
Robert O. Bonow, MD, MS
No Relationships to Disclose
Northwestern University Feinberg School of MedicineBluhm Cardiovascular Institute
Northwestern Memorial Hospital
The ACC/AHA Guidelinesfor Management of Aortic Insufficiency:
Pitfalls and Nuances
Robert O. Bonow, MD, MS
No Relationships to Disclose
Northwestern University Feinberg School of MedicineBluhm Cardiovascular Institute
Northwestern Memorial Hospital
The 5 Most ControversialRecommendations for AR Management
in the US and European Guidelines

www.acc.orgwww.americanheart.org
www.esc.org
www.acc.orgwww.americanheart.org
www.esc.org
www.acc.orgwww.americanheart.org

The 5 most controversial recommendations:
• Evidence-based recommendations?
• Surgery for BAV with aortic aneurysms?
• The asymptomatic patient with severe AR?
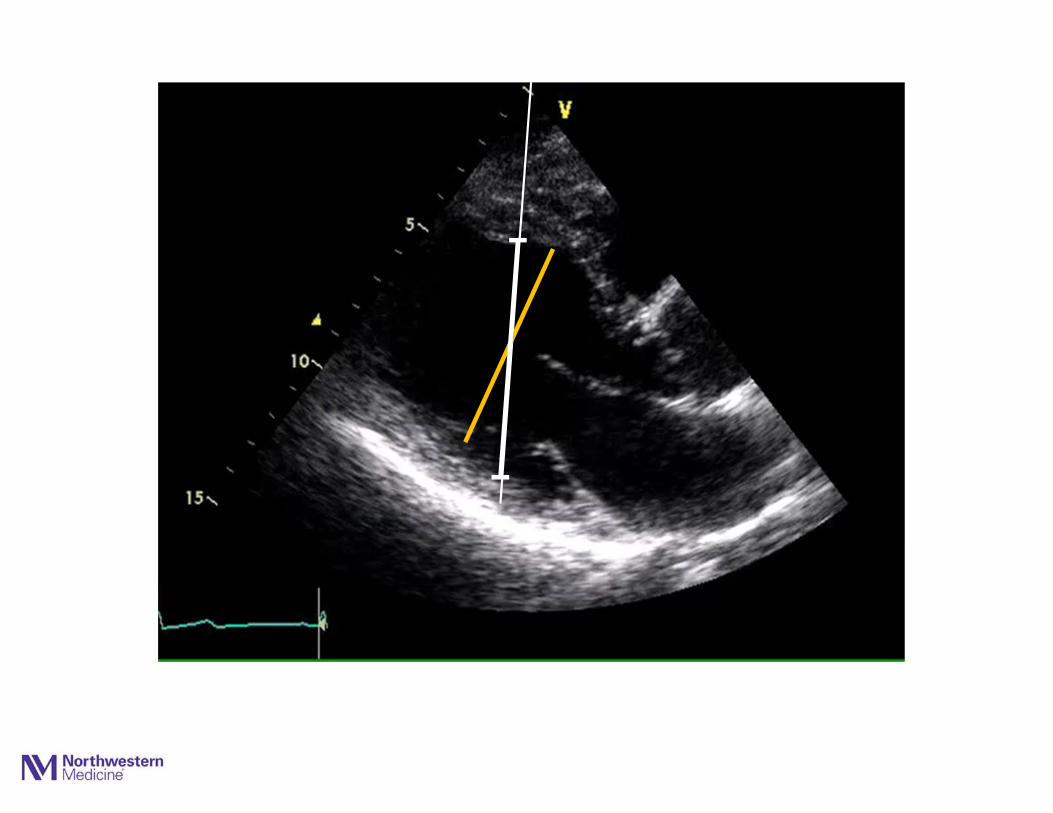
• LV volume assessment: M-mode vs 3D?
• Selection of a valve prosthesis?
Aortic Regurgitation
The 5 most controversial recommendations:
Aortic Regurgitation
• Evidence-based recommendations?
• Surgery for BAV with aortic aneurysms?
• The asymptomatic patient with severe AR?
• LV volume assessment: M-mode vs 3D?
• Selection of a valve prosthesis?
In the absence of randomized clinical trials, virtually all of the recommendations for AR are based on expert consensus
--- Level of Evidence C

The 5 most controversial recommendations:
Aortic Regurgitation
• Evidence-based recommendations?
• Surgery for BAV with aortic aneurysms?
• The asymptomatic patient with severe AR?
• LV volume assessment: M-mode vs 3D?
• Selection of a valve prosthesis?
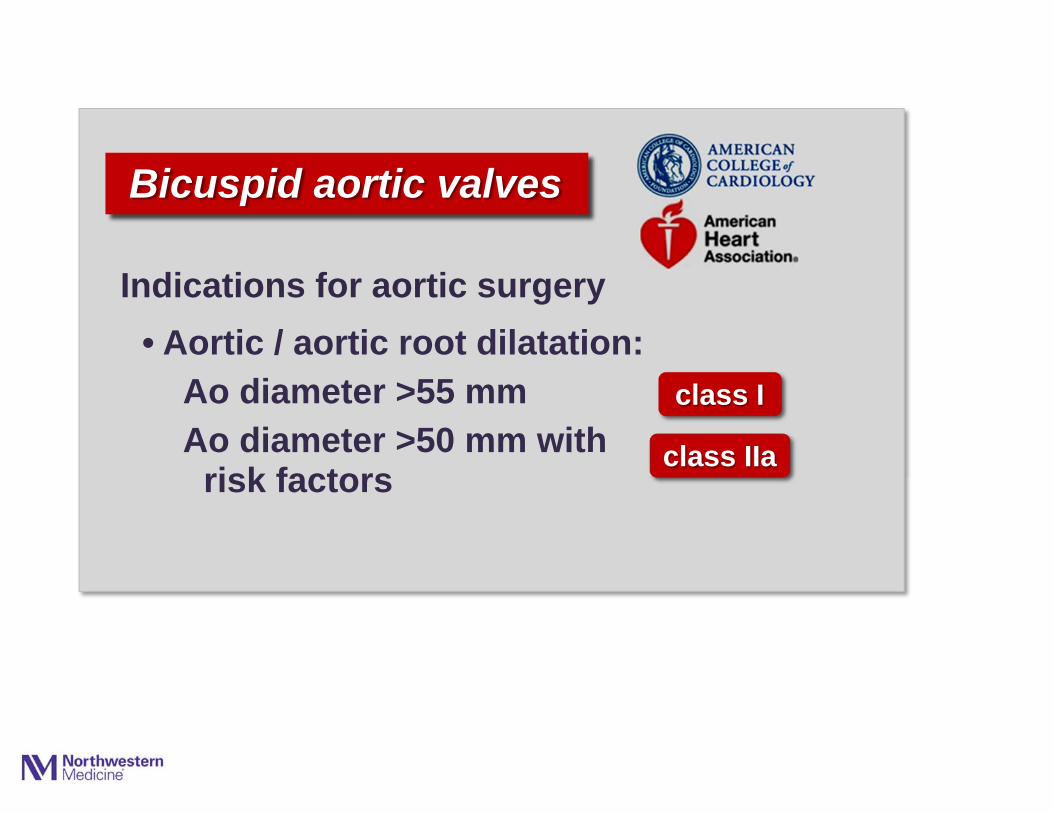
• Aortic / aortic root dilatation:Ao diameter >55 mmAo diameter >50 mm with
risk factors
Bicuspid aortic valves
Indications for aortic surgery
class I
class IIa

• Aortic / aortic root dilatation:Ao diameter >55 mmAo diameter >50 mm with
risk factors
Bicuspid aortic valves
Indications for aortic surgery
class I
class IIa
New 2014
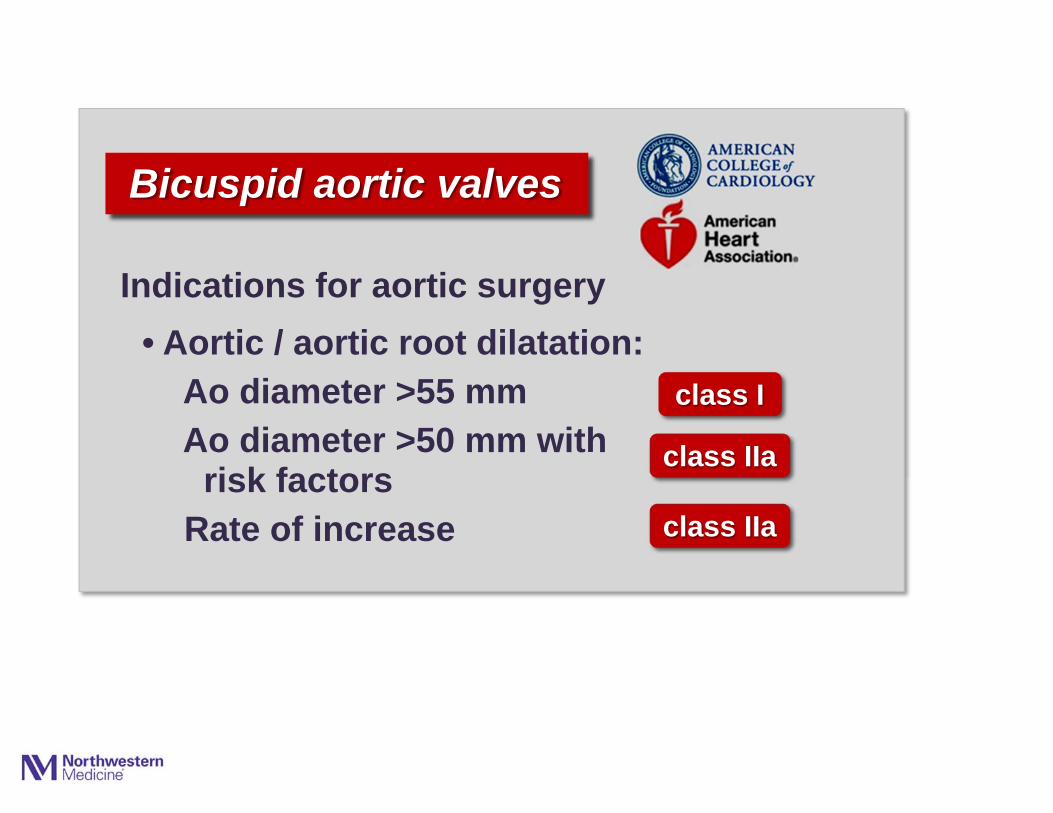
• Aortic / aortic root dilatation:Ao diameter >55 mmAo diameter >50 mm with
risk factors Rate of increase
Bicuspid aortic valves
Indications for aortic surgery
class I
class IIa
class IIa

• Aortic / aortic root dilatation:Ao diameter >55 mmAo diameter >50 mm with
risk factors Rate of increase
• Patients with criteria for AVR:Ao diameter >45 mm
Bicuspid aortic valves
Indications for aortic surgery
class I
class IIa
class IIa
class IIa

• Aortic / aortic root dilatation:Ao diameter >55 mmAo diameter >50 mm with
risk factors Rate of increase
• Patients with criteria for AVR:Ao diameter >45 mm
class IIa
Bicuspid aortic valves
Indications for aortic surgery
class I
class IIaclass IIa
class IIaclass IIa
class IIa class IIa
class IIa
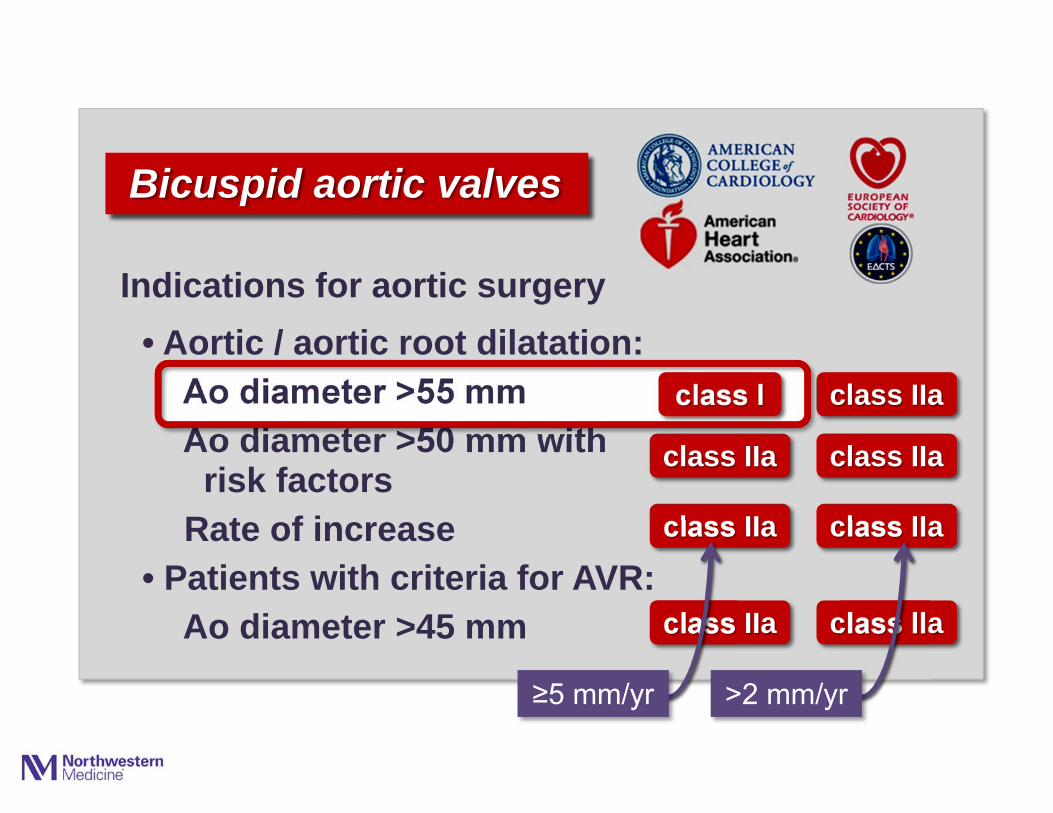
Bicuspid aortic valves
Indications for aortic surgery
class I
class IIaclass IIa
class IIaclass IIa
class IIa class IIa
>2 mm/yr≥5 mm/yr
class I• Aortic / aortic root dilatation:
Ao diameter >55 mmAo diameter >50 mm with
risk factors Rate of increase
• Patients with criteria for AVR:Ao diameter >45 mm
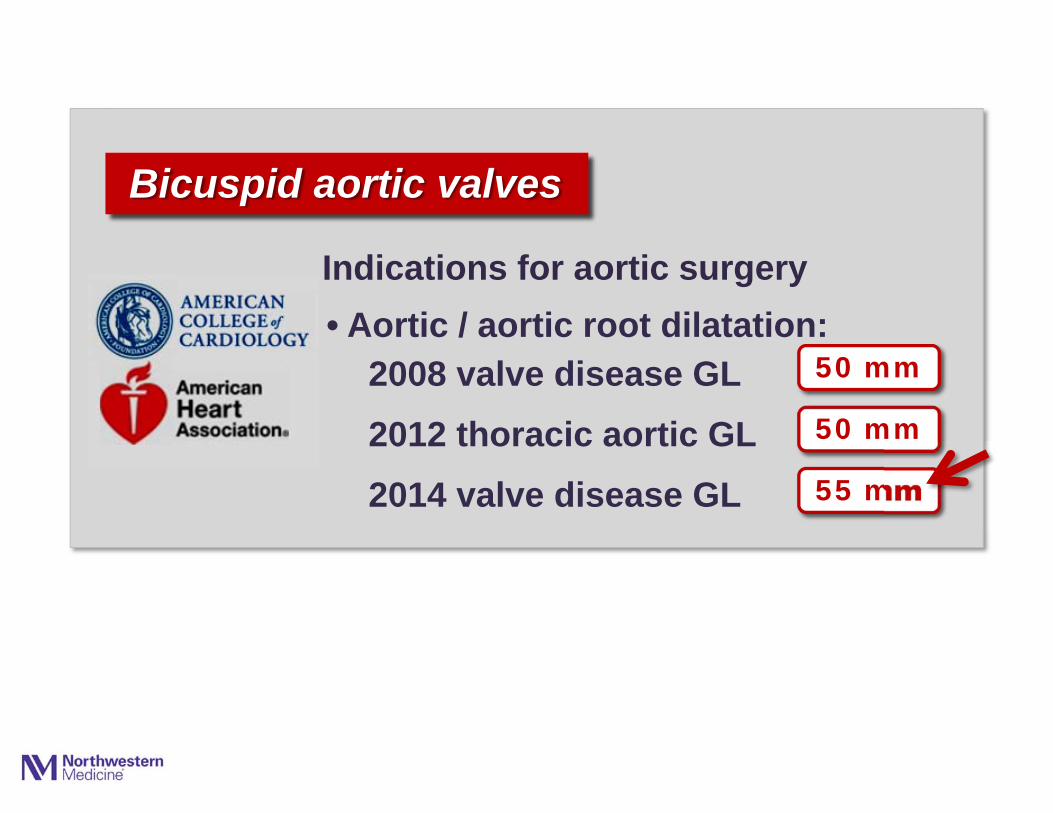
Bicuspid aortic valves
Indications for aortic surgery
50 mm
• Aortic / aortic root dilatation:2008 valve disease GL2012 thoracic aortic GL2014 valve disease GL
50 mm
55 mm
2010 ACCF/AHA/ACR/ASA/SCA/SCAI/STS/SVM Guidelines for theDiagnosis and Management of Patients with Thoracic Aortic Disease
2014 AHA/ACC Guidelines for the Management of Patients with ValvularHeart Disease
www.acc.orgwww.americanheart.org

The 5 most controversial recommendations:
Aortic Regurgitation
• Evidence-based recommendations?
• Surgery for BAV with aortic aneurysms?
• The asymptomatic patient with severe AR?
• LV volume assessment: M-mode vs 3D?
• Selection of a valve prosthesis?
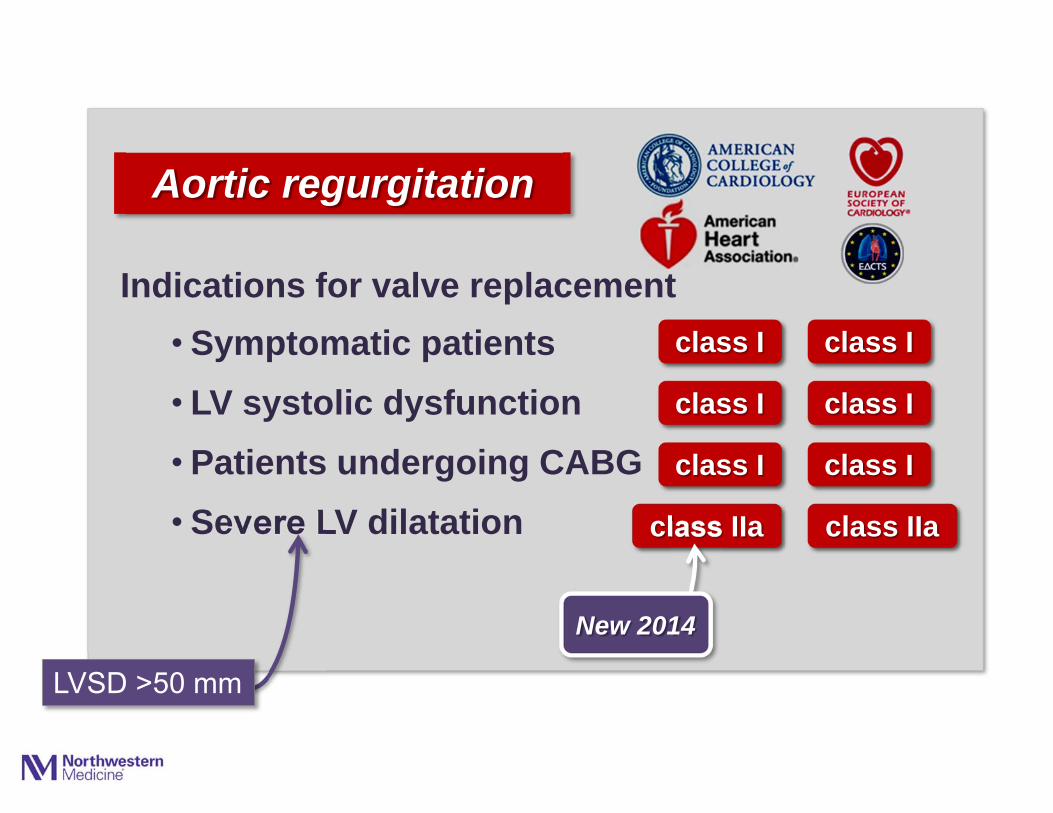
• Symptomatic patients class I
Indications for valve replacement
Aortic regurgitation
class I

• Symptomatic patients• LV systolic dysfunction
class I
class I
Indications for valve replacement
Aortic regurgitation
class I
class I
• Symptomatic patients• LV systolic dysfunction• Patients undergoing CABG
class I
class I
class I
Indications for valve replacement
Aortic regurgitation
class I
class I
class I
• Symptomatic patients• LV systolic dysfunction• Patients undergoing CABG• Severe LV dilatation
class I
class I
class I
Indications for valve replacement
Aortic regurgitation
class IIa
class I
class I
class I
class IIa

• Symptomatic patients• LV systolic dysfunction• Patients undergoing CABG• Severe LV dilatation
LVSD >50 mm
class I
class I
class I
Indications for valve replacement
Aortic regurgitation
class IIa
class I
class I
class I
class IIa
• Symptomatic patients• LV systolic dysfunction• Patients undergoing CABG• Severe LV dilatation
LVSD >50 mm
class I
class I
class I
Indications for valve replacement
Aortic regurgitation
class IIa
class I
class I
class I
class IIa
New 2014
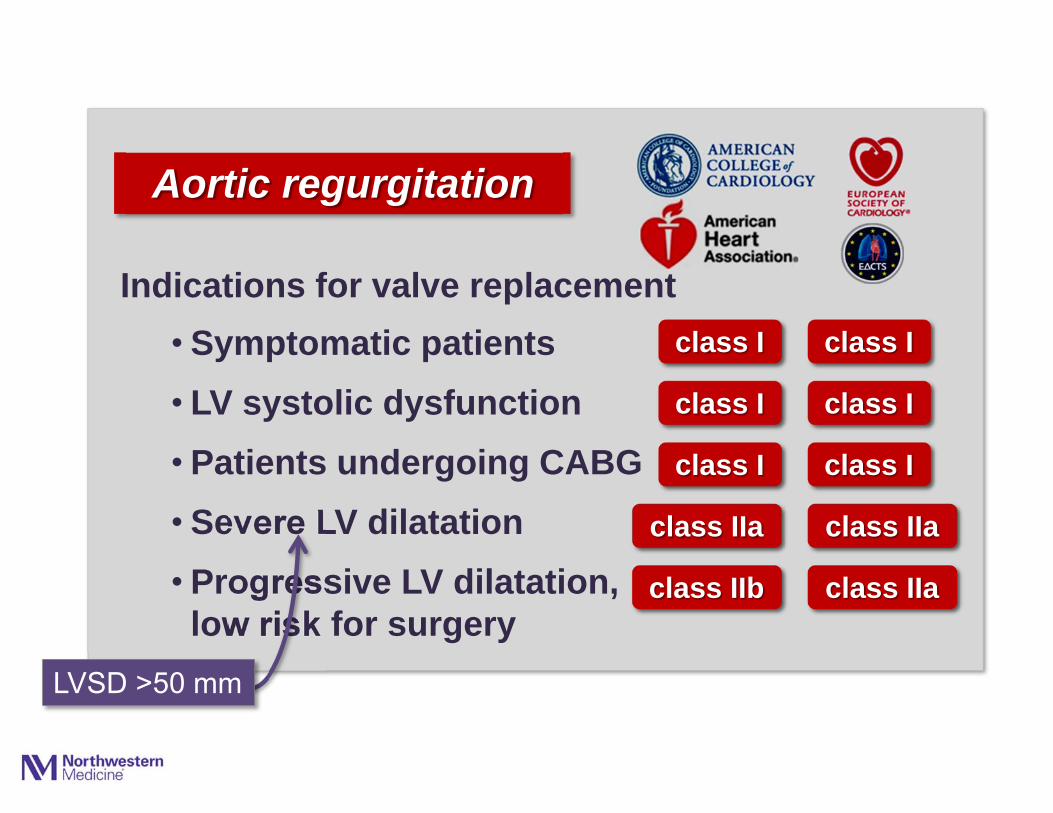
• Symptomatic patients• LV systolic dysfunction• Patients undergoing CABG• Severe LV dilatation • Progressive LV dilatation,
low risk for surgeryLVSD >50 mm
class I
class I
class I
Indications for valve replacement
Aortic regurgitation
class IIa
class IIb
class I
class I
class I
class IIa
class IIa

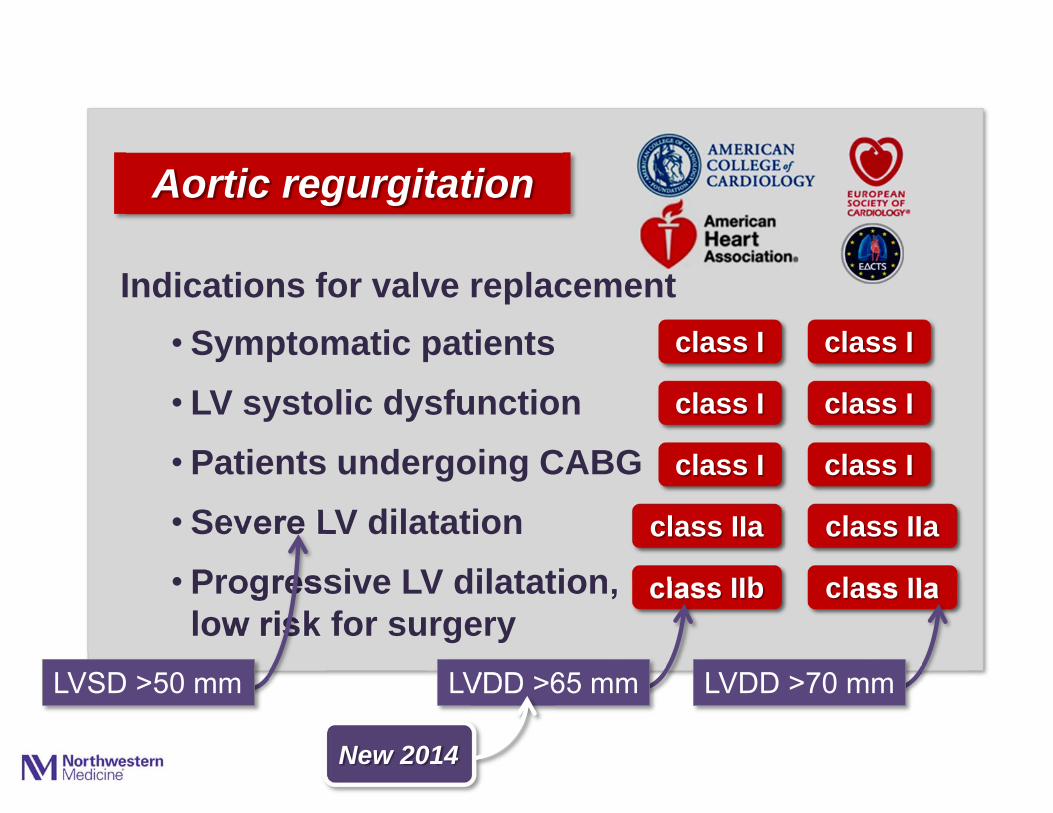
• Symptomatic patients• LV systolic dysfunction• Patients undergoing CABG• Severe LV dilatation • Progressive LV dilatation,
low risk for surgeryLVSD >50 mm
class I
class I
class I
Indications for valve replacement
Aortic regurgitation
class IIa
class IIb
class I
class I
class I
class IIa
class IIa
LVDD >70 mmLVDD >65 mm
• Symptomatic patients• LV systolic dysfunction• Patients undergoing CABG• Severe LV dilatation • Progressive LV dilatation,
low risk for surgeryLVSD >50 mm
class I
class I
class I
Indications for valve replacement
Aortic regurgitation
class IIa
class IIb
class I
class I
class I
class IIa
class IIa
LVDD >70 mmLVDD >65 mm
New 2014


The 5 most controversial recommendations:
Aortic Regurgitation
• Evidence-based recommendations?
• Surgery for BAV with aortic aneurysms?
• The asymptomatic patient with severe AR?
• LV volume assessment: M-mode vs 3D?
• Selection of a valve prosthesis?

Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Data from national Medicare database 1994-1999684 hospitals
142,488 AVRs
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5Time (years)
100
80
60
40
20
00 2 4 6 8 10
Eve
nt-F
ree
Sur
viva
l(p
erce
nt)
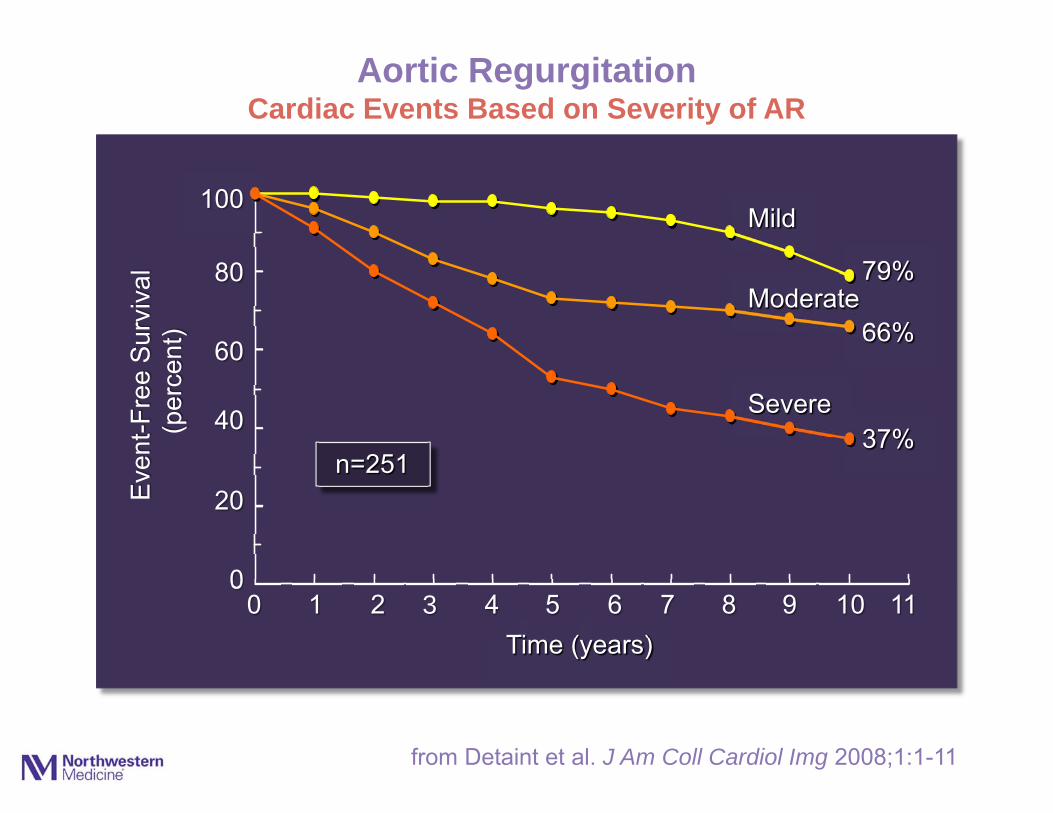
Aortic RegurgitationCardiac Events Based on Severity of AR
1 3 5 7 9 11
66%
37%
from Detaint et al. J Am Coll Cardiol Img 2008;1:1-11
Mild
Moderate
Severe
79%
n=251

Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Data from national Medicare database 1994-1999684 hospitals
142,488 AVRs
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5Time (years)
100
80
60
40
20
00 2 4 6 8 10
Eve
nt-F
ree
Sur
viva
l(p
erce
nt)
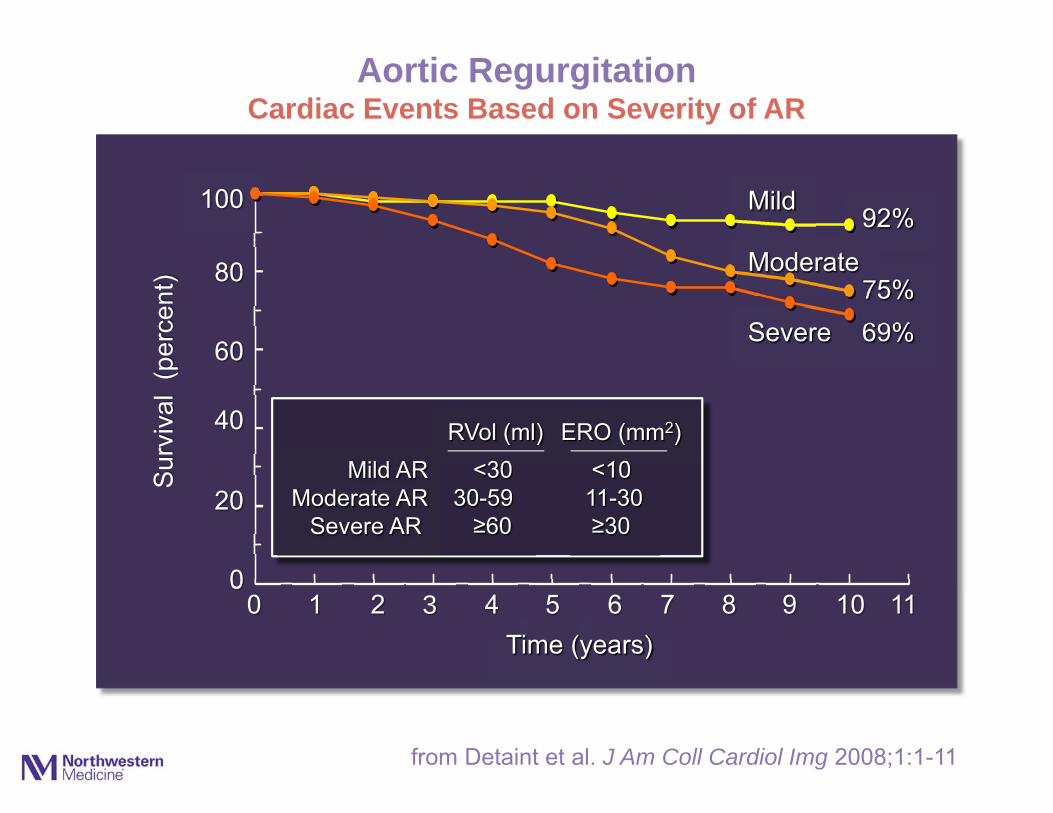
Aortic RegurgitationCardiac Events Based on Severity of AR
1 3 5 7 9 11
66%
79%
37%
Mild
Moderate
Severe
Mild ARModerate AR
Severe AR
<30 <1030-59 11-30≥60 ≥30
RVol (ml) ERO (mm2)
from Detaint et al. J Am Coll Cardiol Img 2008;1:1-11
Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Data from national Medicare database 1994-1999684 hospitals
142,488 AVRs
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5Time (years)
100
80
60
40
20
00 2 4 6 8 10
Sur
viva
l (p
erce
nt)
Aortic RegurgitationCardiac Events Based on Severity of AR
1 3 5 7 9 11
69%75%
92%Mild
Moderate
Severe
Mild ARModerate AR
Severe AR
<30 <1030-59 11-30≥60 ≥30
RVol (ml) ERO (mm2)
from Detaint et al. J Am Coll Cardiol Img 2008;1:1-11

Multivariate analysis:Predictors of cardiac events
BNP OR 6.9 p=0.0001ERO OR 3.4 p=0.001LVESD OR 4.3 p=0.01LVEDD OR 2.1 p=0.09
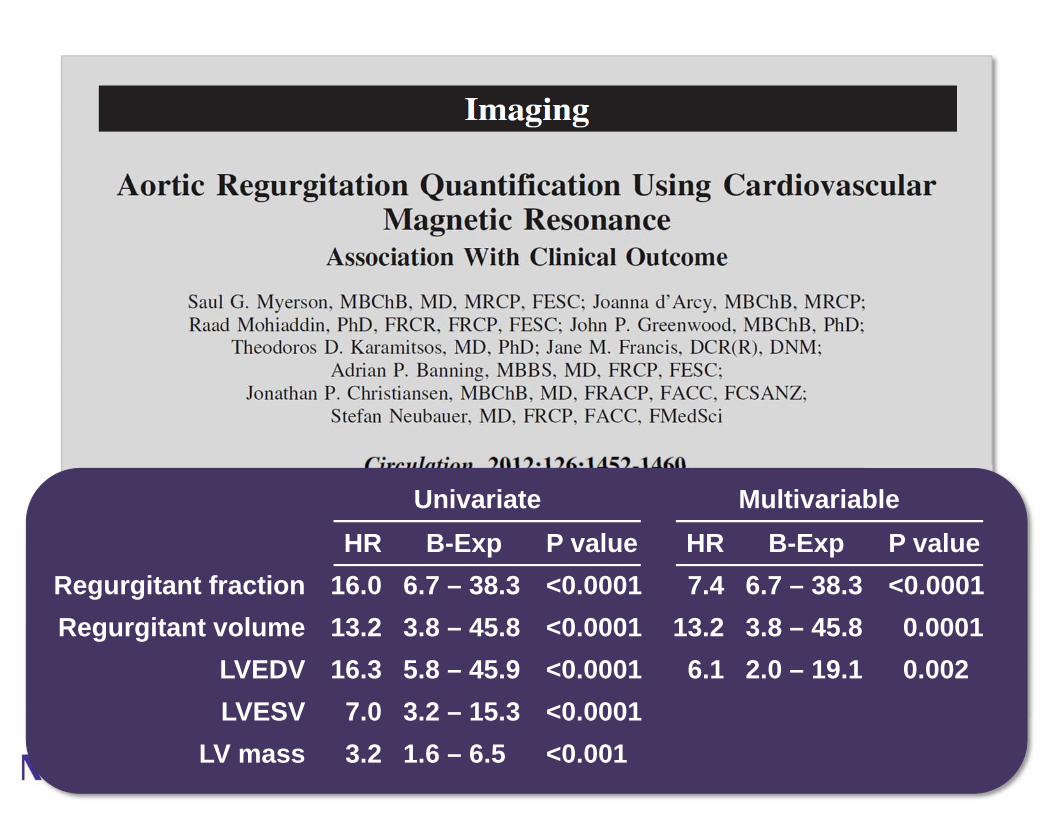
HR B-Exp P value16.0 6.7 – 38.3 <0.000113.2 3.8 – 45.8 <0.000116.3 5.8 – 45.9 <0.0001
7.0 3.2 – 15.3 <0.00013.2 1.6 – 6.5 <0.001
HR B-Exp P value7.4 6.7 – 38.3 <0.0001
13.2 3.8 – 45.8 0.00016.1 2.0 – 19.1 0.002
Regurgitant fractionRegurgitant volume
LVEDVLVESV
LV mass
Univariate Multivariable


Recommended

















