RHEUMATIC FEVERRHEUMATIC FEVER
By Dr Bashir Ahmed DarChinkipora Sopore KashmirAssociate Professor MedicineEmail [email protected]







RHEUMATIC FEVERRHEUMATIC FEVER
Is a post streptococcal infection caused by group A beta hemolytic streptococci.Occurs usually after an attack of phyrangitis
Between age group of 5-15years.Male and female equally affected Can also occur at any age

What are these Streptococci What are these Streptococci
A ‘coccus’ is a spherical bacteria
Staphylococcus tend to cluster in groups
While Streptococcus tend to line up in strings
Some are pyogenic while others are non pyogenic.


Classification of StreptococciClassification of Streptococci
Streptococci are classified according to their hemolytic ability after incubation overnight on blood agar medium.
Beta-hemolytic streptococci produce an enzyme that completely lyses the red blood cells in the medium, leaving a clear zone of hemolysis around the colony. This pattern is best characterized by Streptococcus pyogenes.

Classification of StreptococciClassification of Streptococci
Alpha-hemolytic streptococci produce an enzyme that partially lyses the RBCs and converts red hemoglobin to green methemoglobin leaving a greenish discoloration of the culture medium surrounding the colony. This discolored area contains unlysed red blood cells and a green-colored metabolite of hemoglobin. This pattern is seen with the some Viridans streptococci and Streptococcus pneumoniae.

Classification of StreptococciClassification of Streptococci
Gamma-hemolytic streptococci are unable to hemolyze the RBCs, and therefore we should really not use the word "hemolytic" in this situation. This pattern is seen with most Lancefield group D streptococci.

Common streptococciCommon streptococci
The most common Streptococcus species isolated from humans are as follows
Streptococcus Pyogenes Streptococcus Agalactiae Streptococcus bovis Streptococcus pneumoniae and the Streptococcus Viridans group.

Common streptococciCommon streptococci
1.Streptococcus Pyogenes is a beta hemolytic streptococci and cause bacterial phyrangitis
It also causes Scarlet fever due to the erythrogenic toxin . They are also known as "flesh eating" bacteria and can cause life-threatening disease, necrotising facitis.it also causes Skin infections and Streptococcal toxic shock syndrome.

Pharyngitis Pharyngitis



Scarlet feverScarlet fever


Necrotising fascitisNecrotising fascitis



Skin infectionsSkin infections


Common streptococciCommon streptococci
2.Streptococcus agalacticae is also B beta streptococci. associated with neonates. They are normal flora of the GI tract and vaginal secretions. This bacteria can cause s
neonatal sepsis during birth, neonatal meningitis, postpartum fever, and wound infections, endocarditis, pneumonia, pyelonephritis in the immunosuppressed individuals.

Common streptococciCommon streptococci
Post Streptococcus pyogenes infection also cause non suppurative infection like Rheumatic Fever and Post streptococcal glomerulonephritis

Common streptococciCommon streptococci
3.Streptococcus bovis is a group D Streptococcus, non-Enterococcus. It is usually gamma-hemolytic but may be alpha-hemolytic. They may cause wound infection, urinary tract infection, and abdominal abscesses.

Common streptococciCommon streptococci
4.Streptococcus pneumoniae are gram-positive, lancet shaped diplococci. They are alpha-hemolytic. They are typically normal respiratory flora but may cause lobar pneumonia in the elderly and alcoholics, otitis media in infants and children, meningitis, and community-acquired bacterial pneumonia.

Common streptococciCommon streptococci
5.Streptococcus viridans form large group of commensal streptococcal bacteria that are either α-hemolytic, producing a green coloration on blood agar plates (hence the name "viridans", from Latin "vĭrĭdis", green), or non-hemolytic. They possess no Lancefield antigens.

Common streptococciCommon streptococci
These organisms are most abundant in the mouth and one member of the group, S. mutans, is the etiologic agent of dental caries. Others may be involved in other mouth or gingival infections.
Viridans group are difficult to classify due to changing nomenclature and significant problems of identification by phenotypic analysis.

Lancefield classificationLancefield classification
Based on antigens on streptococcal cell wall
antigens Ag-17 groups (A, B, C….).those that are
not possessing antigens are non groupable e.g.
Viridans streptococci.

Common streptococciCommon streptococci
Streptococcal viridans if introduced into the bloodstream they have the potential of causing endocarditis, particularly in individuals with damaged heart valves. They are the most common causes of subacute bacterial endocarditis especially after dental procedures.

Antigenic Structure
Capsule: . The capsule of group A streptococci is composed of hyaluronic acid (hyloronidase) that breaks down connective tissue and is antiphagocytosis
The group B streptococci contain
M protein
binds IgM, IgG and 2-macroglobulin; interfere with phagocytosis.
Lipoteichoic acid: binds to epithelial cells.
F protein: a major adhesin of S. pyogenes, binding with fibronectin.


Pathogenesis
So streptococci is able to cause
Adherence to the epithelial cells;
invasion into the epithelial cells;
Which in turn is mediated by M protein and F protein and is important for persistent infections and invasion into deep tissues

Enzymes and toxins secreted or produced by S.cocci
Streptokinase (fibrinolysin)
Can lyse blood clots and may be responsible for the rapid spread of the organism.
Used (IV injection) for treatment of pulmonary emboli, coronary artery thrombosis and venous thrombosis.
Streptodornase (DNases A to D)
Decreases viscosity of DNA suspension. A mixture of this and streptokinase is used in enzymatic debridement-liquifies exudates and facilitates removal of pus and necrotic tissue.
C5a peptidase
Prevents streptococci from C5a-mediated recruitment and activation of phagocytes, and is important for survival of S. pyogenes in tissue and blood.

Also produces Hemolysins like
Streptolysin O: O2-labile; causes hemolysis deep in
blood agar plates. ASO (antistreptolysin O) titer >160-200
units suggests recent infection or exaggerated immune
response to an earlier respiratory infection. However, skin
infection does not induce ASO.
Streptolysin S: O2-stable. Causes -hemolysis on the
surface of blood agar plates. Cell-bound, not antigenic. Produced in the presence of serum. Kills phagocytes by releasing the lysosomal contents after engulfment.


pyogenic toxin (erythrogenic) – induces fever and typical red rashsuperantigens – strong monocyte and
lymphocyte stimulants that cause the release of tissue necrotic factor


Epidemiology
.
Crowding increases the opportunity for the pathogen to spread, particularly during the winter months.
the organisms are introduced into the superficial or deep tissue through a break in the skin.
Low social economic conditions are at risk.
Portal of entry through droplets,contact,food,fomites.

How does streptococci cause How does streptococci cause Rheumatic feverRheumatic fever
The streptococci contain antigens as already said , to these antigens antibodies are formed in the body.
But before these antibodies are formed the streptococcal infection is over

How does streptococci cause How does streptococci cause Rheumatic feverRheumatic fever
So these antibodies are searching streptococci but find none there
Instead these antibodies now react to various tissues in the body.
Since most cells of body have same constituents as that of streptococcal cells therefore react with cells of body causing antigen antibody reaction.thus rheumatic fever is immune mediated.

How does streptococci cause How does streptococci cause Rheumatic feverRheumatic fever
These auto immune antibodies produce inflammatory lesions primarily involving the heart, joints, and subcutaneous tissue producing e.g cardiac leisions etc.

Cardiac LesionsCardiac Lesions
Involvement of the interstitial tissue of all the three layers of the heart, the so-called pancarditis takes place in RF.
The characteristic feature of pancarditis in RF is the presence of Aschoff nodules or Aschoff bodies.

The Aschoff nodules or bodiesThe Aschoff nodules or bodies
Are spheroidal or fusiform distinct tiny structures or granulomas, 1-2 mm in size, occurring in the interstitium of the heart in RF and may be visible to naked eye.especially found in the vicinity of small blood vessels in the myocardium and endocardium and occasionally in the pericardium.Lesions similar to the Aschoff nodules may be found in the extracardiac tissues.

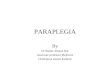
Vegetation
Mitral Valve
Stick in Perforation

Acute Rheumatic vegetations: Acute Rheumatic vegetations: Mitral v.Mitral v.
ValveValve
VegetationsVegetations
Papillary musclePapillary muscle

How are Aschoff bodies How are Aschoff bodies formedformed
Formed in 3 stages. 1. Early (Exudative or degenerative) stage. Initially, there is oedema of the connective tissue
and increase in acid mucopolysaccharide in the ground substance.This results in separation of the collagen fibres by accumulating ground substance.Eventually, the collagen fibres are fragmented and disintegrated,that takes the stain of a fibrin.hence called fibrinoid degeneration.

How are Aschoff bodies How are Aschoff bodies formedformed
2. 2nd stage (Proliferative or granulomatous)This includes infiltration by lymphocytes
(mostly T cells),plasma cells, a few neutrophils and the characteristic cardiac
histiocytes (Anitschkow cells) at the margin of the lesion.

Acute RF: Aschoff bodyAcute RF: Aschoff body
Aschoff body: – Fibrinoid degeneration– T lymphocytes– Plasma cells– Macrophages
Anitschkow cells Aschoff giant cells
– Around blood vessel.

Aschoff body in Acute RFAschoff body in Acute RF Anitschkow cells Capillary T lymphocyte Myocyte

Aschoff body in Acute RFAschoff body in Acute RF Fibrinoid necrosis Aschoff giant cells. Cardiac Muscle
fibres.

Cardiac histiocytes or Cardiac histiocytes or Anitschkow cells Anitschkow cells
Are present in small numbers in normal heart but their number is increased in the Aschoff bodies; therefore they are not characteristic of RHD.

Cardiac histiocytes or Cardiac histiocytes or Anitschkow cellsAnitschkow cells
These are large mononuclear cells having central round nuclei and contain moderate amount of amphophilic cytoplasm. The nuclei are vesicular and contain prominent central chromatin mass which is longitudinal section appears serrated or caterpillar-like, while in cross-section the chromatin mass appears as a small rounded body in the centre of the vesicular nucleus, just like an owl's eye.

Cardiac histiocytes or Cardiac histiocytes or Anitschkow cellsAnitschkow cells
Some of these modified cardiac histiocytes become multinucleate cells containing 1 to 4 nuclei and are called Aschoff cells and are characteristic of RHD.

Aschoff Body & Anitskow cellAschoff Body & Anitskow cell
Aschoff Body
Aschoff Body

Aschoff Giant Cells:Aschoff Giant Cells:

Acute Rheumatic Fever-Rh Acute Rheumatic Fever-Rh nodulenodule

How are Aschoff bodies How are Aschoff bodies formedformed
3. 3rd stage Late (healing or fibrous) stage.This stage is healing by fibrosis of the
Aschoff nodule and occurs in about 12 to 16 weeks after the illness resulting in fibrous scar.

Rheumatic ValvulitisRheumatic Valvulitis
The valves in acute RF show thickening and loss of translucency of the valve leaflets or cusps. This is followed by the formation of characteristic, small (1 to 3 mm in diameter), multiple,warty vegetations or verrucae, chiefly along the line of closure of the leaflets and cusps. These tiny vegetations are almost continuous so that the free margin of the cusps or leaflets appear as a rough and irregular ridge.

Acute Rheumatic vegetations: Acute Rheumatic vegetations: Mitral v.Mitral v.
ValveValve
VegetationsVegetations
Papillary musclePapillary muscle

Fish mouth stenosis:Fish mouth stenosis:

Rheumatic ValvulitisRheumatic Valvulitis
The vegetations in RF appear grey-brown, transuuent and are firmly attached so that they are not likely to get detached to form emboli, unlike the friable vegetations of infective endocarditis.

Chronic RHD:Chronic RHD:
Valve leaflet thickening.
Shortening, thickening and fusion of chordae tendineae.

Acute on Chronic RHDAcute on Chronic RHD
Note: Thickening of valve, opaque, inflammed, irregular border, shortening of chordae tendinae also seen.

Chronic RHDChronic RHD
Note: Thickening of valve, opaque, vascularized irregular border, shortening of chordae tendinae. (no significant inflammation)

Rheumatic ValvulitisRheumatic Valvulitis
Through all the four heart valves are affected, their frequency and severity of involvement varies: mitral valve alone being most common site, followed in decreasing order of frequency, by combined mitral and aortic valve. The tricuspid and pulmonary valves usually show infrequent and slight involvement.

Rheumatic ValvulitisRheumatic Valvulitis
The higher incidence of vegetations onleft side of heart is possibly because of the
greater mechanical stresses on the valves of the left heart, especially along the line of closure of the valve cusps.

Rheumatic ValvulitisRheumatic Valvulitis
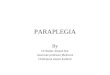
Due to vegetations and thickening the mitral valve may look like 'fish mouth' or 'button hole'. Mitral stenosis and insufficiency are commonly combined in chronic RHD. Calcific aortic stenosis may also be found.

Fish mouth Mitral stenosisFish mouth Mitral stenosis
Scar nodule
Left Atrium
Mitral Valve

Chronic RHD - Aortic ValveChronic RHD - Aortic Valve
Stenotic, Fused valve
Stenotic, Fused valve
Coronary Artery (normal)
Coronary Artery (normal)

Fish mouth Mitral stenosis:Fish mouth Mitral stenosis:

Rheumatic ValvulitisRheumatic Valvulitis
Thickening, shortening and fusion of the chordae tendineae further contribute to the chronic valvular lesions.

Rheumatic ValvulitisRheumatic Valvulitis
Vegetations present at the free margins of cusps appear as tiny structures mainly consisting of fibrin with superimposed platelet thrombi and do not contain bacteria.

Rheumatic ValvulitisRheumatic Valvulitis
In the healed (chronic) stage, the vegetations have undergone organization and fibrous formation., and often calcification. Vascularisation of the valve cusps may still be evident in the form of thick-walled blood vessels.Aschoff bodies are rarely seen in the valves at this stage.

Infective endocarditis with perforation of mitral valve leaflet
Vegetation
Mitral Valve
Stick in Perforation

Rheumatic Mural EndocarditisRheumatic Mural Endocarditis
Mural endocardium may also show features of rheumatic carditis though the changes are
less conspicuous as compared to valvular changes.

Rheumatic Mural EndocarditisRheumatic Mural Endocarditis
Grossly, the lesions most commonly seen is MacCallum's patch which is region of endocardial surface in the posterior wall of the left atrium just above the posterior leaflet of the mitral valve. MacCallum's patch appears as a map-like area
of thickened, roughened and wrinkled part of the endocardium.

Rheumatic Mural EndocarditisRheumatic Mural Endocarditis
Microscopically, the appearance of MacCallum's patch is similar to that seen in rheumatic valvulitis. The affected area shows oedema, fibrinoid change in the collagen, and cellular infiltrate of lymphocytes, plasma cells and macrophages with many Anitschkow cells.

Rheumatic MyocarditisRheumatic Myocarditis
Grossly in early (acute) stage, the myocardium, especially of the left ventricle, is soft and flabby.In the intermediate stage, the interstitial tissue of the myocardium shows small foci of necrosis. Later, tiny pale foci of the Aschoff bodies may be visible throughout the myocardium.
Microscopically, the most characteristic feature of rheumatic myocarditis is the presence of distinctive Aschoff bodies..

Rheumatic MyocarditisRheumatic Myocarditis
These nodules are scattered throughout the interstitial tissue of the myocardium and are most frequent in the interventricular septum, left ventricle and left atrium.

Rheumatic pericarditis.Rheumatic pericarditis.
Grossly, the usual findings is fibrinous pericarditis in which there is loss of normal shiny pericardial surface due to deposition of fibrin on its surface and accumulation of exudate in the pericardial sac. If the parietal pericardium is pulled off from the visceral pericardium, the two separated surfaces are shaggy due to thick fibrin covering them.

Rheumatic pericarditisRheumatic pericarditis
This appearance is often likened to 'bread and butter appearance' i.e. resembling the buttered surfaces of two slices in a sandwich when they are gently pulled apart.If fibrinous pericarditis fails to resolve and, instead,undergoes organization, the two layers of the pericardium form fibrous adhesions resulting in chronic adhesive pericarditis.

Granular Visceral Pericardial Surface of Fibrinous Pericarditis

Fibrinous Pericarditis:Fibrinous Pericarditis:

Extracardiac LesionExtracardiac Lesion
Develop in joint, subcutaneous tissue, arteries, brain and lungs.
Polyarthritis acute and painful inflammation of the synovial membranes of some of the joints,
especially the larger joints of the limbs, is seen in about 90% cases of RF in adults and less often in children. As pain and swelling subside in one joint, others tend to get involved, producing
the characteristic 'migratory polyarthritis' involving two or more joints at a time.

Migratory arthritis Migratory arthritis






Subcutaneous nodulesSubcutaneous nodules
The subcutaneous nodules of RF occur more often in children than in adult. These nodules are
small (0.5 to 2 cm in diameter), spherical or ovoid and painless. They are attached to deeper structures like tendons,ligaments, fascia or periosteum and therefore often remain
unnoticed by the patient. Characteristic locations are extensor surface of the wrists, elbows, ankles and knees.

Subcutaneous nodulesSubcutaneous nodules




Subcutaneous nodulesSubcutaneous nodules
Subcutaneous nodules of RF are larger, painful and tender and persist for months to years than that of rheumatoid arthritis that are painless and non-tender.


Erythema marginatumErythema marginatum
This non-pruritic erythematous rash is characteristic of RF. The lesions occur mainly on the trunk and proximal parts
of the extremities. The erythematous area develops central clearing and has slightly elevated red margins.The erythema is transient and migratory.





Acute Rh Fever: Erythema Acute Rh Fever: Erythema MarginatumMarginatum

Rheumatic ArteritisRheumatic Arteritis
Arteritis in RF involves not only the coronary arteries and aorta but also occurs in arteries of various other organs such as renal,mesenteric and cerebral arteries. The lesions in the coronaries are seen mainly in the small intramyocardial branches.

Chorea MinorChorea Minor
Chorea minor or Sydenham's chorea or Saint Vitus' dance is a delayed manifestation of RF as a result of involvement of the central nervous system. The condition is characterized by disordered and involuntary jerky movements of
the trunk and extremities accompanied by some degree of emotional instability. The condition occurs more often in younger age, particularly in girls.

Chorea MinorChorea Minor
Histologically, the lesions are located in the cerebral hemispheres,brainstem and the basal ganglia. They consist of small haemorrhages, oedema and perivascular infiltration of lymphocytes. There may be endarteritis obliterans and thrombosis of cortical and meningeal vessels.

Rheumatic pneumonitis and Rheumatic pneumonitis and pleuritispleuritis
Involvement of the lungs and pleura occurs rarely in RF. Pleuritis is often accompanied
with serofibrinous pleural effusion but definite Aschoff bodies are not present. In rheumatic pneumonitis, the lungs are large, firm and rubbery.

Diagnosis of RFDiagnosis of RF
The following set of guidelines called revised Jones' criteria are followed for diagnosis of RF.

Major criteria Major criteria
1. Carditis2. Polyarthritis.3. Chorea (Sydenham's chorea)4. Erythema marginatum5. Subcutaneous nodules

Minor criteria Minor criteria
1. Fever2. Arthralgia3. Previous history of RF4. Laboratory findings of elevated ESR,
raised C reactive protein, and leucocytosis.5.ECG finding of prolonged PR interval

You should haveYou should have
Two major or one major and two minor of the criteria.

Supportive evidenceSupportive evidence
Positive throat culture .Raised titers of (antispreptolysin O and S,
antistreptokinase, anti-streptohyaluronidase and anti DNAase)

Outcome and complicationsOutcome and complications
Myocarditis, in particular, is the most life-threatening due to involvement of the conduction system of the heart and results in serious arrhythmias. The long term sequelae or stigmata are the chronic valvular deformities,especially the mitral stenosis, AS, AI,etc as already explained.

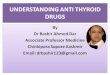
Normal valve is Transparent, avascular, thin flexible membrane.
Normal & Rheumatic Mitral Normal & Rheumatic Mitral valve:valve:
RHD: Thick, fibrous scarred stenotic & fixed (MS/MR) with Blood Vessels.
Recurrent Inflammation Scarring

Outcome and complicationsOutcome and complications
a stage of compensation occurs, while later decompensation of the heard leads to full-blown cardiac failure. Currently, surgical replacement of the damaged valves can alter the clinical course of the disease.

Outcome and complicationsOutcome and complications
The major causes of death in RHD are cardiac failure, bacterial endocarditis and embolism:

Secondary effectsSecondary effects
Marked left atrial dilatation may result from severe mitral stenosis or insufficiency.
formation of mural thrombi.Cor pulmonale may develop as a
consequence of secondary pulmonary hypertension induced by severe mitral valve disease

Course and diagnosisCourse and diagnosis
Valve replacement may become necessary. those who suffer recurrent attacks and complications.

Treatment of Rheumatic FeverTreatment of Rheumatic Fever
Bed restPatients who have not had carditis should
be advised bed rest until temperature and ESR become normal.
Patients who have had carditis should continue bed rest for 2-6 weeks after ESR and temperature became normal.

Anti-streptococcal theraphyAnti-streptococcal theraphy
A course of antibiotic should be given to eradicate the streptococci.
Even if throat culture is negative.One of the following may be used1.single injection of benzathine penicillin
1.2 million units intramascularly.2.daily injection of procaine penicillin
600000 units I/M x10days.

Anti-streptococcal theraphyAnti-streptococcal theraphy
Oral erythromycin 250-500mg 6-8 hrly if patient is sensitive to pencillin.

SalicylatesSalicylates
Aspirin is effective in providing symptomatic relief.
5-8 grams given daily in divided doses upto six times a day.until clinical improvement or systemic toxicity develops like tinnitus ,headache,hyperpnoea.
Aspirin at this dose continued until ESR is normal and then gradually tapered over 4-6 weeks.

CorticosteroidsCorticosteroids
Indications areSevere carditisCCFNot responding to aspirinPrednisolone 60-120 mg/day QID until ESR
normal, then tapered over 2 weeks.Monitoring of corticosteroids also based on
ESR, CRP.

Supportive theraphySupportive theraphy
Includes treatment of CCF, valvular leisions, heart blocks and chorea.

Prevention of Rheumatic Prevention of Rheumatic FeverFever
Primary preventionTreat group A streptococcal pharyngitis
when ever it occursMass pencillin treatment of population if
outbreak of rheumatic fever occurs.Treat streptococcal pharyngitis by pencillin
or erythromycin.

Secondary Secondary prevention(prophylaxis of RF)prevention(prophylaxis of RF)
Should be given to all patients who have experienced attack of rheumatic fever.
Broad outlines areThose under age of 18 should receive
continuous prophylaxis.Those who are over 18yrs who develop RF
without carditis should receive prophylaxis for a minimum period of 5 yrs..

Secondary Secondary prevention(prophylaxis of RF)prevention(prophylaxis of RF)
Decision to continue prophylaxis beyond 5 yrs in second group depend on many factors like age of patient, relative risks like acquiring infection, socioecnomic state, presence of rheumatic heart disease etc.

Secondary Secondary prevention(prophylaxis of RF)prevention(prophylaxis of RF)
One of the following regimens may be used.
I/M injection of 1.2 million units of benzathine pencillin G every 3 weeks.
Oral pencillin V 250 mg twice a day.Erythromycin 250 mg BD orally in case
allergic to pencillin.

ChoreaChorea
Intermittent or continuous fast jerky involuntary movements of parts of body.
Movements may be more on one side called hemichorea.
Facial chorea results from infrequent grimacing,blinking and slurring of speech.
The movements subside in sleep.Hypotonia may be present.

Treatment of Sydenham's Treatment of Sydenham's chorea/saint vitus dancechorea/saint vitus dance
Padded side boards for bed to prevent injury.
Haloperidol/sodium valproate with diazepam.
Rheumatic fever prophylaxis.Carbamazepine.

THANK YOU HELP PATIENTS SELFLESSLY
Recommended