Sleep Apnea and Bariatric Surgery
Richard P. Millman, MDMedical Director
Sleep Disorders Center of Lifespan HospitalsVice Chairman and Professor of MedicineAlpert Medical School of Brown University
Disclosures
• Consultant Johnson and Johnson Development Corporation



LapBand
• Most widely used bariatric surgery world wide
• Received FDA approval in 2002 for US
• Expected weight loss 30 – 40 % of excess body weight in the first year and 50 – 55 % in 5 – 10 years
LapBand
• May be longer term issues with durability
• 15 year data shows some weight regain with 35% excess body weight loss maintained
• Band tightness needs constant monitoring and may need readjustment
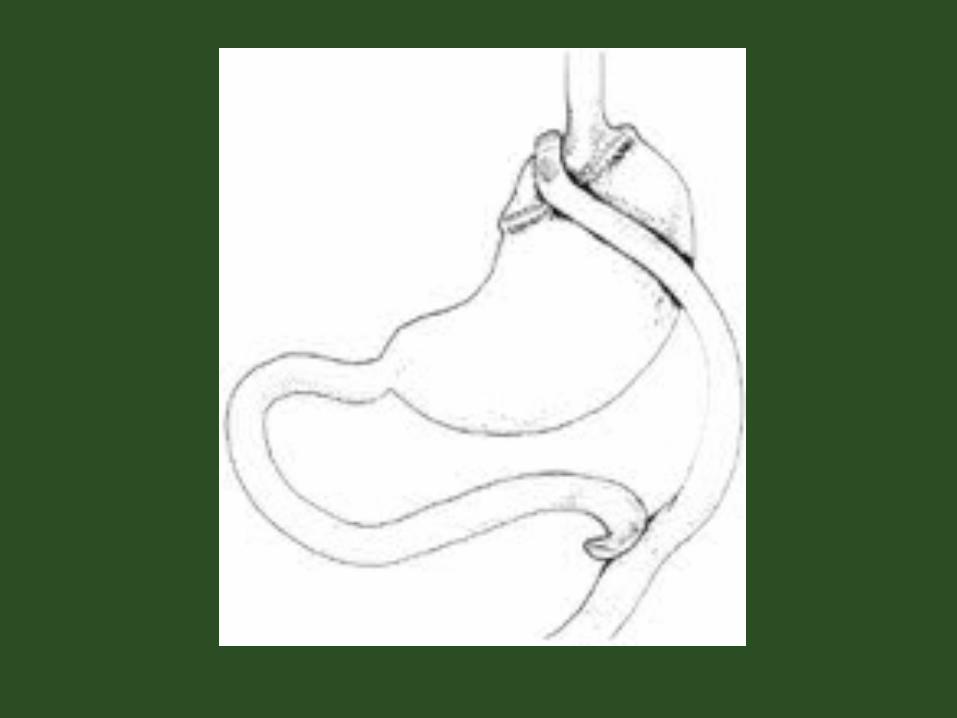

Roux en Y gastric bypass
• Designed after observed weight loss in total gastrectomy patients
• Small proximal pouch
• Duodenum excluded
• 90 to150 cm Roux limb
• Can be done open or laparoscopically
• Excess body weight loss 60% at one year
Selection Criteria
• BMI > 35 with significant comorbidities
• BMI > 40
• Failed conventional weight loss attempts
Selection Criteria
• Psychiatrically stable
• Women should not plan to be pregnant for 2 years
• Able to tolerate anesthesia

Comparative Risk to Medical Management
• Long term studies – patients eligible for surgery who don’t versus those who have surgery
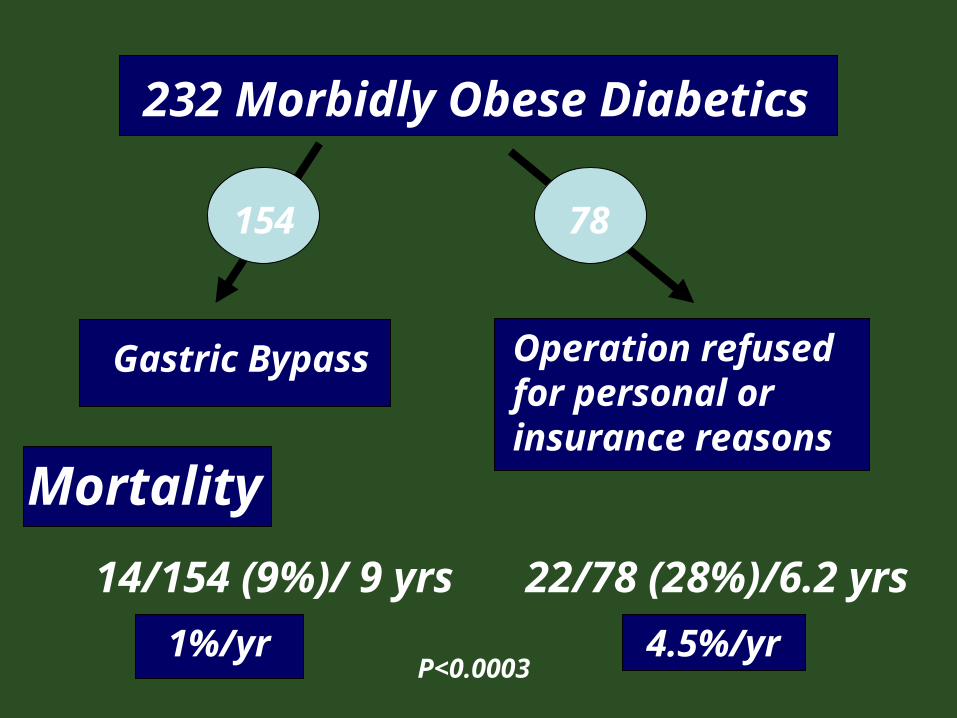
78
232 Morbidly Obese Diabetics
154
Gastric Bypass Operation refused for personal or insurance reasons
22/78 (28%)/6.2 yrs14/154 (9%)/ 9 yrs
P<0.0003
Mortality
1%/yr 4.5%/yr

Nicolas V. Christou MD PhDMc Gill University 2004
n Mortality
Controls 1,035 6.17%
Bariatric Surgery
5,746 0.68%
Reduction of relative risk of death by 89%
Longitudinal Assessment of Bariatric Surgery (LABS)
• NIH/NIDDK Consortium
• Six sites / 5 years
• Short term –operative risk, selection
• Long term – comorbidity control, behavioral issues, economics
• $15,000,000 direct

Comorbidities Raise Operative Risk
• Obstructive sleep apnea
• Diabetic vascular disease
• Reflux with reactive airway disease
• NASH with hepatomegaly

Why is Sleep Apnea an Issue?
Anesthetic agents and narcotics can
• Increase pharyngeal muscle relaxation leading to airway collapse
• Depress respiratory drive

Mary and Bariatric Surgery
• 50 year old woman with known sleep apnea on PAP
• Underwent a Roux en Y procedure • After leaving the PACU was sent to a
regular surgery floor• CPAP was not given since the surgeon
felt that the pressure could blow out the sutures

• The surgeon saw her a couple of hours later and increased the basal rate on her PCA morphine pump because she had 7/10 pain
• Later on she demonstrated increasing confusion but a blood gas was not checked
• She had an arrest and eventually died• The family marched outside the hospital
carrying signs stating “They Killed My Mother”
How could have this been prevented?
• Sending the patient to a stepdown unit with continuous monitoring of heart rate, respiratory rate and pulse oximetry
• Putting the patient on her PAP post operatively
• Avoidance of a continuous infusion of morphine
What if we do not know if they have sleep apnea?
• Sleep apnea is common in obese individuals
• What should we do about patients who haven’t been diagnosed with sleep apnea?
• Sleep studies are expensive and inconvenient. We certainly do not want to perform sleep studies in every patient going for weight loss surgery; do we?

Does this woman have sleep apnea?
Does this one?

Predicting Obstructive Sleep ApneaAmong Women Candidates for Bariatric
Surgery
• 296 consecutive women being evaluated for bariatric surgery who had undergone polysomnography
• Mean age 42 years (age 19-61)• 86% had OSA (AHI = 5 or higher)• 53 % had moderate to severe disease (AHI >
15)
• Sharkey et al JOURNAL OF WOMEN’S HEALTH 2010; 19: 1-9

Results
• Age, BMI, neck circumference, the presence of hypertension, observed apneas during sleep, and snoring all predicted to some degree AHI
• The presence or absence of symptoms of snoring, observed apneas or daytime sleepiness did not correlate with:
1. the absence of OSA2. the presence of any sleep apnea3. the presence of moderate to severe
OSA
Conclusions
• In other words we could not predict who had moderate to severe sleep apnea
• Everybody needed polysomnography
Is there anything special about sleep studies prior to bariatric
surgery?
Yes
• You should make sure you study them on their back!

What about CPAP?
Who needs CPAP and how much?
• You have to decide ahead of time who needs a CPAP titration?
• Should it be an AHI of 5, 15, 30?
• When you do a titration in the sleep center study them on their back to mimic a post-op condition.
Possible Protocol
• Set the patient up on appropriate PAP settings for a month
• See them in followup and assess objectively and subjectively whether they are using PAP
• Make appropriate adjustments in therapy
The Day of Surgery
• Patient should bring PAP device to the hospital (or should bring in settings for a Respiratory Therapy unit)
• After leaving the PACU the patient should go to a stepdown unit with monitoring capabilities
• The patient should be put on PAP
• Continuous basal rates of narcotics should be avoided if possible

Should the patient continue to use PAP at home?
• They definitely should if they had symptoms of OSA prior to the surgery or had severe OSA on polysomnography
• A repeat sleep study should be performed off PAP once stable weight loss has been obtained
• Pressures may need to be decreased as the patient is losing weight
Recommended

















