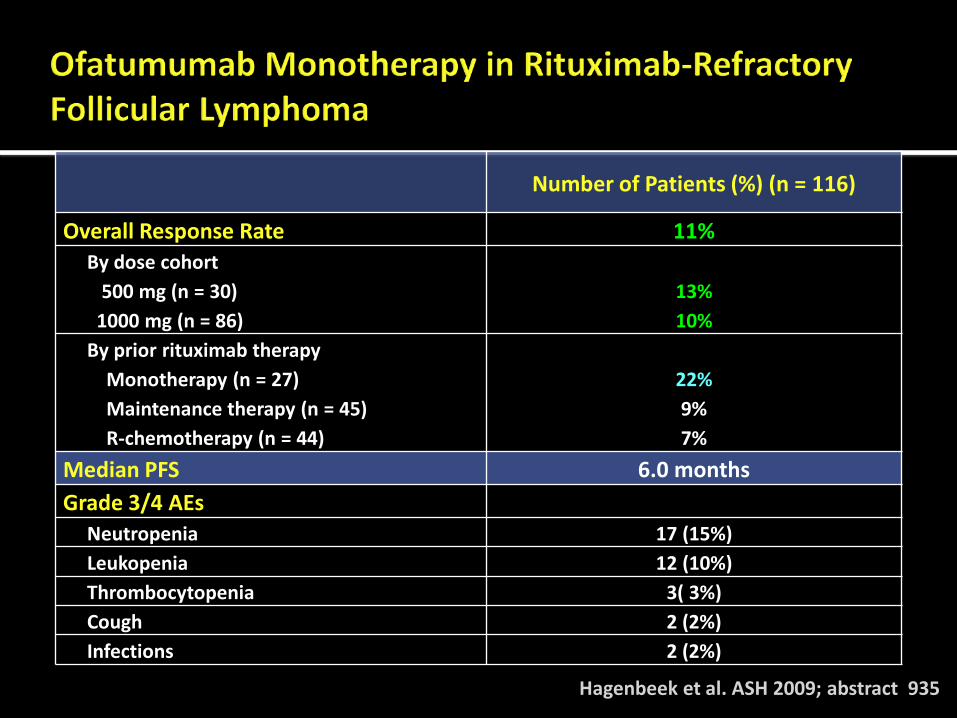
Hagenbeek et al. ASH 2009; abstract 935
Number of Patients (%) (n = 116)
Overall Response Rate 11% By dose cohort 500 mg (n = 30) 1000 mg (n = 86)
13% 10%
By prior rituximab therapy Monotherapy (n = 27) Maintenance therapy (n = 45) R-chemotherapy (n = 44)
22% 9% 7%
Median PFS 6.0 months Grade 3/4 AEs
Neutropenia 17 (15%) Leukopenia 12 (10%) Thrombocytopenia 3( 3%) Cough 2 (2%) Infections 2 (2%)
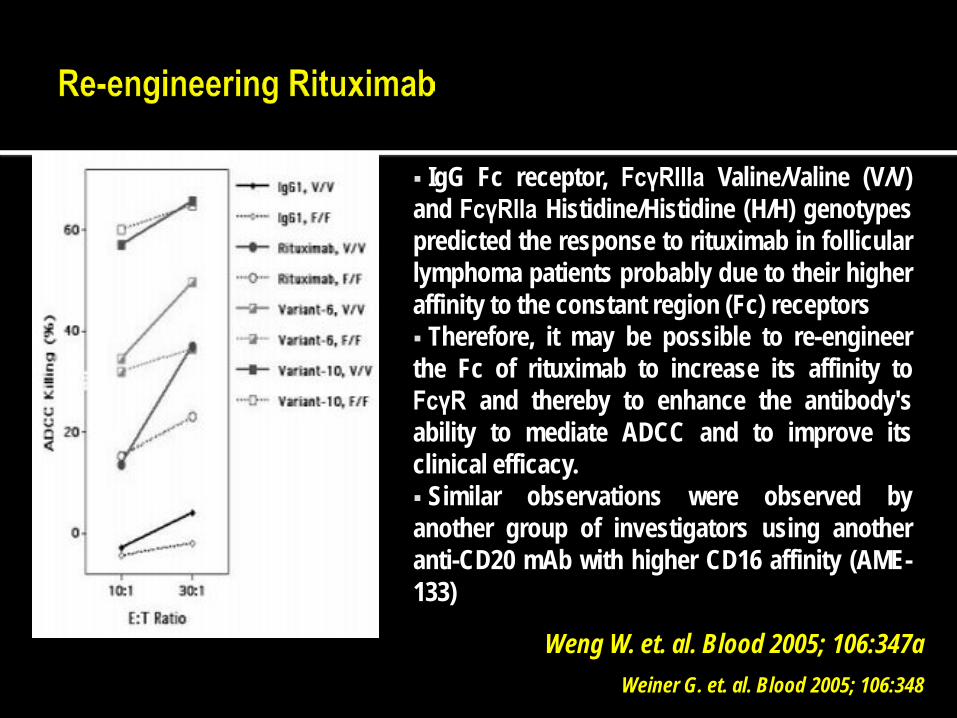
Weng W. et. al. Blood 2005; 106:347a Weiner G. et. al. Blood 2005; 106:348
IgG Fc receptor, FcγRIIIa Valine/Valine (V/V) and FcγRIIa Histidine/Histidine (H/H) genotypes predicted the response to rituximab in follicular lymphoma patients probably due to their higher affinity to the constant region (Fc) receptors Therefore, it may be possible to re-engineer the Fc of rituximab to increase its affinity to FcγR and thereby to enhance the antibody's ability to mediate ADCC and to improve its clinical efficacy. Similar observations were observed by another group of investigators using another anti-CD20 mAb with higher CD16 affinity (AME-133)
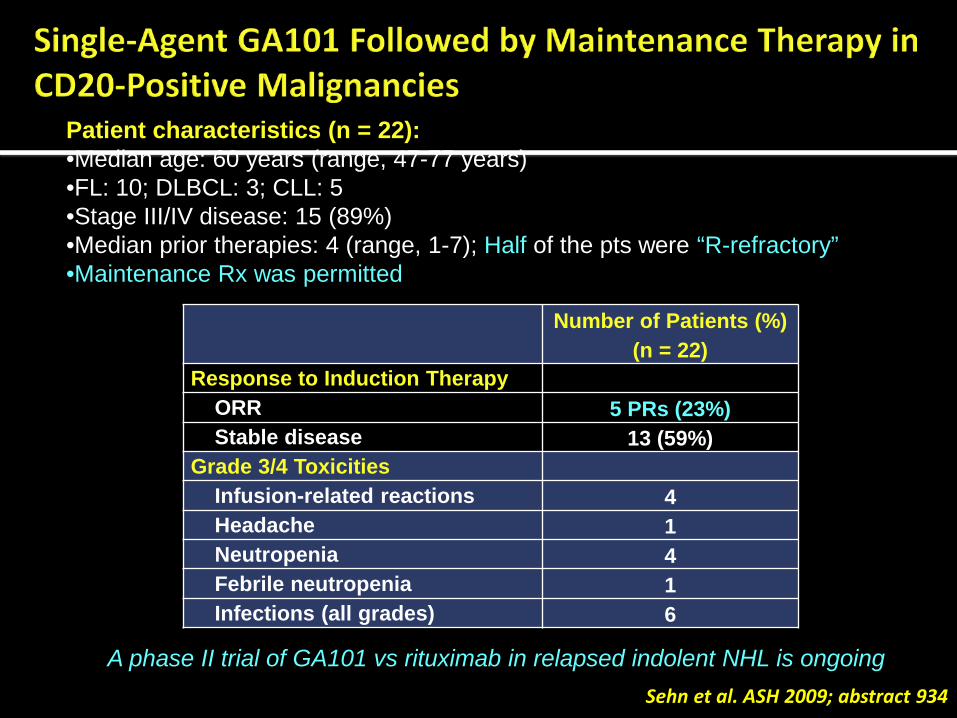
Sehn et al. ASH 2009; abstract 934
Number of Patients (%) (n = 22)
Response to Induction Therapy ORR 5 PRs (23%) Stable disease 13 (59%)
Grade 3/4 Toxicities Infusion-related reactions 4 Headache 1 Neutropenia 4 Febrile neutropenia 1 Infections (all grades) 6
Patient characteristics (n = 22): •Median age: 60 years (range, 47-77 years) •FL: 10; DLBCL: 3; CLL: 5 •Stage III/IV disease: 15 (89%) •Median prior therapies: 4 (range, 1-7); Half of the pts were “R-refractory” •Maintenance Rx was permitted
A phase II trial of GA101 vs rituximab in relapsed indolent NHL is ongoing
Cartron G et al, Blood, 2002; 99: 754-758 Ghielmini M. et al. Blood 2004; 104:588a
The role of FcγRIIIa genotype and effector cells in the biological responses to Rituximab
Survival in Days100806040200
Cum
ulat
ive
Surv
ival
1.2
1.0
.8
.6
.4
.2
0.0
-.2
Rituximab (Neutrophils present)*
Control
P= 0.0003
Rituximab (Neutrophils depleted)*
Survival in Days100806040200
Cum
ulat
ive
Surv
ival
1.2
1.0
.8
.6
.4
.2
0.0
-.2
Rituximab (Neutrophils present)*
Control
P= 0.0003
Rituximab (Neutrophils depleted)*
Survival in Days
120100806040200
Cum
ulat
ive
Sur
viva
l
1.2
1.0
.8
.6
.4
.2
0.0
-.2Placebo/NK & Neutrophils
Placebo/NK cells
Rituximab/NK & Neutrophils
Rituximab/NK cells
P<0.0001Survival in Days
120100806040200
Cum
ulat
ive
Sur
viva
l
1.2
1.0
.8
.6
.4
.2
0.0
-.2Placebo/NK & Neutrophils
Placebo/NK cells
Rituximab/NK & Neutrophils
Rituximab/NK cells
P<0.0001
*Animals were also NK cell-depleted
Hernandez-Ilizaliturri et al Clin Can Res, 2003; 9:5866-73

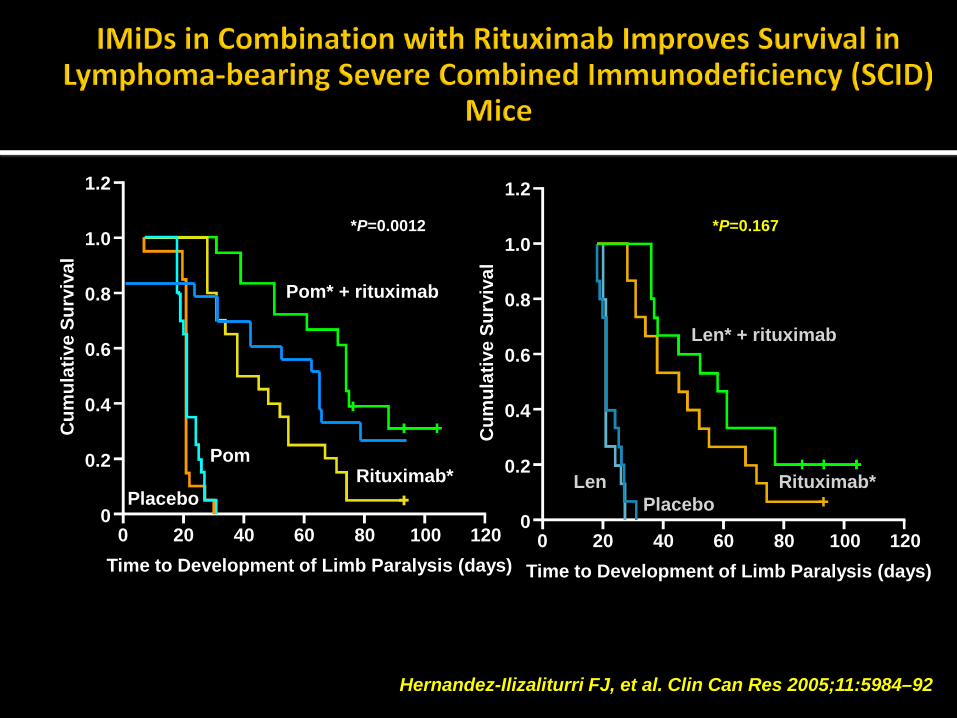
Hernandez-Ilizaliturri FJ, et al. Clin Can Res 2005;11:5984–92
Time to Development of Limb Paralysis (days) 0 20 40 60 80 100 120
Cum
ulat
ive
Surv
ival
1.2
1.0
0.8
0.6
0.4
0.2
0
Pom* + rituximab
Placebo
Pom
*P=0.0012
Rituximab*
Time to Development of Limb Paralysis (days) 0 20 40 60 80 100 120
Cum
ulat
ive
Surv
ival
1.2
1.0
0.8
0.6
0.4
0.2
0
Len* + rituximab
Placebo Len Rituximab*
*P=0.167
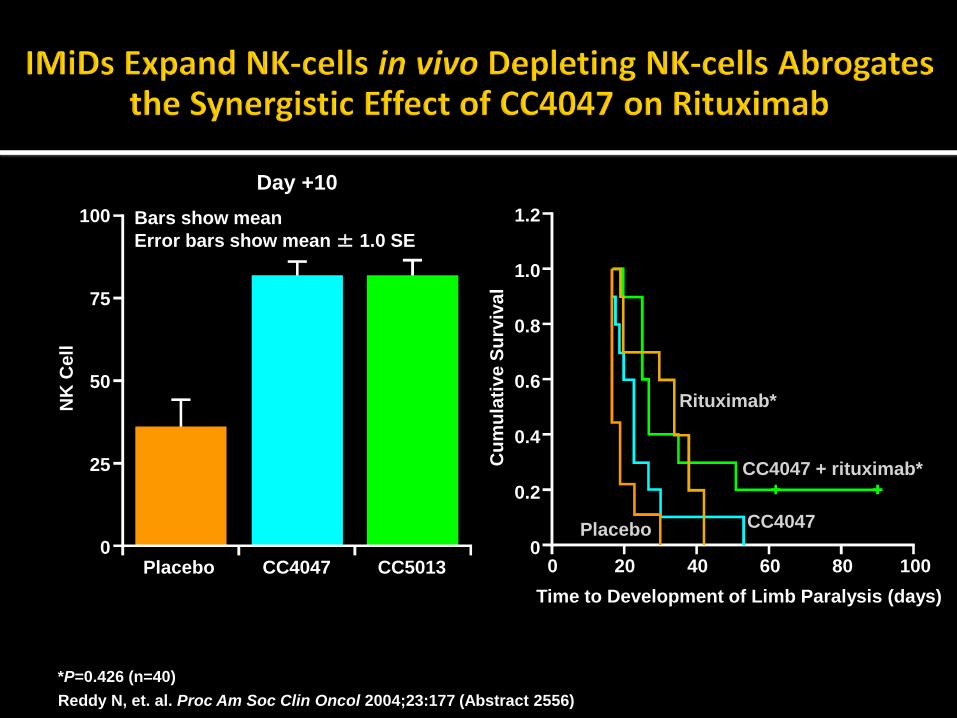
Reddy N, et. al. Proc Am Soc Clin Oncol 2004;23:177 (Abstract 2556)
Time to Development of Limb Paralysis (days) 0 20 40 60 80 100
Cum
ulat
ive
Surv
ival
1.2
1.0
0.8
0.6
0.4
0.2
0
*P=0.426 (n=40)
CC4047 + rituximab*
Placebo CC4047
Rituximab* NK
Cel
l
100
75
50
25
0
Day +10
Placebo CC4047 CC5013
Bars show mean Error bars show mean ± 1.0 SE

Dutia et al. ASH 2009; abstract 1679 Fowler et al. ASCO 2010; abstract 8036
Dutia et al n = 16
Fowler et al. n = 48/ 30FL
Patient Population Relapsed/Refractory
Previously untreated (FLIPI Intermediate 60%/High 27%)
Treatment Lenalidomide Rituximab TLS prophylaxis
25 mg/day, d1-21, q 28d
375 mg/m2/week, beg. d15 X 4 Allopurinol
20 mg/day (10mg/d for SLL) , d1-21, q 28d
375 mg/m2, beg. day 1 X 6 None
Response ORR CR/CRu
12 (75%) 5 (31%)
89% (93% for FL) 73% (86% fir FL)
Safety Rash Lymphopenia Neutropenia Myalgia Hyponatremia Fatigue
NR
4 (25%) 3 (18%)
NR 3 (18%) 2 (12%)
6
NR 7 4
NR 1
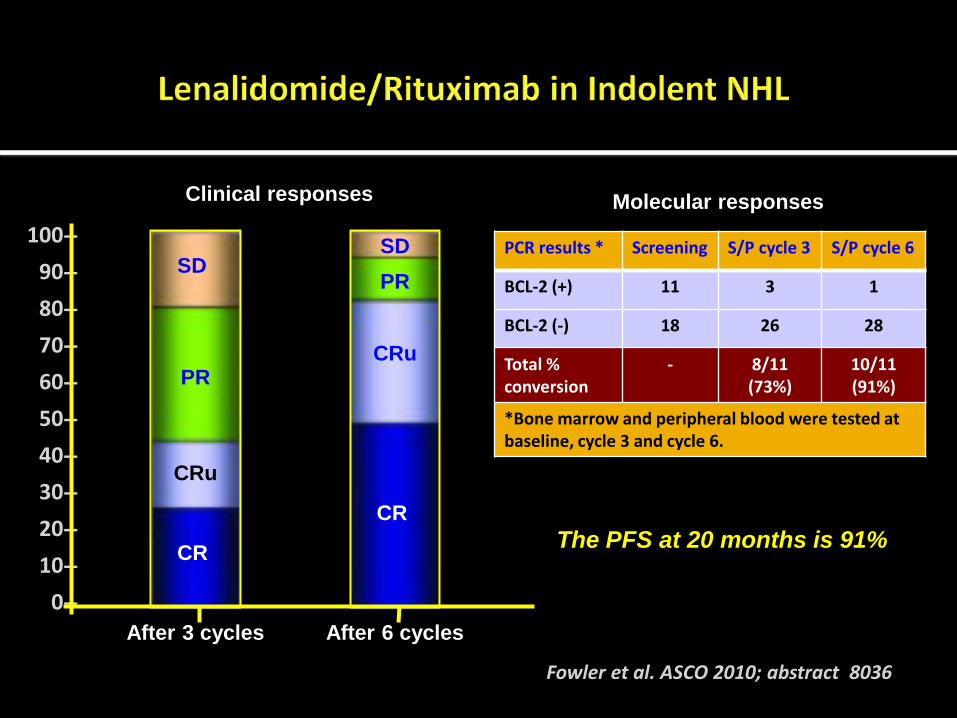
Fowler et al. ASCO 2010; abstract 8036
100-- 90-- 80-- 70-- 60-- 50-- 40-- 30-- 20-- 10--
0--
CR
CRu PR
SD
CR
CRu
PR SD
After 3 cycles After 6 cycles
The PFS at 20 months is 91%
PCR results * Screening S/P cycle 3 S/P cycle 6
BCL-2 (+) 11 3 1
BCL-2 (-) 18 26 28
Total % conversion
- 8/11 (73%)
10/11 (91%)
*Bone marrow and peripheral blood were tested at baseline, cycle 3 and cycle 6.
Molecular responses Clinical responses

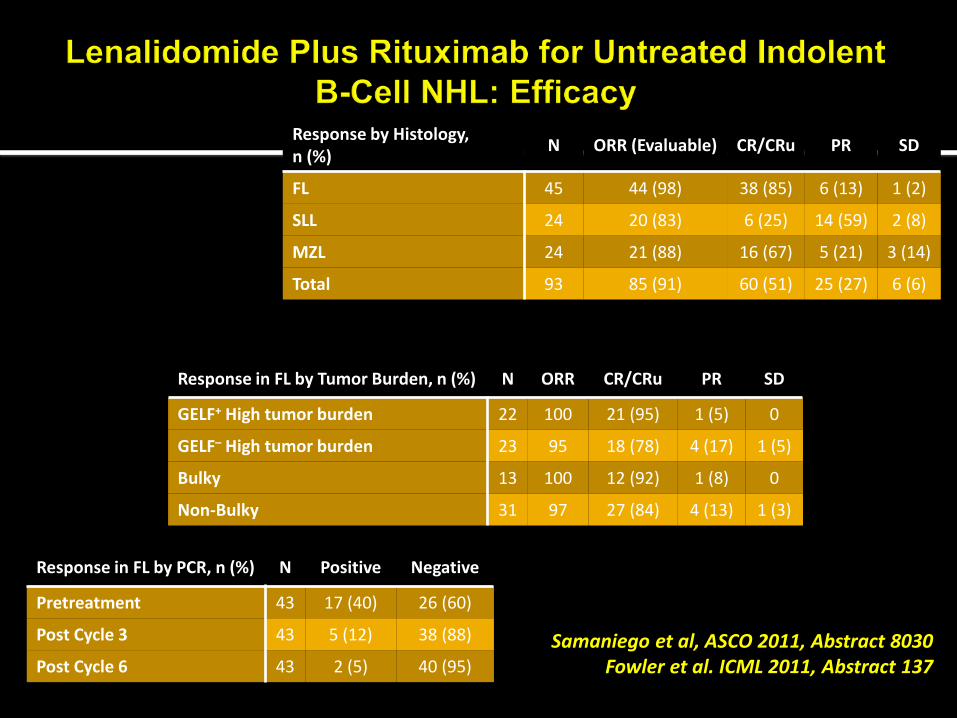
• Phase II, open label, single arm, single institution study • Primary endpoint: ORR; Secondary: PFS, OS, Safety • Designed to enroll 110 patients in 3 cohorts:
• 50 FL (grade I/II), 30 MZL, 30 SLL/CLL • Restaging was performed after cycles 3 and 6 • Lenalidomide increased to 25 mg/day after 3 cycles if SD
Samaniego et al, ASCO 2011, Abstract 8030 Fowler et al. ICML 2011, Abstract 137
Cheson et al. J Clin Oncol. 1999;17:1244-1253
Drug Dose Administration
Rituximab 375 mg/m2 IV Day 1/28 x6 cycles; if clinical benefit, can give 12 cycles
Lenalidomide 20 mg/day* PO Days 1-21/28 x6 cycles; if clinical benefit, can give 12 cycles
*SLL patients received 10 mg/day cycle 1, 15 mg/day cycle 2, 20 mg/day on cycle 3.

*GELF Criteria: • 3 nodes > 3 cm or 1
greater than 7cm • Systemic/local
symptoms from disease • Compression/risk of
compression of vital organ
• Cytopenia due to marrow infiltration
• Splenomegaly > 16cm
Patient Characteristics, n (%) (N = 100)
Median Age (range) 58 years (34 – 84 years)
Histology
Marginal Zone 27 (27)
SLL 24 (24)
Follicular 49 (49)
FLIPI Score (N = 49)
Low 10 (20)
Intermediate 25 (51)
High 14 (29)
GELF Criteria for High Tumor Burden* 50 (50)
Bulky Disease (mass > 7 cm, or 3 nodes > 3 cm) 22 (22)
Stage III/IV 100 (100)
LDH ≥ 500 31 (31)
Samaniego et al, ASCO 2011, Abstract 8030 Fowler et al. ICML 2011, Abstract 137
Samaniego et al, ASCO 2011, Abstract 8030 Fowler et al. ICML 2011, Abstract 137
Response by Histology, n (%) N ORR (Evaluable) CR/CRu PR SD
FL 45 44 (98) 38 (85) 6 (13) 1 (2)
SLL 24 20 (83) 6 (25) 14 (59) 2 (8)
MZL 24 21 (88) 16 (67) 5 (21) 3 (14)
Total 93 85 (91) 60 (51) 25 (27) 6 (6)
Response in FL by Tumor Burden, n (%) N ORR CR/CRu PR SD
GELF+ High tumor burden 22 100 21 (95) 1 (5) 0
GELF– High tumor burden 23 95 18 (78) 4 (17) 1 (5)
Bulky 13 100 12 (92) 1 (8) 0
Non-Bulky 31 97 27 (84) 4 (13) 1 (3)
Response in FL by PCR, n (%) N Positive Negative
Pretreatment 43 17 (40) 26 (60)
Post Cycle 3 43 5 (12) 38 (88)
Post Cycle 6 43 2 (5) 40 (95)

Samaniego et al, ASCO 2011, Abstract 8030 Fowler et al. ICML 2011, Abstract 137
Follicular Lymphoma All Evaluable Patients
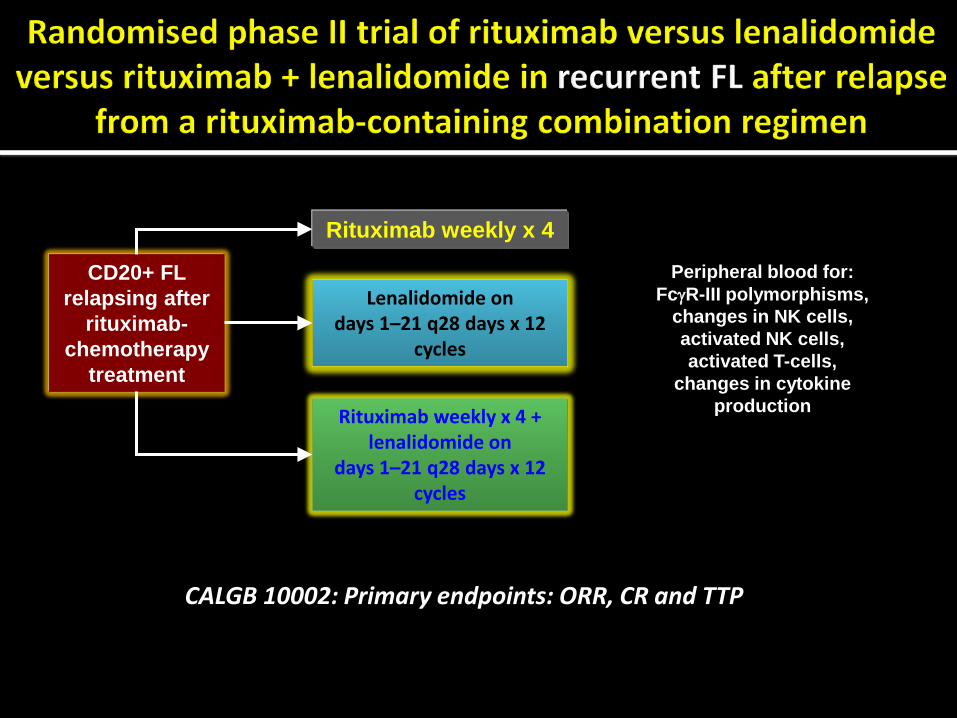
CD20+ FL relapsing after
rituximab-chemotherapy
treatment
Peripheral blood for: FcγR-III polymorphisms,
changes in NK cells, activated NK cells, activated T-cells,
changes in cytokine production
Rituximab weekly x 4
Lenalidomide on days 1–21 q28 days x 12
cycles
Rituximab weekly x 4 + lenalidomide on
days 1–21 q28 days x 12 cycles
CALGB 10002: Primary endpoints: ORR, CR and TTP
GELA FL-001*
Phase III randomized study of lenalidomide vs R-Chemo in 1st-line FL patients
On-Going lenalidomide Lymphoma Registration Study In FL
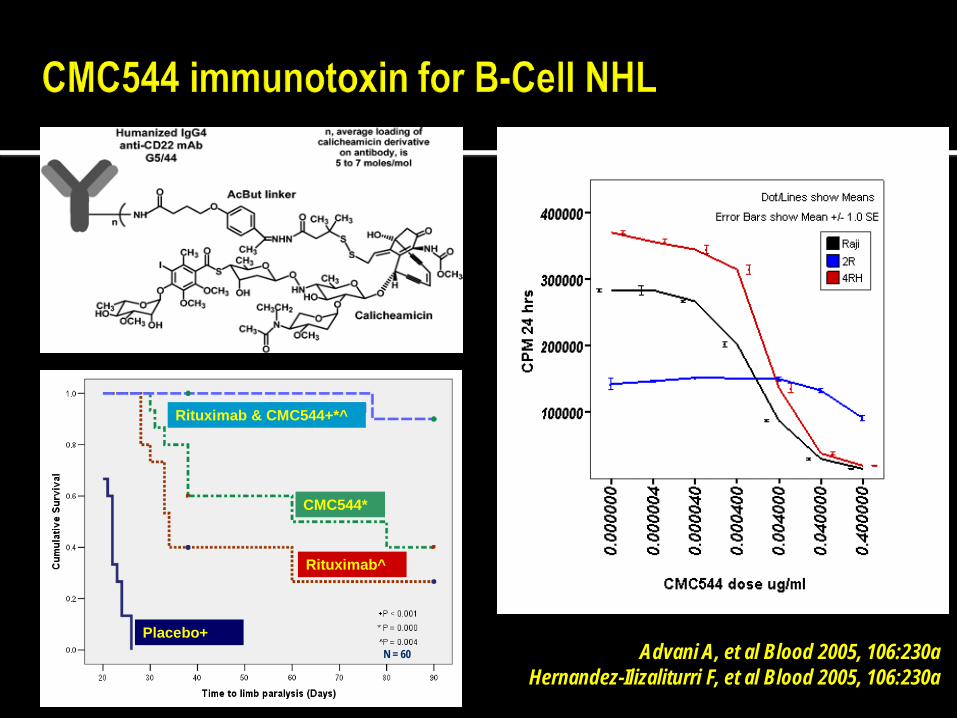
Advani A, et al Blood 2005, 106:230a Hernandez-Ilizaliturri F, et al Blood 2005, 106:230a
N = 60N = 60
Rituximab & CMC544+*^
CMC544*
Rituximab^
Placebo+N = 60N = 60
Rituximab & CMC544+*^
CMC544*
Rituximab^
Placebo+
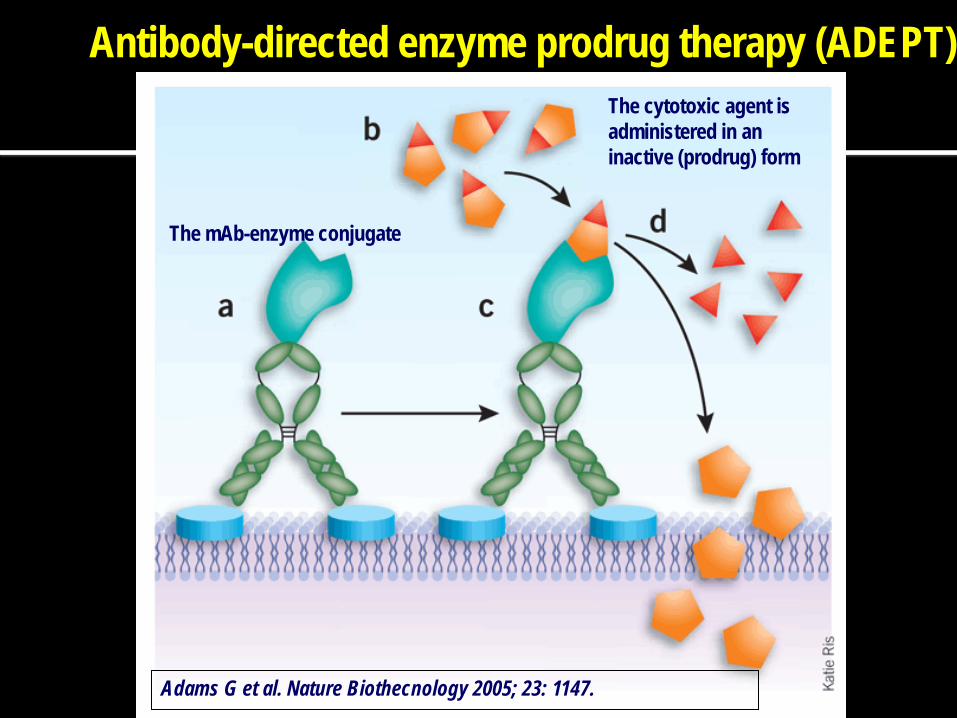
Antibody-directed enzyme prodrug therapy (ADEPT)
The mAb-enzyme conjugate
The cytotoxic agent is administered in an inactive (prodrug) form
Adams G et al. Nature Biothecnology 2005; 23: 1147.
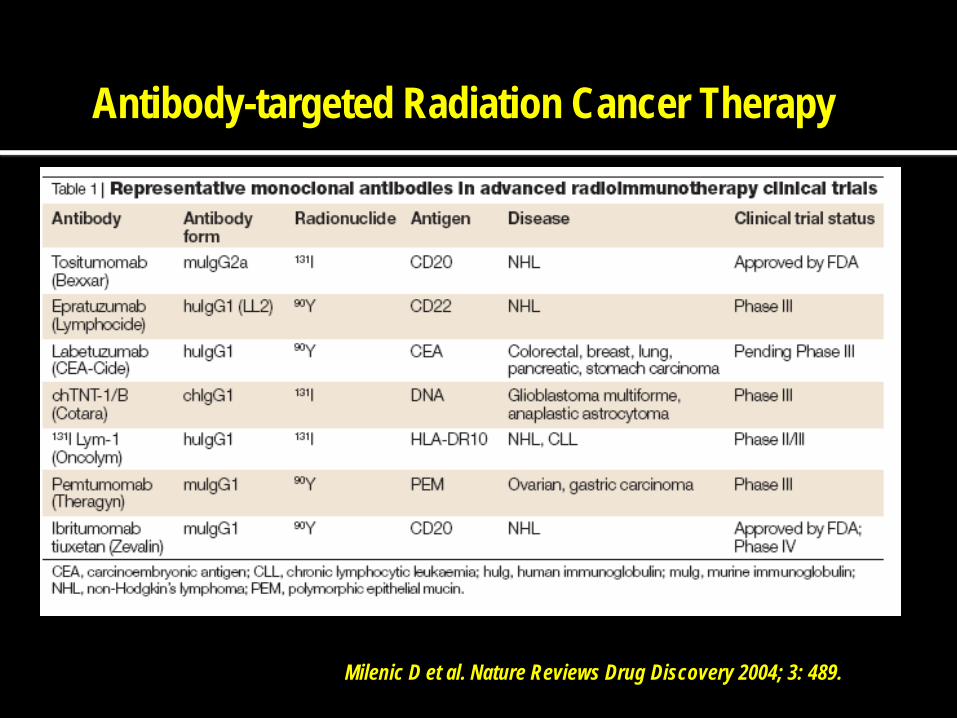
Antibody-targeted Radiation Cancer Therapy
Milenic D et al. Nature Reviews Drug Discovery 2004; 3: 489.
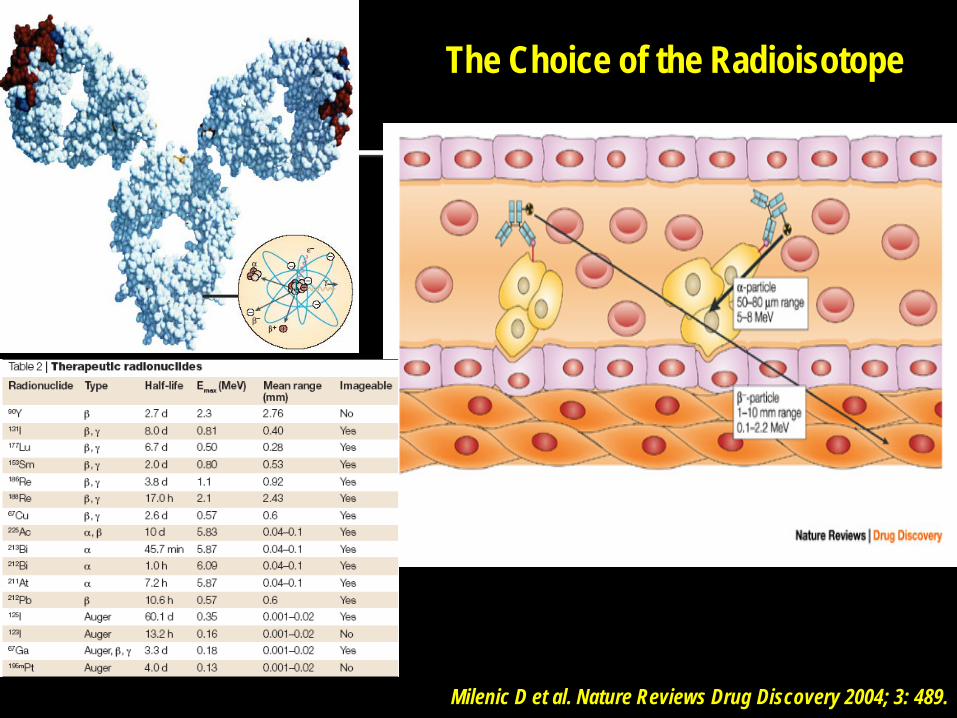
Milenic D et al. Nature Reviews Drug Discovery 2004; 3: 489.
The Choice of the Radioisotope
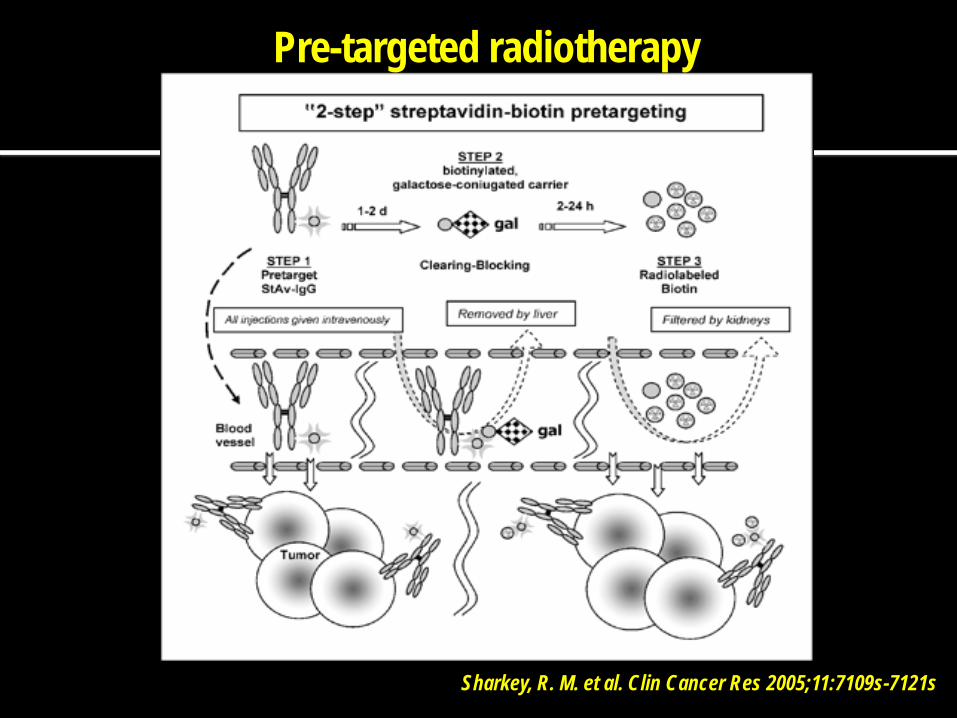
Pre-targeted radiotherapy
Sharkey, R. M. et al. Clin Cancer Res 2005;11:7109s-7121s
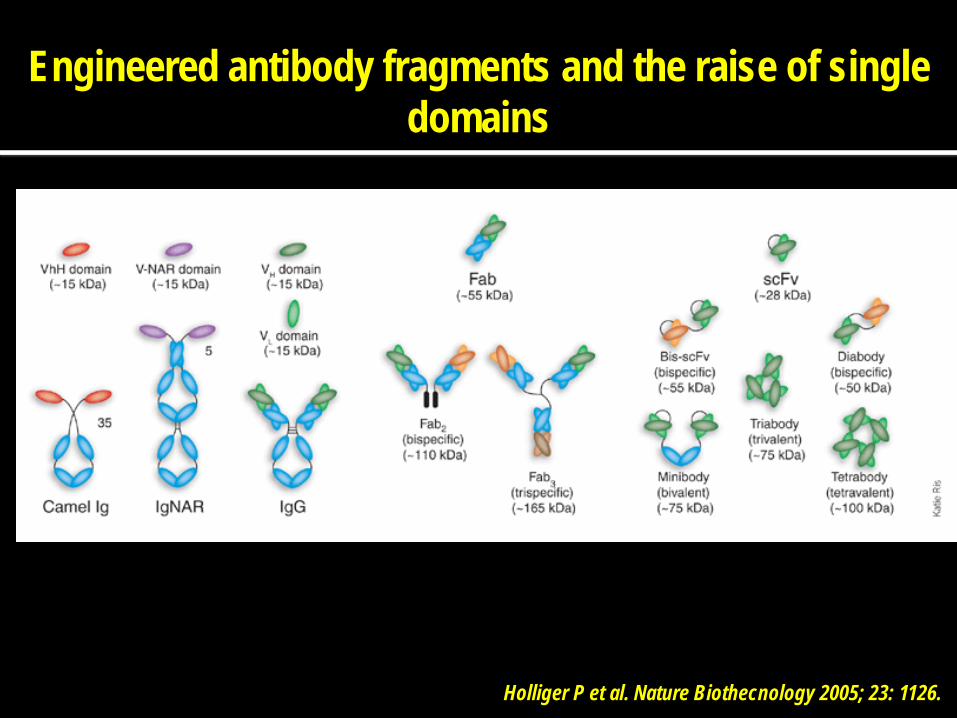
Engineered antibody fragments and the raise of single domains
Holliger P et al. Nature Biothecnology 2005; 23: 1126.

LS174T Colon Ca C6 Glioma
Imaging 18 hrs after infusion of a 124I labeled anti-CEA T84.66 diabody, minibody
or scFv-Fc
Engineered antibody fragments
Holliger P et al. Nature Biothecnology 2005; 23: 1126.
Anti-Her2/neu abs

CD80
CD86
CD28
CD152
APC T-cell
Dominant interaction
CTLA-4 expression and T-cell activation
APC T-cell
Dominant interaction
Inactivation of CD28 mediated signaling, i.e. T-cell inactivation
APC T-cell
Galiximab biding to CD80
Inactivation of the negative interaction between CD152 and CD80 leading to T-cell activation
Can mAb trigger adaptive immune responses? Galiximab, ipilimumab
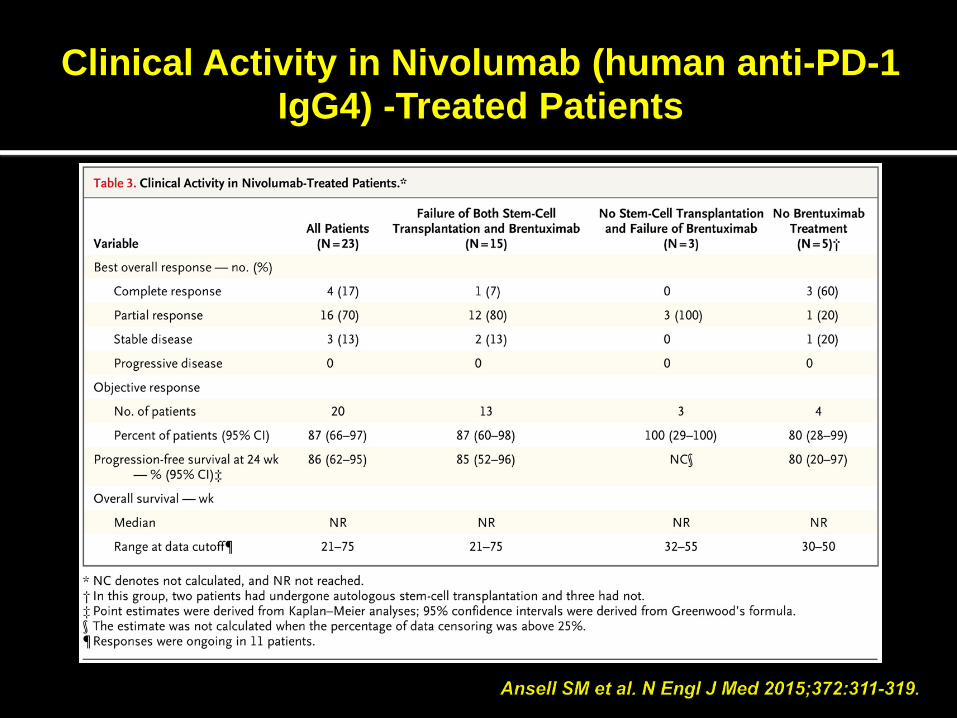
Clinical Activity in Nivolumab (human anti-PD-1 IgG4) -Treated Patients
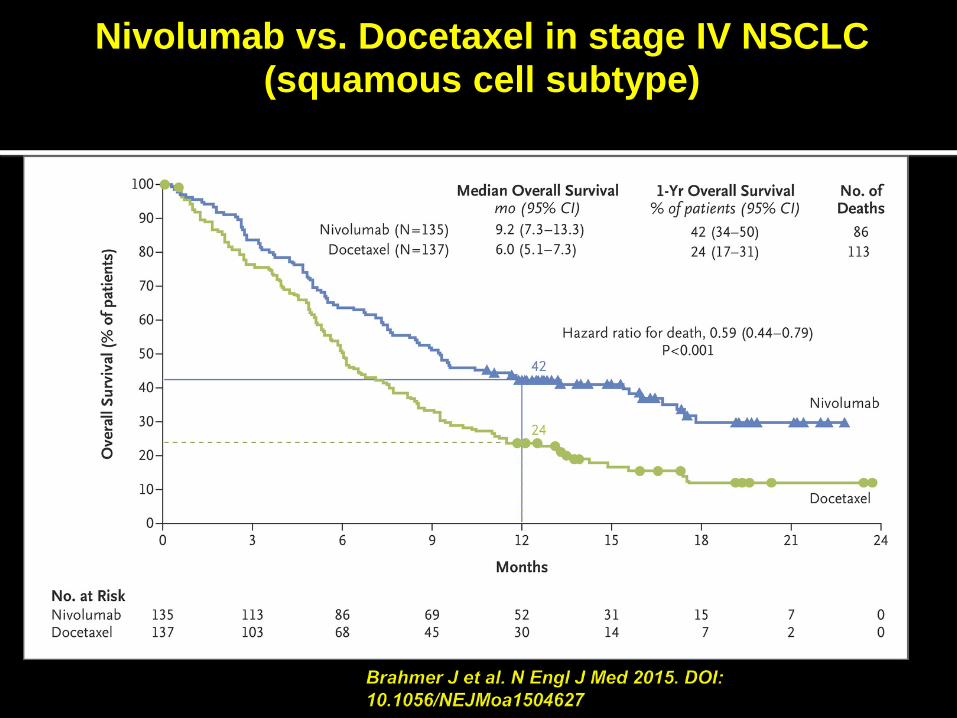
Nivolumab vs. Docetaxel in stage IV NSCLC (squamous cell subtype)

Recommended






![Monoclonal Antibodies - Copy [Autosaved]](https://img.dokumen.tips/doc/110x75/577c7e6a1a28abe054a109e9/monoclonal-antibodies-copy-autosaved.jpg)










![Monoclonal antibodies [autosaved]](https://img.dokumen.tips/doc/110x75/55a733441a28ab80028b4829/monoclonal-antibodies-autosaved.jpg)