
RESEARCH ARTICLE
Subchondral bone histology and grading in
osteoarthritis
Olli-Matti Aho1*, Mikko Finnila2, Jerome Thevenot2, Simo Saarakkala2,3, Petri Lehenkari1,4
1 Department of Anatomy and Cell Biology, Institute of Biomedicine, University of Oulu, Oulu, Finland,
2 Research Unit of Medical Imaging, Physics and Technology, Faculty of Medicine, University of Oulu, Oulu,
Finland, 3 Department of Diagnostic Radiology, Medical Research Center, Oulu University Hospital, Oulu,
Finland, 4 Division of Orthopaedic and Trauma Surgery, Department of Surgery, Medical Research Center,
Oulu University Hospital, Oulu, Finland
Abstract
Objective
Osteoarthritis (OA) has often regarded as a disease of articular cartilage only. New evidence
has shifted the paradigm towards a system biology approach, where also the surrounding
tissue, especially bone is studied more vigorously. However, the histological features of sub-
chondral bone are only poorly characterized in current histological grading scales of OA.
The aim of this study is to specifically characterize histological changes occurring in sub-
chondral bone at different stages of OA and propose a simple grading system for them.
Design
20 patients undergoing total knee replacement surgery were randomly selected for the
study and series of osteochondral samples were harvested from the tibial plateaus for histo-
logical analysis. Cartilage degeneration was assessed using the standardized OARSI grad-
ing system, while a novel four-stage grading system was developed to illustrate the changes
in subchondral bone. Subchondral bone histology was further quantitatively analyzed by
measuring the thickness of uncalcified and calcified cartilage as well as subchondral bone
plate. Furthermore, internal structure of calcified cartilage-bone interface was characterized
utilizing local binary patterns (LBP) based method.
Results
The histological appearance of subchondral bone changed drastically in correlation with the
OARSI grading of cartilage degeneration. As the cartilage layer thickness decreases the
subchondral plate thickness and disorientation, as measured with LBP, increases. Calcified
cartilage thickness was highest in samples with moderate OA.
Conclusion
The proposed grading system for subchondral bone has significant relationship with the cor-
responding OARSI grading for cartilage. Our results suggest that subchondral bone remod-
eling is a fundamental factor already in early stages of cartilage degeneration.
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 1 / 16
a1111111111
a1111111111
a1111111111
a1111111111
a1111111111
OPENACCESS
Citation: Aho O-M, Finnila M, Thevenot J,
Saarakkala S, Lehenkari P (2017) Subchondral
bone histology and grading in osteoarthritis. PLoS
ONE 12(3): e0173726. https://doi.org/10.1371/
journal.pone.0173726
Editor: Luc Malaval, Universite de Lyon, FRANCE
Received: September 6, 2016
Accepted: February 24, 2017
Published: March 20, 2017
Copyright: © 2017 Aho et al. This is an open
access article distributed under the terms of the
Creative Commons Attribution License, which
permits unrestricted use, distribution, and
reproduction in any medium, provided the original
author and source are credited.
Data Availability Statement: All relevant data are
within the paper and its Supporting Information
files.
Funding: This study was financially supported by
the Academy of Finland (project 127198), and
strategic funding of the University of Oulu (project
24001200). The funders had no role in study
design, data collection and analysis, decision to
publish, or preparation of the manuscript.
Competing interests: The authors have declared
that no competing interests exist.

Introduction
Osteoarthritis (OA) is a progressive joint disorder characterized by the uneven and gradual
degeneration of articular cartilage, joint pain, stiffness and loss of function in the absence of
chronic autoimmune or autoinflammatory mechanisms [1]. It is the most common form of
arthritis and a significant factor in the public health of industrialized countries [2]. In the
United States alone, over 27 million adults are affected by OA and its prelevance is rising all
the time [3]. OA has traditionally been seen primarily as a disorder of the articular cartilage
[4]. However, increasing evidence suggests that OA should be considered a disease of the
whole joint unit and a gradual shift from cartilage-centered view towards a system biology
approach can be seen [1–2, 4–7].
The main methods of OA diagnostics are clinical evaluation by a physician, followed by
radiography, magnetic resonance imaging (MRI), and in selected cases, arthroscopy [8]. Diag-
nosis of OA is still mainly focused on detecting cartilage degeneration and skeletal changes are
acknowledged only at later stages, even in histological assessment. The first widely accepted
and adopted histological OA grading system was the Mankin scoring [9]. It focuses on archi-
tectural changes in articular cartilage and tidemark while also attending to cellular changes
and proteoglycan content of cartilage [9–10]. A more novel, and presumably more consistent
[10–11], Osteoarthritis Research Society International (OARSI) grading system focuses on the
depth of cartilage degeneration and its extent over the whole joint surface [12]. OARSI grading
system also accounts for some subchondral bone changes in the higher grades. Despite its
growing popularity, OARSI grading system is yet to be systematically compared with the
changes in subchondral bone, especially in lower OARSI grades.
Regardless of their omission in common histological evaluation, the changes that occur in
subchondral bone in osteoarthritic joints have been widely recognized in literature [1, 13–15].
In early OA, the mineral apposition rate of subchondral bone and bone remodeling increase
and new remodeling sites arise, which leads to reduced thickness of the subchondral plate
[16]. As degeneration advances, changes in remodeling balance occur in four main processes:
reduced bone turnover, subchondral sclerosis, thickening of calcified cartilage and thinning of
trabeculae [17]. The defining feature of subchondral bone in late-stage OA is clearly increased
bone volume and apparent density [18].
Bobinac et al. [19] previously compared articular cartilage and subchondral bone histomor-
phometry in humans utilizing Mankin score. Using four histomorphometric parameters
(bone volume, trabecular thickness, trabecular number and trabecular separation) they found
significant linear correlations between articular cartilage degeneration and subchondral bone
changes. Bone volume and trabecular thickness were found to increase, whereas trabecular
number and separation decreased. They also suggested the changes of subchondral bone to be
secondary to cartilage damage. To our knowledge, there are no studies in which the subchon-
dral bone histological changes have been directly correlated with OARSI grading system. Fur-
thermore, no literature can be found aiming to incorporate subchondral bone into complete
histological assessment of OA.
We believe that the subchondral bone should not be disregarded in histological grading of
OA. There is indisputable evidence [1, 13–19] that subchondral bone remodeling is an essen-
tial part of OA pathogenesis but much less is known about the causality. Much like current his-
tological cartilage OA grading scales (Mankin, OARSI), a standardized and easily adaptable
scale for subchondral bone would make evaluating and reporting of histological data more
consistent. Furthermore it could help us to link the changes in cartilage and bone for a better
understanding of joint degeneration. Ultimately we believe that the histological features both
of cartilage and bone should be incorporated into one standardized grading scale.
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 2 / 16

In the present study, based on previous literature, we aimed to create a simple proposal of a
histological grading system for changes occurring in subchondral bone during OA. This new
grading system was correlated with the OARSI grading of overlying cartilage. Furthermore,
subchondral bone histological changes were specifically analyzed quantitatively with digital
image analysis software by measuring the thickness of non-calcified and calcified cartilage as
well as subchondral plate. Finally, the internal structure of cartilage-bone interface was ana-
lyzed using the local binary patterns (LBP) based method.
Materials & methods
Selection of patients and sample processing
20 patients (mean age 74.5 years, range 57-88 years) suffering from OA and undergoing uni-
or bilateral total knee arthroplasty in Oulu University Hospital were randomly selected for this
study (Table 1). Tibial plateau surface, which is routinely extracted during the surgery, was col-
lected and frozen to serve as a sample material. Collection of tissue samples for this study was
authorized by the institutional review board of The Northern Ostrobothnia Hospital District
(EETTMK: 191/2001) and a written consent was obtained from each patient in this study.
Each tibial plateau surface was visually graded into three categories in terms of uniformity of
the articular cartilage: 1) most inviolable (intact) cartilage, 2) moderate cartilage degeneration,
and 3) partly or fully exposed subchondral bone. Grading was conducted by an experienced
Table 1. Patient characteristics.
Patient number Age (years) Sex BMI (kg/m2) Rheumatoid arthritis Mean OARSI Score Operated knee
1 57 Female 35.6 - 3.4 Both
2 61 Female 36.1 - 3.7 Left
3 79 Male 27.8 - 4.3 Right
4 87 Female 22.3 - 5.1 Right
5 78 Female 27.6 * 4.2 Left
6 83 Female 26.5 - 4.3 Right
7 78 Female 28.7 - 3.9 Left
8 88 Female 30.2 - 3.8 Right
9 84 Female 25.0 - 4.4 Right
10 76 Female 25.9 - 3.6 Right (medial)
11 84 Female 34.4 - 4.2 Left
12 77 Male 26.0 - 4 Right
13 66 Female 26.2 - 4.1 Right
14 61 Female 33.3 - 4.4 Both
15 75 Female 34.1 - 4.6 Both
16 62 Female 30.2 - 4.7 Left
17 61 Female 33.3 - 4 Both
18 81 Female 34.6 + 3.4 Right
19 70 Male 36.1 - 3.7 Left
20 82 Female 30.4 - 3.6 Right
BMI = Body mass index.
* = patient 5 suffered from spondylarthritis. Only medial tibia of patient 10 was operated.
+ = yes
- = no.
Mean OARSI score from all the samples collected from each patient is presented.
https://doi.org/10.1371/journal.pone.0173726.t001
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 3 / 16
orthopaedist (PL). Using an industrial grade upright drill (TA-FE Drill Press model TFL-16,
Teras Oy, Finland), three adjacent osteochondral sample series, one sample (diameter 6mm)
from each of the three categories of each plateau, were extracted with special care to avoid any
cartilage damage. Two series were used for histology and were formalin fixed, decalcified and
paraffin embedded and finally 5 μm thick sections were stained with Safranin O or hematoxy-
lin and eosin stain. Decalcification was done using 14% EDTA solution for four weeks for par-
affin embedded samples. One series was used for non-decalcified histology. These ’hard tissue’
samples were prepared using ethanol series-dehydrated samples and methacrylate based resin
including dibutyl phthalate, benzoylperoxide in 30˚C for 2 days and at 36˚C for a 5-7 days.
PMMA sections were cut into 5 μm thickness and after PMMA removal with 2-Mehoxyethyl
acetate the sections were stained with Masson Trichrome method.
OARSI grading
Standardized OARSI grading system [12] was used to assess the grade of OA in histological
sections. Three independent researchers (OMA, MF, SS), familiar with OARSI grading,
assessed Safranin O stained samples accordingly.
Subchondral bone grading
Based on previous studies describing the changes in subchondral bone [1, 13–18] and the
rough observations of OA sample material by two researchers (OMA, PL), a simple four-stage
grading system for subchondral bone (Figs 1 and 2) was proposed.
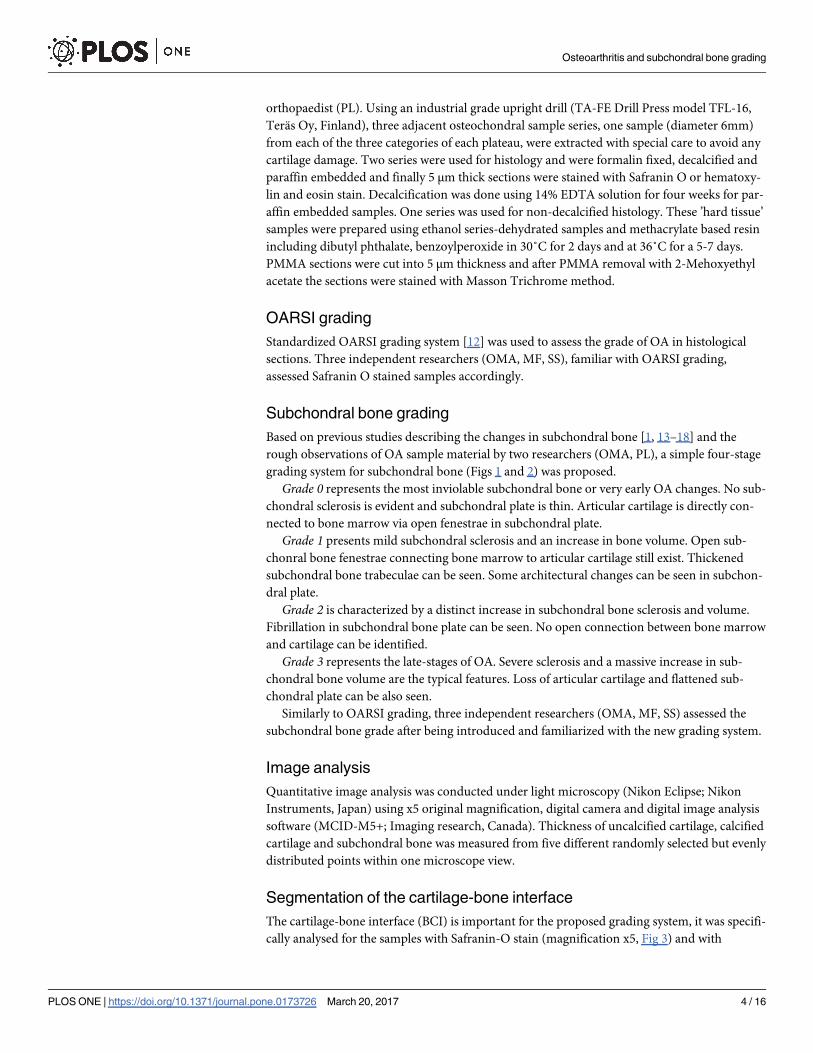
Grade 0 represents the most inviolable subchondral bone or very early OA changes. No sub-
chondral sclerosis is evident and subchondral plate is thin. Articular cartilage is directly con-
nected to bone marrow via open fenestrae in subchondral plate.
Grade 1 presents mild subchondral sclerosis and an increase in bone volume. Open sub-
chonral bone fenestrae connecting bone marrow to articular cartilage still exist. Thickened
subchondral bone trabeculae can be seen. Some architectural changes can be seen in subchon-
dral plate.
Grade 2 is characterized by a distinct increase in subchondral bone sclerosis and volume.
Fibrillation in subchondral bone plate can be seen. No open connection between bone marrow
and cartilage can be identified.
Grade 3 represents the late-stages of OA. Severe sclerosis and a massive increase in sub-
chondral bone volume are the typical features. Loss of articular cartilage and flattened sub-
chondral plate can be also seen.
Similarly to OARSI grading, three independent researchers (OMA, MF, SS) assessed the
subchondral bone grade after being introduced and familiarized with the new grading system.
Image analysis
Quantitative image analysis was conducted under light microscopy (Nikon Eclipse; Nikon
Instruments, Japan) using x5 original magnification, digital camera and digital image analysis
software (MCID-M5+; Imaging research, Canada). Thickness of uncalcified cartilage, calcified
cartilage and subchondral bone was measured from five different randomly selected but evenly
distributed points within one microscope view.
Segmentation of the cartilage-bone interface
The cartilage-bone interface (BCI) is important for the proposed grading system, it was specifi-
cally analysed for the samples with Safranin-O stain (magnification x5, Fig 3) and with
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 4 / 16
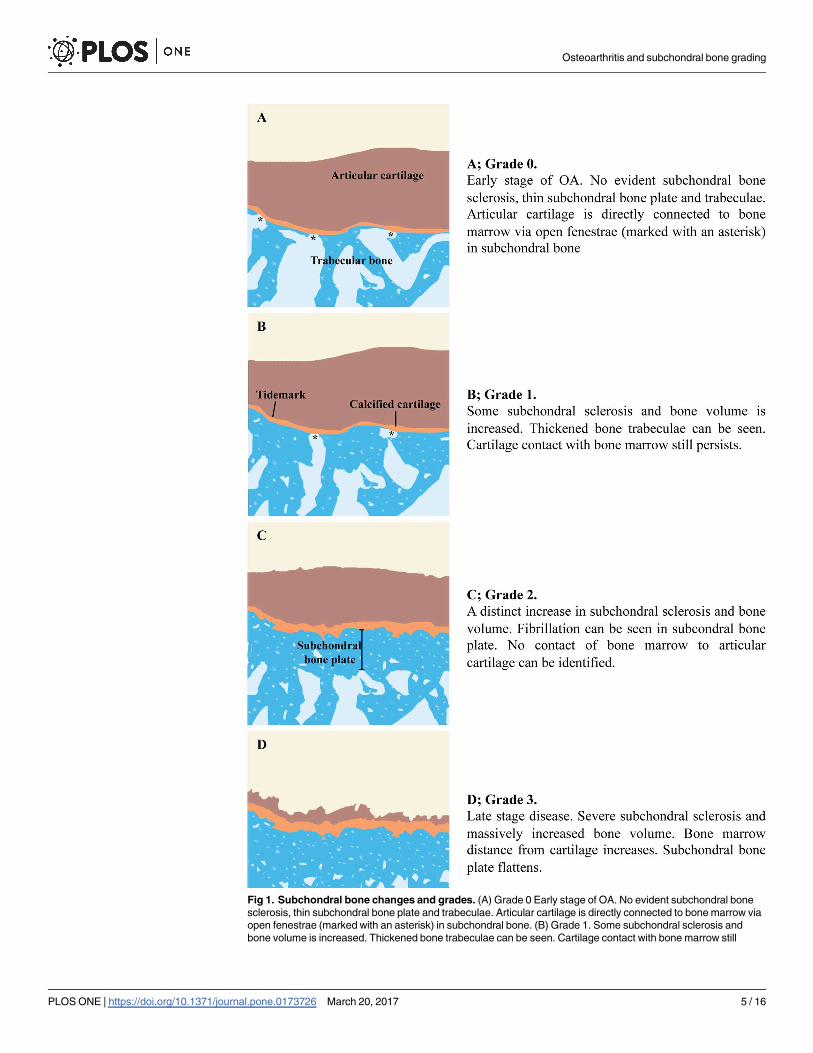
Fig 1. Subchondral bone changes and grades. (A) Grade 0 Early stage of OA. No evident subchondral bone
sclerosis, thin subchondral bone plate and trabeculae. Articular cartilage is directly connected to bone marrow via
open fenestrae (marked with an asterisk) in subchondral bone. (B) Grade 1. Some subchondral sclerosis and
bone volume is increased. Thickened bone trabeculae can be seen. Cartilage contact with bone marrow still
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 5 / 16

remaining cartilage (OARSI<5, N = 18). Shape and structure of BCI was correlated to OARSI
and proposed grading system. For this purpose, the interface was first manually segmented in
each picture to select only the data not affected by artefacts (e.g. cuts in the samples, blurry and
out of focus areas) and containing BCI in the middle of a seven pixels thick layer (Fig 3). Sub-
sequently, a custom-made algorithm developed in MATLAB (version R2014b, MathWorks,
Inc., Natick, MA, USA) was applied to keep solely the pixels within this layer that are either at
the interface itself or at its edges. As a result, the final mask for analysis of the interface was a
thinner layer (�three pixels thick) than the original manually segmented data.
persists. (C) Grade 2. A distinct increase in subchondral sclerosis and bone volume. Fibrillation can be seen in
subcondral bone plate. No contact of bone marrow to articular cartilage can be identified. (D) Grade 3. Late stage
disease. Severe subchondral sclerosis and massively increased bone volume. Bone marrow distance from
cartilage increases. Subchondral bone plate flattens.
https://doi.org/10.1371/journal.pone.0173726.g001
Fig 2. Safranin O (A-D) and Masson’s trichrome stained histological samples of subchondral bone grades. Images taken with a light microscope
using digital camera. White triangle marks articular cartilage, white cross shows calcified cartilage. (A and E) Black asterisks marks fenestrae in subchondral
bone plate connecting the articular cartilage to bone marrow in grade 0 and (B and F) grade 1. (C and G) Fibrillation on subchondral bone plate can be seen in
grade 2. (D and H) Distinctive sclerosis and loss of articular cartilage mark late-stage OA in grade 3. Scale bar 200 μm.
https://doi.org/10.1371/journal.pone.0173726.g002
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 6 / 16
Local binary patterns (LBP) based method to assess local angles
To assess the local angles within the pixels of the BCI, LBP-based method was adapted from
the previous literature [20–21]. Briefly, the neighbours of a central (studied) pixel are evaluated
to assess if some have an equal or higher grey level values than the studied pixel. Based on the
location of these occurrences, a local pattern is derived, providing information on the local ori-
entation of the neighbourhood. Eventually, the result was the distribution of local angles distri-
bution of BCI (Fig 3), describing the internal structure or “fibrillation” of the BCI.
Cartilage-bone interface parameters
For each sample, both the entropy and the homogeneity of the local angles were calculated.
The entropy of local angles describes the randomness of local angles. The homogeneity index
of the angles describes spatial distribution of the elevation angles and provides indication on
its continuity. An angle-level co-occurrence matrix (ALCM) was first calculated with volumet-
ric rotational invariance, to assess the spatial distribution of the elevation angles. Eventually in
this study, a high value of homogeneity of the angles corresponds to an interface made of con-
secutive pixels with similar elevation angles, while a low value suggests the occurrence of sharp
angles along the BCI.
Statistical analysis
Statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS)
version 20.0 (Chicago, Illinois, USA). The intra-observer repeatability and consistency of the
proposed subchondral bone grading system was analyzed by calculating the intra-class correla-
tion coefficient (ICC). One-way ANOVA and Turkey’s post hoc test were used for studying
Fig 3. LBP analysis of the interface bone-cartilage for a sample with early OA. On left an image of a sample with light degeneration (OARSI: 1.0) and a
sample with severe OA on right (OARSI: 4.5). (A) Original image, original magnification x5. (B) Manual segmentation of the interface bone-cartilage and (C)
distribution of local angles at the interface from LBP analysis.
https://doi.org/10.1371/journal.pone.0173726.g003
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 7 / 16

the relationship between OARSI grading and subchondral bone grading, as well as between
subchondral bone grading and image analysis data. As parameters were applicable, indepen-
dent t-test between OA samples grouped by severity assessed from the subchondral bone was
applied to analyse how well the LBP-based parameters are distributed in this grading system.
Linear regression analysis was performed between LBP-based parameters and OARSI grades.
Results
Osteochondral samples from the tibial plateau had a large internal variation in the OARSI
grade depending on the harvesting site. Visually most inviolable graded samples had a mean
OARSI score of 2.1, whereas visual grade 2 and 3 reached mean scores of 4.4 and 5.3, respec-
tively. Overall, the OARSI grades varied from 0.5 to 6 (mean±SD = 4.07±1.31) and subchon-
dral bone grades varied from 0 to 3 (mean±SD = 1.94±0.99). The intra-observer reliability of
subchondral bone grading was excellent ICC = 0.97.
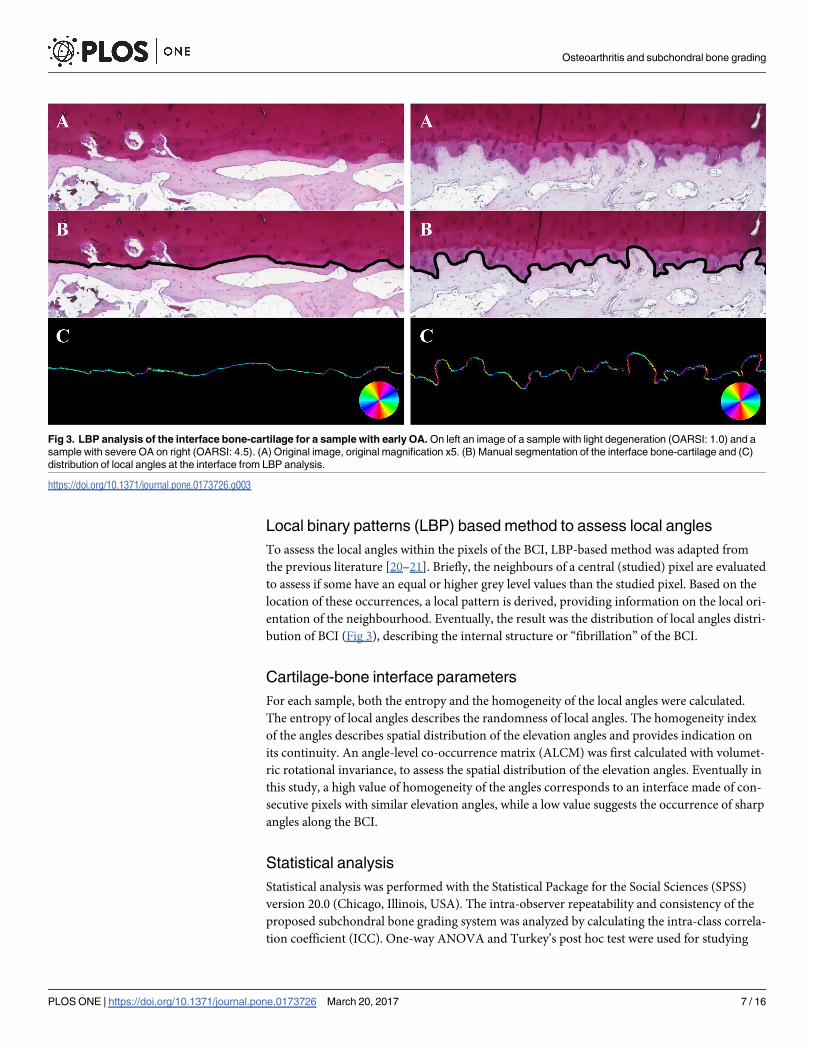
General histological features of subchondral bone
Subchondral bone histology undergoes distinct changes in OA and increasing thickness of
bone plate can clearly be seen. The surface of subchondral plate is also altered as more rugged
and uneven fibrillating surface pattern can be seen in samples with more advanced joint
degeneration. Similarly, trabecular bone structure seems to become disoriented. Late-stage
OA samples typically showed pronounced cartilage erosion accompanied by flattened sub-
chondral plate and massive subchondral sclerosis (Figs 2 and 4).
Subchondral bone grading was in accordance with OARSI grades
Samples with subchondral bone grade 0 had a mean OARSI grade of 1.46, whereas samples
with subchondral grades 1,2 and 3 had mean OARSI grades of 3.45; 3,99 and 5.19, respectively
(Fig 5A).
The thickness of articular cartilage decreases in samples with higher
subchondral bone grade
Samples with subchondral bone grade 0 had the highest cartilage thickness (mean±SD =
2374 μm±506) and lowest calcified cartilage thickness (mean±SD = 84 μm±69). However, no
major differences in cartilage layer was observed in samples between subchondral bone grade
1 (mean±SD = 1753 μm±615) and 2 (mean±SD = 1826 μm±1268). Grade 2 samples had
thicker calcified cartilage layer (mean±SD = 128 μm±50) than grade 1 (mean±SD = 104 μm
±62,44) but the difference was not statistically significant. Subchondral bone grade 3 samples
had already lost most of the cartilage and calcified cartilage layers (mean±SD = 82 μm±142
and 36 μm±46, respectively). (Fig 5B and 5D).
Subchondral plate thickness greatly increases by subchondral bone
grade
Grade 0 samples had the lowest subchondral bone plate thickness (mean±SD = 58 μm±28).
The thickness increased 3-fold already in grade 1 (mean±SD = 176 μm±87), increased up to
8-fold in grade 2 (mean±SD = 473 μm±229) and ultimately to over 21-fold in grade 3 (mean
±SD = 1245 μm±448) (Fig 5C).
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 8 / 16
Fibrillation in cartilage-bone interface increases in moderate joint
degeneration
Cartilage-bone interface plate gets rugged and uneven as OA advances. The LBP-based
method to analyze local angles and ‘bone patterns’ was used to quantify this phenomenon.
Both the homogeneity and entropy of local angles were able to discriminate the different levels
of OA (Fig 6) with statistical significance (p<0.05). Homogeneity of the angles was inversely
correlated with the OARSI grade (R2 = 0.58) while the entropy of angles was positively corre-
lated (R2 = 0.61) (Fig 6).
Fig 4. Masson’s trichrome (A, C-F) and HE stained (B) histological images of the features of subchondral
bone. (A) Subchondral bone fenestra marked with an asterisk. (B) Subchondral trabeculae showing some intra-
trabecular cartilage (triangles), polarized light microscopy. (C-D) Some of the more degenerated samples were
seen with cartilage (triangle) among trabecular bone. (E-F) Late-stage degeneration samples revealing
degenerated and apoptotic cartilage. Scale bar 200 μm.
https://doi.org/10.1371/journal.pone.0173726.g004
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 9 / 16

Discussion
This study focuses on the histomorphometry of subchondral bone in different phases of OA in
humans. Based on existing knowledge and our preliminary observations, we proposed a simple
four-stage evaluation scale for these changes and tested its correlation to different stages of car-
tilage erosion.
Cell proliferation and increased matrix remodeling are regarded as the very first signs of
OA and both responses can be seen in both the articular cartilage and subchondral bone [1].
Articular chondrocytes try to maintain the integrity and homeostasis of the tissue by synthesiz-
ing matrix molecules while they also increase their own destruction with proinflammatory
cytokines and destructive enzymes [1]. In parallel to the changes in cartilage, increased cellular
activity in the underlying bone ultimately leads to subchondral bone sclerosis with thickening
of the cortical plate, extensive remodeling of the trabeculae, and osteophyte formation at the
outer edges of the joint [22]. Changes in the subchondral cortical plate and trabeculae are asso-
ciated with activation of the bone remodeling cycle, most likely as an adaptation to changes in
Fig 5. Mean OARSI scores of subchondral bone grades and histological image analysis data in correlation to samples bone
OA grade. (A) OARSI score increases by subchondral oa grade. Samples with subchondral grade 0 reached mean OARSI score of
1.46. Subchondral OA grades 1, 2 and 3 had mean OARSI scores of 3.45, 3.99 and 5.19 respectively. Each bar and point represents
the mean ± S.E. (B) Mean cartilage thickness. (C) Mean subchondral bone plate thickness. (D) Mean calcified cartilage thickness. Each
bar and point represents the mean ± S.E. * p<0.05, *** p<0.001
https://doi.org/10.1371/journal.pone.0173726.g005
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 10 / 16

the biomechanics of the joint or in an attempt to repair microdamages [4]. High remodeling
in subchondral bone may compromise the biomechanical properties of the tissue [1].
Early OA changes in subcrondral bone are believed to be caused by increased bone remod-
eling and an increase in remodeling sites within the bone, which further lead to reduced thick-
ness of subchondral plate [13, 23]. In the new grading system, grade 0 represents the samples
with most inviolable subchondral bone found in our series of osteoarthritic human tibias.
Grade 0 samples are characterized by a thin subchondral plate and trabeculae and a direct con-
nection to bone marrow. The histology of articular cartilage in grade 0 samples did express
some mild but evident degeneration having a mean OARSI grade of 1.46. Interestingly, grade
0 samples had a lot of variation in calcified cartilage thickness, which shows heterogeneity
among these samples. Thinned subchondral plate and articular cartilage degeneration were
Fig 6. LBP based homogeneity and entropy of subchondral bone in correlation to bone and cartilage OA grade. (A) Homogeneity and (B) entropy
in samples with subchondral bone grade 0-2. Grade 3 samples had smooth and worn surface and were excluded. (N = 2, 9 and 7 for grades 0, 1 and 2
respectively). Linear regression models between (C) homogeneity, (D) entropy and cartilage OARSI grade, r2(C) = 0.583, r(D) = 0.612. * p<0.05, *** p<0.001.
https://doi.org/10.1371/journal.pone.0173726.g006
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 11 / 16

associated previously in two different post-traumatic canine OA models [24]. Also in one
experimental model with rabbits, increased bone remodeling and thinning of the subchondral
plate resulted in increased cartilage damage [25]. Some human studies have also linked
increased bone remodeling to progressive OA [26–28].
Increased bone remodeling ultimately leads to increased subchondral bone volume and
density which are the definitive features of late-stage OA [18]. Previous studies have also
reported both decreased and increased thickness (together with decreased trabecular number
and separation) of bone trabeculae, thickened calcified cartilage and reduced bone turnover
[17, 19]. A clear increase in subchondral plate thickness is well documented [19, 29–30]. In
quantitative analyses on two different human studies, bone mineral density has been reported to
increase up to 15% and bone volume up to 30% in OA [30–31]. The mechanical consequences
of subchondral sclerosis are, however, not entirely clear [16]. One animal study utilizing sheep
with induced subchondral sclerosis (without induced bone remodeling) reported no deteriora-
tion of overlaying cartilage even after five years [32] suggesting that subchondral densification
alone does not inevitably lead to OA. Furthermore, in another study by Cox et al. (2012) noted
that in OA the changes in subchondral bone mineralization occur only beneath the areas of sig-
nificant cartilage destruction [33]. It can be, therefore, suggested that the subchondral sclerosis
by itself is not the key factor in OA but rather the increased remodeling as it also causes struc-
tural and biochemical changes that affect the functionality of subchondral plate.
The proposed subchondral bone grading scale focuses on bone remodeling, and increase
in bone volume is perhaps the most figurative change in higher grades. Subchondral bone
grade 1 samples already have increased subchondral plate thickness to some extent and typi-
cally an increase in bone trabeculae thickness can be seen. Porous subchondral plate is one
fundamental difference from grade 2. Further increase in bone volume and trabecular thick-
ness can be seen in grade 2 and 3 samples, the latter representing late stage disease with mas-
sively increased subchondral plate thickness. As in many previous studies [1, 4, 17, 23, 33–34],
we found a clear correlation between increased bone remodeling and cartilage degeneration.
In addition, measured subchondral bone thickness greatly increased by bone grades. Calcified
cartilage thickened up to grade 2 although there was considerable variation. All of our grade 3
samples showed massive cartilage erosion and some had only pieces of calcified cartilage left.
The middle grades of our scale (i.e. 1 and 2) had the least differences in cartilage degeneration
and average cartilage thickness in grade 2 samples was actually higher than in grade 1 although
also showing considerable variation. It can be speculated whether there is “a point of no re-
turn” in remodeling response balance somewhere between bone grades 1 and 2 from which
onwards the rate of cartilage degeneration increases.
One notable feature of increased subchondral bone remodeling is increased vascularization
[13]. One previous study associated elevated angiogenetic factors in synovial fluid with carti-
lage degeneration [35], and these factors have been shown to increase the synthesis of catabolic
enzymes in chondrycytes [34, 36]. Another interesting feature affecting the structural changes
in OA is endochondral ossification. In various studies it has been shown that during OA,
chondrocytes near the tidemark obtain a hypertrophic phenotype which is typically observed
in the growth plate [37]. Chondrocytes start expressing type X collagen and mineralize while
vascular endothelian growth factor (VEGF) expression is also increased. Furthermore, this
could induce the vascularization observed in OA and be responsible for delivering osteoclast
precursors enabling the resorption of mineralized cartilage, similar to endochondral ossifica-
tion during growth [37]. Endochondral ossification is likely to also affect the architecture of
subcondral bone plate during the pathogenesis of OA. In our image analysis, we found some
clear arcitechtual changes in subchondral bone plate in samples with distinct degeneration but
notable cartilage thickness. In fact, one of the defining features of subcondral bone grade 2 was
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 12 / 16

the increased “fibrillation” in bone surface. In some samples we also witnessed vascular tissue
inside the ‘protrusions’ arising from subchondral plate.
In their bone studies, Hirvasniemi et al. [20] and Thevenot et al. [21] suggested that the
entropy of local bone patterns calculated either from radiographs [20] or μCT data [21], is pro-
portionate to the increase of OA severity. Similarly to their results suggesting that “new” local
bone patterns occur with an increase of OA level, we report here that the cartilage-bone inter-
face has an increase of “new” local angles with OA. Basically, this increase of entropy suggests
that the interface presents more variations in its orientation, going from an almost planar shape
to a fluctuating one. The homogeneity of local angles reported here assesses the continuity of
the interface, providing an index representative of the sharpness of the curves along the sample.
As OA increases, the decrease in homogeneity corresponds to an increase of the interface
roughness. The results obtained from both the entropy and homogeneity of local angles suggest
that the bone-cartilage interface becomes more chaotic with the increase of OA severity.
Our image analysis revealed also something quite unexpected as in some samples cartilage
was found under the subchondral plate. In some cases nodules of hyaline cartilage were found
among bone marrow, while some samples had what it seemed like cartilage inside bone trabec-
ulae. We were not able to find any information on such findings in previous literature and the
origin of these can be only speculated. Previously, it has been shown that in some cases chronic
inflammatory processes can even lead to formation of cartilage among organizing granulation
tissue [37]. In fact, one piece of cartilage we found was surrounded by shreds of tissue that
shared some similarities with organizing fibrous granulation neotissue. It is known that
inflammatory processes have an essential role in the pathogenesis of osteoarthritis and studies
have been published on the topic [38].
Only one previous study has systematically compared the histological cartilage grading
(Mankin score) with subchondral bone histomorphometry [19]. Subchondral bone volume
and trabecular thickness were found to increase in samples with higher level of cartilage degen-
eration whereas trabecular number and separation decreased. The study classified the samples
into three groups or “stages” according to Mankin score each including scores from 0-6, 7-9
and 10-14, respectively. One other study compared joint histology and μCT scans in an experi-
mental rat OA model [39]. The study similarly reported a clear correlation between cartilage
degeneration and bone remodeling. In addition, both of these studies concluded that the
changes in bone histomorphometric parameters are secondary to cartilage degeneration. This
statement is today perhaps somewhat disputed. The grading system we developed did prove
itself to be easy-to-apply in histological analysis and intra-observer reliability was excellent.
Also when compared to cartilage histology, the bone grading scale does seem quite logical and
justifiable it its admittedly robust current form.
The most prominent interfering and limiting factor in our results originates from the
understandable limitation of our study and sample collecting methods. Since our patients were
selected for joint replacement, the sample population obviously presents various grades of os-
teoarthritis, although most commonly only the medial sides of the tibial plateus were affected.
This results in the lack of intact and ‘truly healthy’ cartilage samples. It has been previously
shown that joints with osteoarthritis can have areas of nearly intact and healthy cartilage, and
based of our OARSI grading it was very much the case in our samples, too. However, we found
no data on whether this is the case for subchondral bone.
Conclusions
Osteoarthritis causes many structural and biochemical changes in both the articular cartilage
and subchondral bone. Whereas these changes have been previously well documented the
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 13 / 16

relation between cartilage and bone degeneration can still be discussed. Increased bone
remodeling is however strongly associated with increased cartilage damage. We conclude that
subchondral bone should be taken into account in histological assessment of joint degenera-
tion and a more universal grading scale merging cartilage and bone changes for profound his-
tological analysis is needed.
Supporting information
S1 Dataset. Supporting data spreadsheet.
(XLSX)
Author Contributions
Conceptualization: OMA MF SS PL.
Data curation: OMA MF JT.
Formal analysis: OMA MF JT SS PL.
Funding acquisition: OMA SS PL.
Investigation: OMA MF JT SS PL.
Methodology: OMA MF JT SS PL.
Project administration: OMA PL.
Resources: OMA MF JT SS PL.
Software: OMA MF JT.
Supervision: SS PL.
Validation: OMA MF JT SS PL.
Visualization: OMA JT.
Writing – original draft: OMA.
Writing – review & editing: OMA MF JT SS PL.
References1. Lories RJ and Luyten FP. The bone-cartilage unit in osteoarthritis. Nat Rev Rheumatol. 2011; 7:43–9.
https://doi.org/10.1038/nrrheum.2010.197 PMID: 21135881
2. Sellam J, Herrero-Beaumont G, Berenbaum F. Osteoarthritis: pathogenesis, clinical aspects and diag-
nosis. EULAR compendium on rheumatic diseases. Italy; BMJ Publishing Group LTD. 2009;p444–63.
3. Moskowitz RW. The burden of osteoarthritis: clinical and quality-of-life issues. Am.J.Manag.Care 2009;
15:S223–9. PMID: 19817508
4. Goldring MB, Goldring SR. Articular cartilage and subchondral bone in the pathogenesis of osteoarthri-
tis. Ann N Y Acad Sci. 2010; 1192:230–7. https://doi.org/10.1111/j.1749-6632.2009.05240.x PMID:
20392241
5. Pastoureau PC, Chomel AC, Bonnet J. Evidence of early subchondral bone changes in the meniscecto-
mized guinea pig. A densitometric study using dual-energy X-ray absorptiometry subregional analysis.
OA Cartilage 1999; 7:466–73
6. Day JS, Ding M, van der Linden JC, Hvid I, Sumner DR, Wainans H. A decreased subchondral trabecu-
lar bone tissue elastic modulus is associated with pre-arthritic cartilage damage. J Orthop Res. 2011;
19:914–8.
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 14 / 16
7. Hayami T, Pickarski M, Zhuo Y, Wesolowski GA, Rodan GA, Duong le T. Characterization of articular
cartilage and subchondral bone changes in the rat anterior cruciate ligament transection and meniscec-
tomized models of osteoarthritis. Bone. 2006; 38:234–43. https://doi.org/10.1016/j.bone.2005.08.007
PMID: 16185945
8. Wang SZ, Huang YP, Wang Q, Zheng YP, He YH. Assessment of depth and degeneration depen-
dences of articular cartilage refractive index using optical coherence tomography in vitro. Connect.Tis-
sue Res. 2010; 51:36–47. https://doi.org/10.3109/03008200902890161 PMID: 20067415
9. Mankin HJ, Dorfman H, Lippiello I, Zanrins A. Biochemical and metabolic abnormalities in articular carti-
lage from osteoarthritic human hips. II. Correlation of morphology with biochemical and metabolic data.
J Bone Joint Surg Am. 1971; 53:523–37. PMID: 5580011
10. Custers RJ, Creemers LB, Verbout AJ, van Rijen MH, Dhert WJ, Saris DB. Reliability, reproducibility
and variability of the traditional Histologic/Histochemical Grading System vs the new OARSI Osteoar-
thritis Cartilage Histopathology Assessment System. Osteoarthritis Cartilage. 2007 Nov; 15(11):1241–
8. https://doi.org/10.1016/j.joca.2007.04.017 PMID: 17576080
11. Pearson RG, Kurien T, Shu KS, Scammell BE. Histopathology grading systems for characterisation of
human knee osteoarthritis—reproducibility, variability, reliability, correlation, and validity. Osteoarthritis
Cartilage. 2011 Mar; 19(3):324–31. https://doi.org/10.1016/j.joca.2010.12.005 PMID: 21172446
12. Pritzker KP, Gay S, Jimenez SA, Ostergaard K, Pelletier JP, Revell PA, et al. Osteoarthritis cartilage
histopathology: grading and staging. Osteoarthritis Cartilage 2006; 14:13–29. https://doi.org/10.1016/j.
joca.2005.07.014 PMID: 16242352
13. Burr DB. Anatomy and physiology of the mineralized tissues: role in the pathogenesis of osteoarthrosis.
Osteoarthritis Cartilage. 2004; 12 Suppl A:S20–30.
14. Castaneda S, Roman-Blas JA, Largo R, Herrero-Beaumont G. Subchondral bone as a key target for
osteoarthritis treatment. Biochem Pharmacol. 2012 Feb 1; 83(3):315–23. https://doi.org/10.1016/j.bcp.
2011.09.018 PMID: 21964345
15. Li G, Yin J, Gao J, Cheng TS, Pavlos NJ, Zhang C, et al. Subchondral bone in osteoarthritis: insight into
risk factors and microstructural changes. Arthritis Res Ther. 2013; 15(6):223. https://doi.org/10.1186/
ar4405 PMID: 24321104
16. Burr DB and Gallant MA. Bone remodeling in osteoarthritis. Nat rev rheumatol. 2012; 8:665–73. https://
doi.org/10.1038/nrrheum.2012.130 PMID: 22868925
17. Karsdal MA, Leeming DJ, Dam EB, Henriksen K, Alexandersen P, Pastoureau P, et al. Should sub-
chondral bone turnover be targeted when treating osteoarthritis? OA cartilage. 2008; 16:638–46.
18. Fazzalari N and Parkinson IH. Fractal properties of subchondral cancellous bone in severe osteoarthri-
tis of the hip. J Bone Miner Res. 1997; 12:632–40. https://doi.org/10.1359/jbmr.1997.12.4.632 PMID:
9101375
19. Bobinac D, Spanjol J, Zoricic S, Maric I. Changes in articular cartilage and subchondral bone histomor-
phometry in osteoarthritic knee joints in humans. Bone. 2003 Mar; 32(3):284–90. PMID: 12667556
20. Hirvasniemi J, Thevenot J, Immonen V, Liikavainio T, Pulkkinen P, Jamsa T, et al. Quantification of dif-
ferences in bone texture from plain radiographs in knees with and without osteoarthritis. OA Cartilage.
2014; 22(10):1724–1731.
21. Thevenot J, Chen J, Finnila M, Nieminen M, Lehenkari P, Saarakkala S, et al. Local Binary Patterns to
Evaluate Trabecular Bone Structure from Micro-CT Data: Application to Studies of Human Osteoarthri-
tis. ECCV 2014 Workshops Part II, LNCS 8926. 2015: pp.63–79.
22. Thambyah A and Broom N. On new bone formation in the pre-osteoarthritic joint. OA cartilage. 2009;
17:230–7.
23. Intema F, Hazenwinkel HAW, Gouwens D, Bijlsma JWJ, Weinans H, Lafeber FPJG, et al. In early OA,
thinning of the subchondral plate is directly related to cartilage damage: results from a canine ACLT-
meniscectomy model. OA cartilage. 2010; 18:691–8.
24. Sniekers YH, Intema F, Lafeber FP, van Osch GJ, van Leeuwen JP, Weinans H, et al. A role for sub-
chondral bone changes in the process of osteoarthritis: a micro-CT study of two canine models. BME
Musculoskelet Disord. 2008; 9:20.
25. Bellido M, Lugo L, Roman-Blas JA, Castañeda S, Caeiro JR, Dapia S, et al. Subchondral bone micro-
structural damage by increased remodelling aggravates experimental osteoarthritis preceded by osteo-
porosis. Arth Res Ther. 2010; 12:R152.
26. Dieppe P, Cushnaghan J, Young P, Kirwan J. Prediction of the progression of joint space narrowing in
osteoarthritis of the knee by bone scintigraphy. Ann Rheum Dis. 1993; 52:557–63. PMID: 8215615
27. Mansell JP, Tarlton JF, Bailey AJ. Biochemical evidence for altered subchondral bone collagen metabo-
lism in osteoarthritis of the hip. Br J Rreumatol. 1997; 36:16–9.
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 15 / 16

28. Reichenbach S, Guermazi A, Niu J, Neogi T, Hunter DJ, Roemer FW, et al. Prevalence of bone attrition
on knee radiographs and MRI in a community-based cohort. OA cartilage. 2008; 16:1005–10.
29. Milz S, Putz R. Quantitative morphology of the subchondral plate of the tibial plateau. J Anat. 1994;
185:103–10. PMID: 7559105
30. Noble J, Alexander K. Studies of tibial subchondral bone density and its significance. J Bone Joint Surg
Am. 1985; 67-A:295–302.
31. Arden NK, Griffiths GO, Hart DJ, Doyle DV, Spector TD. The association between osteoarthritis and
osteoporotic fracture: the Chingford study. Br J Rreumatol. 1996; 35:1299–1304.
32. Brown TD, Radin EL, Martin RB, Burr DB. Finite element studies of some juxtarticular stress changes
due to localized subchondral stiffening. J Biomech. 1984; 17:11–24. PMID: 6715384
33. Cox LGE, van Donkelaar CC, van Rietbergen B, Emans PJ, Ito K. Decreased bone tissue mineralization
can partly explain subchondral sclerosis observed in osteoarthritis. Bone. 2012; 50:1152–61. https://
doi.org/10.1016/j.bone.2012.01.024 PMID: 22342798
34. Brown RA and Weiss JB. Neovascularization and its role in the osteoarthritic process. Ann Rheum Dis.
1988; 47:881–5. PMID: 2462856
35. Brown RA, Tomlinson IW, Hill CR, Weiss JB, Phillips P, Kumar S. Relationship of angiogenesis factor in
synovial fluid to various joint diseases. Ann Rheum Dis. 1983; 42:301–7. PMID: 6859962
36. Luyten FR, Lories RJU, Verschueren P, de Vlam K, Westhovens R. Contemporary concepts of inflam-
mation, damage and repair in rheumatic diseases. Best Pract Res Clin Rheumatol. 2006; 5:829–48.
37. Cox LGE, van Donkelaar CC, van Rietbergen B, Emans PJ, Ito K. Alterations to the subchondral bone
architecture during osteoarthritis: bone adaptation vs endochondral bone formation. OA Cartilage.
2013; 21:331–8.
38. Aho O-MA, Lehenkari P, Ristiniemi J, Lehtonen S, Risteli J, Leskela H-V. The mechanism of action of
induced membranes in bone repair. J Bone Joint Surg Am. 2013; 95;597–604. https://doi.org/10.2106/
JBJS.L.00310 PMID: 23553294
39. Bagi CM, Zakur DE, Berryman E, Andresen CJ, Wilkie D. Correlation between μCT imaging, histology
and functional capacity of the osteoarthritic knee in the rat model of osteoarthritis. J Transl Med. 2015;
13:276 https://doi.org/10.1186/s12967-015-0641-7 PMID: 26303725
Osteoarthritis and subchondral bone grading
PLOS ONE | https://doi.org/10.1371/journal.pone.0173726 March 20, 2017 16 / 16
Recommended


![The subchondral bone in articular cartilage repair ... · the subchondral plate as the initiating event in osteoarthritis [13]. While the entire osteochondral unit remains the same](https://img.dokumen.tips/doc/110x75/60f326de55812e0e3d2df913/the-subchondral-bone-in-articular-cartilage-repair-the-subchondral-plate-as.jpg)



![Histology Slides - mediconotes.commediconotes.com/freenotes/basic/histology_laboratory_slides.pdf[Histology] Histology Slides MedicoNotes provides real laboratory Histological slides](https://img.dokumen.tips/doc/110x75/5ae110e87f8b9a5a668e6aa3/histology-slides-histology-histology-slides-mediconotes-provides-real-laboratory.jpg)










