
Extranodal Extension on Sentinel Lymph Node Dissection: Why Should We Treat It Differently?Audrey Choi MD, Matthew Surrusco MD, Samuel Rodriguez MD, Khaled Bahjri MD, MPH, Naveen Solomon MD, Carlos Garberoglio MD, Sharon Lum MD, Maheswari Senthil MD

Background» Completion axillary lymph node dissection has remained the standard of
care for sentinel lymph node metastasis
» ACOSOG Z0011 trial
~ T1-T2, breast conservation surgery (BCS) with radiation, underwent sentinel lymph node dissection (SLND) with 1-2 positive SLN
~ Randomized to completion axillary lymph node dissection (ALND) or no further surgery
~ 27% of patients in ALND group had additional nodal burden
~ No difference in locoregional recurrence and overall survival at median follow up time (6.3 years)

Background» ACOSOG Z0011 showed
selected patients with limited axillary nodal burden on SLND can avoid added morbidity of ALND
~ Patients with extranodal extension (ENE) on pathology were excluded from the study
» Current standard of care is to proceed with ALND if ENE is found on SLND
~ Significance of ENE identified on SLND is not well defined

Objective
»To determine the impact of ENE detected on sentinel lymph node dissection on:
~ Axillary nodal burden
~ Disease recurrence
~ Overall survival

Design
»Retrospective cross-sectional study, prospectively collected database
»Included patients with breast cancer undergoing SLND at Loma Linda University Medical Center
»2005-2012
»Statistical analysis
~ Adjusted and unadjusted analyses of covariates associated with disease recurrence and overall survival

ResultsAll patients with SLND
2005-2012N=655
No SLN metastasis
N=478 (73.0%)
SLN metastasis without ENE
N=124 (70.1%)
SLN metastasis with ENE
N=53 (29.9%)
SLN metastasispresent
N=177 (27.0%)
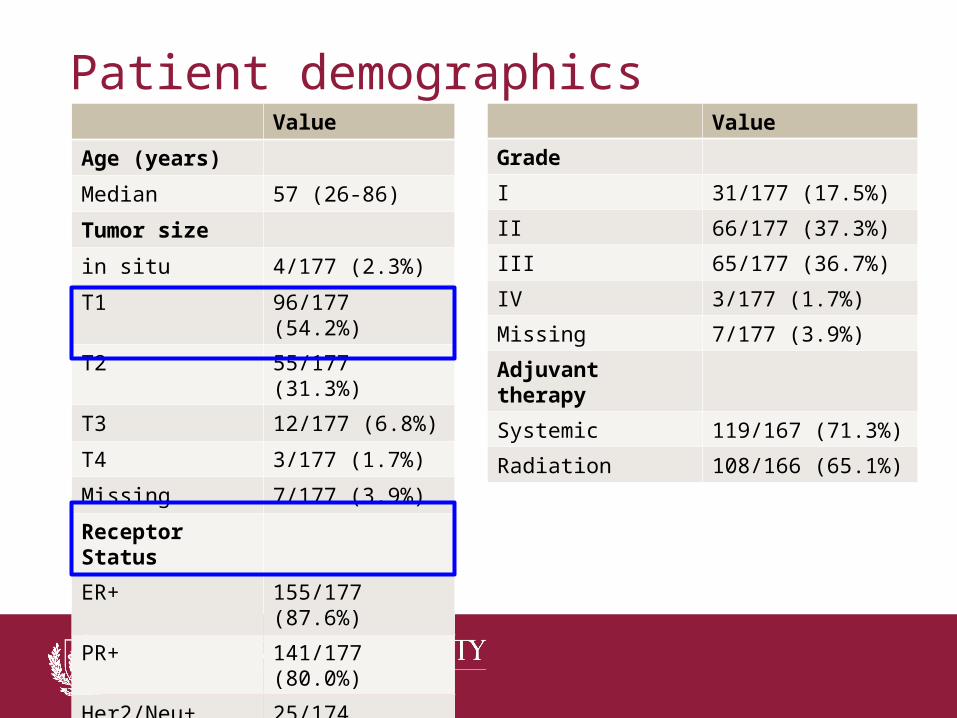
Patient demographicsValue
Age (years)
Median 57 (26-86)
Tumor size
in situ 4/177 (2.3%)
T1 96/177 (54.2%)
T2 55/177 (31.3%)
T3 12/177 (6.8%)
T4 3/177 (1.7%)
Missing 7/177 (3.9%)
Receptor Status
ER+ 155/177 (87.6%)
PR+ 141/177 (80.0%)
Her2/Neu+ 25/174 (14.4%)
Value
Grade
I 31/177 (17.5%)
II 66/177 (37.3%)
III 65/177 (36.7%)
IV 3/177 (1.7%)
Missing 7/177 (3.9%)
Adjuvant therapy
Systemic 119/167 (71.3%)
Radiation 108/166 (65.1%)

Non-SLN metastasis
NSLN metastasis
N=26 (57.8%)
SLN metastasis without ENE
N=124 (70.1%)
SLN metastasis with ENE
N=53 (29.9%)
NSLN metastasis
N=37 (44.0%)
No further diseaseN=47
No ALNDN=40
No further diseaseN=19
No ALNDN=8
ALND
N=84
ALND
N=45
SLN metastasispresentN=177

Increased axillary nodal burden
P = 0.01*

Type of recurrence
+ENE
» ENE associated with increased disease recurrence
-ENE

Disease recurrence
Adjusted analyses of covariates associated with disease recurrence
» 4 times the odds of experiencing disease recurrence if +ENE on SLND» Trend toward significance on adjusted analysis

Overall survival
» Over 7 times the odds for decreased survival if +ENE on SLND
» Statistically significant after controlling for other factors
Adjusted analyses of covariates associated with overall survival

Conclusions» Extranodal extension on sentinel lymph node dissection was associated
with:
~ Increased axillary nodal burden
~ Increased disease recurrence
~ Associated with poor survival outcome
» Extranodal extension on SLND should be considered a poor prognostic factor
» Extranodal extension found on SLND still warrants completion axillary lymph node dissection

Thank you!
Recommended










![Clinical Study Increasing the Efficacy of SLNB in Cases of …downloads.hindawi.com/archive/2014/920349.pdf · 2019-07-31 · SLNB and has nowadays become the standard of care [ ]](https://img.dokumen.tips/doc/110x75/5f02d4567e708231d4063801/clinical-study-increasing-the-efficacy-of-slnb-in-cases-of-2019-07-31-slnb-and.jpg)






