11RD-RD-Teaching Aids: NNF
Respiratory distressRespiratory distress
• Cause of significant morbidity and Cause of significant morbidity and mortalitymortality
• Incidence 4 to 6% of live birthsIncidence 4 to 6% of live births• Many are preventableMany are preventable• Early recognition, timely referral, Early recognition, timely referral,
appropriate treatment essentialappropriate treatment essential
22RD-RD-Teaching Aids: NNF
Respiratory distressRespiratory distress
• RR > 60/ minRR > 60/ min**• Retractions Retractions • GruntGrunt• ++ Cyanosis Cyanosis
* Tachypnea* Tachypnea
33RD-RD-Teaching Aids: NNF
Causes of respiratory distressCauses of respiratory distress
• PulmonaryPulmonary
• Cardiac- Congenital heart disease Cardiac- Congenital heart disease
• CNS- Asphyxia, IC bleedCNS- Asphyxia, IC bleed
• Metabolic-Hypoglycemia, acidosisMetabolic-Hypoglycemia, acidosis

44RD-RD-Teaching Aids: NNF
Causes of respiratory distress - MedicalCauses of respiratory distress - Medical
• Respiratory distress syndrome (RDS)Respiratory distress syndrome (RDS)• Meconium aspiration syndrome (MAS)Meconium aspiration syndrome (MAS)• Transient tachypnoea of newborn (TTNB)Transient tachypnoea of newborn (TTNB)• Asphyxial lung diseaseAsphyxial lung disease• Pneumonia- Congenital, aspiration, nosocomialPneumonia- Congenital, aspiration, nosocomial• Persistent pulmonary hypertension (PPHN)Persistent pulmonary hypertension (PPHN)
55RD-RD-Teaching Aids: NNF
Surgical causes of respiratory distressSurgical causes of respiratory distress
• Tracheo-esophageal fistulaTracheo-esophageal fistula
• Diaphragmatic hernia Diaphragmatic hernia
• Lobar emphysemaLobar emphysema
• Pierre -Robin syndromePierre -Robin syndrome
• Choanal atresiaChoanal atresia
66RD-RD-Teaching Aids: NNF
Approach to respiratory distressApproach to respiratory distress
History History • Onset of distress Onset of distress • GestationGestation• Antenatal steroidsAntenatal steroids• Predisposing factors- PROM, feverPredisposing factors- PROM, fever• Meconium stained amniotic fluid Meconium stained amniotic fluid • AsphyxiaAsphyxia

77RD-RD-Teaching Aids: NNF
Approach to respiratory distressApproach to respiratory distressExaminationExamination• Severity of respiratory distressSeverity of respiratory distress• Neurological statusNeurological status• Blood pressure, CFTBlood pressure, CFT• HepatomegalyHepatomegaly• CyanosisCyanosis• Features of sepsisFeatures of sepsis• Look for malformationsLook for malformations
88RD-RD-Teaching Aids: NNF
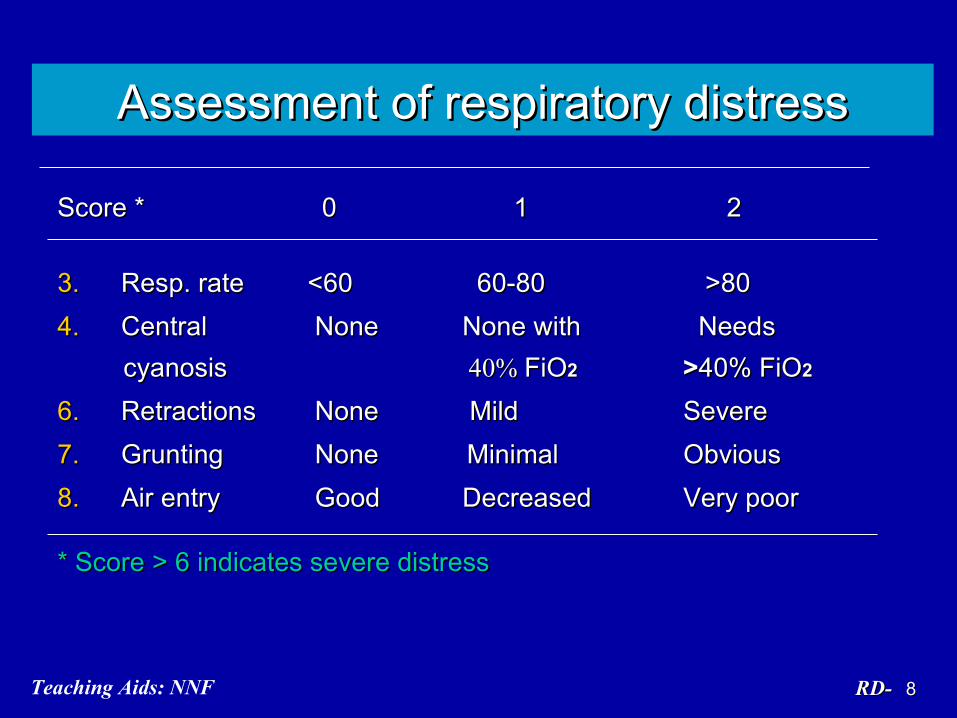
Assessment of respiratory distressAssessment of respiratory distress
Score *Score * 0 0 1 2 1 2
3.3. Resp. rateResp. rate <60 <60 60-80 60-80 >80 >80
4.4. Central Central None None None with Needs None with Needs cyanosiscyanosis 40% 40% FiOFiO2 2 >>40% FiO40% FiO2 2
6.6. Retractions NoneRetractions None Mild Mild Severe Severe
7.7. GruntingGrunting None Minimal None Minimal Obvious Obvious
8.8. Air entryAir entry Good Good Decreased Decreased Very poor Very poor
* Score > 6 indicates severe distress* Score > 6 indicates severe distress
99RD-RD-Teaching Aids: NNF
Approach to respiratory distressApproach to respiratory distress
Chest examinationChest examination
• Air entryAir entry
• Mediastinal shiftMediastinal shift
• Adventitious soundsAdventitious sounds
• HyperinflationHyperinflation
• Heart soundsHeart sounds
1010RD-RD-Teaching Aids: NNF
Preterm - Possible etiologyPreterm - Possible etiology
Early progressive - Early progressive - Respiratory distressRespiratory distress syndrome or hyaline syndrome or hyaline membrane disease membrane disease
(HMD)(HMD)
Early transient - Early transient - Asphyxia, metabolic Asphyxia, metabolic causes, hypothermiacauses, hypothermia
Anytime - PneumoniaAnytime - Pneumonia

1111RD-RD-Teaching Aids: NNF
Term – Possible etiologyTerm – Possible etiology
Early well lookingEarly well looking - - TTNB,TTNB, p polycythemiaolycythemiaEarly severe distress Early severe distress - MAS, asphyxia, - MAS, asphyxia,
malformations malformations Late sick with - CardiacLate sick with - Cardiac hepatomegaly hepatomegaly Late sick with shock Late sick with shock - Acidosis - AcidosisAnytime Anytime - Pneumonia - Pneumonia

1212RD-RD-Teaching Aids: NNF
Suspect surgical causeSuspect surgical cause
• Obvious malformationObvious malformation
• Scaphoid abdomenScaphoid abdomen
• FrothingFrothing
• History of aspirationHistory of aspiration
1313RD-RD-Teaching Aids: NNF
InvestigationsInvestigations
• Gastric aspirateGastric aspirate
• Polymorph countPolymorph count
• Sepsis screen Sepsis screen
• Chest X-rayChest X-ray
• Blood gas analysisBlood gas analysis
1414RD-RD-Teaching Aids: NNF
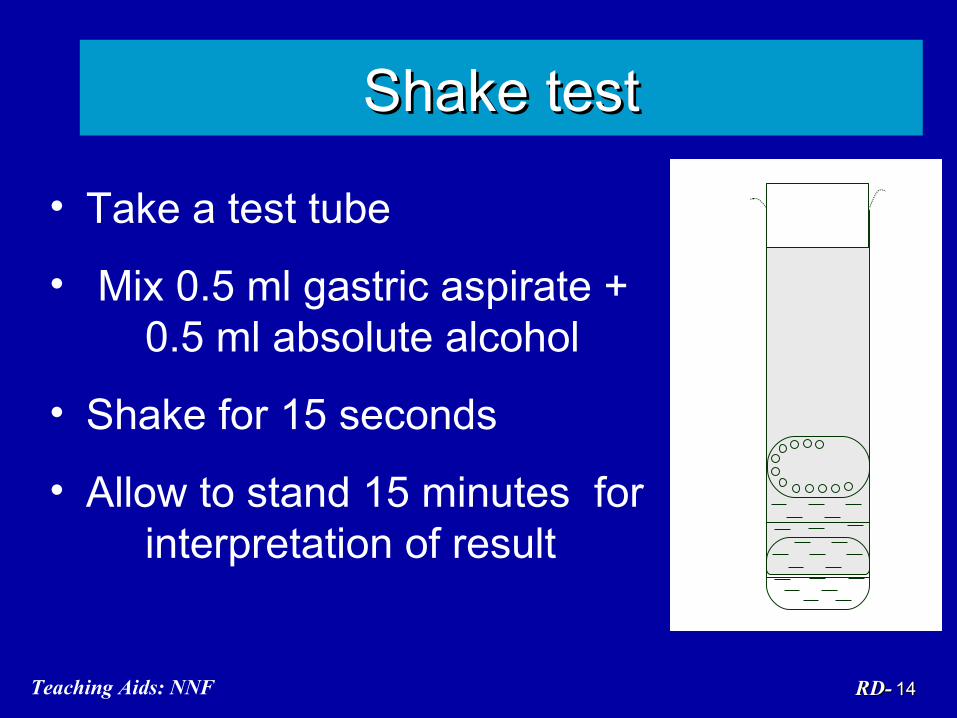
Shake testShake test
• Take a test tube
• Mix 0.5 ml gastric aspirate + 0.5 ml absolute alcohol
• Shake for 15 seconds
• Allow to stand 15 minutes for interpretation of result
1515RD-RD-Teaching Aids: NNF
Respiratory distress - Respiratory distress - ManagementManagement
• Monitoring Monitoring • SupportiveSupportive
- - IV fluidIV fluid- Maintain vital signs- Maintain vital signs- Oxygen therapy- Oxygen therapy- Respiratory support- Respiratory support
• SpecificSpecific
1616RD-RD-Teaching Aids: NNF
Oxygen therapy*Oxygen therapy* IndicationsIndications
• All babies with distressAll babies with distress• CyanosisCyanosis• Pulse oximetry SaOPulse oximetry SaO22 < < 90%90%
MethodMethod• Flow rate 2-5 L/ minFlow rate 2-5 L/ min• Humidified oxygen by hood or nasal prongsHumidified oxygen by hood or nasal prongs
* Cautious administration in pre-term* Cautious administration in pre-term
1717RD-RD-Teaching Aids: NNF
Pulse oximetryPulse oximetry
• Effective non invasive monitoring of Effective non invasive monitoring of oxygen therapyoxygen therapy
• Ideally must for all sick neonates and Ideally must for all sick neonates and those requiring oxygen therapythose requiring oxygen therapy
• Maintain SaOMaintain SaO22 between 90 – 93 % between 90 – 93 %
1818RD-RD-Teaching Aids: NNF
Respiratory distress syndrome (RDS)Respiratory distress syndrome (RDS)
• Pre-term babyPre-term baby
• Early onset within 6 hoursEarly onset within 6 hours
• Supportive evidence: Negative shake testSupportive evidence: Negative shake test
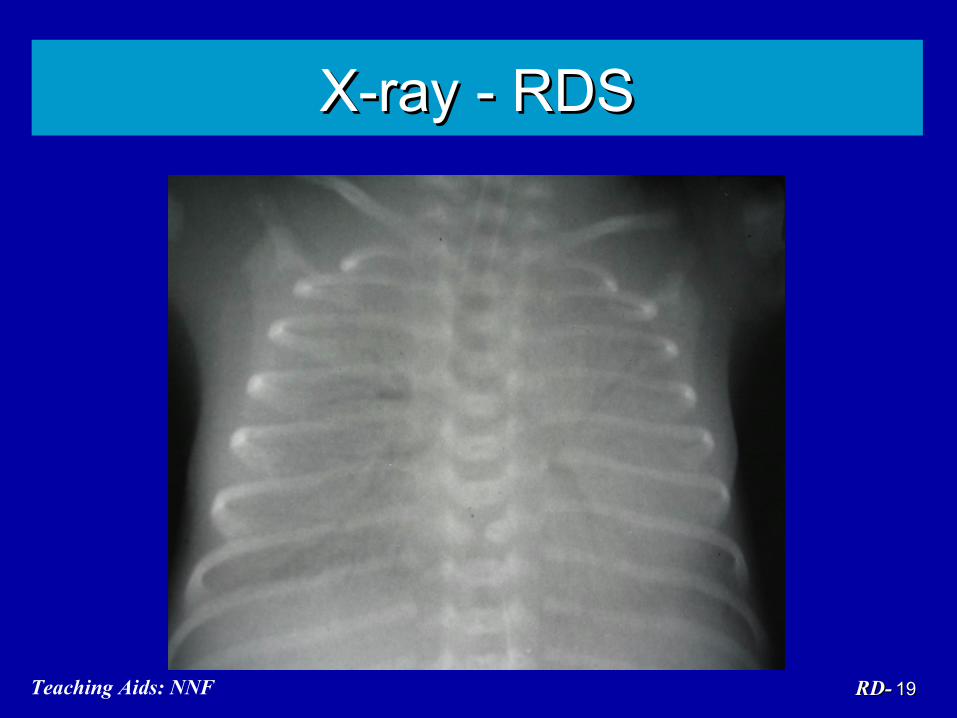
• Radiological evidenceRadiological evidence
1919RD-RD-Teaching Aids: NNF
X-ray - RDSX-ray - RDS
2020RD-RD-Teaching Aids: NNF
Pathogenesis of RDSPathogenesis of RDS
• Decreased or abnormal surfactantDecreased or abnormal surfactant
• Alveolar collapse Alveolar collapse
• Impaired gas exchangeImpaired gas exchange
• Respiratory failureRespiratory failure
2121RD-RD-Teaching Aids: NNF
RDS - Predisposing factorsRDS - Predisposing factors
• Prematurity Prematurity • Cesarean bornCesarean born• Asphyxia Asphyxia
• Maternal diabetesMaternal diabetes
RDS - Protective factorsRDS - Protective factors• PROMPROM• IUGRIUGR• SteroidsSteroids
2222RD-RD-Teaching Aids: NNF
Antenatal corticosteroidAntenatal corticosteroid - - Simple therapy that saves neonatal livesSimple therapy that saves neonatal lives
• Preterm labor 24-34 weeks of gestation Preterm labor 24-34 weeks of gestation irrespective of PROM, hypertension and irrespective of PROM, hypertension and diabetesdiabetes
• Dose:Dose:Inj Betamethasone 12mg IM every 24 hrs X Inj Betamethasone 12mg IM every 24 hrs X 2 doses; or Inj Dexamethasone 6 mg IM 2 doses; or Inj Dexamethasone 6 mg IM every 12 hrs X 4 dosesevery 12 hrs X 4 doses
• Multiple doses not beneficialMultiple doses not beneficial
2323RD-RD-Teaching Aids: NNF
Surfactant therapy - IssuesSurfactant therapy - Issues
• Should be used only if facilities for Should be used only if facilities for ventilation availableventilation available
• CostCost
• Prophylactic Vs rescueProphylactic Vs rescue
2424RD-RD-Teaching Aids: NNF
Prophylactic therapyProphylactic therapy Extremely preterm <28 wks Extremely preterm <28 wks <1000 gm <1000 gm Not routine in IndiaNot routine in India
Rescue therapyRescue therapy Any neonate diagnosed to have RDSAny neonate diagnosed to have RDS
Surfactant therapy - Issues
Dose 100mg/kg phospholipid Intra trachealDose 100mg/kg phospholipid Intra tracheal

2525RD-RD-Teaching Aids: NNF
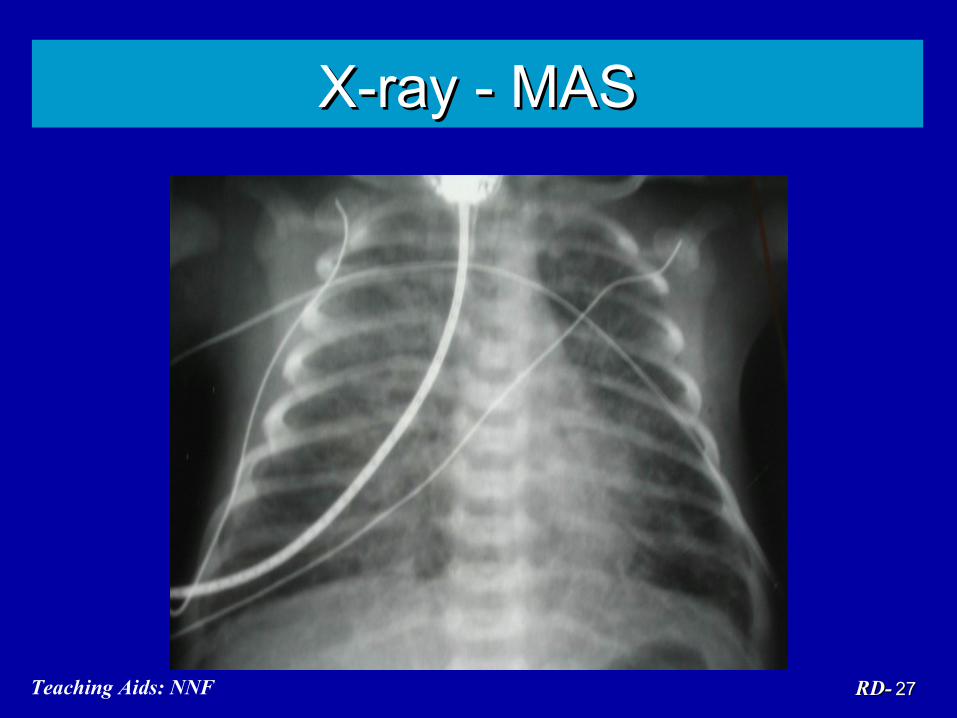
Meconium aspiration syndrome (MAS)Meconium aspiration syndrome (MAS)
• Meconium stainingMeconium staining - Antepartum, intrapartum- Antepartum, intrapartum• ThinThin - Chemical pneumonitis- Chemical pneumonitis• ThickThick - Atelectasis, airway blockage, air - Atelectasis, airway blockage, air
leak syndromeleak syndrome

2626RD-RD-Teaching Aids: NNF
Meconium aspiration syndromeMeconium aspiration syndrome
• Post term/SFDPost term/SFD
• Meconium staining – cord, nails, skinMeconium staining – cord, nails, skin
• Onset within 4 to 6 hoursOnset within 4 to 6 hours
• Hyperinflated chestHyperinflated chest
2727RD-RD-Teaching Aids: NNF
X-ray - MASX-ray - MAS
2828RD-RD-Teaching Aids: NNF
MAS - PreventionMAS - Prevention
• Oropharyngeal suction before delivery of Oropharyngeal suction before delivery of shoulder for shoulder for all all neonates born through neonates born through MSAFMSAF
• Endotracheal suction for Endotracheal suction for non vigorous* non vigorous* neonates born through MSAFneonates born through MSAF
**Avoid bag & mask ventilation till trachea is Avoid bag & mask ventilation till trachea is clearedcleared
2929RD-RD-Teaching Aids: NNF
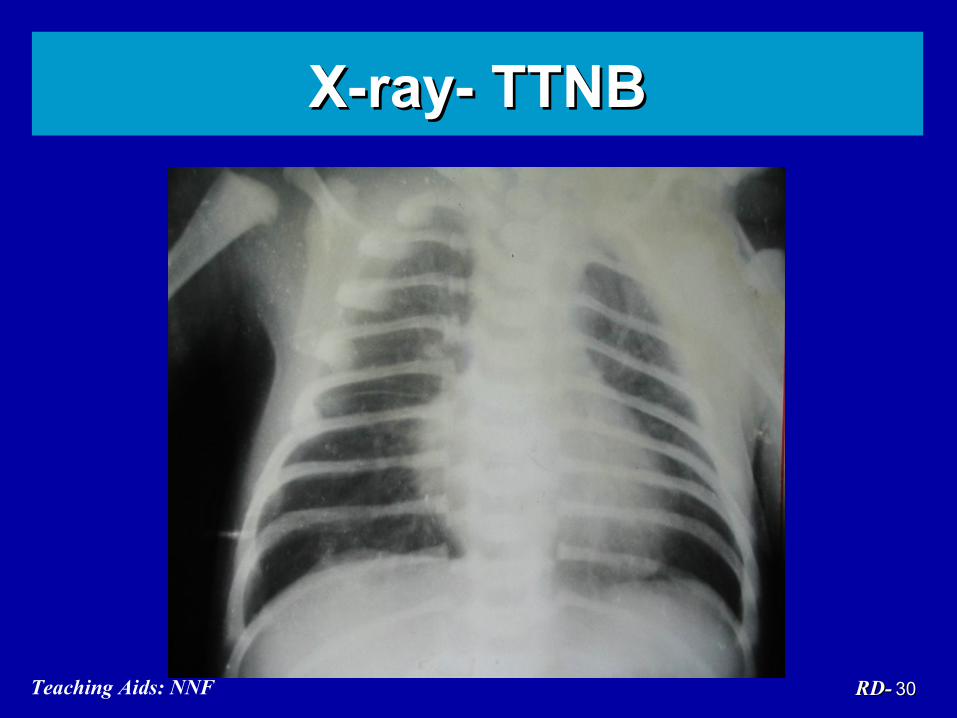
Transient tachypnoea of newborn Transient tachypnoea of newborn (TTNB)(TTNB)
• Cesarean born, term babyCesarean born, term baby
• Delayed clearance of lung fluidDelayed clearance of lung fluid
• Diagnosis by exclusionDiagnosis by exclusion
• Management: supportiveManagement: supportive
• Prognosis - goodPrognosis - good
3030RD-RD-Teaching Aids: NNF
X-ray- TTNBX-ray- TTNB

3131RD-RD-Teaching Aids: NNF
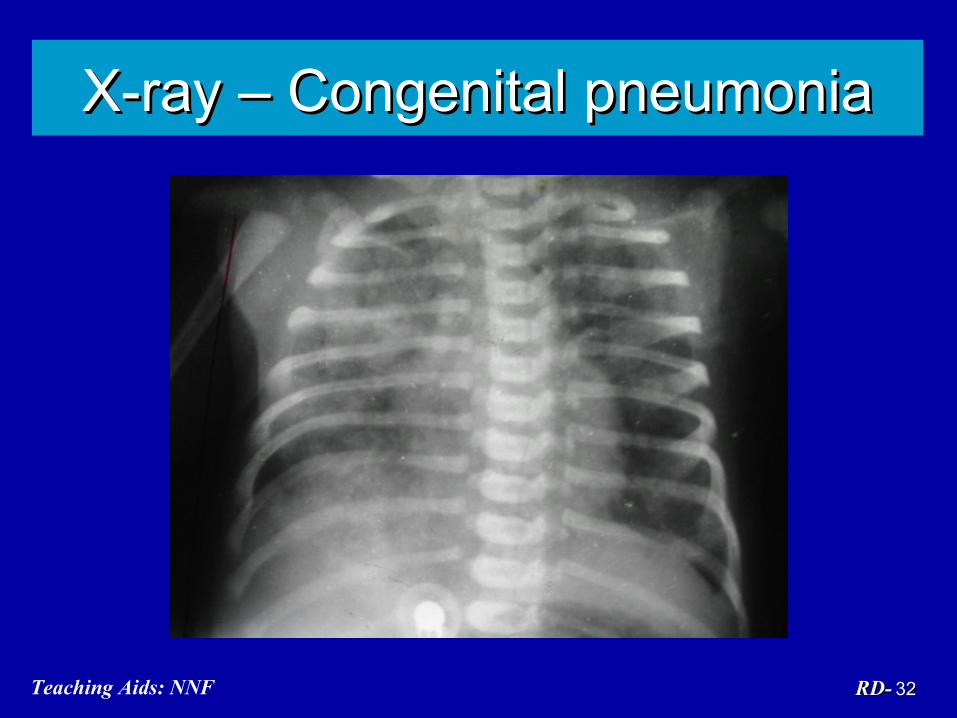
Congenital pneumoniaCongenital pneumonia
Predisposing factorsPredisposing factors PROM >24 hours, foul smelling liquor, PROM >24 hours, foul smelling liquor,
Peripartal fever, unclean or multiple per Peripartal fever, unclean or multiple per vaginal vaginal
TreatmentTreatment Thermoneutral environment, NPO, IV Thermoneutral environment, NPO, IV
fluids, Oxygen, antibiotics-fluids, Oxygen, antibiotics-(Amp+Gentamicin)(Amp+Gentamicin)
3232RD-RD-Teaching Aids: NNF
X-ray – Congenital pneumoniaX-ray – Congenital pneumonia
3333RD-RD-Teaching Aids: NNF
Nosocomial pneumoniaNosocomial pneumonia
Risk Factor Risk Factor : Ventilated neonates: Ventilated neonates : Preterm neonates: Preterm neonates
Prevention Prevention : Handwash: Handwash: Use of disposables: Use of disposables
: Infection control : Infection control measures measures
Antibiotics Antibiotics : Usually require higher : Usually require higher antibiotics antibiotics
3434RD-RD-Teaching Aids: NNF
Respiratory distress in a neonate with Respiratory distress in a neonate with asphyxiaasphyxia
• Myocardial dysfunctionMyocardial dysfunction
• Cerebral edema Cerebral edema
• Asphyxial lung injury Asphyxial lung injury
• Metabolic acidosisMetabolic acidosis
• Persistent pulmonary hypertensionPersistent pulmonary hypertension

3535RD-RD-Teaching Aids: NNF
PneumothoraxPneumothorax
EtiologyEtiologySpontaneous, MAS, Positive pressure Spontaneous, MAS, Positive pressure
ventilation (PPV)ventilation (PPV)
Clinical featuresClinical featuresSudden distress, indistinct heart soundsSudden distress, indistinct heart sounds
ManagementManagement Needle aspiration, chest tubeNeedle aspiration, chest tube

3636RD-RD-Teaching Aids: NNF
X-ray - PneumothoraxX-ray - Pneumothorax
3737RD-RD-Teaching Aids: NNF
Persistent pulmonary Persistent pulmonary hypertension (PPHN) hypertension (PPHN)
CausesCauses• Primary Primary • Secondary: MAS, asphyxia, sepsis Secondary: MAS, asphyxia, sepsis
Management Management • Severe respiratory distress needing Severe respiratory distress needing
ventilatory support, pulmonary ventilatory support, pulmonary vasodilatorsvasodilators
• Poor prognosis Poor prognosis
3838RD-RD-Teaching Aids: NNF
Respiratory distressRespiratory distress (needing referral) (needing referral)
• RDS (HMD)RDS (HMD)• MASMAS• Surgical or cardiac causeSurgical or cardiac cause• PPHNPPHN• Severe or worsening distressSevere or worsening distress
Recommended

















