Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/304573118
Theefficacyofpainneuroscienceeducationonmusculoskeletalpain:Asystematicreviewoftheliterature
ArticleinPhysiotherapyTheoryandPractice·June2016
DOI:10.1080/09593985.2016.1194646
READS
275
4authors:
AdriaanLouw
InternationalSpineandPainInstitute
40PUBLICATIONS277CITATIONS
SEEPROFILE
KoryZimney
UniversityofSouthDakota
9PUBLICATIONS13CITATIONS
SEEPROFILE
EmilioLouiePuentedura
UniversityofNevada,LasVegas
56PUBLICATIONS431CITATIONS
SEEPROFILE
InaDiener
StellenboschUniversity
24PUBLICATIONS185CITATIONS
SEEPROFILE
Allin-textreferencesunderlinedinbluearelinkedtopublicationsonResearchGate,
lettingyouaccessandreadthemimmediately.
Availablefrom:AdriaanLouw
Retrievedon:13August2016
https://www.researchgate.net/publication/304573118_The_efficacy_of_pain_neuroscience_education_on_musculoskeletal_pain_A_systematic_review_of_the_literature?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_2https://www.researchgate.net/publication/304573118_The_efficacy_of_pain_neuroscience_education_on_musculoskeletal_pain_A_systematic_review_of_the_literature?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_3https://www.researchgate.net/?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_1https://www.researchgate.net/profile/Adriaan_Louw?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_4https://www.researchgate.net/profile/Adriaan_Louw?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_5https://www.researchgate.net/profile/Adriaan_Louw?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_7https://www.researchgate.net/profile/Kory_Zimney?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_4https://www.researchgate.net/profile/Kory_Zimney?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_5https://www.researchgate.net/institution/University_of_South_Dakota?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_6https://www.researchgate.net/profile/Kory_Zimney?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_7https://www.researchgate.net/profile/Emilio_Puentedura?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_4https://www.researchgate.net/profile/Emilio_Puentedura?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_5https://www.researchgate.net/institution/University_of_Nevada_Las_Vegas?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_6https://www.researchgate.net/profile/Emilio_Puentedura?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_7https://www.researchgate.net/profile/Ina_Diener2?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_4https://www.researchgate.net/profile/Ina_Diener2?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_5https://www.researchgate.net/institution/Stellenbosch_University?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_6https://www.researchgate.net/profile/Ina_Diener2?enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ%3D%3D&el=1_x_7
REVIEW
The efficacy of pain neuroscience education on musculoskeletal pain:A systematic review of the literatureAdriaan Louw, PT, PhDa, Kory Zimney, PT, DPTb, Emilio J. Puentedura, PT, DPT, PhDc, and Ina Diener, PT, PhDd
aInternational Spine and Pain Institute, Story City, IA, USA; bDepartment of Physical Therapy, School of Health Sciences, University of SouthDakota, Vermillion, SD, USA; cDepartment of Physical Therapy, School of Allied Health Sciences, University of Nevada, Las Vegas, Las Vegas,NV, USA; dDepartment of Physiotherapy, Stellenbosch University, Stellenbosch, South Africa
ABSTRACTObjective: Systematic review of randomized control trials (RCTs) for the effectiveness of painneuroscience education (PNE) on pain, function, disability, psychosocial factors, movement, and health-care utilization in individuals with chronic musculoskeletal (MSK) pain. Data Sources: Systematicsearches were conducted on 11 databases. Secondary searching (PEARLing) was undertaken, wherebyreference lists of the selected articles were reviewed for additional references not identified in theprimary search. Study Selection: All experimental RCTs evaluating the effect of PNE on chronicMSK painwere considered for inclusion. Additional Limitations: Studies published in English, published withinthe last 20 years, and patients older than 18 years. No limitationswere set on specific outcomemeasures.Data Extraction: Data were extracted using the participants, interventions, comparison, and outcomes(PICO) approach. Data Synthesis: Study quality of the 13 RCTs used in this review was assessed by2 reviewers using the PEDro scale. Narrative summary of results is provided for each study in relation tooutcomes measurements and effectiveness. Conclusions: Current evidence supports the use of PNEfor chronic MSK disorders in reducing pain and improving patient knowledge of pain, improvingfunction and lowering disability, reducing psychosocial factors, enhancing movement, and minimizinghealthcare utilization.
ARTICLE HISTORYReceived 12 November 2015Revised 19 December 2015Accepted 26 January 2016
KEYWORDSChronic pain; explain pain;pain neuroscienceeducation; therapeuticneuroscience education
Introduction
Pain is a normal human experience and the inability toexperience pain provides a significant risk to survivalfor any human being (Gifford, 2014; Moseley, 2003a;Moseley, 2007). Living in pain though is not a normalhuman experience and a powerful motivating force toseek help (Bernard and Wright, 2004; Louw, Louw, andCrous, 2009; Mortimer et al., 2003). One treatmentstrategy aimed at helping ease pain and often theassociated suffering and disability is patient education(Brox et al., 2008; Engers et al., 2008; Heymans et al.,2005; Liddle, Gracey, and Baxter, 2007). Traditionalmusculoskeletal (MSK) education models have focusedheavily on biomedical education focusing on anatomy,biomechanics, and pathoanatomy (Brox et al., 2008;Maier-Riehle and Härter, 2001; Moseley, 2003a, 2004).In these educational models clinicians aim to explain apain experience to patients from a tissue perspective, beit contrasting healthy (anatomy) and injured tissues(pathoanatomy) or highlighting a mechanical deviancefrom normal expected patterns of movement (biome-chanics) or a disease state such as degenerative changes(pathoanatomy) (Haldeman, 1990; Louw and Butler,
2011). Although these models may have clinical valuein more acute phases of injury, surgical, or diseasestates, they lack the ability to explain complex issuesassociated with pain, including peripheral and centralsensitization, facilitation and inhibition, neuroplasticity,immune and endocrine changes, and more, all of whichhave been implicated in more complex and persistentpain states (Gifford, 2014; Moseley, 2003a; Nijs et al.,2013; Woolf, 2007). Furthermore, these biomedicaleducational models have not only shown limited effi-cacy in alleviating pain and disability (Brox et al., 2008;Koes, van Tulder, van der Windt, and Bouter, 1994;Maier-Riehle and Härter, 2001; Waddell, 2004) but mayeven increase patient fears, anxiety, and stress, thusnegatively impacted their intended outcomes (Hirschand Liebert, 1998; Maier-Riehle and Härter, 2001;Nachemson, 1992; Poiraudeau et al., 2006).
In lieu of the limited efficacy of traditional education toalleviate pain and disability, especially in persistent pain, anew model was needed and proposed (Butler andMoseley, 2003; Gifford, 1998; Gifford, 2014; Gifford andButler, 1997; Gifford and Muncey, 1999; Moseley andButler, 2015). People in pain are interested in learning
CONTACT Adriaan Louw, PT, PhD [email protected] International Spine and Pain Institute, P.O. Box 232, Story City, IA 50248, USA.
PHYSIOTHERAPY THEORY AND PRACTICEhttp://dx.doi.org/10.1080/09593985.2016.1194646
© 2016 Taylor & Francis
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
https://www.researchgate.net/publication/13531014_The_physical_and_psychological_experience_of_pain_The_effects_of_labeling_and_cold_pressor_temperature_on_three_pain_measures_in_college_women?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/13531014_The_physical_and_psychological_experience_of_pain_The_effects_of_labeling_and_cold_pressor_temperature_on_three_pain_measures_in_college_women?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/14030942_The_integration_of_pain_science_into_clinical_practice?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/14030942_The_integration_of_pain_science_into_clinical_practice?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/5823405_Systematic_review_of_back_schools_brief_education_and_fear-avoidance_training_for_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/5823405_Systematic_review_of_back_schools_brief_education_and_fear-avoidance_training_for_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/5823405_Systematic_review_of_back_schools_brief_education_and_fear-avoidance_training_for_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/21009682_North_American_Spine_Society_failure_of_the_pathology_model_to_predict_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/233581683_Reconceptualising_pain_according_to_modern_pain_science?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8945857_Evidence_for_a_direct_relationship_between_cognitive_and_physical_change_during_an_education_intervention_in_people_with_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/246556801_Pain_the_Tissues_and_the_Nervous_System_A_conceptual_model?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/278127279_Chronic_pain_in_the_ED?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/7043310_Fear-avoidance_beliefs_about_back_pain_in_patients_with_subacute_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/11788203_The_effects_of_back_schools_-_A_meta-analysis?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/11788203_The_effects_of_back_schools_-_A_meta-analysis?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/11788203_The_effects_of_back_schools_-_A_meta-analysis?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/277726211_15_Years_of_Explaining_Pain_-_The_Past_Present_and_Future?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/277726211_15_Years_of_Explaining_Pain_-_The_Past_Present_and_Future?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/292698054_Preoperative_education_for_lumbar_surgery_for_radiculopathy?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/292698054_Preoperative_education_for_lumbar_surgery_for_radiculopathy?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/10621657_A_pain_neuromatrix_approach_to_patients_with_chronic_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/10621657_A_pain_neuromatrix_approach_to_patients_with_chronic_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/10621657_A_pain_neuromatrix_approach_to_patients_with_chronic_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/51378861_Advice_for_the_management_of_low_back_pain_A_systematic_review_of_randomised_controlled_trials?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/7560707_Back_schools_for_nonspecific_low_back_pain_a_systematic_review_within_the_framework_of_the_Cochrane_Collaboration_Back_Review_Group?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/7560707_Back_schools_for_nonspecific_low_back_pain_a_systematic_review_within_the_framework_of_the_Cochrane_Collaboration_Back_Review_Group?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==
more about their pain (Louw, Louw, and Crous, 2009;Louw, Diener, Butler, and Puentedura, 2013; Moseley,2003b; Rönnberg et al., 2007). This educational model ofteaching people about pain biology and physiology iscalled therapeutic neuroscience education (Louw,Puentedura, Diener, and Peoples 2015; Zimney, Louw,and Puentedura, 2014), explain pain (Butler andMoseley, 2003; Moseley and Butler, 2015), and pain neu-roscience education (PNE) (Nijs et al., 2011, 2013). PNEaims to explain to patients the biological and physiologi-cal processes involved in a pain experience and, moreimportantly, defocus the issues associated with the anato-mical structures (Louw, Diener, Butler, and Puentedura,2011; Moseley, 2007; Moseley, Nicholas, and Hodges,2004; Nijs et al., 2011, 2013). Following early calls forthe further study and clinical application of PNE(Gifford, 1998; Gifford and Butler, 1997) and the firstconference presentation of explaining pain to patients(Gifford and Muncey, 1999), scientists used an evi-dence-based platform to further investigate PNE.Subsequently, various randomized controlled trials(RCT) and two systematic reviews explored the efficacyof PNE (Clarke, Ryan, and Martin, 2011; Louw, Diener,Butler, and Puentedura, 2011; Meeus et al., 2010; Moseley,2002; Moseley, Nicholas, and Hodges, 2004; Ryan, Gray,Newton, and Granat, 2010). At the end of 2011, thesystematic review of Louw, Diener, Butler, andPuentedura (2011) demonstrated for MSK pain, TNEprovides compelling evidence in reducing pain, disability,pain catastrophization, and limited physical movement.
The review by Louw, Diener, Butler, and Puentedura(2011) included eight studies (Meeus et al., 2010;Moseley, 2002, 2003b, 2003c, 2004; Moseley, Nicholas,and Hodges, 2004; Ryan, Gray, Newton, and Granat,2010; Van Oosterwijck et al., 2011), ranging in datefrom 2002 (Moseley, 2002) to 2011 (Van Oosterwijcket al., 2011). Since the publication of the last systematicreview, various studies utilizing PNE have been pub-lished (Gallagher, McAuley, and Moseley, 2013;Ittersum et al., 2014; Louw, Diener, Landers, andPuentedura, 2014; Robinson and King, 2011; VanIttersum, van Wilgen, Groothoff, and Van der Schans,2011). This growth of additional PNE studies, alongwith the reflection by Moseley and Butler (2015) on15 years of teaching people about pain begs the ques-tion if the increased research activity in PNE hasresulted in any increased evidence for this educationalapproach? The original review was also handicapped inassessing efficacy by including lower level papers andthe inability to evaluate methodologically each study incomparative fashion. The goal of this systematic reviewis to update and explore the efficacy of PNE as atreatment approach for people suffering MSK pain.
Methods
In line with the goal of the updated systematic review,the authors used the same methodology reported byLouw, Diener, Butler, and Puentedura (2011) as ameans to add to and thus combine the cumulativeevidence for PNE. The end result would be an expan-sion of the research results ranging from 2002(Moseley, 2002) to the present. Additionally, the newreview only included RCTs.
Search strategy
An electronic search was performed between June 2015and August 2015, covering the last 14 years (2002–2015)from the following databases: Biomed Central, BMJ.com,CINAHL, the Cochrane Library, NLM Central Gateway,OVID, ProQuest (Digital Dissertations), PsycInfo,PubMed/Medline, ScienceDirect, and Web of Science.Each database has its own indexing terms and functions,and therefore different search strategies were developedfor each database by the authors. The main searchitems were education, neuroscience, neurobiology, neu-rophysiology, pain, pain education, pain science, andtherapeutic. In PubMed, medical subject headings(MeSH) terms were used where possible, with Booleanoperators. The search strategies for remaining databasesincluded synonyms of the main search items. Secondarysearching (PEARLing) was undertaken, whereby refer-ence lists of the selected articles were reviewed foradditional references not identified in the primary search.The titles and abstracts of all the identified literature werescreened by one primary reviewer using the inclusioncriteria below. The full text of all potentially relevantarticles were retrieved and screened by two reviewersusing the same criteria, in order to determine theeligibility of the paper for inclusion in the review.
Inclusion criteria
All titles and abstracts were read to identify relevantpapers. Papers were included in this systematic reviewif they met the inclusion criteria listed in Table 1. Giventhe heterogeneous nature of the original systematicreview’s outcome measures, no parameters were seton the exact measurement tools used to assess the effectof PNE on patients suffering from MSK pain. Whenthere was uncertainty regarding the eligibility of thepaper from the abstract, the full text version of thepaper was retrieved and evaluated against the inclusioncriteria. The full text version of all papers that met theinclusion criteria were retrieved for quality assessmentand data extraction.
2 A. LOUW ET AL.
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
https://www.researchgate.net/publication/11024294_Combined_physiotherapy_and_education_is_efficacious_for_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==
Quality assessment
Critical appraisal of each included study was conductedby determining the level of evidence on the AustralianNational Health and Medical Research Council(NHMRC) Hierarchy of Evidence (National Healthand Medical Research Council, 1999). This provides abroad indication of bias based on study design. Studieshigher on the hierarchy potentially contain less biasthan those that are lower on the hierarchy. Given theincreased activity in the field of PNE, study designsother than RCT were excluded in this review becauseof the lower level of evidence they provide.
Methodological quality of the design and reporting ofeach study was assessed against the PEDro scale (Elkinset al., 2010). The PEDro scale has become widely used torate physical therapy interventions and has been shownto have reliability and a valid measure of methodologicalquality of clinical trials (de Morton, 2009; Maher et al.,2003). A high-quality study was defined by the authorsas scoring positive on a minimum of 50% (5/10) ofthe items. Each reviewer conducted an independentevaluation and PEDro scoring of the studies in thereview. The Physiotherapy Evidence Database wascross-referenced for any article already having aconfirmed review, and the confirm score was used ifpresent. If differences were found between reviewers,a discussion was held to attempt consensus. Any differ-ences that could not be agreed upon were to be evaluatedby a third reviewer (E. J. Puentedura) to come to a finaljudgement among all reviewers. No disagreements inPEDro scoring occurred during assessment of thearticles.
Outcome assessment
Due to the heterogeneous nature of the original systema-tic review’s outcome measures and to determine thepossible influence of PNE for MSK pain, results wereposted in narrative form and outcomes were defined as“positive” (experimental group obtained a significantlygreater improvement than the control group); “neutral”(there were no statistically significant differences
between the groups); or “negative” (the control groupobtained a significant greater improvement than theexperimental group). An alpha of p < 0.05 was used todefine a significant outcome measure. This method, usedin previous systematic reviews, demonstrated four levelsof scientific evidence on the quality and the outcome ofthe trials: (1) strong evidence: multiple, relevant, high-quality RCTs with generally consistent outcomes;(2) moderate evidence: one relevant, high-quality RCTAND one or more relevant, low-quality RCTs with gen-erally consistent outcomes; (3) limited evidence: onerelevant, high-quality RCT OR multiple relevant low-quality RCTs with generally consistent outcomes; and(4) inconclusive evidence: only one relevant, low-qualityRCT, no relevant RCTs or randomized trials withinconsistent outcomes (Ezzo et al., 2000; Fernández-de-las-Peñas et al., 2006).
A study was considered “relevant” when at least oneof the outcome measures concerned pain or disability.For being “generally consistent,” at least 75% of thetrials that analyzed the same PNE had to have thesame result (positive, neutral, or negative).
Data extraction
Data were extracted by the authors using the PICOapproach: Participants: diagnosis treated, age, sex, dura-tion of the symptoms, type of referral source,and diagnostic criteria; Interventions: type, intensity,duration, educational tools/props, in combination orstand-alone physical therapy; Comparison: to anothertreatment, no treatment, or “usual” treatment; andOutcomes: domains and tools used to measure the effectsof the intervention. Although outcomes were not speci-fied or limited, primary outcomes in line with “relevance”stated above included pain and/or function (Stone, 2002).
Data on the effectiveness of the PNE were alsoextracted for each study. To determine the effect ofthe PNE on each outcome measure, the mean and95% confidence intervals (CI) for the between-groupdifferences were calculated for RCTs and comparativestudies, based on the results provided in each article
Table 1. Inclusion criteria used in the systematic review.Criterion Justification
English language Search reviewers’ primary language is English, and major journals in the subject area are published inEnglish.
1999–2015 First study found was published in 2002.Humans older than 18 years Increase homogeneity of participants between studies as educational needs for infants, children, and
adolescents.MSK pain Increase homogeneity of participants being treated with educational strategies incorporating PNE.RCTs Utilization of Level 1 evidence according to Centre for Evidence-based Medicine.PNE Increase homogeneity on type of educational intervention.Outcomes: pain, function, psychosocial factors,movement, healthcare utilization
These are primary outcome measurements performed in the literature regarding individuals withMSK pain. No limitation was set on specific measurement tools utilized to examine effect onoutcomes in these areas.
PHYSIOTHERAPY THEORY AND PRACTICE 3
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
https://www.researchgate.net/publication/11214288_Popping_the_PICO_question_in_research_and_evidence-based_practice?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/287176734_Is_acupuncture_effective_for_the_management_of_chronic_pain_A_systematic_review?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/47460008_Rating_the_quality_of_trials_in_systematic_reviews_of_physical_therapy_interventions?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/47460008_Rating_the_quality_of_trials_in_systematic_reviews_of_physical_therapy_interventions?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/26234749_The_PEDro_scale_is_a_valid_measure_of_the_methodological_quality_of_clinical_trials_a_demographic_study?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==
(Herbert, 2000). Moreover, the mean changes betweenpre- and post-treatment (and 95% CI) were calculatedfor the RCTs. Pain reduction of more than 20%, irre-spective of the measurement tool used, was consideredclinically worthwhile (Farrar et al., 2001; Ferreira et al.,2002). It was expected that there would be heterogene-ity in participants, interventions, comparisons, andoutcomes. Therefore, the results of the studies weresynthesized in a narrative format.
Results
Search strategy yield
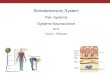
Initially, therewere 25,911hits gathered fromdatabases andsecondary searches for the search dates defined in themethods. After reviewing titles and abstracts, articlesnot meeting inclusion criteria were removed. Full textreview left 99 eligible articles, after removal ofduplicates there were 8 studies from the updated review
Table 2. Assessment of the quality of the randomized trials (n = 13) using the PEDro scale.Criteria 1 2 3 4 5 6 7 8 9 10 11 Total
Moseley (2002) Y Y Y Y N N Y Y Y Y Y 8/10Moseley (2003c) Y Y Y Y N N Y Y N Y Y 7/10Moseley et al. (2004) Y Y Y Y Y Y Y Y N Y Y 9/10Ryan et al. (2010) Y Y Y Y N Y Y Y N Y Y 8/10Meeus et al. (2010) Y Y Y Y Y N Y Y Y Y Y 9/10Vibe Fersum et al. (2013) Y Y Y Y Y N Y N N Y Y 7/10Gallagher et al. (2013) Y Y Y Y Y Y Y Y Y Y Y 10/10Van Oosterwijck et al. (2013) Y Y Y Y Y N Y Y Y Y Y 9/10Ittersum et al. (2014) Y Y Y Y N N Y N Y Y Y 7/10Louw et al. (2014) Y Y Y Y Y N Y Y Y Y Y 9/10Téllez-García et al. (2014) Y Y Y Y N N Y Y Y Y Y 8/10Beltran-Alacreu et al. (2015) Y Y Y Y N N Y Y Y Y Y 8/10Pires et al. (2015) Y Y Y Y N sN Y Y Y Y Y 8/10
Figure 1. Retrieval and review process.
4 A. LOUW ET AL.
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
https://www.researchgate.net/publication/290928812_Clinical_importance_of_changes_in_chronic_pain_intensity_measured_on_an_11-point_numerical_pain_rating_scale?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/11024292_Does_spinal_manipulative_therapy_help_people_with_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/11024292_Does_spinal_manipulative_therapy_help_people_with_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/11675650_How_to_estimate_treatment_effects_from_reports_of_clinical_trials_I_Continuous_outcomes?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==
along with 5 eligible studies from previous review. Thissystematic review is based on these 13 published RCTs(Figure 1) (Beltran-Alacreu, Lopez-de-Uralde-Villanueva,Fernandez-Carnero, and La Touche, 2015; Gallagher,McAuley, and Moseley, 2013; Ittersum et al., 2014; Louw,Diener, Landers, and Puentedura, 2014; Meeus et al., 2010;Moseley, 2002, 2003c; Moseley, Nicholas, and Hodges,2004; Pires, Cruz, and Caeiro, 2015; Ryan, Gray, Newton,and Granat, 2010; Téllez-García et al., 2014; VanOosterwijck et al., 2013; Vibe Fersum et al., 2013). The13 RCTs comprised 734 patients.
Critical appraisal
Hierarchy of evidenceAll 13 published papers were RCTs.
Methodological qualityThe papers were reviewed against the PEDro scale.Agreement was obtained between reviewers and com-pared with the PEDro Database on each of the cri-teria in the PEDro scale with results listed in Table 2.All the studies scored a 6/10 or higher on the PEDroscale demonstrating good methodological quality.The blinding of subjects and those that administeredthe therapy were the most common criteria not met.This is partially due to the face-to-face delivery styleof the intervention of PNE making it difficult toblind the person providing and receiving the PNE.
Educational content and delivery methods
Naming the interventionThe original systematic review (Louw, Diener, Butler,and Puentedura, 2011) reported on the variousnames given to the educational intervention ofexplaining the biology of the pain experience to thepatient with the aim at reducing pain and disability.The continued variation in the interventional nameused by the various authors continues: (1) pain neu-rophysiology education (Pires, Cruz, and Caeiro,2015); (2) therapeutic patient education (Beltran-Alacreu, Lopez-de-Uralde-Villanueva, Fernandez-Carnero, and La Touche, 2015); (3) neuroscienceeducation (Téllez-García et al., 2014); (4) painphysiology education (Meeus et al., 2010; Moseley,2003c; Van Oosterwijck et al, 2013); (5) Pain neu-roscience education (Ittersum et al, 2014; Louw,Diener, Landers, and Puentedura, 2014); (6) neuro-physiology education (Moseley, Nicholas, andHodges, 2004); (7) pain biology education (Ryan,Gray, Newton, and Granat, 2010); and (8) neurophy-siology of pain education (Moseley, 2002).
Two studies did not directly call the educationalintervention a specific name but were a part of a bookof metaphors and stories to help understand thebiology of pain (Gallagher, McAuley, and Moseley,2013) and the cognitive component of the educationintervention (Vibe Fersum et al., 2013).
Patient characteristicsThere were 734 subjects in the reviewed manuscriptswith 398 of them receiving PNE (70% female). Themean age of subjects receiving educational interventionwas 41.7 years (calculated from the means of the meanreported ages from each study). The youngest cohorthad a mean age of 24 ± 10 years (Moseley, Nicholas,and Hodges, 2004) and the oldest cohort had 50.9 ± 6.2years (Pires, Cruz, and Caeiro, 2015). PNE was utilizedfor multiple pain conditions: low back pain, chronicfatigue syndrome, fibromyalgia, lumbar radiculopathyawaiting lumbar surgery, and chronic neck pain.
Content of therapeutic neuroscience educationSpecific content of each of the educational sessions canbe found in Table 3. Summary of the PNE content were
● Neurophysiology of pain (Beltran-Alacreu, Lopez-de-Uralde-Villanueva, Fernandez-Carnero, and LaTouche, 2015; Gallagher, McAuley, and Moseley,2013; Ittersum et al., 2014; Louw, Diener, Landers,and Puentedura, 2014; Meeus et al., 2010;Moseley, 2002, 2003c; Moseley, Nicholas, andHodges, 2004; Pires, Cruz, and Caeiro, 2015;Ryan, Gray, Newton, and Granat, 2010; VanOosterwijck et al., 2013; Vibe Fersum et al., 2013)
● No reference of anatomic or patho-anatomicmodels (Moseley, 2002, 2003c; Moseley, Nicholas,and Hodges, 2004; Téllez-García et al., 2014)
● No discussion of the emotional or behavioralaspects of pain (Moseley, 2003c; Moseley,Nicholas, and Hodges, 2004)
● Nociception and nociceptive pathways (Gallagher,McAuley, and Moseley, 2013; Ittersum et al., 2014;Louw, Diener, Landers, and Puentedura, 2014;Moseley, 2003c; Moseley, Nicholas, and Hodges,2004; Pires, Cruz, and Caeiro, 2015; Téllez-Garcíaet al., 2014)
● Synapses (Moseley, 2003c; Moseley, Nicholas, andHodges, 2004)
● Action potentials (Louw, Diener, Landers, andPuentedura, 2014)
● Spinal inhibition and facilitation (Gallagher,McAuley, and Moseley, 2013; Moseley, 2003c;Van Oosterwijck et al., 2013; Vibe Fersum et al.,2013)
PHYSIOTHERAPY THEORY AND PRACTICE 5
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
https://www.researchgate.net/publication/11024294_Combined_physiotherapy_and_education_is_efficacious_for_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/11024294_Combined_physiotherapy_and_education_is_efficacious_for_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/11024294_Combined_physiotherapy_and_education_is_efficacious_for_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/11024294_Combined_physiotherapy_and_education_is_efficacious_for_chronic_low_back_pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/8390478_A_Randomized_Controlled_Trial_of_Intensive_Neurophysiology_Education_in_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/51845607_Louw_A_Diener_I_Butler_DS_Puentedura_EJ_The_effect_of_neuroscience_education_on_pain_disability_anxiety_and_stress_in_chronic_musculoskeletal_pain_YAPMR_201192122041-56?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/51845607_Louw_A_Diener_I_Butler_DS_Puentedura_EJ_The_effect_of_neuroscience_education_on_pain_disability_anxiety_and_stress_in_chronic_musculoskeletal_pain_YAPMR_201192122041-56?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/265475362_Aquatic_exercise_and_pain_neurophysiology_education_versus_aquatic_exercise_alone_for_patients_with_chronic_low_back_pain_A_randomized_controlled_trial?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/265475362_Aquatic_exercise_and_pain_neurophysiology_education_versus_aquatic_exercise_alone_for_patients_with_chronic_low_back_pain_A_randomized_controlled_trial?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/265475362_Aquatic_exercise_and_pain_neurophysiology_education_versus_aquatic_exercise_alone_for_patients_with_chronic_low_back_pain_A_randomized_controlled_trial?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45504301_Pain_Physiology_Education_Improves_Pain_Beliefs_in_Patients_With_Chronic_Fatigue_Syndrome_Compared_With_Pacing_and_Self-Management_Education_A_Double-Blind_Randomized_Controlled_Trial?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45504301_Pain_Physiology_Education_Improves_Pain_Beliefs_in_Patients_With_Chronic_Fatigue_Syndrome_Compared_With_Pacing_and_Self-Management_Education_A_Double-Blind_Randomized_Controlled_Trial?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45504301_Pain_Physiology_Education_Improves_Pain_Beliefs_in_Patients_With_Chronic_Fatigue_Syndrome_Compared_With_Pacing_and_Self-Management_Education_A_Double-Blind_Randomized_Controlled_Trial?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/42833167_Pain_biology_education_and_exercise_classes_compared_to_pain_biology_education_alone_for_individuals_with_chronic_low_back_pain_A_pilot_randomised_controlled_trial?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/42833167_Pain_biology_education_and_exercise_classes_compared_to_pain_biology_education_alone_for_individuals_with_chronic_low_back_pain_A_pilot_randomised_controlled_trial?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45692408_Joining_Forces_-_Combining_Cognition-Targeted_Motor_Control_Training_with_Group_or_Individual_Pain_Physiology_Education_A_Successful_Treatment_For_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45692408_Joining_Forces_-_Combining_Cognition-Targeted_Motor_Control_Training_with_Group_or_Individual_Pain_Physiology_Education_A_Successful_Treatment_For_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45692408_Joining_Forces_-_Combining_Cognition-Targeted_Motor_Control_Training_with_Group_or_Individual_Pain_Physiology_Education_A_Successful_Treatment_For_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45692408_Joining_Forces_-_Combining_Cognition-Targeted_Motor_Control_Training_with_Group_or_Individual_Pain_Physiology_Education_A_Successful_Treatment_For_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45692408_Joining_Forces_-_Combining_Cognition-Targeted_Motor_Control_Training_with_Group_or_Individual_Pain_Physiology_Education_A_Successful_Treatment_For_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45692408_Joining_Forces_-_Combining_Cognition-Targeted_Motor_Control_Training_with_Group_or_Individual_Pain_Physiology_Education_A_Successful_Treatment_For_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45692408_Joining_Forces_-_Combining_Cognition-Targeted_Motor_Control_Training_with_Group_or_Individual_Pain_Physiology_Education_A_Successful_Treatment_For_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45692408_Joining_Forces_-_Combining_Cognition-Targeted_Motor_Control_Training_with_Group_or_Individual_Pain_Physiology_Education_A_Successful_Treatment_For_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==https://www.researchgate.net/publication/45692408_Joining_Forces_-_Combining_Cognition-Targeted_Motor_Control_Training_with_Group_or_Individual_Pain_Physiology_Education_A_Successful_Treatment_For_Chronic_Low_Back_Pain?el=1_x_8&enrichId=rgreq-b149cc5231536143ba3b4772ca18bebf-XXX&enrichSource=Y292ZXJQYWdlOzMwNDU3MzExODtBUzozODAyMDE3NTUyNjcwNzJAMTQ2NzY1ODU3MDk5MQ==
Table3.
Participants,interventions,and
outcom
esin
thereview
edstud
ies.
Participants
Interventio
nsOutcomes
Author
nSample
characteristics
Diagn
ostic
criteria
Treatm
ent
Control
Outcome
instruments
Timeof
assessment
Moseley
(2002)
57●
LBP>2
mon
ths
●Wom
en=
59%
●Ag
e(years):
EG*43
±7
andCG
**38
±7 Durationof
symptom
s(m
onths):EG
=39
±18
and
CG37
±12
NA
Twoph
ysiotherapysessions
perweekfor4
weeks;m
anualtherapy
includ
ingmob
ilizatio
nandmanipulation,softtissuemassage,m
uscle
andneural-m
obilizatio
ntechniqu
es,b
utno
electrop
hysicalm
odalities;specific
trun
kstabilizatio
nprog
ram;m
aintainho
me
exercisesindefin
itely;1
hour
educational
sessionon
ceaweekfor4weeks;o
ne-on-on
eeducationform
atby
anindepend
ent
therapist;content=neurop
hysiolog
yof
pain
with
noreferenceto
lumbarspine;
accompanied
byworkbookwith
onepage
ofrevision
materiala
ndthreecomprehensive
exercisesperdayfor10
days
Ong
oing
medicalcare
asadvisedby
their
generalp
ractition
er.
Noattend
ance
ofph
ysiotherapy
●Num
ericratin
gscale(NRS);
meaning
fuld
if-ferencesetat
2po
ints
●Roland
Morris
Disability
Questionn
aire
(RMDQ);mean-
ingful
diffe
rence
setat
4po
ints
●Num
bers
needed
totreat(NNT)
Baseline,1mon
thafter
interventio
nand1year
afterinterventio
n
Moseley
(2003c)
41●
LBP>3
mon
ths
●Wom
en=EG
67%
andCG
=60%
●Ag
e(years):
EG=40
±7
yearsandCG
=42
±7years
Durationof
symptom
s(m
onths):EG
=33
±11
and
CG=30
±14
NA
Individu
al4×1ho
ureducationalsession
ontheph
ysiology
ofpain
andinjury
bya
physiotherapist;additio
nally
received
two
physiotherapysessions
perweekfor4weeks
focusing
onspinalstabilizatio
nexercises
Group
sessioninvolved
asing
le4-ho
ursession
with
agrou
pof
7–10
patientsprovided
bya
physiotherapist;ph
ysiology
ofpain
andinjury;
additio
nally
received
twoph
ysiotherapy
sessions
perweekfor4weeks
focusing
onspinalstabilizatio
nexercises
●Num
ericratin
gscale(NRS)
●Roland
Morris
Disability
Questionn
aire
(RMDQ)
●Num
bers
needed
totreat(NNT)
Baseline,1mon
thfollowing“ong
oing
medicaltreatm
ent”and1
mon
thand2mon
thsafter
educationaland
physiotherapysessions
(Con
tinued)
6 A. LOUW ET AL.
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
Table3.
(Con
tinued).
Participants
Interventio
nsOutcomes
Author
nSample
characteristics
Diagn
ostic
criteria
Treatm
ent
Control
Outcome
instruments
Timeof
assessment
Moseley
etal.(2004)
58●
LBP>6
mon
ths
●Ag
e(years):
EG=24
±10
andCG
=45
±6
●Durationof
pain
(mon
ths):
EG=18
±11
andCG
=20
±11
NA
Educationsessionby
aph
ysiotherapistinon
e-to-one
seminar
form
at;session
lasted
3ho
urs;
diagramsandhypo
thetical
exam
ples
used
asteaching
tools;at
conclusion
:workbookwith
10sections;p
atientsaskedto
read
one
sectionperdayandansw
erthreequ
estio
nson
each
session
Neurophysiology
Education
Nospecificapplicationwas
madeto
thelower
back,o
rto
emotionaland
behavioralpatterns
common
lyassociated
with
chronicpain
such
ascatastroph
icthou
ghtprocessesor
fear
avoidance
TheNervousSystem
Presentatio
nof
thebasicstructureof
the
nervou
ssystem
,with
afocuson
the
compo
nentsof
theno
ciception/pain
pathways;thissectioninclud
edan
outline
ofthefunctio
nalsignificance
ofeach
compo
nent
Synapses
Presentatio
nof
how
nerves
“talkto
each
other,”
includ
ingtheconceptof
“chemicals”
(neurotransm
itters),p
ostsynaptic
receptors,
andaconceptual“volum
eknob
”(postsynaptic
excitatio
nandinhibitio
n),w
itha
specialfocus
onthe“dangermesseng
ernerve”
(secon
dorderno
ciceptiveneuron
)Plasticity
oftheNervousSystem
Theadaptabilityof
thenervou
ssystem
includ
ing:
afferent
andefferent
pathways;the
variablestateof
neuralstructures
includ
ing
norm
alstate,perip
heral,andcentral
sensitizatio
n;receptor
synthesis;axon
alsprouting;
theneuralrespon
seto
inactivity;
andmovem
entcontrol
Educationsessionby
aph
ysiotherapistinon
e-to-one
seminar
form
at;session
lasted
3ho
urs;
diagramsandhypo
theticalexam
ples
used
asteaching
tools;at
conclusion
:workbookwith
10sections;p
atientsaskedto
read
one
sectionperdayandansw
erthreequ
estio
nson
each
session
BackEducation
Anatom
yandph
ysiology
ofthebo
nesand
jointsof
thelumbarspine;theintervertebral
disc;the
trun
kandback
muscles;n
ormal
spinalcurves;p
osture
andmovem
ents,
includ
inganalysisof
postures
andactivities
accordingto
intra-discalpressuresandjoint
forces;liftingtechniqu
esandliftin
gloads;
liftin
gaids
andergo
nomicsadvice;p
rinciples
ofstretching
;and
streng
th,end
urance,and
fitness
training
Itdidno
tinclud
einform
ationabou
tthe
nervou
ssystem
,exceptforou
tlining
the
locatio
nandcourse
ofthespinalcord
andthe
spinalnerveroots;itwas
similarto
education
materialthathasbeen
researched
elsewhere
andtheeducationcompo
nentsof
back
scho
olsandfunctio
nalrestoratio
nprog
rams
●Roland
Morris
Disability
Questionn
aire
(RMDQ)
●BriefSurvey
ofPain
Attitud
es(revised)(SOPA
(R))
●Pain
Catastroph
ization
Scale(PCS)
●Straight
Leg
Raise(SLR)
(inclinom
eter)
●ForwardBend
ing
Rang
e(Distance
from
long
estfin
-gerto
floor)
●Ab
dominal
Draw
InTask
(ADIT)
Pre-treatm
ent,3weeks
(Con
tinued)
PHYSIOTHERAPY THEORY AND PRACTICE 7
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
Table3.
(Con
tinued).
Participants
Interventio
nsOutcomes
Author
nSample
characteristics
Diagn
ostic
criteria
Treatm
ent
Control
Outcome
instruments
Timeof
assessment
Ryan
etal.(2010)
38●
LBP>3
mon
ths
Educationgroup
●n=18
●11
wom
en●
Age(years)=
45.5
±9.5
●Durationof
pain
(mon
ths)
=13.7
±10.2
Educationand
Exercisegroup
●n=20
●14
wom
en●
Age(years)
45.2
±11.9
●Durationof
pain
(mon
ths)
=7.6±7
NA
PainBiologyOnly
A2.5-ho
urpain
biolog
yeducationsession
Cogn
itive
behavioralinterventio
nfocusedon
reshapingtheparticipant’s
beliefsand
attitud
esabou
ttheirback
pain,attem
ptingto
decrease
fear
avoidanceandharm
beliefs,
increase
self-efficacy,anddecrease
avoidance
behavior
Thebiolog
yof
pain
Verbal
commun
ication,
prepared
diagrams
andfree-handdraw
ings
Additio
nally,all
participants
received
“The
Back
Book”
PainBiologyandExercise
A2.5-
hour
pain
biolog
yeducationsession
Cogn
itive
behavioralinterventio
nfocusedon
reshapingtheparticipant’s
beliefsand
attitud
esabou
ttheirback
pain,attem
ptingto
decrease
fear
avoidanceandharm
beliefs,
increase
self-efficacy,anddecrease
avoidance
behavior
Thebiolog
yof
pain
Verbalcommun
ication,
prepared
diagrams
andfree-handdraw
ings
Additio
nally,allparticipantsreceived
“The
Back
Book”
Exercisecomponent
“Backto
Fitnessexercise
classes”;sixclasses,
oneaweekfor6weeks;the
classesinvolved
circuit-based,
graded,aerob
icexerciseswith
somecore
stability
exercises
Theclassesinvolved
awarm-upph
ase(10
minutes),an
aerobicph
ase(20–30
minutes),
andawarm-dow
nph
ase(10–15
minutes);the
aerobicph
aseinvolved
circuit-basedexercise;
formostexercises,therewas
aneasy,
mod
erate,andhard
version,
andthe
participantcouldchoose
which
versionto
perform
●Roland
Morris
Disability
Questionn
aire
(RMDQ)
●Num
ericRatin
gScale(NRS)
●Repeated
sit-to-
standtest
●The50-footwalk
test
●5-minutewalk
test
●Tampa
Scaleof
Kinesiop
hobia
(TSK-13)
●Pain
Self-Efficacy
Questionn
aire
(PSEQ)
●Step
coun
t(activPA
L™activ-
itymon
itor)
Pre-treatm
entand8weeks
later,3mon
thslater
Meeus
etal.(2010)
46●
Chronicfati-
guesynd
rome
andwide-
spread
pain
●Wom
en:EG=
22andCG
=18
●Ag
e(years):
EG=38.3
±10.6andCG
=42.3
±10.2
1994
Centersfor
Disease
Control
andPreventio
ncriteria
forCFS
(Fukud
aet
al.,
1994)
PainPhysiology
One
30-m
inuteinteractivesession
Physiology
ofthenervou
ssystem
ingeneral
andof
thepain
system
inparticular
Thetheoretic
inform
ationwas
illustrated
with
pictures
andexam
ples
Theob
jectiveof
theeducationwas
toteach
patientsthefunctio
n,mechanism
s,and
mod
ulationof
(chron
ic)pain,and
soforth
PacingandSelf-Management
One
30-m
inuteinteractivesession;pacing
and
self-managem
enteducationwas
provided
toallp
articipantsin
thecontrolg
roup
;pacingis
astrategy
inwhich
patientsareencouraged
toachievean
approp
riate
balancebetween
activity
andrest
inorderto
avoid
exacerbatio
nandto
setrealistic
goalsfor
increasing
activity;followingthisenergy
managem
entstrategy,p
atientsshou
ldavoid
activities
atan
intensity
that
exacerbates
symptom
s,or
they
shou
ldintersperse
activities
with
perio
dsof
rest
●Neuroph
ysiology
ofPain
Test
●Pain
Catastroph
ization
Scale(PCS)
●Pain
Coping
Inventory(PCI)
●Tampa
Scaleof
Kinesiop
hobia
(TSK)
●Pain
Threshold
Assessment
(Fisher
algo
meter)
Pre-treatm
entand
immediatelypo
st-
treatm
ent
(Con
tinued)
8 A. LOUW ET AL.
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
Table3.
(Con
tinued).
Participants
Interventio
nsOutcomes
Author
nSample
characteristics
Diagn
ostic
criteria
Treatm
ent
Control
Outcome
instruments
Timeof
assessment
Vibe
Fersum
etal.
(2013)
94●
Non
-specific
low
back
pain
>3mon
ths
Classification-
basedCognitive
Functional
Therapygroup
(CB-CFT)
●27
wom
enand24
men
●Ag
e(years):
41.0
±10.3
ManualTherapy
andExercise
group(MT-EX)
●21
wom
enand22
men
●Ag
e(years):
42.9
±12.5
NA
CB-CFT
group
Acogn
itive
compo
nent
basedon
finding
sfrom
OrebroMusculoskeletal
Pain
Questionn
aire
Specificmovem
entexercisesas
directed
bythemovem
entclassification
Targeted
functio
nalintegratio
nof
activities
indaily
life
Physicalactivity
prog
ram
tailoredto
the
movem
entclassification;
initialsessionof
1ho
ur,follow-ups
30–45minutes;patientsseen
weeklyforfirst
2–3weeks
andthen
prog
ressed
toon
esessionever
2–3weeks
for
12-weekinterventio
nperio
d;meannu
mberof
treatm
ents
7.7(range
4–16;SD2.6)
MT-EX
group
Jointmob
ilizatio
nor
manipulationtechniqu
esto
spineor
pelvisbeston
currentmanual
therapypractice;generale
xerciseof
motor
controle
xercises;m
otor
controle
xercises
involvingisolated
contractions
ofdeep
abdo
minalmuscles
indiffe
rent
functio
nal
positio
ns;initialsession
,1ho
ur,follow-ups,30
minutes;m
eannu
mberof
treatm
ents
8.0
(range
3–17;SD2.9)
Primaryoutcom
emeasures
●Osw
estry
Disability
Index
(ODI)
●Pain
Intensity
Num
ericRatin
gScale(PINRS)
Secondaryoutcom
es●
Hop
kins
Symptom
sCh
ecklist(HSCL-
25)
●Fear-Avoidance
Belief
Questionn
aire
(FAB
Q)
●Totallum
bar
spinerang
eof
motion
●Patient
satisfaction
●Sick-leavedays
●Care-seeking
Baseline,po
st12-week
interventio
nand12
mon
thspo
st-in
terventio
n
(Con
tinued)
PHYSIOTHERAPY THEORY AND PRACTICE 9
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
Table3.
(Con
tinued).
Participants
Interventio
nsOutcomes
Author
nSample
characteristics
Diagn
ostic
criteria
Treatm
ent
Control
Outcome
instruments
Timeof
assessment
Gallagh
eret
al.
(2013)
79●
Pain
sufficient
todisrup
tactivities
ofdaily
livingfor
>than
pre-
viou
s3
mon
ths
Metaphorsgroup
●n=40
(26
female)
●Ag
e(years):
42±11
●Durationof
pain
(mon
ths):
25±19
Advicegroup
●n=39
(22
female)
●Ag
e(years):
45±11
●Durationof
pain
(mon
ths):
31±20
NA
Booklet1
Metapho
rsandstoriesto
help
understand
the
biolog
yof
pain
Materialfrom
PainfulY
arns:8
0pagesdivided
in11
sections
Readability
onGun
ning
FogIndexwas
7
Booklet2
Advice
abou
tmanagingpain;m
ateriald
rew
from
TheBack
Book
andManageYour
Pain;80
pagesdividedin
11sections;readabilityon
Gun
ning
FogIndexwas
8
Primaryoutcom
emeasures
●Pain
Biolog
yQuestionn
aire
(PBQ
)●
Pain
Catastroph
izing
Scale(PCS)
Secondaryoutcom
es●
Pain
(11-po
int
numericscale)
●Patient-Specific
Functio
nalS
cale
(PSFS)
Baseline,3weeks
and12
weeks
Controlg
roup
cross-over:
15weeks
and24
weeks
(Con
tinued)
10 A. LOUW ET AL.
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
Table3.
(Con
tinued).
Participants
Interventio
nsOutcomes
Author
nSample
characteristics
Diagn
ostic
criteria
Treatm
ent
Control
Outcome
instruments
Timeof
assessment
VanOosterwijcket
al.
(2013)
30●
Fibrom
yalgia
Experim
ental
group
●n=15
(12
wom
en)
●Ag
e(years):
45.8
±9.5
●Durationof
onset
(mon
ths):1
56±96
Controlgroup
●n=15
(14
female)
●Ag
e(years):
45.9
±11.5
Durationof
onset
(mon
ths):1
16±46
1990
American
College
ofRh
eumatolog
y(ACR
)criteria
Experim
entalg
roup
received
educationon
pain
neurop
hysiolog
y;received
inoral
form
atwith
writtenleafletcontaining
inform
ation
andencouraged
totake
homeandread
severaltimes;1
weeklatersecond
interventio
ndelivered
over
theph
one
Controlg
roup
received
educationon
pacing
self-managem
enttechniqu
es;receivedin
oral
form
atwith
writtenleafletcontaining
inform
ationandencouraged
totake
home
andread
severaltimes;1
weeklatersecond
interventio
ndelivered
over
theph
one
Primaryoutcom
emeasures
●Spatial
summa-
tion
procedures
(SSP)
●Fibrom
yalgia
Impact
Questionn
aire
(FIQ)
●Medical
Outcomes
Short
Form
36Health
Status
Survey
(SF-36)
●Pain
Coping
Inventory(PCI)
●Pain
Catastroph
izing
Scale(PCS)
●Pain
Vigilance
andAw
areness
Questionn
aire
(PVA
Q)
●Tampa
Scale
Kinesiop
hobia
(TSK)
●Neuroph
ysiology
ofPain
Test
Secondaryoutcom
es●
Pain
Pressure
Threshold
Baseline,2weeks,3
mon
ths
(Con
tinued)
PHYSIOTHERAPY THEORY AND PRACTICE 11
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
Table3.
(Con
tinued).
Participants
Interventio
nsOutcomes
Author
nSample
characteristics
Diagn
ostic
criteria
Treatm
ent
Control
Outcome
instruments
Timeof
assessment
Ittersum
etal.(2014)
105
●Fibrom
yalgia
Pain
Neuroscience
Educationgroup
●n=53
(50
female)
●Ag
e(years):
47.6
±9.1
●Illness
dura-
tion(years):
8.5
Relaxation
Educationgroup
●n=52
(48
female)
●Ag
e(years):
45.8
±9.8
●Illness
dura-
tion(years):
8.0
American
College
ofRh
eumatolog
y(ACR
)criteria
Pain
NeuroscienceEducationreceived
aneducationalb
ooklet
with
writtenand
illustrated
inform
ationon
painph
ysiology
and
themechanism
sof
centralsensitization;
educationalb
ooklet
explainedstructureand
functio
nof
nervou
ssystem
anddiffe
rence
betweenno
ciceptionandpain;central
sensitizatio
nisintrod
uced
ashypersensitivity
ofthenervou
ssystem
throug
hmetapho
r;explainedfactorsat
onsetandmaintenance
ofcentralsensitization;
threecase
exam
ples
used
toexplainho
wto
usethisinform
ationin
daily
life;bo
okletof
15pages,and
encouraged
toread
severaltimes;received
follow-upsupp
ortin
gteleph
onecall2weeks
post
receivinginform
ation
Relaxatio
neducationgrou
preceived
written
inform
ationon
relaxatio
nexercise
and
instructions
onho
wto
perform
such
exercises;
Loeser’smod
elof
pain
used
tobriefly
explain
physicalandpsycho
logicalfactorswith
chronicpain;b
ooklet
15pages,and
encouraged
toread
severaltimes
andapply
inform
ationin
daily
life;received
follow-up
supp
ortin
gteleph
onecall2weeks
post
receivinginform
ation
Primaryoutcom
emeasures
●Fibrom
yalgia
Impact
Questionn
aire
(FIQ)
Secondaryoutcom
es●
RevisedIllness
Perceptio
nQuestionn
aire
for
FM(IPQ-R_FM)
●Pain
Catastroph
izing
Scale(PCS)
●Patient
opinions
abou
tthebo
ok-
leton
six-po
int
Likertscale
Baseline,6weeks,6
mon
thsfollow-up
Louw
etal.(2014)
67Patientswith
lumbar
radiculopathy
schedu
ledfor
lumbarsurgery
Experim
ental
group
●n=32
●Ag
e(years):
49.59
●Durationof
symptom
s(days):9
1.41
Controlgroup
●n=35
●Ag
e(years):
49.65
●Durationof
symptom
s(days):9
2.29
NA
Pre-op
erativeneuroscience
education(NE)
covered:
(1)decision
tohave
lumbarsurgery;
(2)nervou
ssystem
physiology
andpathways;
(3)perip
heraln
erve
sensitizatio
n;(4)surgical
experiences
andenvironm
entalissues’effects
onnervesensitivity;(5)
calmingthenervou
ssystem
;(6)
recovery
afterlumbarsurgery;(7)
scientificevidence;(8)
reflectionandwriting
questio
nsforsurgeonpriorto
surgery.NE
provided
byph
ysicaltherapistin
one-on
-one
sessionaveraging30
minutes
usingpictures,
exam
ples,m
etapho
rs,and
draw
ings;p
atients
weregivenbo
okletthat
summarized
educationalsession
inform
ationandaskedto
read
atleaston
cebefore
surgery;patients
also
received
“usualcare”regarding
preoperativeeducationfrom
surgeonand
staff
“Usualcare”regardingpreoperativeeducation
from
respectivesurgeonandstaff
Primaryoutcom
emeasures
●Num
ericPain
Ratin
gScales
(NPRS)
●Osw
estry
Disability
Index
(ODI)
Secondaryoutcom
es●
Thou
ghts/beliefs
abou
tsurgery
numericscale(1–
10)
●Health
care
utili-
zatio
nqu
estio
ns
Baseline,1,
3,6,
and12
mon
th(s)
(Con
tinued)
12 A. LOUW ET AL.
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
Table3.
(Con
tinued).
Participants
Interventio
nsOutcomes
Author
nSample
characteristics
Diagn
ostic
criteria
Treatm
ent
Control
Outcome
instruments
Timeof
assessment
Téllez-Garcíaet
al.
(2014)
12●
Chronicno
n-specificlow
back
pain
TrP-DN
group
●n=6(4
female)
●Ag
e(years):
37±13
●Timewith
pain
(mon
ths):
19±8
TrP-DN+EDU
group
●n=6(4
female)
●Ag
e(years):
36±5
●Timewith
pain
(mon
ths):
17±9
NA
Neuroscienceeducationgrou
p(TrP-DN+
EDU)received
30-m
inuteeducationsession,
once
perweekforthelast
twosessions
(treatmentsession2and3)
afterTrP-DN
treatm
ent(asperformed
incontrolg
roup
);face-to-face
individu
alinstructionon
neurop
hysiolog
yof
pain
with
noparticular
referenceto
thelumbarspine;inform
edabou
ttherole
ofbeliefsandattitud
estowardtheir
pain;P
owerPointpresentatio
nbasedon
ExplainPain
was
used;d
uringthesession,
patientswereencouraged
toaskqu
estio
nsto
individu
alizeinform
ation;
writteninform
ation
abou
tpain
physiology
concepts
were
provided
asho
mew
orkbetweensessions
Clinicianwith
10yearsexperienced
intechniqu
edelivered
triggerp
oint-dryneedling
(TrP-DN)do
neto
activetriggerpo
ints
ingluteusmediusandqu
adratuslumbo
rum;
positio
nwas
side
lying,
with
depthof
needle
insertionapproximately20–25mm
and
moved
inmulti-directions
until
first
local
twitchrespon
sewas
obtained;n
eedling
performed
with
upanddo
wnmovem
ent
5–8mm
with
norotatio
nat
approximately1
Hzfor25–30second
s;treatm
entdo
neon
etim
eperweekover
3weeks
Primaryoutcom
emeasures
●Roland
–Morris
Disability
Questionn
aire
(RMDQ)
●Osw
estryLow
Back
Pain
Disability
Index
(ODI)
●Num
erical
Pain
Rate
Scale(NPRS)
●Tampa
Scaleof
Kinesiop
hobia
(TSK)
●Pressure
pain
threshold(PPT)
Baseline,1weekafterlast
interventio
n
(Con
tinued)
PHYSIOTHERAPY THEORY AND PRACTICE 13
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
Table3.
(Con
tinued).
Participants
Interventio
nsOutcomes
Author
nSample
characteristics
Diagn
ostic
criteria
Treatm
ent
Control
Outcome
instruments
Timeof
assessment
Beltran-Alacreu
etal.
(2015)
45●
Non
-specific
chronicneck
pain
Experim
ent
group1
●n=15
(13
female)
●Ag
e(years):
40.9
±16.2
●Pain
duratio
n(m
onths):5
4.9
±57.1
Experim
ent
group2
●n=15
(10
female)
●Ag
e(years):
39.8
±13.4
●Pain
duratio
n(m
onths):8
3.4
(94.1)
Controlgroup
●n=15
(12
female)
●Ag
e(years):
43.5
±15.9
●Pain
duratio
n(m
onths):9
5.8
±77.5
NA
Experim
entalgroup
1(Exp1)
Eigh
ton
e-on
-one
sessions
over
1mon
th;
sametreatm
entas
controlg
roup
with
additio
nof
pain
neuroscience
educationin
twosessions;n
euroscienceeducationbased
onbiob
ehaviorala
pproachdividedinto
three
parts:cogn
itive,o
perant,and
respon
dent;
neuroscience
educationdu
ratio
nwas
approximately20
minutes
foreach
oftwo
sessions;firstsessionon
initialvisitcoverin
gcogn
itive
part;u
seof
PowerPointwith
diagrams,images,and
textswith
education
alon
gwith
inform
ationbo
okletreview
ing
relevant
contentof
educationfrom
first
session;second
sessionon
fifth
visitreview
ing
first
sessionandop
erantandrespon
dent
parts.Operant
sectionexplainedself-
treatm
enttechniqu
esandcoping
strategies
toredu
ceattentionto
pain.
Experim
entalgroup
2(Exp2)
Received
sameinterventio
nas
Experim
ental
grou
p1with
additio
nof
therapeutic
exercise
prog
ram;exerciseprog
ram
basedon
neck
stabilizatio
nexercisesfordeep
neck
flexors
andextensorsandneuralself-mob
ilizatio
ns;
prog
ressiveexercise
prog
ram
was
addedin
sessions
5–8;
with
integrationof
exercise
treatm
entdu
ringtreatm
entsessionmanual
therapy,tim
ewas
halved;p
atientsaskedto
perform
exerciseson
ceperdayat
home
Eigh
ton
e-on
-one
sessions
over
1mon
th;
manualtherapy
techniqu
eswith
specific
passivemovem
ents
ofcervicalfacetjoints,
glob
almob
ilizatio
nof
cervicalspineandhigh
-velocity
techniqu
eto
dorsalspine
Primaryoutcom
emeasure
●NeckDisability
Index(NDI)
Secondaryoutcom
es●
Tampa
Scaleof
Kinesiop
hobia
(TSK)
●Fear
Avoidance
Beliefs
Questionn
aire
(FAB
Q)
●NeckFlexor
Muscle
Endu
rance
(NFM
E)test
●Visual
Analog
Fatig
ueScale
(VAF
S)
Baseline,4,
8,16
weeks
Pireset
al.(2015)
62●
Chroniclow
back
pain
Educationgroup
●n=30
(20
female)
●Ag
e(years):
50.9
±6.2
Controlgroup
●n=32
(20
female)
●Ag
e(years):
51.0
±6.3
NA
Completed
aquatic
exercisesprog
ram
similar
tocontrolw
ithadditio
nof
pain
neurop
hysiolog
yprog
ram;twogrou
psessions,9
0minutes
each;top
icsaddressed:
acutepain
originin
nervou
ssystem
,transition
from
acuteto
chronicpain,central
sensitizatio
n,role
ofbrainin
pain
perceptio
n,cogn
itive
andbehavioralrespon
sesrelatedto
pain,flare-upmanagem
entandpacing
;metapho
rsandpictures
used
throug
hout
the
session
Six-weekprog
ram
of12
biweeklysessions
ofaquatic
exercise;g
roup
sof
6–9participants
lasting30–50minutes;three
phases:(1)
warm-up;
(2)specificexercises;(3)warm-
down
Primaryoutcom
emeasures
●Visual
Analog
ueScale(VAS
)●
QuebecBack
Pain
Disability
Scale
Secondaryoutcom
es●
Tampa
Scaleof
Kinesiop
hobia
(TSK)
Baseline,6weeks
after
beginn
ingprog
ram
and3
mon
thsfollow-up
*EG,experimentalg
roup
;**CG,con
trol
grou
p.
14 A. LOUW ET AL.
Dow
nloa
ded
by [
Nov
a So
uthe
aste
rn U
nive
rsity
] at
06:
31 3
0 Ju
ne 2
016
● Peripheral sensitization (Gallagher, McAuley, andMoseley, 2013; Ittersum et al., 2014; Louw, Diener,Landers, and Puentedura, 2014; Moseley, 2003c;Van Oosterwijck et al., 2013; Vibe Fersum et al.,2013)
● Central sensitization (Gallagher, McAuley, andMoseley, 2013; Ittersum et al., 2014; Louw,Diener, Landers, and Puentedura, 2014; Moseley,2003c; Moseley, Nicholas, and Hodges, 2004;Pires, Cruz, and Caeiro, 2015; Vibe Fersum et al.,2013)
● Plasticity of the nervous system (Gallagher,McAuley, and Moseley, 2013; Louw, Diener,Landers, and Puentedura, 2014; Moseley, 2003c;Moseley, Nicholas, and Hodges, 2004; VanOosterwijck et al., 2013)
● Psychosocial factors and beliefs contributing topain (Beltran-Alacreu, Lopez-de-Uralde-Villanueva,Fernandez-Carnero, and La Touche, 2015;Gallagher, McAuley, and Moseley, 2013; Pires, Cruz,and Caeiro, 2015; Téllez-García et al., 2014; VibeFersum et al., 2013)
The book Explain Pain by Butler and Moseley (2003)was directly referenced in six of the studies (Meeuset al., 2010; Pires et al., 2015; Ryan, Gray, Newton,and Granat, 2010; Téllez-García et al., 2014; VanOosterwijck et al., 2013).
Professionals performing PNEPhysical therapists have been the delivery professionalof PNE in all of the studies found in this review. In onestudy, utilizing booklets, the lead author was anoccupational therapist, but no direct education (otherthan the book, authored by a physical therapist) wasprovided (Gallagher, McAuley, and Moseley, 2013).
Duration and frequency of PNEThe time and frequency of delivery was varied witha shift toward shorter durations found more com-mon in the more recent studies. Longest duration ofthe documented sessions was 4 hours (Moseley,2003c) in one session, with shortest duration beingaround 30 minutes (Louw, Diener, Landers, andPuentedura, 2014; Meeus et al., 2010; Téllez-Garcíaet al., 2014; Van Oosterwijck et al., 2013). Shortestfrequency was one time educational session(Moseley, Nicholas, and Hodges, 2004; Pires, Cruz,and Caeiro, 2015) with other studies utilizing edu-cation spread out over multiple episodes during thecourse of treatment.
Educational format and toolsThe primary format for delivery of PNE was verbalone-on-one between patient and provider; two studiesutilized group sessions (Moseley, 2003c; Pires, Cruz,and Caeiro, 2015) and one study did not have anyface-to-face contact and only the information from abook that was read by the subjects (Gallagher,McAuley, and Moseley, 2013). The one-on-onesessions were most often described in terms of con-versational, with encouragement for subjects to askquestions, so material could be individualized andnot a straight lecture format. Various teaching aidswere used during the delivery of the education con-sisting of prepared pictures, PowerPoint presentations,drawings, examples, metaphors, and books comple-menting the in person education information.
Adjunct treatment to PNEDifferent study methodologies were used in the studiesunder review. The use of PNE was used in conjunctionwith other active movement-based therapy interventionsin many of the studies. The list of other therapeuticactivities used with PNE consisted of:
● Mobilization and manipulation (Moseley, 2002)● Soft tissue massage (Moseley, 2002)● Muscle and neural mobilization (Beltran-Alacreu,
Lopez-de-Uralde-Villanueva, Fernandez-Carnero,and La Touche, 2015; Moseley, 2002)
● Trunk stabilization (Moseley, 2002, 2003c; Ryan,Gray, Newton, and Granat, 2010)
● Circuit-based aerobic exercise (Ryan, Gray,Newton, and Granat, 2010)
● Movement exercises (Vibe Fersum et al., 2013)● Paced/graded exposure with activities of daily
(Meeus et al., 2010; Vibe Fersum et al., 2013)● Trigger point dry needling (Téllez-García et al., 2014)● Neck stabilization exercises (Beltran-Alacreu,
Lopez-de-Uralde-Villan
Recommended